Left Lateral Decubitus | Rib Resection Two Levels Above Target | Segmental Vessel Ligation at Mid-Body | Mandatory Chest Tube
- Left lateral decubitus is preferred to keep the aorta under direct vision and avoid the liver, which obstructs the lower field on the right.
- The rib resected is typically two levels cephalad to the target vertebral body, giving the correct angle to reach the disc space perpendicularly.
- Segmental vessels are ligated at the mid-vertebral body level (well away from the neural foramen) to allow safe subperiosteal exposure and aortic mobilisation.
- The artery of Adamkiewicz usually arises from a left segmental artery between T9 and T12 (about 80 percent of individuals) - identify and preserve it if possible.
- A chest tube (28-32 French) is mandatory post-operatively, placed posteriorly and basally with an apical port if pneumothorax risk is high.
When & Why
What it exposes. The transthoracic (thoracotomy) approach gives direct anterior exposure of the thoracic vertebral bodies and discs from approximately T4 to T12 through a left (preferred) or right thoracotomy, after rib resection and transpleural entry. No other approach offers the same degree of anterior column access without traversing the spinal canal. Why this approach is chosen. It allows a complete corpectomy, decompression of the spinal canal from the front, and reconstruction with strut grafts, cages or vascularised fibula. It is therefore the workhorse exposure for anterior pathology where posterior approaches are inadequate or high-risk. Indications - Anterior corpectomy and reconstruction for tumour (primary or metastatic)
- Vertebral osteomyelitis with abscess or instability requiring debridement
- Thoracic disc herniation with myelopathy when anterior decompression is needed
- Post-traumatic kyphosis or burst fracture with anterior column deficiency
- Deformity correction requiring anterior release or osteotomy
- Failed posterior surgery with persistent anterior pathology Contraindications - Severe pulmonary disease precluding single-lung ventilation
- Previous thoracotomy with dense adhesions (relative)
- Active pleural infection or empyema
- Inability to tolerate the lateral decubitus position
- High thoracic levels (T1-T3) better accessed via manubrium or sternotomy Alternative approaches - Posterior transpedicular or costotransversectomy for selected tumours
- Lateral extracavitary approach for the thoracolumbar junction
- Endoscopic (VATS) transthoracic approach for selected disc herniations
- Combined anterior-posterior staged procedures for complex tumours
- When it is used
- Left lateral decubitus, rib two levels above target - most common for T6-T11
- When it is used
- Right lateral decubitus for upper thoracic T4-T6, where the aorta is less of an issue
- When it is used
- Cervicothoracic junction T1-T3 (rare)
Position & landmarks. The patient is placed in the left lateral decubitus position on a radiolucent table. Confirm the double-lumen endotracheal tube with fibreoptic bronchoscopy, establish an arterial line and central venous access, and place a Foley catheter. Support position with a beanbag, place an axillary roll under the dependent axilla to protect the brachial plexus, pad every pressure point, and abduct the upper arm less than 90 degrees. Flexing the table at the thoracolumbar junction (with a kidney rest if needed) opens the intercostal spaces. C-arm or O-arm access is verified from both anterior and lateral; neuromonitoring leads (MEP/SSEP) are placed if used. Surface anatomy and incision planning - Spinous processes - counted from C7 (vertebra prominens) downward
- Scapula - the inferior angle lies approximately at T7
- Iliac crest - approximately the L4-L5 level, for reference
- Latissimus dorsi forms the posterior border of the incision, serratus anterior the anterior border, and the paravertebral muscles the medial limit The incision is centred over the rib to be resected - typically two levels cephalad to the target vertebra (for the T7 body, the eighth or ninth rib is commonly resected). It runs from the paravertebral line anteriorly in a gentle curve or hockey-stick shape, 15-20 cm long. Fluoroscopic confirmation of the rib level is mandatory before the skin incision. At thoracotomy the surgeon counts ribs directly: the first rib is identified by its articulation with the manubrium and its lack of a costal groove, while the second rib is the first to carry a costal groove.
Single-lung ventilation can cause hypoxia, hypercarbia and raised pulmonary vascular resistance. The anaesthetist must be experienced with double-lumen tubes, arterial blood gases are monitored continuously, and the team must be ready to reinflate the lung. Keep operative time reasonable and reinflate the lung periodically if exposure is prolonged.
The Exposure
Work down through the chest wall, protecting the intercostal neurovascular bundle during rib resection, enter the pleura and deflate the lung, then ligate segmental vessels at the mid-body to mobilise the aorta and expose the vertebral column.
Chest-wall anatomy on the way in
- Key structures
- Superficial branches of intercostal nerves
- Clinical relevance
- Incision planning over the selected rib
- Key structures
- Latissimus dorsi, serratus anterior, intercostal muscles
- Clinical relevance
- Split or divide in the line of their fibres
- Key structures
- Periosteum, intercostal neurovascular bundle in costal groove
- Clinical relevance
- Strip subperiosteally; protect the bundle
- Key structures
- Parietal and visceral pleura
- Clinical relevance
- Transpleural entry; deflate the lung
Step-by-step exposure
- Make the skin incision through subcutaneous tissue directly over the selected rib (two levels cephalad to the target).
- Identify latissimus dorsi posteriorly and serratus anterior anteriorly, and split or divide them in the line of the incision to reach the rib periosteum.
- Incise the periosteum along the superior border of the rib with electrocautery - the neurovascular bundle lies in the costal groove on the inferior surface, so begin here where it is absent.
- Strip the periosteum circumferentially with a periosteal elevator, then carefully elevate the inferior periosteum, protecting the intercostal neurovascular bundle in the costal groove (vein-artery-nerve, superior to inferior).
- Cut the rib posteriorly at the costotransverse joint and anteriorly at the costochondral junction using rib cutters, and remove the segment.
- The resected rib can be morcellised for autograft. Smooth the cut ends of the remaining rib to prevent later lung injury.
- Incise the parietal pleura carefully and enter the pleural cavity.
- Identify the lung and confirm deflation. Divide any adhesions sharply or with electrocautery under direct vision, then place a rib spreader to maintain exposure.
- Deflate the left lung with the double-lumen tube and gently retract it anteriorly and medially with a malleable or lung retractor, protecting the parenchyma with moist sponges.
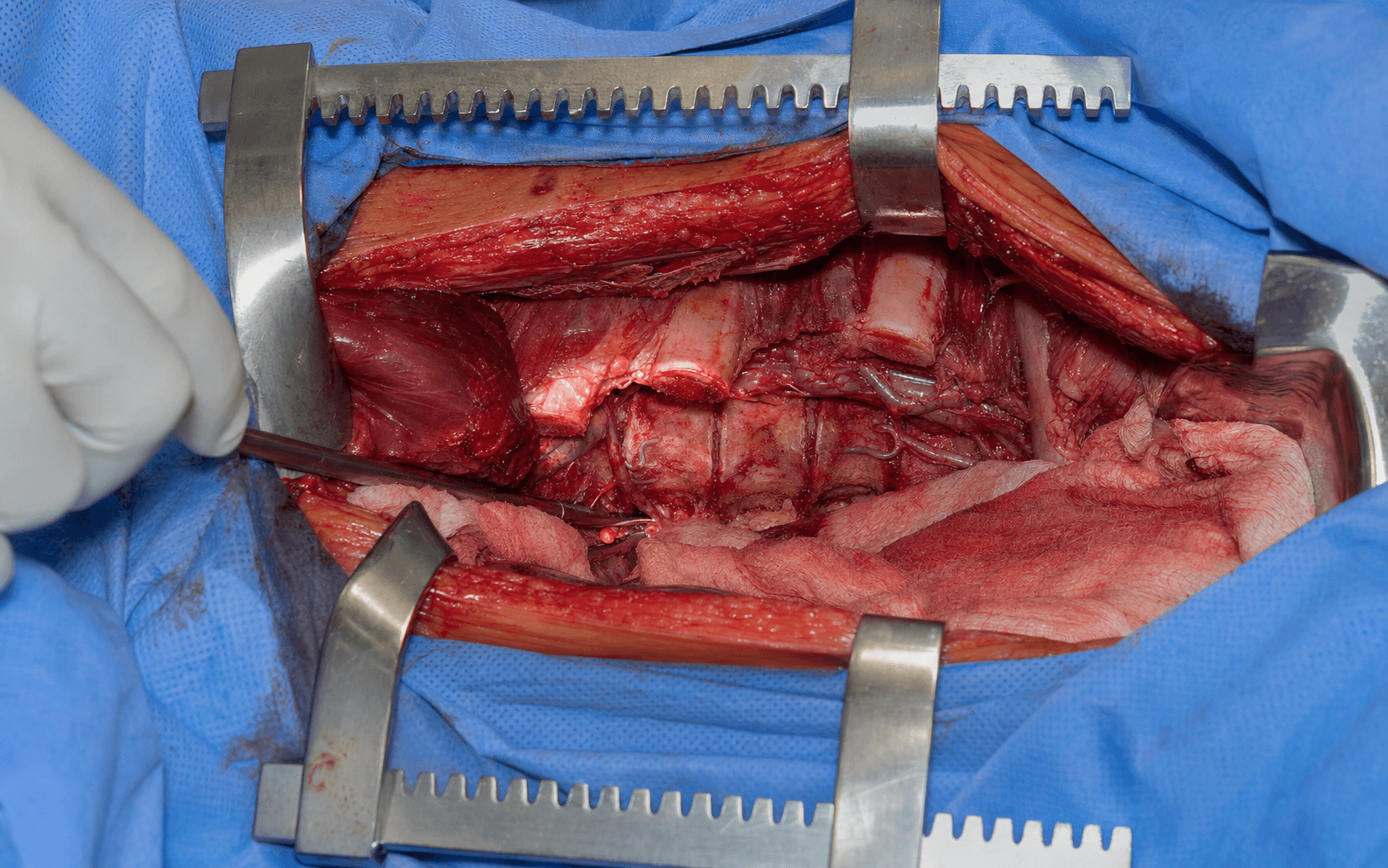
- Identify the descending aorta, the azygos vein and the thoracic duct.
- Identify the segmental vessels crossing the mid-vertebral body and ligate them with silk ties or vascular clips at mid-body level - well away from the neural foramen - then divide between ligatures.
- Mobilise the aorta gently off the vertebral bodies with a Cobb elevator or peanut dissector, and protect it with a malleable retractor.
- Identify and protect the thoracic duct (right of the aorta in the mid-thorax; it crosses to the left at T4-T5).
- Trace the sympathetic chain running along the rib heads and preserve it unless tumour involvement requires sacrifice.
- Watch for the artery of Adamkiewicz, usually arising from a left segmental vessel between T9 and T12, and preserve it if possible.
- With the aorta mobilised, the anterior longitudinal ligament, disc spaces and vertebral bodies are fully exposed.
- Incise the discs with a knife and remove them with rongeurs and curettes; perform corpectomy with osteotomes, rongeurs and a high-speed burr, protecting the dura with a Penfield dissector.
- Achieve meticulous haemostasis of all raw surfaces and irrigate the pleural cavity copiously with warm saline.
- Inspect the lung for injury or air leak, and confirm that all segmental vessels are securely ligated and the aorta is intact.
- Place a 28-32 French chest tube through a separate stab incision in the posterior axillary line, positioned posteriorly and basally (add an apical tube if pneumothorax risk is high), and connect to underwater seal.
- Close the parietal pleura (absorbable) if possible, approximate the intercostal muscles, then close latissimus dorsi and serratus anterior, subcutaneous tissue and skin. Confirm lung re-expansion and obtain a chest radiograph.
The transthoracic approach does not rely on a true internervous plane, because the exposure traverses the chest wall and pleural cavity rather than splitting muscle between two nerve supplies. Safety comes from subperiosteal rib resection, single-lung ventilation, and precise ligation of segmental vessels at the mid-vertebral body rather than near the foramen. The intercostal nerve is protected within the costal groove, and the lung is deflated to create working space without forceful retraction.
Dangers & Extensions
Structures at risk, layer by layer
- Structure at risk
- Intercostal neurovascular bundle (vein-artery-nerve in costal groove)
- Protection
- Identify before rib resection; strip the rib superiorly first; protect the bundle
- Structure at risk
- Lung parenchyma
- Protection
- Double-lumen deflation; gentle, moist-sponge retraction; inspect for air leak
- Structure at risk
- Segmental vessels and the aorta
- Protection
- Ligate at mid-body away from the foramen; mobilise the aorta gently; malleable retractor protection
- Structure at risk
- Artery of Adamkiewicz (left T9-T12)
- Protection
- Preoperative angiography in elective cases; intraoperative Doppler; preserve if identified
- Structure at risk
- Thoracic duct (crosses left at T4-T5)
- Protection
- Identify and protect; ligate proximally and distally if injured
- Structure at risk
- Sympathetic chain along the rib heads
- Protection
- Preserve unless tumour involvement requires sacrifice
The most critical structure at risk. Arises most commonly from a left segmental artery between T9 and T12 and supplies the anterior spinal artery to the lower thoracic cord. Injury produces anterior spinal artery syndrome - paraplegia with loss of pain and temperature but preserved dorsal column sensation. Identify with preoperative angiography in elective cases or intraoperative Doppler.
Ascends on the right of the aorta from T5-T6 and crosses to the left at T4-T5, so it is at risk during a left thoracotomy in the upper field. Injury causes chylothorax with high-output milky drainage; if injured, ligate proximally and distally and monitor chest-tube output for chyle.
The descending aorta lies immediately anterior to the left side of the vertebral bodies - mobilise gently only after segmental ligation. The azygos vein lies on the right and crosses the midline at T4. Protect both with malleable retractors; major injury requires immediate vascular repair or shunt.
Runs in the costal groove on the inferior border of each rib in the order vein-artery-nerve. It is most vulnerable at the costotransverse joint where it emerges from the foramen. Injury causes intercostal neuralgia or bleeding - protect it during periosteal stripping.
Runs vertically along the rib heads, anterior to the vertebral bodies. Injury causes ipsilateral Horner syndrome (ptosis, miosis, anhidrosis) if the stellate ganglion at T1 is involved. Preserve unless tumour involvement requires sacrifice.
At risk during rib resection, retractor placement and closure. Avoid forceful retraction and inspect for air leak before closure. The chest tube prevents pneumothorax; bronchopleural fistula is rare but serious.
Adamkiewicz injury management - If suspected intraoperatively: maintain blood pressure, consider steroids per protocol, and obtain an urgent MRI.
- Postoperative paraplegia: immediate MRI, maintain mean arterial pressure greater than 85 mmHg, and consider a CSF drain.
- Prevention is paramount - preoperative angiography in elective tumour cases, careful ligation technique, and avoidance of hypotension. Extensile modifications - Proximal (cervicothoracic junction, T1-T3): the standard thoracotomy is limited by the scapula and first rib. Options are an extended incision with scapular mobilisation (Paulsen approach), a manubrial split or sternotomy with clavicle osteotomy, or a combined cervical and thoracic exposure.
- Distal (thoracolumbar junction, T11-L2): the diaphragm must be managed - a radial incision with peripheral detachment, circumferential detachment from the chest wall, or conversion to a formal thoracoabdominal approach, mobilising the psoas anteriorly to reach the lumbar bodies.
- Combined anterior-posterior: staged or same-day anterior decompression then posterior stabilisation is common for tumours and fractures; some centres do both in the lateral position through a separate posterior incision.
- Minimally invasive: VATS or mini-thoracotomy with tubular retractors for selected discs and biopsies reduces pulmonary morbidity but limits the extent of reconstruction. Complications
- Prevention
- Fluoroscopy, rib counting, preoperative marking
- Management
- Immediate re-exploration if recognised
- Prevention
- Preoperative angiography, careful ligation
- Management
- Maintain MAP greater than 85 mmHg, CSF drain
- Prevention
- Gentle mobilisation, adequate exposure
- Management
- Immediate vascular repair, shunt if needed
- Prevention
- Identify and protect
- Management
- Ligate proximally and distally
- Prevention
- Protect the bundle during rib resection
- Management
- Local anaesthetic, neuropathic pain management
- Prevention
- Careful retraction, single-lung ventilation
- Management
- Repair the laceration, chest tube
- Incidence
- 10-20 percent
- Prevention
- Early mobilisation, incentive spirometry
- Treatment
- Chest physiotherapy, antibiotics
- Incidence
- 1-3 percent
- Prevention
- Identify the duct, ligate if injured
- Treatment
- Conservative (drain, TPN) or surgical ligation
- Incidence
- 2-5 percent
- Prevention
- Prophylactic antibiotics, meticulous closure
- Treatment
- Irrigation, debridement, antibiotics
- Incidence
- 3-8 percent
- Prevention
- Adequate reconstruction, anterior-posterior construct
- Treatment
- Revision surgery
- Incidence
- 1-5 percent
- Prevention
- Careful decompression, maintain perfusion
- Treatment
- MRI, blood pressure management, re-exploration
- Incidence
- 10-30 percent
- Prevention
- Intercostal nerve protection, multimodal analgesia
- Treatment
- Neuropathic agents, nerve blocks
Pulmonary complications (atelectasis, pneumonia, prolonged ventilation) occur in 10-20 percent of transthoracic spine procedures. Risk factors are advanced age, smoking, obesity, prolonged operative time and poor pain control. Aggressive pulmonary toilet, early mobilisation and multimodal analgesia reduce this risk significantly.
Closure and post-operative care - Chest tube: keep on underwater seal, monitor output and air leak, and obtain daily chest radiographs. Remove when output is less than 100 mL per day and the lung is fully expanded.
- Pain control: multimodal - PCA, intercostal blocks, NSAIDs and paracetamol; avoid excessive opioids that suppress respiration.
- Pulmonary toilet: incentive spirometry every hour while awake, early mobilisation to chair, chest physiotherapy.
- Neurological monitoring: hourly neurovascular checks for the first 24 hours (lower limb power, sensation, reflexes).
- DVT prophylaxis: mechanical (intermittent pneumatic compression) plus pharmacological (LMWH) once haemostasis is secure.
- Mobilisation: to chair on day 1 if stable; ambulate once the chest tube is out and pain is controlled; brace with a TLSO if the posterior elements are deficient or instrumentation is marginal; no heavy lifting or bending for 6-12 weeks.
- Follow-up: 2 weeks (wound, CXR, neurology), 6 weeks (radiographs, activity), 3 months (reconstruction stability), 6 months (function), 1 year (final review).
Procedures Through This Approach
- Spine tumour decompression and stabilisation - the principal indication for this exposure.
- Anterior corpectomy with cage or strut-graft reconstruction for tumour, infection or fracture.
- Anterior decompression of a thoracic disc herniation with myelopathy.
- Debridement and reconstruction for vertebral osteomyelitis.
- En bloc or piecemeal resection of primary or metastatic vertebral tumours.
- Anterior release and fusion for scoliosis or kyphosis.
- Anterior instrumentation with plate or rod constructs. Reconstruction options: titanium or PEEK cage with autograft or allograft; vascularised fibular strut graft for large defects; anterior plate fixation (less common in the thoracic spine); or combined anterior and posterior instrumentation for instability.
Viva & Exam Focus
THORACICThe exposure, step by step
ADAMKDanger structures, layer by layer
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old with known breast cancer presents with progressive thoracic back pain and mild lower limb weakness. MRI shows a T8 vertebral body metastasis with retropulsion and cord compression. How would you approach anterior decompression and reconstruction?”
“A 45-year-old presents with progressive myelopathy and a large central T7-T8 disc herniation on MRI. Posterior approaches are considered high risk due to cord compression. Describe your surgical plan using the transthoracic approach.”
“A 58-year-old diabetic presents with T10 osteomyelitis, discitis and a large paravertebral abscess causing sepsis. Posterior surgery has failed to control infection. Describe the transthoracic approach for debridement and reconstruction.”
Positioning
- Left lateral decubitus (right side up for upper thoracic)
- Double-lumen ETT for single-lung ventilation
- Axillary roll, beanbag, all pressure points padded
- Table flexed at the thoracolumbar junction
Rib selection
- Resect the rib two levels cephalad to the target vertebra
- Fluoroscopic confirmation mandatory before incision
- Count ribs from the top after pleural entry
- T10 vertebra - resect the twelfth rib
Internervous plane
- No true internervous plane (transpleural approach)
- Protect the intercostal bundle in the costal groove
- Ligate segmental vessels at the mid-vertebral body
- Mobilise the aorta gently after ligation
Danger structures
- Artery of Adamkiewicz (left T9-T12) - preserve if possible
- Thoracic duct (crosses at T4-T5 on a left approach)
- Aorta and azygos vein - mobilise carefully
- Sympathetic chain - preserve unless tumour involved
Closure
- 28-32Fr chest tube in the posterior basal position
- Layered chest wall closure
- Confirm lung re-expansion on the table
- Daily chest radiograph until the tube is removed
Procedures
- Anterior corpectomy and cage reconstruction
- Thoracic disc herniation decompression
- Tumour resection (en bloc or piecemeal)
- Infection debridement and reconstruction
References
The transthoracic approach is used worldwide for anterior thoracic spine pathology. Principles are consistent across advanced orthopaedic practice and other examination systems: careful patient selection, preoperative imaging to identify the artery of Adamkiewicz when possible, meticulous segmental vessel ligation at the mid-body, and mandatory chest tube drainage.
- Position on the transthoracic approach
- Anterior approach indicated for tumours, infection and selected deformities; preoperative vascular imaging recommended for elective cases; combined anterior-posterior constructs for instability
- Position on the transthoracic approach
- Transthoracic approach appropriate for thoracic disc herniation with myelopathy when posterior access is high risk; chest tube management protocol essential
- Position on the transthoracic approach
- Multidisciplinary team approach for spinal tumours; anterior decompression considered when cord compression is primarily anterior
- Position on the transthoracic approach
- High-volume centres should offer transthoracic expertise; transfer protocols for complex thoracic spine pathology
Registry evidence - The AO Spine Tumour Registry and similar databases show that anterior reconstruction improves local control and neurological outcomes in selected thoracic metastases.
- Pulmonary complication rates of 10-20 percent are consistently reported; aggressive perioperative pulmonary care is the key modifiable factor. Global practice variation In high-resource settings, navigation, intraoperative angiography and advanced reconstruction implants are routine. In resource-limited settings the same principles apply using standard rib resection, silk ties for vessels, and autograft from the resected rib. Chest tube management remains mandatory everywhere. Consent (globally applicable) Discuss paraplegia risk from Adamkiewicz injury (1-3 percent in experienced hands), chylothorax (1-3 percent), pulmonary complications (10-20 percent), wound infection (2-5 percent), post-thoracotomy pain, and the need for chest tube drainage for several days postoperatively.
Be able to describe the left transthoracic approach step by step: lateral decubitus positioning, double-lumen tube, rib two levels above the target, subperiosteal resection protecting the intercostal bundle, segmental vessel ligation at the mid-body, Adamkiewicz identification, and chest tube closure. Know the danger structures and how to manage each complication.
Surgical Approach to Thoracic Disc Herniation
- Transthoracic approach provided superior exposure for central thoracic disc herniations compared with posterior approaches
- Neurological improvement in 87 percent of myelopathic patients
- Pulmonary complications occurred in 12 percent but were manageable with chest tube drainage
Anterior excision of herniated thoracic discs
- Anterior transthoracic excision of herniated thoracic discs achieved neurological improvement in the majority of patients with myelopathy
Transthoracic approaches to thoracic disc herniations
- Transthoracic approach provides excellent exposure for central thoracic disc herniations with low morbidity when performed with proper technique and chest tube management
Experience in the surgical management of symptomatic thoracic disc herniations
- Transthoracic corpectomy and discectomy for thoracic pathology yields high rates of neurological recovery when segmental vessels are managed appropriately