Pathologic genu varum | Medial physeal growth disturbance | Infantile vs adolescent forms
- Differentiation from physiologic genu varum: Physiologic resolves by age 2-3 years, bilateral, MDA under 11 degrees, no radiographic metaphyseal changes
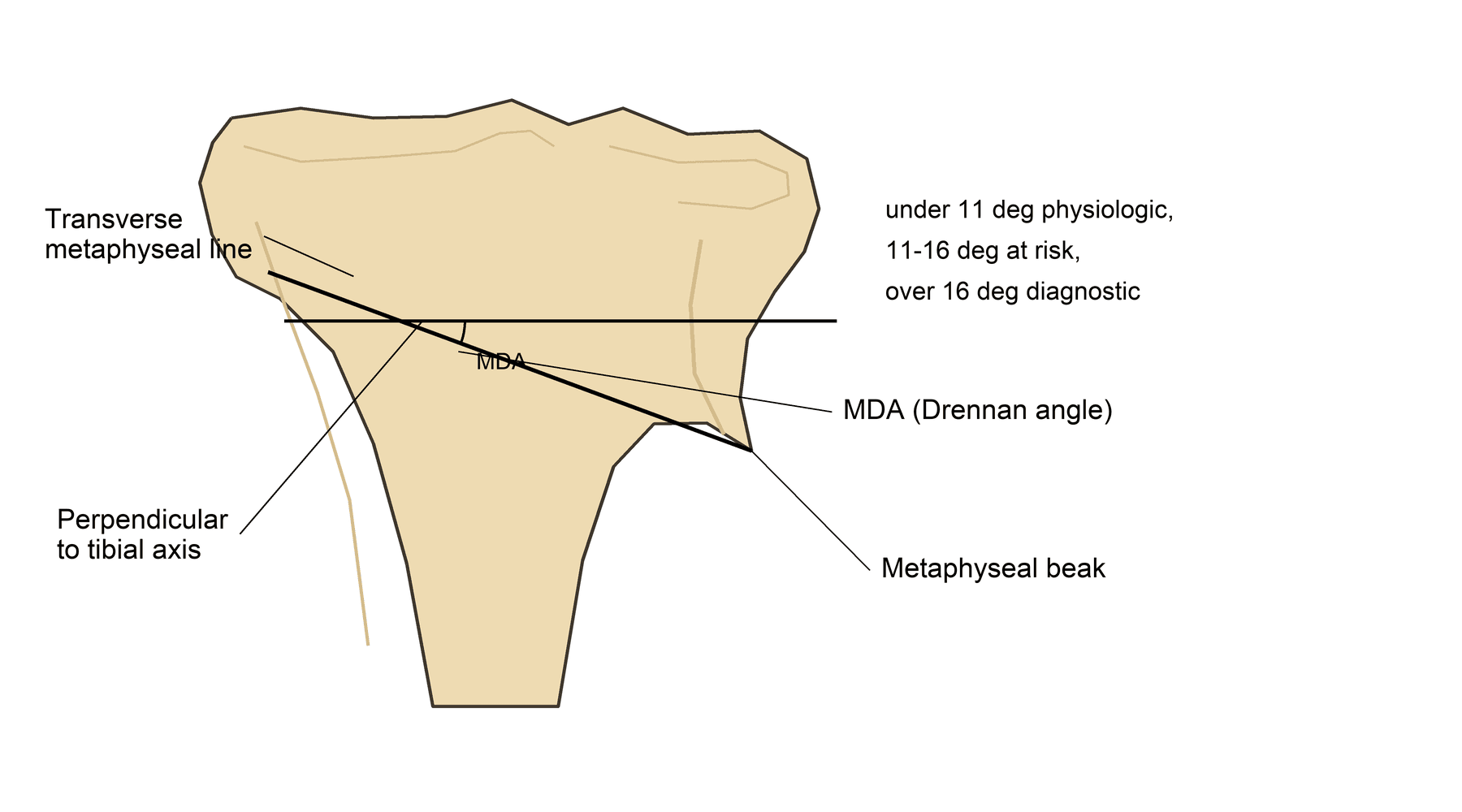
- Critical imaging measurement: Metaphyseal-diaphyseal angle (Drennan) measured on standing AP radiograph - over 11 degrees predicts progression, over 16 degrees diagnostic
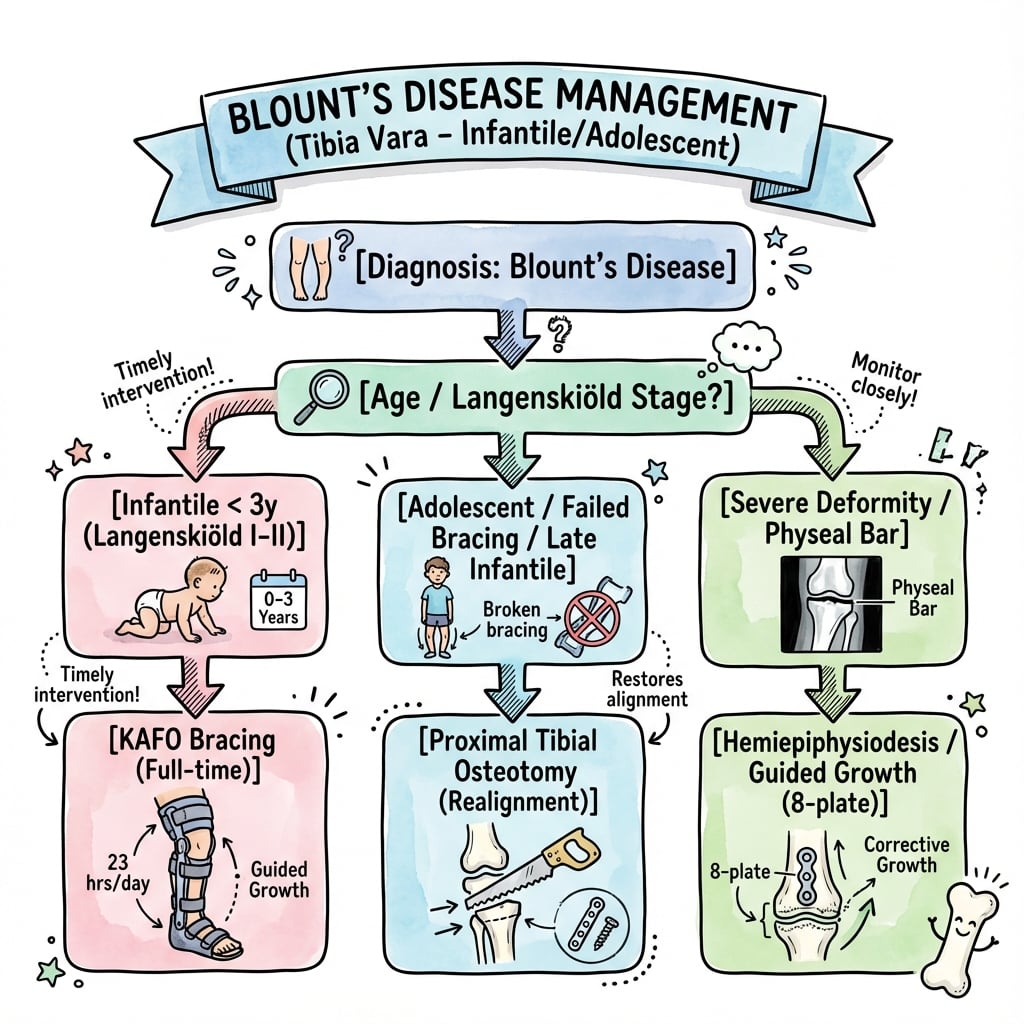
- Two distinct forms: Infantile (under 4 years, often bilateral, better bracing response) vs adolescent (over 8 years, unilateral, obesity-related, poor bracing response)
- Bracing window: Most effective for Stage I-II infantile disease in children aged 1-3 years, requires KAFO (knee-ankle-foot orthosis) worn 23 hours daily for 1-2 years
- Surgical timing: Osteotomy preferred before age 4 years (better remodeling); recurrence risk falls sharply after age 5; adolescent form requires osteotomy at presentation
- “Langenskiöld Stage IV or higher = surgery required
- “MDA over 16 degrees = pathologic, will not resolve spontaneously
- “Beware combined femoral and tibial deformity in severe cases
- “Physeal bar develops in neglected cases - Stage VI disease
Physiologic Genu Varum: Bilateral, resolves by age 2-3. MDA less than 11°. No metaphyseal changes.
Rickets: Widened physis, biochemical abnormalities. FFCD: Unilateral, abrupt angulation. Dysplasia: Multiple joints, short stature.
Drennan's Angle (MDA): The single most important measurement. Langenskiöld Staging: Determines treatment.
Overview and Epidemiology
Blount disease (tibia vara) is a pathologic growth disturbance of the medial aspect of the proximal tibial physis, resulting in progressive genu varum deformity. It represents a failure of normal endochondral ossification at the medial metaphysis.
Two distinct clinical entities:
-
Infantile form (most common):
- Onset before age 4 years
- Often bilateral (60-80%)
- More common in early walkers
- Higher prevalence in children of African and Hispanic descent
- Better response to conservative management
-
Adolescent form:
- Onset after age 8-10 years
- Usually unilateral (80%)
- Strong association with obesity
- Less predictable, worse prognosis
- Requires surgical management
Global epidemiology:
- Prevalence varies markedly by population - higher in populations of African and Afro-Caribbean descent and in regions where early walking is common
- Relatively rare in Northern European/Caucasian populations
- Incidence rising worldwide in parallel with the childhood obesity epidemic, especially the adolescent (late-onset) form
- Male predominance (approximately 3:1)
Risk factors:
- Early walking (before 10 months)
- Obesity (especially adolescent form; BMI is an independent predictor of being listed for surgery)
- African or Hispanic descent
- Vitamin D deficiency (controversial)
- Mechanical stress on the immature medial physis
The condition is progressive if untreated, leading to permanent deformity, lateral thrust gait, medial compartment osteoarthritis, and functional disability.
INFANTINFANT - Infantile Blount Disease Features
Hook:INFANT Blount - remember these key features of the infantile form to distinguish from physiologic bowing and guide an appropriate bracing trial.
Pathophysiology
Normal proximal tibial growth:
- Proximal tibial physis contributes 55-60% of tibial growth
- Medial and lateral physeal growth should be symmetric (approximately 6mm per year overall)
- Peak growth velocity in infancy and early adolescence
Normal lower limb alignment evolution:
- Birth: 10-15 degrees varus (physiologic)
- Age 12-18 months: neutral mechanical axis
- Age 2-4 years: 10-12 degrees valgus (physiologic)
- Age 6-7 years: 5-7 degrees valgus (adult alignment)
Mechanical axis: A line from the femoral head centre to the ankle centre normally passes through (or just lateral to) the medial tibial spine. In Blount disease it passes medial to the knee, overloading the medial compartment.
Hueter-Volkmann principle (the central mechanism):
- Increased compression → decreased growth; decreased compression → increased growth
- Medial physeal compression from mechanical overload suppresses medial growth
- This creates a vicious cycle: varus → increased medial stress → more varus
Histologic findings:
- Disorganized physeal architecture (loss of columnar arrangement)
- Fibrocartilaginous tissue replacing normal physeal cartilage
- Thickened periosteum medially
- Metaphyseal cartilage islands (failure of resorption)
- Progressive changes from Stage I to Stage VI
Mechanical contributing factors:
- Early walking increases medial compartment stress
- Obesity dramatically increases joint reaction forces
- Internal tibial torsion increases the frontal-plane moment arm, producing asymmetric loading of the medial physis
Progressive deformity components:
- Varus angulation (primary deformity)
- Internal tibial torsion (60-80% of cases)
- Procurvatum (anterior bowing) in advanced cases
- Medial physeal bar formation (Stage VI)
- Leg length discrepancy (asymmetric growth)
BLOUNTBLOUNT - Key Pathophysiology Features
Hook:Remember BLOUNT when you see a child with progressive genu varum - think about the Loading forces causing Bowing in Obese children.
Classification
The Langenskiöld classification (1952, revised 1964) describes six progressive stages of infantile Blount disease based on the radiographic appearance of the proximal medial tibial metaphysis and epiphysis. It is the gold standard classification used worldwide.
Critical for surgical decision-making: Stages I-III may respond to bracing; Stages IV-VI require surgery.

Beak vs Defect: Stage II has a clear metaphyseal depression/defect.
The Beak: Stage IV shows metaphyseal overgrowth projecting beneath the epiphysis.
The Bridge: Stage VI shows a medial physeal bar (bony bridge).
Treatment: Stages I-III = Brace (if under 3y). Stages IV-VI = Surgery.
MEDIALMEDIAL - Langenskiöld Progressive Stages
Hook:The MEDIAL progression tracks increasing severity - from Mild beaking to a Locked physeal bar. Stage IV is when surgery becomes mandatory.
The Depressed Medial Plateau (Intra-Articular Deformity)
In advanced infantile and adolescent disease the deformity is not only metaphyseal. The medial tibial plateau becomes depressed - the medial joint surface slopes downward medially, producing joint-line obliquity and medial articular incongruity (the LaMont type C "vertical down-sloping epiphysis and metaphysis" carries the worst prognosis). Recognising this second, intra-articular level of deformity is critical because a standard metaphyseal osteotomy does not address it.
Two Levels of Deformity in Severe Blount Disease
Severe (advanced infantile and adolescent) Blount disease has TWO levels of deformity: metaphyseal varus AND an intra-articular depressed medial tibial plateau (a downsloping medial joint surface with joint-line obliquity - the LaMont type C lesion). A standard metaphyseal valgus osteotomy corrects the metaphyseal varus but leaves a depressed medial plateau untouched, so the limb can look aligned yet the joint stays incongruent and the lateral thrust persists - a setup for recurrence and early medial osteoarthritis. When the medial plateau is significantly depressed (typically the older child, over 7 years, with advanced disease), add a medial plateau (hemiplateau) elevation osteotomy combined with a metaphyseal osteotomy and a lateral hemiepiphysiodesis to restore joint congruity.
Clinical Presentation
Presenting complaint:
- Parents notice bowed legs that are not improving or are worsening
- Abnormal gait (waddling, lateral thrust)
- Knee or leg pain in older children (uncommon in infantile form)
- Concerns about shoe wear (lateral sole wear)
Age at presentation:
- Infantile form: typically 18 months to 3 years (after walking established)
- Adolescent form: 8-15 years (often coincides with growth spurt)
Key history questions:
- Age of first walking (under 10 months = risk factor)
- Birth weight and current weight (obesity assessment)
- Unilateral vs bilateral deformity
- Progressive or static deformity
- Family history of bowed legs or metabolic bone disease
- Dietary history (vitamin D, calcium intake)
- Previous bracing or treatment
Red flags for an alternative diagnosis:
- Short stature (consider skeletal dysplasia)
- Other joint involvement (consider skeletal dysplasia)
- Pathologic fractures (consider rickets or metabolic disease)
- Developmental delay (consider genetic syndrome)
Physical Examination
Gait assessment (most important):
- Lateral thrust gait: dynamic varus thrust during stance phase, indicating functional medial compartment insufficiency and predicting progression
- Waddling gait if bilateral; reduced cadence and stride length
Standing alignment:
- Intercondylar distance: measure between medial femoral condyles with ankles together (normal under 6 cm in young children; over 6-8 cm suggests pathologic bowing)
- Assess asymmetry if unilateral (compare knee heights)
Rotational profile:
- Internal tibial torsion: thigh-foot angle (normally 10 degrees external) - present in 60-80% of cases
- Femoral version: check internal rotation in the prone position
Other examination:
- Varus stress test: increased medial gapping suggests LCL laxity; fixed varus = bony deformity (advanced disease)
- Leg length (true: ASIS to medial malleolus)
- Knee ROM and ligament stability
- Neurovascular status and exclusion of neuromuscular disorder
- General exam: BMI/obesity assessment, height/weight percentiles, signs of rickets (widened wrists, costochondral beading) or skeletal dysplasia
THRUSTTHRUST - Key Clinical Examination Findings
Hook:Watch for the lateral THRUST gait - the most important dynamic clinical sign that predicts progression and the need for intervention.
Investigations
Standing anteroposterior (AP) radiograph - gold standard:
- Must be weight-bearing for accurate alignment; include both knees for comparison
- Key measurements: MDA (Drennan), tibiofemoral angle, intercondylar distance
- Langenskiöld staging based on medial metaphyseal changes
- Look for: medial beaking, metaphyseal defect, physis widening, epiphyseal wedging
Standing long-leg radiograph (full-length):
- Mechanical axis alignment - line from femoral head to ankle; obtain when planning surgery
- Identifies femoral vs tibial contribution to deformity and measures true leg length discrepancy
- Mechanical axis deviation (MAD): distance from knee centre to the mechanical axis
Lateral radiograph: assess for procurvatum (anterior bowing) and tibial slope - useful for surgical planning.
Follow-up imaging schedule:
- Initial diagnosis: standing AP both knees
- Under 3 years with Stage I-II on bracing: repeat every 3-4 months
- Observation: every 6 months until skeletal maturity
- Post-operative: immediate, 6 weeks, 3 months, then every 6 months
IMAGESIMAGES - Essential Radiographic Assessment
Hook:Get your IMAGES right - standing AP radiographs with MDA measurement and Langenskiöld staging are essential for diagnosis and management decisions.
A Triplanar Deformity: Don't Forget Procurvatum
Blount disease is not a pure coronal-plane problem. Alongside the varus (coronal) and internal tibial torsion (axial, in 60-80%), advanced and adolescent cases - particularly in heavier children - develop procurvatum: apex-anterior bowing of the proximal tibia with an increased posterior tibial slope. It is easy to miss because the AP radiograph does not show it - it must be sought on the lateral standing film.
The Three Planes of Blount Deformity
Do not treat Blount disease as a pure frontal-plane problem. Alongside varus (coronal) and internal tibial torsion (axial, 60-80%), advanced and adolescent cases - especially heavier children, where procurvatum correlates with BMI in early-onset disease - develop procurvatum: apex-anterior bowing of the proximal tibia with increased posterior tibial slope. It is easily missed because the AP film does not show it; you must look at the LATERAL standing radiograph. A purely frontal-plane valgus osteotomy that ignores procurvatum leaves residual sagittal malalignment, so significant procurvatum calls for a multiplanar correction (a dome osteotomy or a circular frame) that addresses varus, torsion and procurvatum together.
Differential Diagnosis
The examiner will expect you to differentiate Blount disease from other causes of genu varum in children.
Blount Disease vs Key Differentials
DIFFERDIFFER - Differential Diagnosis Approach
Hook:Think DIFFER when faced with genu varum - systematically rule out physiologic bowing, rickets, and FFCD before confirming Blount disease.
Q: How do you differentiate physiologic genu varum from infantile Blount disease?
A: Key discriminators:
- Age: physiologic improves after age 2, Blount worsens
- MDA (Drennan angle): under 11 degrees = physiologic, over 16 degrees = Blount
- Metaphyseal changes: absent in physiologic, beaking/depression in Blount
- Progression: physiologic resolves spontaneously, Blount progresses
- Langenskiöld staging: specific radiographic stages only in Blount disease
The MDA over 16 degrees is the most reliable single predictor of Blount disease.
Management
- Under 2 years with MDA under 11 degrees → observe (likely physiologic)
- Under 3 years with MDA 11-16 degrees, Stage I-II → bracing trial
- Age 3-4 years → bracing only if compliant, lower success
- Over 4 years → surgery (bracing ineffective)
- Adolescent (over 8 years) → surgery required
- Stage I-II → bracing may succeed if young (under 3 years)
- Stage III → borderline, may attempt bracing only if very young
- Stage IV or higher → surgery mandatory
- MDA decreasing → continue 12-24 months
- No response by 6-12 months, or progression → convert to surgery
- Young child (under 5 years), moderate deformity → osteotomy +/- external fixator
- Child 5-10 years with growth remaining and moderate deformity → consider guided growth (tension band plate)
- Adolescent or severe deformity → proximal tibial valgus osteotomy
- Langenskiöld Stage
- Any
- MDA
- Under 11°
- Treatment
- Observe
- Langenskiöld Stage
- I-II
- MDA
- 11-16°
- Treatment
- Bracing trial
- Langenskiöld Stage
- I-III
- MDA
- Any
- Treatment
- Bracing with caution
- Langenskiöld Stage
- Any
- MDA
- Any
- Treatment
- Surgery
- Langenskiöld Stage
- Any
- MDA
- Any
- Treatment
- Surgery
Key points: age under 3 years is critical for bracing success; Stage IV or higher = surgery regardless of age; MDA over 16° = diagnostic; overcorrect to 5-10° valgus to prevent recurrence.

Surgical Pitfall - Peroneal Nerve Injury
The common peroneal nerve is at significant risk during proximal tibial osteotomy:
- It courses around the fibular neck, close to the surgical site
- Risk is highest with lateral closing wedge osteotomy, proximal fibular osteotomy, and excessive acute lengthening or stretch
Prevention: know the anatomy (the nerve lies posterior to the biceps femoris tendon, anterior to the lateral gastrocnemius); avoid excessive lateral dissection; perform fibular osteotomy mid-shaft (or protect the nerve if proximal); limit acute lengthening to under 10-15mm; consider an external fixator for gradual correction if risk is high.
If injury occurs: usually a neurapraxia that recovers over 3-6 months. Document baseline neuro exam pre-op and immediately post-op, and apply an AFO for foot-drop.
- Langenskiöld stage II disease (aged 30-40 months) failing bracing, treated with valgus osteotomy
- Recurrence 28.6% (4/14 legs) without overcorrection (FTA 7-13 degrees) vs 12.5% (6/48 legs) with overcorrection (FTA over 13 degrees)
- Difference did not reach statistical significance (p = 0.434)
- ROC analysis showed overcorrection beyond 15 degrees valgus gave no additional benefit
- Prospective series of 34 patients with 65 deformities treated with a non-locking tension band (2-hole) plate
- 32/34 patients corrected to neutral at a mean of 11 months with no permanent growth arrests
- Correction approximately 30% faster than with stapling; 4 idiopathic genu valgum cases had rebound
- Only the 2 adolescent Blount patients had insufficient correction and may need osteotomy
Complications
Peroneal nerve palsy:
- Most feared complication of proximal tibial osteotomy; incidence 1-5% depending on technique
- Usually a neurapraxia that recovers over 3-6 months
- Risk factors: lateral closing wedge, excessive acute lengthening, proximal fibular osteotomy
- Management: document immediately post-op, foot-drop brace (AFO), monitor for recovery; EMG at 6 weeks if no recovery
Compartment syndrome:
- Rare but devastating; risk rises with extensive soft-tissue dissection or acute lengthening
- Presents with pain out of proportion and pain on passive stretch
- Immediate fasciotomy if suspected - do NOT delay
Vascular injury: very rare; anterior tibial artery at risk with proximal fibular osteotomy. Know the anatomy; vascular consultation if suspected.
Wound complications / hardware issues: infection, dehiscence, haematoma (more common with external fixator pin sites and in obese patients); loss of fixation or prominent hardware.
RECURSRECURS - Preventing Recurrence After Osteotomy
Hook:Recurrence RECURS most commonly in young children - plan for it with overcorrection, monitoring, and realistic family counseling about potential revision surgery.
- 82 patients (115 limbs) over 22 years; 48 limbs required at least one repeat surgery for recurrence
- Mean age at surgery 4.3 years (no recurrence) vs 6.2 years (recurrence) - age 5 a critical transition
- Recurrence high for Langenskiöld stage III (50%) and stage IV (69.6%)
- A modified A/B/C classification of metaphyseal/epiphyseal slope predicted recurrence (type C 71.7%) better than Langenskiöld; pre-op MAD, MPTA and BMI did not differ between groups
Outcomes and Prognosis
Infantile Blount disease:
- Bracing success (Stage I-II, under age 3 years): 60-80% achieve correction
- Surgical outcomes: 85-90% satisfactory alignment at maturity if treated appropriately
- Recurrence: 30-50% if operated under age 4, 15-20% age 4-8, under 10% after age 8
- Long-term function: excellent if treated early; low OA risk if corrected before a persistent lateral thrust develops
Adolescent Blount disease:
- Bracing: ineffective
- Surgical outcomes: 85-90% satisfactory short-term alignment
- Recurrence: lower than infantile (under 10%) due to limited remaining growth
- Long-term function: good, but higher rate of early OA from pre-existing overload; obesity management is critical
Factors affecting prognosis: age at treatment, Langenskiöld stage (and slope morphology), obesity, compliance, and laterality (bilateral infantile often responds better to bracing).
Guidelines, Registries & Global Practice
Global epidemiology:
- Prevalence varies markedly by population - higher in those of African, Afro-Caribbean and Hispanic descent and in regions where infants walk early
- Relatively rare in Northern European/Caucasian populations
- Rising worldwide with childhood obesity, particularly the adolescent (late-onset) form; obesity is an independent, modifiable risk factor for needing surgery
Side-by-side principles (consistent across major bodies):
- There is no single dominant national guideline for Blount disease; practice is driven by classic and contemporary evidence (Levine & Drennan; Feldman & Schoenecker; Stevens; LaMont) and instructional reviews (e.g. POSNA/JPO updates)
- Diagnosis: standing AP radiograph with the Drennan MDA is the universally accepted screening/diagnostic tool; MRI is favoured (over CT) for physeal/bar assessment in children to limit radiation
- Conservative care: KAFO bracing for infantile Stage I-II under age 3 is widely offered, though its efficacy remains debated and is not universally adopted
- Surgery: proximal tibial valgus osteotomy is the global workhorse; growth modulation (tension band plating) and circular external fixators (Ilizarov, Taylor Spatial Frame) are established alternatives where expertise and implants are available
Registry note: Blount disease is a paediatric deformity condition and is not tracked by arthroplasty/implant registries (NJR, AJRR, AOANJRR, SHAR, NZJR). Evidence derives from single-centre and multicentre paediatric series rather than registry data.
High- vs limited-resource variation:
- In well-resourced settings, early screening, MRI, guided growth, and computer-assisted hexapod fixators are available, enabling earlier and less invasive correction
- In limited-resource or remote settings, late presentation with severe (Stage IV-VI) deformity is more common; treatment relies on osteotomy with simple internal or external fixation, and weight-management/lifestyle programmes may be less accessible
- Culturally appropriate counselling, family involvement, and interpreter support improve adherence to bracing and follow-up in all settings
MCQ Practice Points
The following topics are frequently tested in Orthopaedic exams related to Blount disease:
Q: What is the most important radiographic measurement for predicting progression of physiologic genu varum to Blount disease?
A: Drennan's metaphyseal-diaphyseal angle (MDA).
- MDA under 11 degrees: physiologic, likely to resolve
- MDA 11-16 degrees: at risk for progression, close monitoring required
- MDA over 16 degrees: diagnostic of Blount disease, will not resolve spontaneously
MDA is measured on standing AP radiograph as the angle between a line tangent to the medial and lateral metaphyseal beaks and a line along the tibial shaft longitudinal axis.
Q: A 2-year-old child with bilateral genu varum has an MDA of 13 degrees and Langenskiöld Stage I changes. What is the most appropriate initial management?
A: Full-time KAFO bracing for 12-24 months, worn 23 hours daily.
This child meets the criteria for a bracing trial: age appropriate (under 3 years), Stage I disease, MDA in the predictive range (11-16 degrees). Success rate is 60-80% for Stage I-II under age 3. Monitor every 3-4 months; convert to surgery if no improvement by 6-12 months.
Critical point: night-time only bracing is ineffective - it must be full-time.
Q: What Langenskiöld stage represents the threshold beyond which bracing is ineffective and surgery is required?
A: Stage IV (medial metaphyseal overgrowth). Stages I-III may respond to bracing if early and age-appropriate. Once Stage IV changes are present (medial metaphyseal beak projecting beneath the epiphysis), osteotomy is required. Stages V and VI absolutely require surgery.
Q: A 3.5-year-old undergoes proximal tibial valgus osteotomy for bilateral Blount disease. What is the most common complication?
A: Recurrence of varus deformity. Recurrence rates: under age 4-5 years 30-50%; age 4-8 years 15-20%; over age 8 years under 10%. Prevention includes overcorrection to 5-10 degrees valgus, lateral hemiepiphysiodesis, and intensive monitoring until skeletal maturity.
Q: What nerve is most at risk during proximal tibial osteotomy for Blount disease?
A: Common peroneal nerve, which courses around the fibular neck. Risk is highest with lateral closing wedge osteotomy, proximal fibular osteotomy, excessive acute lengthening (over 10-15mm), and significant lateral dissection. Most injuries are neurapraxia recovering over 3-6 months. Document baseline and immediate post-op neuro exam.
Q: What is the target correction angle for proximal tibial valgus osteotomy in Blount disease?
A: 5-10 degrees valgus (overcorrection from neutral) to compensate for the recurrence tendency and restore the mechanical axis. Under-correction to neutral results in higher recurrence; more aggressive overcorrection (~10 degrees) may be used in recurrent cases or very young children, though overcorrection beyond ~15 degrees gives no added benefit.
Q: What percentage of Blount disease cases have associated internal tibial torsion?
A: 60-80%. Assess with the thigh-foot angle (prone, knees flexed 90 degrees; normal ~10 degrees external). Internal tibial torsion should be corrected simultaneously during osteotomy by externally rotating the distal fragment 10-20 degrees; failure to address rotation leaves persistent functional impairment despite angular correction.
Q: Which form of Blount disease has a lower recurrence rate after surgery, infantile or adolescent?
A: The adolescent form has a lower recurrence rate (under 10% vs 30-50% for infantile operated under age 4) because of limited remaining growth. However, the adolescent form has worse overall outcomes - it often presents late with severe deformity, has limited remodeling potential, is strongly linked to obesity, and carries a higher risk of early osteoarthritis from chronic overload prior to correction.
At a Glance
The OnePagerSummary above provides a comprehensive at-a-glance overview of Blount disease including the Langenskiöld classification, key statistics, must-know concepts, and exam pearls.
MDAMDA - Key Angles for Blount Disease
Hook:MDA guides everything - under 11° is physiologic, 11-16° is concerning, over 16° is diagnostic. Always measure the MDA first!
Summary
Blount disease (tibia vara) is a pathologic growth disturbance of the medial proximal tibial physis producing progressive genu varum. Two distinct forms exist: infantile (onset under 4 years, often bilateral) and adolescent (onset after 8 years, obesity-related, usually unilateral).
Key diagnostic features:
- Drennan's metaphyseal-diaphyseal angle (MDA): over 16 degrees diagnostic; 11-16 degrees a gray zone
- Langenskiöld classification (Stages I-VI): Stage IV is the threshold for surgery
Management:
- Observation: physiologic genu varum with MDA under 11 degrees
- Bracing (KAFO): age under 3 years, Stage I-II, MDA 11-16 degrees, 23 hours daily for 12-24 months (60-80% success)
- Surgery: Stage IV or higher, failed bracing, age over 4 years, all adolescent disease
- Options: proximal tibial valgus osteotomy (workhorse; correct to 5-10 degrees valgus); guided growth for selected early cases; external fixator for severe/complex or very young
Critical exam points: differentiate from physiologic bowing using MDA and age; Stage IV = surgery mandatory; overcorrect to 5-10 degrees valgus; address internal tibial torsion (60-80%); and counsel about recurrence when operating on young children. Long-term monitoring until skeletal maturity is essential, particularly after early surgery.
Exam Day Cheat Sheet
Must-Know Classification
- **Langenskiöld Stages I-VI**: I (mild beaking) → II (metaphyseal defect) → III (fragmentation) → IV (metaphyseal overgrowth) → V (epiphyseal separation) → VI (physeal bar)
- **Stage IV = surgery mandatory threshold**
- **Drennan MDA**: Under 11° (physiologic), 11-16° (at risk), over 16° (diagnostic)
- **Two forms**: Infantile (under 4 years, bilateral, better bracing response) vs Adolescent (over 8 years, unilateral, obesity-related, poor bracing response)
Critical Differentials
- **Physiologic genu varum**: Resolves by age 2-3, MDA under 11°, bilateral, no metaphyseal changes
- **Rickets**: Widened physis throughout skeleton, frayed metaphysis, low Ca/PO4, elevated ALP
- **Focal fibrocartilaginous dysplasia**: Unilateral, abrupt angulation, cortical defect, self-limiting
- **Skeletal dysplasia**: Multiple joint involvement, short stature, family history
Bracing Protocol (MUST KNOW ALL CRITERIA)
- **Age under 3 years** (preferably 1-3 years) - critical factor
- **Langenskiöld Stage I-II** (occasionally early Stage III)
- **MDA 11-16 degrees** (some include up to 20 degrees)
- **KAFO worn 23 hours daily** for 12-24 months; night-time only = ineffective
- Success rate 60-80% for Stage I-II under age 3 years
- Monitor every 3-4 months, recognize failure by 6-12 months
Surgical Indications & Principles
- **Langenskiöld Stage IV or higher** (absolute indication)
- **Failed bracing**, **age over 4 years**, all **adolescent** disease, progressive deformity with lateral thrust
- **Proximal tibial valgus osteotomy** = workhorse procedure
- **Target: 5-10 degrees valgus** (overcorrect; beyond ~15° no benefit)
- **Address internal tibial torsion** simultaneously (present in 60-80%)
- **Fibular osteotomy** often required (mid-shaft safer for peroneal nerve)
Complications (High Yield)
- **Peroneal nerve palsy** (1-5% incidence, usually recovers in 3-6 months)
- **Recurrence** (most common long-term; 30-50% if under age 4-5, under 10% over age 8)
- **Compartment syndrome** (rare but devastating - high index of suspicion)
- **Physeal bar formation** (Stage VI or from surgery crossing physis)
- **Malunion** and **leg length discrepancy**
Viva Scenario Approach
- **Always measure MDA** - under 11° vs 11-16° vs over 16° guides management
- **Stage the disease** using Langenskiöld - Stage IV is the surgery threshold
- **Assess age** - under 3 years consider bracing, 3-4 borderline, over 4 surgery
- **Rule out metabolic causes** if atypical (young age, short stature, bilateral symmetric)
- **Counsel about recurrence** if operating on young children (30-50% if under age 4-5)
- **Don't forget rotation** - internal tibial torsion in 60-80%, correct simultaneously
Quick Exam Tips
- MDA over 16° = diagnostic of Blount disease (will NOT resolve)
- Stage IV = medial metaphyseal beak = surgery required
- Age under 3 + Stage I-II = try bracing (23 hrs/day, not night-only)
- Peroneal nerve at risk - ALWAYS mention in surgical consent/complications
- Overcorrect to 5-10° valgus to prevent recurrence
- Recurrence highest if surgery under age 4-5 years
- Adolescent form = unilateral, obesity, poor bracing response, needs surgery
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 20-month-old child presents with bilateral genu varum. The parents are concerned that the bowing is worsening. The child walked at 11 months of age. The standing AP radiograph shows an MDA of 9 degrees bilaterally with no metaphyseal changes. How would you manage this child?”
“A 3.5-year-old child with bilateral infantile Blount disease has been compliant with full-time KAFO bracing for 18 months (started at age 2 years). Initial MDA was 14 degrees bilaterally, Langenskiöld Stage II. Current radiographs show MDA 17 degrees and progression to Stage III bilaterally. What is your recommendation?”
“A 13-year-old obese boy (BMI 35) presents with right knee pain and progressive varus deformity over the past year. Standing long-leg radiographs show MDA 22 degrees, Langenskiöld Stage IV, mechanical axis passes 4 cm medial to knee center, and 2 cm leg length discrepancy (right shorter). How would you manage this patient?”
“A 7-year-old child presents with recurrent varus deformity. She had bilateral proximal tibial valgus osteotomies at age 3.5 years for infantile Blount disease with good initial correction. Current radiographs show MDA 16 degrees bilaterally, Langenskiöld Stage IV bilaterally, and mechanical axis medial to knees. She has a lateral thrust gait. What would you do?”
Evidence Base
- Defined the metaphyseal-diaphyseal angle (MDA) to differentiate physiologic bowing from infantile tibia vara before radiographic changes appear
- 29 of 30 extremities with an initial MDA over 11 degrees developed radiographic tibia vara
- Only 3 of 58 extremities with an MDA of 11 degrees or less developed diagnostic changes
- Approximately 60% of the deformity in tibia vara arises in the proximal metaphysis vs ~20% in physiologic bowing
- 106 children (179 limbs) with physiologic bowing vs 19 children (32 limbs) with Blount disease
- Mean MDA 9 degrees (physiologic) vs 19 degrees (Blount), p less than 0.0000001
- Greatest false-positive/false-negative overlap (error rate over 5%) when the MDA was between 9 and 16 degrees
- MDA aids identification of Blount disease but should not be the sole diagnostic criterion