Release of the ulnar nerve in the fibro-osseous tunnel at the wrist · Shea-McClain Zones 1–3
- Guyon's canal is a roughly 4 cm fibro-osseous tunnel bounded by the pisiform (ulnar), the hook of hamate (radial), palmaris brevis and the volar carpal ligament (roof), and the flexor retinaculum and pisohamate ligament (floor).
- The ulnar nerve bifurcates within the canal into a superficial sensory branch (small finger and ulnar ring finger sensation) and a deep motor branch, which curves around the hook of hamate to supply all intrinsics except the thenar muscles and the lateral two lumbricals.
- Three-zone classification (Shea and McClain): Zone 1 — proximal to the bifurcation, mixed motor and sensory; Zone 2 — deep motor branch only, a pure motor deficit; Zone 3 — superficial sensory branch only, a pure sensory deficit.
- The most common causes are a ganglion cyst (around half of cases presenting with a mass), ulnar artery thrombosis or aneurysm (hypothenar hammer syndrome), a hook of hamate fracture, and handlebar palsy in cyclists.
- The palmar cutaneous branch of the ulnar nerve runs superficial to the canal and is the structure most commonly injured during the approach — identify and protect it with loupe magnification.
- The deep motor branch is the most critical structure in the field — injury causes intrinsic paralysis and devastating functional loss, so it must be protected and fully decompressed.
- An Allen test is mandatory before any ulnar artery intervention, to confirm adequate radial artery perfusion through the palmar arches.
- Hook of hamate fractures should be excised (not fixed) because of poor healing and the high risk of nerve injury with ORIF.
When & Why
Indication. Surgical decompression of Guyon's canal is offered for ulnar nerve compression at the wrist (ulnar tunnel syndrome) that is progressive, disabling, or driven by a space-occupying lesion — after a documented failure of conservative care (activity modification, splinting, and addressing any vascular or occupational cause). Typical triggers are progressive intrinsic weakness with atrophy, a mass compressing the nerve, persistent symptoms for 3 to 6 months despite non-operative management, electrodiagnostic studies localising compression to the wrist, or acute trauma with an expanding haematoma in the canal.
Progressive motor weakness with intrinsic atrophy despite conservative care; a space-occupying lesion (ganglion, thrombosed ulnar artery, hook of hamate fracture); persistent symptoms for 3 to 6 months despite splinting and activity modification; positive electrodiagnostic studies localising compression to the wrist; acute trauma with expanding haematoma or compartment syndrome in the canal.
Mild to moderate symptoms failing 3 months of conservative care; handlebar palsy in cyclists persisting after bike modification; hypothenar hammer syndrome with ulnar artery thrombosis and digital ischaemia; recurrent symptoms after a previous cubital tunnel release (double crush).
Active infection in the operative field; medical instability requiring optimisation; inadequate radial artery perfusion on Allen test (relative — requires vascular reconstruction if ulnar artery work is needed); severe peripheral vascular disease affecting both radial and ulnar arteries.
The decision turns on the zone and the cause. Document which zone is compressed pre-operatively (it predicts recovery) and decide whether the operation is a simple release or a release plus lesion management (ganglion excision, hook excision, or ulnar artery work). The single pre-operative test that changes the operation is the Allen test — it determines whether the ulnar artery can be safely ligated if it is diseased. Consent specifically for hypothenar numbness or a painful neuroma of the palmar cutaneous branch (the most common nerve injury, 5 to 10 percent), the rare but devastating deep motor branch injury (less than 1 percent), incomplete or delayed recovery (motor recovery is slow and may be incomplete if atrophy is severe), recurrence (5 to 10 percent), and — if arterial work is planned — a small risk of digital ischaemia. Setup. Supine with the arm on a radiolucent hand table, shoulder abducted about 90 degrees, elbow extended and forearm fully supinated. Regional anaesthesia (axillary or Bier block) is preferred, general anaesthesia if regional is contraindicated. An upper-arm pneumatic tourniquet at 250 mmHg (about 100 mmHg above systolic) with Esmarch exsanguination gives a bloodless field. Loupe magnification (×2.5 to ×3.5) is mandatory — identifying and protecting the small nerve branches and the artery is the whole game.
The Operation
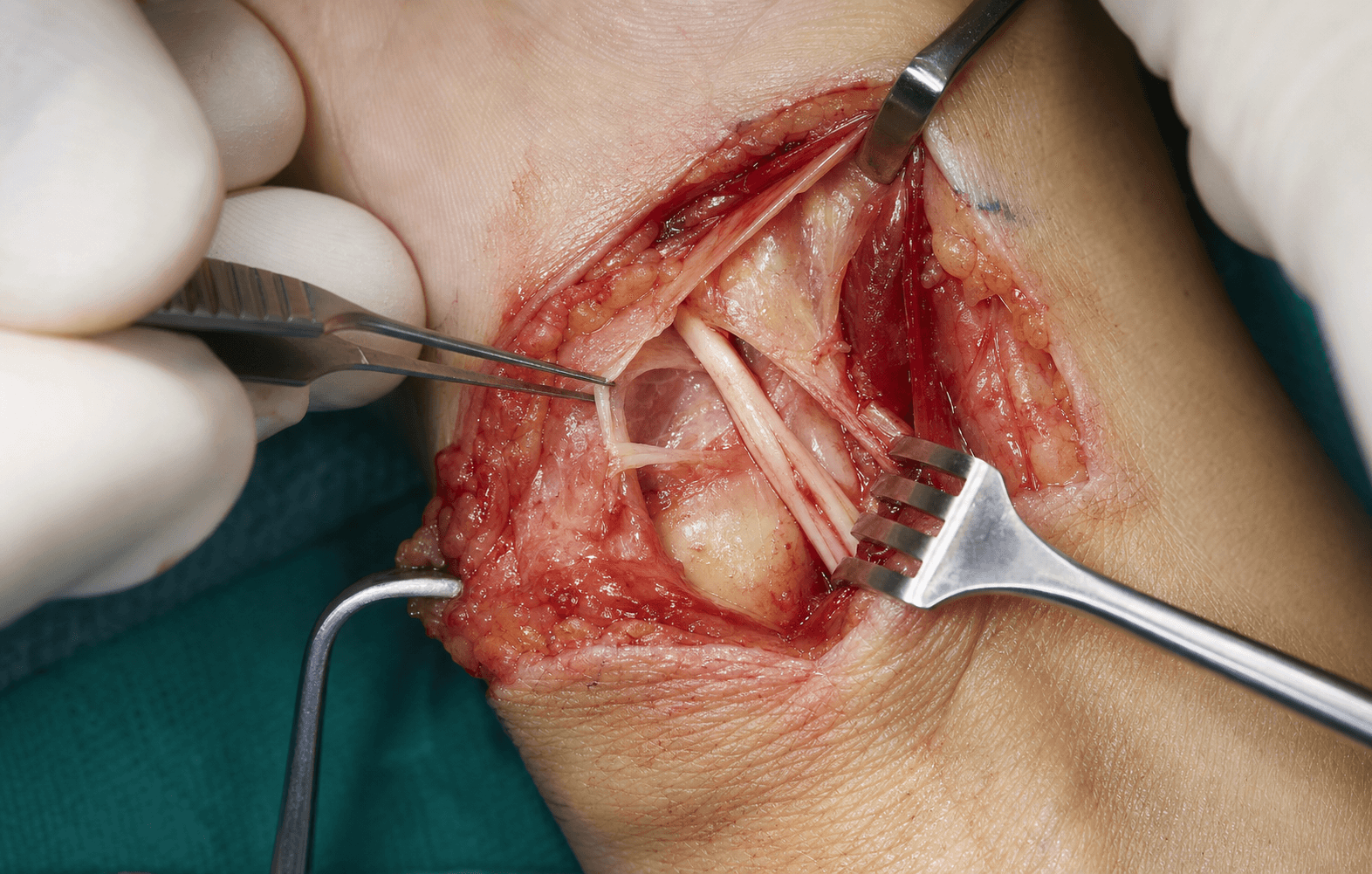
The goal: open the canal through a curvilinear ulnar-palmar incision, identify and protect the palmar cutaneous branch and the ulnar artery, divide the roof completely (proximal to distal), decompress both branches of the ulnar nerve — especially the deep motor branch around the hook of hamate — remove any compressing lesion, and close the skin only. The exposure is laid out in full below.
Operative sequence
- Supine, hand table, shoulder abducted, elbow extended, forearm fully supinated.
- Regional block (axillary or Bier) or general anaesthesia.
- Upper-arm pneumatic tourniquet at 250 mmHg (systolic plus 100), Esmarch exsanguination.
- Chlorhexidine or povidone-iodine prep from mid-forearm to fingertips; drape to expose the volar wrist and palm.
- Loupes on (×2.5 to ×3.5) before the first cut.
- A curvilinear or slightly S-shaped incision, about 4 to 5 cm long.
- Begins 2 to 3 cm proximal to the wrist crease, just ulnar to the FCU tendon.
- Runs distally along the ulnar border of the palm, curving gently palmarward at the level of the pisiform, to the mid-palm (base of the small finger metacarpal).
- The curve allows proximal extension into the forearm and distal extension as needed.
- Incise skin and subcutaneous tissue with a 15 blade, maintaining skin flaps of 2 to 3 mm to avoid necrosis.
- Identify and protect the palmar cutaneous branch of the ulnar nerve: it arises 6 to 8 cm proximal to the wrist, runs superficial to the canal, supplies the hypothenar eminence, and is the most commonly injured nerve in this procedure (5 to 10 percent in some series).
- Use loupe magnification throughout to identify this small superficial branch.
- Pisiform: the key landmark — palpable at the ulnar wrist crease, marks the proximal extent of the canal. All measurements reference this bone.
- Hook of hamate: palpate 1 cm distal and radial to the pisiform (can be hard to feel in obese patients — measure from the pisiform centre).
- FCU tendon: inserts on the pisiform, defines the ulnar border.
- Palmaris brevis: the thin transverse muscle overlying the canal roof.
- Divide the palmaris brevis longitudinally in line with the ulnar nerve.
- Identify the volar carpal ligament (the thin whitish fibrous layer forming the roof) and incise it longitudinally with fine scissors or a 15 blade, using a nerve hook to lift it off the underlying nerve.
- Extend the release at least 2 cm proximal to the pisiform into the distal forearm (the commonest site of inadequate release), and distally beyond the bifurcation.
- The ulnar nerve and artery now come into view — the nerve is superficial/radial, the artery deep/ulnar.
- Follow the ulnar nerve distally from the proximal canal.
- The bifurcation usually lies at the level of the hook of hamate (variable by 5 to 10 mm) into a superficial sensory branch (continuing distally toward the small finger) and a deep motor branch (curving radially around the hook and diving deeper).
- Document the zone of compression from this anatomy.
- The deep motor branch curves radially around the hook of hamate, accompanied by the ulnar motor artery, passing between abductor digiti minimi (ulnar) and flexor digiti minimi brevis (radial) into the deep palm.
- Release every compression point: the pisohamate arcade (fibrous band between pisiform and hook), the fibrous arch of the hypothenar muscles (origins of ADM and FDMB), any bony prominence or fracture of the hook, and any anomalous muscle.
- Trace the branch well into the palm to ensure smooth passage without kinking. Incomplete release here is the leading cause of surgical failure.
- Follow the superficial branch distally from the bifurcation toward the small finger.
- Release any fibrous bands along its course and the fascia between the hypothenar muscles.
- Ensure smooth passage without compression. It is less commonly compressed than the deep branch but must be released completely.
- Ganglion cyst (the commonest mass, usually from the pisotriquetral joint): translucent mucin-filled cyst — excise completely including the stalk to the joint, and send for histology.
- Anomalous muscle (accessory abductor digiti minimi is most common): excise if it is compressing the nerve.
- Other masses (lipoma, neurofibroma, vascular malformation): excise and send for histology.
- Indicated for a symptomatic hook fracture or non-union, a prominent hook compressing the nerve, or a clear intra-operative compression point at the hook.
- Retract the deep motor branch and ulnar motor artery gently, and retract the flexor tendons (FDP to ring and small) radially to protect them.
- Remove the hook with a small rongeur or narrow osteotome in controlled bites, flush with the hamate body; smooth any sharp edges with a burr; irrigate to remove debris; confirm by palpation that no sharp edge remains.
- Excise, do not fix: ORIF has a high non-union rate and a high nerve-injury risk.
- A pre-operative Allen test is mandatory before any ulnar artery intervention (see the callout below).
- If the Allen test is normal and the artery is thrombosed or aneurysmal: ligate proximal and distal to the diseased segment with 3-0 or 4-0 silk, excise the segment, and send for histology (confirm thrombosis, rule out vasculitis). Most patients tolerate ligation well because of the rich palmar collaterals.
- If the Allen test is abnormal: ligation risks hand ischaemia — obtain a vascular surgery opinion for reconstruction (vein graft or bypass) or stage the procedure.
- Indicated when the nerve is flattened or hourglass-shaped, or densely scarred.
- Free the nerve gently from surrounding scar using microsurgical technique and loupes, preserving the small vessels on its surface; ensure 360-degree gliding.
- Never perform internal neurolysis (epineurotomy) — it increases scarring and worsens outcomes.
- Pass a small elevator or Penfield along the entire nerve course from the proximal forearm to the bifurcation and along both branches: it should glide smoothly with no catching, kink, or band.
- Confirm the roof is fully released, both branches are free, every lesion is excised, and the nerve looks healthy.
- Release the tourniquet and achieve meticulous haemostasis with bipolar cautery (no monopolar near the nerve).
- Do not place deep sutures — deep closure risks nerve compression and haematoma accumulation; close the skin only with 4-0 or 5-0 nylon (interrupted or running subcuticular).
- Apply a soft bulky dressing; wrist in neutral, fingers left free, and no splint for an isolated Guyon's release.
- Elevate for the first 48 hours.
The palmar cutaneous branch arises 6 to 8 cm proximal to the wrist and crosses the field superficially, only 2 to 3 mm deep. Identify and protect it under loupe magnification during the superficial dissection. Injury (5 to 10 percent in some series) causes hypothenar numbness and a painful neuroma; a persistent neuroma may need excision and burial in hypothenar muscle.
The deep motor branch curves immediately around the radial side of the hook of hamate. Injury is rare (less than 1 percent) but devastating — intrinsic paralysis with a severe claw and loss of pinch, often needing tendon transfers. Protect it with gentle retraction throughout decompression, hook excision, and mass removal, and confirm it is intact and healthy before closure.
Confirm radial artery collateral flow before ligating the ulnar artery. Occlude both arteries at the wrist, exsanguinate the hand, release the radial artery only — pinkness should return within 5 seconds. If flow is delayed or absent, ligation will cause ischaemia: preserve or reconstruct the artery. Remember the Allen test has false negatives (10 to 20 percent), so monitor perfusion closely afterwards.
The commonest cause of persistent symptoms after surgery is an inadequate proximal release. Always carry the division of the roof at least 2 cm into the distal forearm, past the edge of the flexor retinaculum, and distally beyond the bifurcation.
Multiple studies show that opening the epineurium (internal neurolysis / epineurotomy) adds scarring and worsens outcomes. Only external neurolysis — freeing the nerve from surrounding adhesions — is indicated. This principle is consistent across all nerve decompressions.
Do not close the deep tissues and do not splint an isolated Guyon's release. Deep sutures risk nerve compression and haematoma, and immobilisation breeds adhesions and CRPS. Start finger range-of-motion exercises immediately.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | 0 to 3 days | Bulky dressing, wrist neutral, fingers free, no splint | Elevation and ice; immediate finger ROM | | 2 | 3 to 14 days | Lighter dressing from day 2 to 3 | Finger ROM hourly while awake, gentle wrist ROM; sutures out at 10 to 14 days | | 3 | 2 to 6 weeks | None | Scar massage, progressive wrist and grip strengthening; return to light work at 2 to 3 weeks; avoid repetitive palm impact | | 4 | 6 weeks to 6 months | None | Heavy work at 6 to 8 weeks, sport at 8 to 12 weeks, full grip strength around 3 months; cyclists avoid handlebars for 6 to 8 weeks | Sensory symptoms recover first (weeks to months); motor recovery is slower (3 to 6 months) and depends on the severity of pre-operative atrophy — if wasting was severe, some deficit may be permanent despite an adequate decompression. Around 80 to 90 percent report good to excellent results, with sensory recovery in 85 to 95 percent and useful motor recovery in 70 to 85 percent; about 90 percent return to their previous occupation.
- Recognition
- Hypothenar numbness, painful neuroma, Tinel sign at the incision
- Prevention
- Loupe magnification, identify the nerve early, adequate skin flap thickness
- Management
- Desensitisation, gabapentin; neuroma excision and burial if conservative care fails at 6 months
- Recognition
- Immediate intrinsic paralysis, positive Froment and Wartenberg signs, severe claw
- Prevention
- Microsurgical technique, loupes, gentle handling, protect during hook excision
- Management
- Immediate re-exploration and repair if transected; nerve grafting or tendon transfers (EIP to first DI, ECRL to ADM) for permanent deficit
- Recognition
- Persistent symptoms, no improvement, positive EMG/NCS
- Prevention
- Systematic release of all points, adequate proximal and distal release, remove all masses, elevator test
- Management
- Conservative care for 3 to 6 months, repeat EMG, revision surgery if symptoms persist
- Recognition
- Small finger and ulnar ring finger palmar numbness, painful neuroma if transected
- Prevention
- Identify at the bifurcation, protect during distal release, avoid excessive retraction
- Management
- Neuropraxia: observe; transection: early repair, or grafting if delayed
- Recognition
- Intraoperative bleeding, haematoma, hand ischaemia
- Prevention
- Gentle dissection, identify the artery early, bipolar only, confirm Allen test
- Management
- Pressure and ligation if Allen test normal and repair not possible; vascular consult if abnormal
- Recognition
- Increasing pain, tense swelling, ecchymosis, decreased ROM
- Prevention
- Meticulous haemostasis, no deep closure, bulky dressing, elevation
- Management
- Small: observe, ice, elevation; large or expanding: return to theatre for evacuation
- Recognition
- Pain, erythema, warmth, purulent drainage, fever
- Prevention
- Cefazolin 2 g IV prophylaxis, sterile technique, haemostasis
- Management
- Superficial: oral antibiotics; deep: IV antibiotics and debridement
- Recognition
- Disproportionate pain, allodynia, colour and temperature change, stiffness
- Prevention
- Early mobilisation, vitamin C 500 mg daily perioperatively, avoid immobilisation
- Management
- Hand therapy, gabapentin, sympathetic blocks
- Recognition
- Return of symptoms after initial improvement
- Prevention
- Complete initial decompression, remove all masses, activity modification
- Management
- EMG/MRI, conservative care, revision if a structural cause is found
- Recognition
- Decreased wrist and finger ROM, nerve tethering, painful scar
- Prevention
- Early ROM, no immobilisation, skin-only closure, scar massage
- Management
- Hand therapy, silicone sheeting, revision neurolysis if severe
- Recognition
- Loss of DIP flexion of ring or small finger, triggering
- Prevention
- Visualise during hook excision, retract tendons radially
- Management
- Primary repair if recognised intra-operatively; transfer or graft for attrition rupture
- Recognition
- Persistent intrinsic weakness, incomplete recovery of Froment or Wartenberg signs
- Prevention
- Operate before severe atrophy, set realistic expectations
- Management
- Hand therapy and functional training; tendon transfers if deficit is stable at 12 months
Viva & Exam Focus
GUYONGUYON — anatomic boundaries of the canal
HAMMERHAMMER — hypothenar hammer syndrome features
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old mechanic presents with 6 months of progressive right hand weakness and small finger numbness. Examination shows hypothenar and interosseous atrophy, positive Froment and Wartenberg signs, and numbness isolated to the palmar aspect of the small and ulnar ring fingers. Dorsal ulnar hand sensation is normal. EMG shows denervation in FDI and ADM but a normal FDP to the small finger. Where is the compression, and what are the three zones of Guyon's canal?”
“You are decompressing the ulnar nerve at Guyon's canal and encounter a 2 cm firm, slightly pulsatile mass compressing the nerve just distal to the pisiform. Describe your management and the critical considerations.”
“During Guyon's canal release you need to excise a fractured hook of hamate. Describe your technique and the critical anatomical relationships you must protect.”
Essential anatomy
- 4 cm fibro-osseous tunnel. Roof = palmaris brevis + volar carpal ligament. Floor = flexor retinaculum + pisohamate ligament. Ulnar wall = pisiform. Radial wall = hook of hamate
- Contents: ulnar nerve (bifurcates into superficial sensory and deep motor branches) and ulnar artery
- Deep motor branch curves around the hook of hamate and supplies all intrinsics except the thenar muscles and lateral two lumbricals — injury is devastating
- Palmar cutaneous branch arises 6 to 8 cm proximal to the wrist, runs superficial to the canal, and is the most commonly injured nerve (5 to 10 percent)
Three-zone classification
- Zone 1 (proximal to bifurcation): mixed motor and sensory. Causes: ganglion, ulnar artery aneurysm, fracture-dislocation
- Zone 2 (deep motor): pure motor deficit with normal sensation — the commonest surgical zone (40 to 50 percent). Causes: hook of hamate fracture, ganglion, pisohamate arcade
- Zone 3 (superficial sensory): pure sensory deficit with normal motor — least common (10 to 20 percent)
- Dorsal ulnar hand sensation is spared (dorsal cutaneous branch arises proximal to the wrist) — this distinguishes Guyon's from cubital tunnel
Key indications
- Progressive motor weakness with intrinsic atrophy despite 3 to 6 months of conservative care
- Space-occupying lesion: ganglion, ulnar artery thrombosis or aneurysm, hook of hamate fracture
- Hypothenar hammer syndrome: repetitive palm trauma damaging the ulnar artery
- Handlebar palsy in cyclists persisting after bike modification
- EMG/NCS localising to the wrist: denervation in ulnar intrinsics with normal FDP and FCU
Critical surgical steps
- Curvilinear incision along the ulnar palm from 2 cm proximal to the pisiform to mid-palm; protect the palmar cutaneous branch
- Divide palmaris brevis and the volar carpal ligament; extend the release 2 cm proximal to the pisiform and distal beyond the bifurcation
- Decompress the deep motor branch fully: pisohamate arcade, hypothenar arch, hook pathology
- Manage masses: ganglion (complete excision with stalk), hook fracture (excise, do not fix), ulnar artery (ligate if Allen test normal)
- Skin-only closure, no splint, immediate finger ROM
Danger zones
- Palmar cutaneous branch: superficial to the canal, most commonly injured (5 to 10 percent)
- Deep motor branch: around the hook of hamate; injury causes intrinsic paralysis (less than 1 percent but devastating)
- Ulnar artery: adjacent to the nerve throughout; Allen test mandatory before ligation
- Flexor tendons: FDP to ring and small fingers runs radially adjacent to the hook — at risk during excision
- Superficial sensory branch: injury (2 to 5 percent) causes small finger numbness
Hook of hamate management
- Excision preferred over ORIF: better outcomes, faster return to sport (6 to 8 weeks versus 12 to 16 weeks)
- ORIF problems: poor healing, high non-union rate (30 to 40 percent), hardware complications, nerve-injury risk
- Technique: remove flush with the body, smooth edges, protect the deep motor branch, retract the flexor tendons radially
- Common in golfers, baseball batters, and racquet-sport players, usually as a painful non-union
Hypothenar hammer syndrome
- Allen test mandatory before any ulnar artery intervention
- Normal Allen test (under 5 seconds): safe to ligate; 90 percent tolerate well, but 10 percent still develop ischaemia
- Abnormal Allen test: ligation risks ischaemia — vascular reconstruction or a staged procedure
- If Allen normal: ligate and excise the diseased segment and send for histology
- Occupational: mechanics, carpenters, baseball catchers — workplace modification is crucial to prevent recurrence
Complications and outcomes
- Most common: palmar cutaneous branch injury (5 to 10 percent)
- Most devastating: deep motor branch injury (less than 1 percent), needing tendon transfers
- Incomplete decompression (10 to 15 percent) is the commonest cause of failure — prevent with systematic release and the elevator test
- Success: 80 to 90 percent good to excellent; sensory recovery 85 to 95 percent; motor recovery 70 to 85 percent
- Good prognosis: short duration, minimal atrophy, an identifiable mass removed. Poor: chronic severe compression, marked atrophy, double crush
Background & Evidence
Epidemiology. Ulnar nerve compression at the wrist is far less common than carpal tunnel syndrome or cubital tunnel syndrome. It is strongly associated with occupational and recreational palmar trauma — mechanics, carpenters, baseball catchers, martial artists and cyclists (handlebar palsy) — and with repetitive gripping against the hypothenar eminence. Hypothenar hammer syndrome and hook of hamate fractures share the same mechanism: the ulnar artery and nerve compressed against the hook of hamate. Canal anatomy. Guyon's canal is a roughly 4 cm fibro-osseous tunnel running from just proximal to the pisiform to the fibrous arch of the hypothenar muscles.
- Structures
- Palmaris brevis muscle and the volar (palmar) carpal ligament
- Structures
- Flexor retinaculum (transverse carpal ligament, separating it from the carpal tunnel) and the pisohamate ligament
- Structures
- The pisiform (palpable at the ulnar wrist crease)
- Structures
- The hook of hamate (1 cm distal and radial to the pisiform)
- Structures
- The ulnar nerve (bifurcates within the canal) and the ulnar artery (bifurcates with it), in loose areolar tissue
Nerve anatomy within the canal. Proximally the mixed ulnar nerve carries both motor and sensory fibres. It bifurcates — usually at the level of the hook of hamate (variable by 5 to 10 mm) — into a superficial sensory branch (pure sensory, supplying the small finger and ulnar half of the ring finger, running distally under the hypothenar muscles) and a deep motor branch (pure motor, curving radially around the hook of hamate with the ulnar motor artery, passing between abductor digiti minimi and flexor digiti minimi brevis, crossing the palm deep to the flexor tendons, and supplying all intrinsic muscles except the thenar muscles and the lateral two lumbricals). The dorsal cutaneous branch and the palmar cutaneous branch both arise proximal to the canal, so dorsal hand sensation and hypothenar sensation are spared in a pure canal lesion.
- Branch
- Mixed (proximal to bifurcation)
- Clinical deficit
- Both motor and sensory deficit
- Typical causes
- Ganglion, ulnar artery aneurysm, fracture-dislocation
- Branch
- Deep motor branch
- Clinical deficit
- Pure motor deficit — intrinsic atrophy, weak pinch, claw, normal sensation (the commonest surgical zone, 40 to 50 percent)
- Typical causes
- Hook of hamate fracture, ganglion, pisohamate arcade, anomalous muscle
- Branch
- Superficial sensory branch
- Clinical deficit
- Pure sensory deficit — small finger and ulnar ring numbness, normal motor (least common, 10 to 20 percent)
- Typical causes
- Ganglion, direct trauma
- Key features
- The most common mass (around 50 percent of cases with a mass); usually from the pisotriquetral joint; T2-bright on MRI
- Management
- Complete excision including the stalk; recurrence is 5 to 10 percent after complete excision
- Key features
- Repetitive palm trauma (mechanics, catchers, martial artists); ulnar artery thrombosis or aneurysm; digital ischaemia and Raynaud-like change
- Management
- Allen test first; resect and ligate if normal, reconstruct with vein graft if abnormal
- Key features
- Racquet and bat sports; volar-ulnar pain and weakened grip; CT is the gold standard; usually a painful non-union; may cause FDP attrition
- Management
- Excise the hook (not ORIF); about 95 percent satisfaction and return to sport at 6 to 8 weeks
- Key features
- Accessory abductor digiti minimi most common; a fibrous arch compresses the deep motor branch
- Management
- Release or excise if it is compressing the nerve
- Key features
- Cyclists; chronic external compression of the nerve against the hook
- Management
- Modify the bike, padded gloves; release if symptoms persist
Clinical presentation. Motor findings (deep motor branch) are intrinsic weakness, hypothenar and interosseous atrophy, a positive Froment sign (thumb IP flexion on key pinch from weak adductor pollicis with compensatory FPL), a positive Wartenberg sign (small finger abduction from weak palmar interosseous with unopposed EDM), and clawing of the ring and small fingers in severe cases. Sensory findings (superficial branch) are numbness of the palmar small finger and ulnar ring finger only — the dorsal ulnar hand is spared (dorsal cutaneous branch arises proximal to the wrist). Vascular findings (hypothenar hammer) are cold sensitivity, digital pallor or cyanosis, Raynaud-like change, and a pulsatile mass if an aneurysm. A Tinel sign at the canal and a pressure-provocative test support the diagnosis. Investigations. EMG/NCS is the key test: prolonged distal motor latency, abnormal sensory conduction (unless the lesion is an isolated Zone 2, where sensory studies are normal — a key discriminator), and needle EMG showing denervation in the ulnar intrinsics (FDI, ADM, interossei) with a normal FDP and FCU, which localises the lesion to the wrist rather than the elbow. Imaging: a carpal tunnel view X-ray for a hook of hamate fracture, CT as the gold standard for hook pathology, MRI for soft-tissue masses and denervation change, ultrasound for dynamic assessment and arterial disease, and CT or digital-subtraction angiography for hypothenar hammer syndrome. The Allen test is mandatory before any ulnar artery intervention. Outcomes. Good to excellent results are reported in 80 to 90 percent, with sensory recovery in 85 to 95 percent (faster, over weeks to months) and useful motor recovery in 70 to 85 percent (slower, over 3 to 6 months); about 90 percent return to their previous occupation. Good prognostic factors are a short symptom duration (under 6 months — the strongest predictor), minimal pre-operative atrophy, an identifiable and removable mass, complete decompression, pure sensory symptoms (Zone 3) and younger age. Poor prognostic factors are chronic severe compression (over 12 months), severe intrinsic atrophy, a double crush (cubital tunnel plus Guyon's canal), incomplete initial decompression, significant comorbidity (diabetes, vascular disease), and workers' compensation claims. Guidelines, registries and global practice. No single national framework governs this operation — ulnar tunnel decompression is described consistently across hand-surgery teaching worldwide (ASSH, BSSH/FESSH, IFSSH), and the core principles (complete canal release, address the space-occupying cause, skin-only closure) are universal across the advanced orthopaedic practice (Tr and Orth), advanced orthopaedic practice, EBHS/FESSH, advanced orthopaedic practice and DNB/MS curricula. No implant registry applies, because this is a soft-tissue decompression without an implant, so evidence comes from case series and reviews rather than NJR, AJRR, AOANJRR or SHAR data. For hook of hamate fractures, international consensus favours excision over ORIF for symptomatic fractures and non-unions because of the tenuous blood supply, the deforming pull of attached muscles, the high non-union rate after fixation, and the proximity of the deep motor branch. For hypothenar hammer syndrome, practice varies globally by perfusion status: with a normal Allen test most surgeons resect and ligate the diseased segment, while with an abnormal Allen test vein-graft reconstruction is preferred. Smoking cessation, cold avoidance, and ergonomic and occupational modification are universally recommended to prevent recurrence.
References
Ulnar-nerve compression syndromes at and below the wrist
- Original three-zone classification of ulnar nerve compression in Guyon's canal still used worldwide
- Zone 1 (proximal to bifurcation) produces combined motor and sensory deficit
- Zone 2 (deep motor branch) produces isolated motor deficit; Zone 3 (superficial branch) produces isolated sensory deficit
- Anatomic localisation of compression predicts the clinical syndrome and guides operative exposure
Ulnar tunnel syndrome
- Presentation varies by zone: Zone I motor and sensory, Zone II isolated motor, Zone III isolated sensory
- Guyon's canal anatomy is complex and variable, with multiple space-occupying causes (ganglion most common)
- Activity modification and splinting may help, but surgical exploration is indicated for a space-occupying lesion or progressive deficit
- Complete release of the canal roof and all fibrous arcades is essential to avoid persistent symptoms
Outcomes of hook of hamate fracture excision in high-level amateur athletes
- 12 cases of hook of hamate excision in high-level amateur athletes
- All patients returned to full sport at a mean of 6 weeks after surgery
- Mean postoperative DASH score under 1; all scored 0 on the DASH Sports module with no loss of performance
- Only complication was transient ulnar nerve paraesthesia that resolved fully by 6 weeks
Hook of Hamate Fractures
- Contemporary review: excision of the hook has been adopted by most hand surgeons
- Classic presentation is volar-ulnar pain, grip weakness and possible ulnar nerve paraesthesia
- Good outcomes with high satisfaction are expected once diagnosis is made and treatment delivered
- Treatment choice is shaped by activity level and desired return to work or sport
Hypothenar Hammer Syndrome: Long-Term Results After Vascular Reconstruction
- 12 patients treated for hypothenar hammer syndrome with resection and vascular reconstruction (end-to-end or reverse vein graft)
- 9 of 12 reconstructions remained patent at a mean follow-up of 4.7 years (75 percent patency)
- Patients with a patent reconstruction had relief of pain, dysaesthesia and cold intolerance
- Surgical intervention is a good option after failed non-operative treatment
Anatomic study of variations of hypothenar muscles and arborization patterns of the ulnar nerve in the hand
Detailed anatomical study of ulnar nerve branching patterns and hypothenar muscle variations, with implications for surgical decompression of Guyon's canal.
Anatomy of Guyon's canal — a systematic review
Systematic review of Guyon's canal anatomy, including boundaries, contents, dimensions and anatomical variations relevant to compression syndromes.
Anatomical variations as potential risk factors for ulnar tunnel syndrome: a cadaveric study
Cadaveric study identifying anatomical risk factors for ulnar tunnel syndrome, including anomalous muscles, fibrous bands and vascular variations.
Peripheral neuropathies of the median, radial, and ulnar nerves: MR imaging features
Review of MRI findings in peripheral nerve compression syndromes including Guyon's canal, with imaging pearls for diagnosis.
Ulnar Nerve Compression in Guyon's Canal by Ganglion Cyst
Report of a ganglion cyst causing ulnar nerve compression in Guyon's canal, emphasising early decompression with cyst removal for complete recovery.
The epidemiology of upper extremity fractures in the United States, 2009
Epidemiological study of upper extremity fractures including hook of hamate fractures — incidence, demographics and treatment patterns in the US population.
Symposium: upper extremity nerve compression syndromes
Symposium review of upper extremity nerve compressions, including a detailed surgical technique for Guyon's canal decompression and outcome predictors.