Rarest Benign Cartilaginous Tumor | Eccentric Metaphyseal Lesion | Lobular Myxoid Pattern
- Rarest benign cartilaginous tumor - less than 1% of primary bone tumors, often misdiagnosed
- Eccentric metaphyseal location - classic pattern with endosteal scalloping and cortical expansion
- Lobular histology - characteristic lobules with myxoid matrix, hypercellular periphery, sparse central cells
- High recurrence rate - 25% after simple curettage; consider adjuvants (phenol, PMMA, cryotherapy)
- Can mimic chondrosarcoma - both clinically and histologically, requiring expert pathology review
- “Know the classic imaging triad: eccentric metaphyseal, scalloped margin, sclerotic rim
- “Histology pearl: hypercellular periphery with spindle cells vs hypocellular myxoid center - opposite pattern to chondrosarcoma
- “Be prepared to discuss differential diagnosis: chondroblastoma, ABC, chondrosarcoma, fibrous dysplasia
- “Understand treatment controversy: curettage alone (high recurrence) vs curettage with adjuvants vs en bloc resection
Under 1% of bone tumors. Most orthopaedic surgeons will see few cases in their career. High index of suspicion needed for eccentric metaphyseal lesion in young adult. Often initially misdiagnosed.
Histology can be misleading. Hypercellular areas at lobule periphery may mimic malignancy. Key: CMF has sparse central cells with myxoid matrix; chondrosarcoma has permeative pattern and nuclear atypia.
Eccentric metaphyseal location with endosteal scalloping, cortical expansion, sclerotic rim. Proximal tibia most common (25-30%). Radiographically similar to chondroblastoma but different age.
25% recurrence after curettage. Consider adjuvants: phenol, liquid nitrogen, argon beam, PMMA cement. En bloc resection for aggressive lesions or recurrent disease.
- Imaging Pattern
- Eccentric, sclerotic rim, no soft tissue
- Management
- Observation with serial radiographs
- Key Pearl
- Many are asymptomatic incidental findings
- Imaging Pattern
- Metaphyseal, scalloped, well-defined
- Management
- Extended curettage with adjuvant
- Key Pearl
- Use phenol or cryotherapy to reduce recurrence
- Imaging Pattern
- Cortical breakthrough, soft tissue mass
- Management
- Wide excision with reconstruction
- Key Pearl
- Consider en bloc for expendable bones (fibula, rib)
LOBULARHistologic Lobules Pattern
Hook:LOBULAR architecture is the key! Hypercellular periphery, hypocellular myxoid center - remember this REVERSE pattern.
Overview and Epidemiology
Chondromyxoid fibroma (CMF) is the rarest benign cartilaginous tumor, accounting for less than 1% of all primary bone tumors and approximately 2% of benign bone tumors. First described by Jaffe and Lichtenstein in 1948, it remains one of the most diagnostically challenging bone lesions due to its rarity and potential to mimic chondrosarcoma both radiographically and histologically. Most orthopaedic surgeons will encounter only a handful of cases throughout their career, making high clinical suspicion and expert pathology review essential for accurate diagnosis.
- Age: 10-30 years (second to third decade)
- Gender: Male predominance 2:1
- Location: Metaphysis of long bones (70%)
- Most common sites: Proximal tibia (25-30%), distal femur (15%), pelvis (15%)
- Rare locations: Skull, ribs, small bones of hands/feet
- Growth pattern: Slow-growing, locally aggressive
- Symptoms: Often asymptomatic, found incidentally
- Duration: Symptoms present for months to years
- Recurrence: 25% after simple curettage, 10% with adjuvants
- Malignancy: Exceedingly rare malignant transformation reported
Geographic and Anatomic Distribution
CMF can occur in any bone but shows predilection for metaphyseal regions of long bones, particularly around the knee. Pelvic involvement, especially the iliac wing, is more common than with other benign cartilaginous tumors. Rare axial skeleton involvement (ribs, skull base) can present with unique challenges due to anatomic constraints and difficulty distinguishing from chordoma or chondrosarcoma.
Pathophysiology and Histopathology
Tumor Origin and Biology
The exact cell of origin for CMF remains debated. Theories include:
- Cartilage rest theory: Aberrant cartilage differentiation from primitive mesenchyme
- Metaplastic theory: Fibrous tissue undergoing cartilaginous metaplasia
- Neoplastic chondroblast: Benign proliferation of immature cartilage-forming cells
CMF is a benign but locally aggressive lesion that grows slowly by expansion and endosteal erosion. Unlike true cartilaginous neoplasms (enchondroma, chondrosarcoma), CMF lacks classic hyaline cartilage and instead contains abundant myxochondroid (myxoid and chondroid) matrix. This unique composition reflects its intermediate position between fibrous and cartilaginous lesions, hence the name "chondro-myxo-fibroma."
Gross Pathology
- Color: Gray-white to tan-yellow
- Consistency: Firm, lobulated, rubbery to gritty
- Borders: Well-circumscribed, may have thin shell
- Hemorrhage: Occasional areas of hemorrhage
- Cysts: Focal cystic degeneration possible
- Cortical thinning: Expansion from within
- Endosteal scalloping: Characteristic pattern
- Soft tissue: Usually no soft tissue extension
- Curettage yield: Gelatinous to gritty tissue
- Boundaries: Pseudocapsule often present
Microscopic Histology - The Diagnostic Hallmark
The lobular architecture of CMF is its most distinctive histologic feature. Each lobule consists of three zones:
- Central zone: Sparse stellate and spindle cells in abundant myxoid or chondroid matrix
- Intermediate zone: Increased cellularity with chondroblast-like cells
- Peripheral zone: Hypercellular rim of spindle cells, osteoclast-like giant cells, and reactive bone
This zonal pattern repeats throughout the lesion and is separated by fibrous septa. The hypercellular periphery can be mistaken for chondrosarcoma, but the bland cytology, lack of permeative growth, and myxoid center distinguish CMF.
Histologic Features
Nodular or lobular pattern with fibrous septae separating lobules. This is the single most important diagnostic feature. Each lobule shows zonal variation in cellularity.
Myxochondroid matrix centrally in lobules - abundant extracellular material with myxoid (mucoid) and chondroid components. This gives the lesion its gelatinous appearance on curettage.
Hypercellular periphery with spindle cells, stellate cells, and multinucleated giant cells. This zone can show apparent pleomorphism but lacks true anaplasia. The cells have bland nuclei without permeative pattern.
Calcification uncommon compared to other cartilage tumors. When present, it is focal and stippled within the myxoid matrix, not the ring-and-arc pattern of enchondroma.
Immunohistochemistry
CMF shows variable staining patterns:
- S100 protein: Positive in chondroid areas (confirms cartilaginous differentiation)
- Vimentin: Diffusely positive
- Keratin: Usually negative
- Sox9: Positive in chondrogenic cells
- Ki-67: Low proliferation index (under 5%), confirming benign nature
- GRM1: Overexpressed - a sensitive, relatively specific marker for CMF
Molecular Hallmark: GRM1 Rearrangement
According to PubMed, CMF is now defined molecularly by recurrent rearrangement of the GRM1 gene (encoding metabotropic glutamate receptor 1), in which GRM1 is placed under a constitutively active promoter and over-expressed (Torrence D et al., Histopathology 2024 — DOI). Break-apart FISH detects the rearrangement in roughly 75% of cases, while GRM1 immunohistochemistry is the most sensitive surrogate and is positive in around 97% of CMF yet negative in chondrosarcoma, enchondroma, chondroblastoma, giant cell tumour and other mimics (Toland AMS et al., Am J Surg Pathol 2022 — DOI). This makes GRM1 testing the single most useful ancillary tool when CMF must be separated from low-grade chondrosarcoma on a difficult biopsy.
The hypercellular peripheral zone of CMF can closely mimic chondrosarcoma on small biopsy samples. The key distinguishing features are: (1) CMF has lobular architecture with hypocellular myxoid centers, (2) CMF lacks the permeative growth pattern of chondrosarcoma, (3) CMF shows bland cytology despite cellularity, and (4) clinical/radiographic correlation shows benign features (sclerotic rim, eccentric location). Expert pathology review is essential - misdiagnosis as chondrosarcoma can lead to unnecessary amputation.
Classification

WHO Classification
Chondromyxoid fibroma is classified by the WHO as a benign cartilaginous tumor with low risk of local recurrence and no metastatic potential.
Enneking Classification (Benign Tumors)
- Behavior
- Inactive
- Features
- Well-defined, sclerotic rim, stable
- CMF Applicability
- Incidental CMF, minimal symptoms
- Behavior
- Growing slowly
- Features
- Defined margins, thin rim, may progress
- CMF Applicability
- Typical symptomatic CMF
- Behavior
- Locally aggressive
- Features
- Poorly defined, cortical destruction
- CMF Applicability
- Rare - consider chondrosarcoma
Clinical Classification
- Metaphyseal: Most common (90%), typical appearance
- Diaphyseal: Less common, may be larger at presentation
- Epiphyseal: Rare, more difficult surgical access
- Primary: Initial presentation, most common
- Recurrent: After prior treatment, higher grade suspected if aggressive
S2 (Active) lesions require treatment with extended curettage and adjuvant. S1 (Latent) lesions may be observed if incidental and asymptomatic. S3 (Aggressive) features should raise suspicion for chondrosarcoma and require expert review.
Clinical Presentation
- Pain: Dull, aching, intermittent (most common symptom)
- Duration: Months to years of gradual onset
- Mass: Palpable swelling in superficial locations
- Function: Limitation of motion if near joint
- Night pain: Uncommon (unlike osteoid osteoma)
- Incidental: 20-30% discovered on imaging for other reasons
- Inspection: Mild swelling over metaphyseal region
- Palpation: Firm, fixed to bone, non-tender or mildly tender
- Joint exam: Usually normal range of motion
- Neurovascular: Typically intact
- Skin: No warmth, erythema, or overlying changes
- Lymph nodes: No regional lymphadenopathy
Symptom Patterns by Location
- Typical Symptoms
- Knee pain, limp, activity-related pain
- Physical Findings
- Tenderness over proximal tibia, palpable mass
- Special Considerations
- DDx includes osteosarcoma, GCT, chondroblastoma
- Typical Symptoms
- Deep pelvic pain, gluteal region discomfort
- Physical Findings
- Mass difficult to palpate, check hip ROM
- Special Considerations
- MRI essential for defining extent, can mimic chondrosarcoma
- Typical Symptoms
- Localized pain, swelling, difficulty with footwear
- Physical Findings
- Visible swelling, point tenderness
- Special Considerations
- High recurrence risk in confined space
Pathological Fracture
Unlike more aggressive lesions (ABC, GCT), pathological fracture through CMF is rare due to the typically slow growth and preservation of cortical shell. When fracture occurs, it suggests either:
- Large lesion with significant cortical thinning
- Trauma to weakened bone
- More aggressive behavior warranting wide excision Fracture does not change the benign nature but may necessitate staged treatment (healing, then definitive surgery).
Unusual Presentations
CMF can rarely present with:
- Spinal involvement: Neurological symptoms from cord or nerve root compression
- Sacral lesions: Bowel/bladder symptoms mimicking chordoma
- Rib lesions: Chest wall mass, respiratory symptoms
- Skull base: Cranial nerve palsies, headaches
Imaging and Diagnosis
Plain Radiography - First-Line Investigation
Radiographic Features
Eccentric metaphyseal lesion - the hallmark imaging feature. CMF arises from the cortex and expands outward, causing endosteal scalloping and cortical expansion. This eccentric pattern distinguishes it from central medullary lesions like enchondroma.
Endosteal scalloping - the cortex is thinned from within, creating a scalloped or festooned inner margin. This indicates slow growth with bone remodeling. Aggressive lesions show cortical breakthrough.
Sclerotic border - reactive sclerosis at the margins of the lesion indicates slow growth and benign behavior. Absence of sclerotic rim raises concern for aggressive behavior or malignancy.
Matrix: Usually lucent (lytic) without visible calcification. When present, calcification is faint, amorphous, and irregular - not the classic ring-and-arc of enchondroma or fluffy clouds of chondrosarcoma.
The classic radiographic triad of CMF is: (1) eccentric metaphyseal location, (2) endosteal scalloping with cortical expansion, and (3) sclerotic rim. This combination in a patient aged 10-30 years should raise suspicion for CMF. However, imaging alone cannot distinguish CMF from low-grade chondrosarcoma - biopsy is mandatory for tissue diagnosis before definitive treatment.
Chondroid Matrix Mineralization: "Rings and Arcs"
The topic repeatedly contrasts CMF with the "ring-and-arc" calcification of enchondroma and the "fluffy" matrix of chondrosarcoma, so it is worth understanding what that sign actually is and why CMF characteristically lacks it.
- What it is: "rings and arcs" (also described as punctate, stippled, comma-shaped, flocculent or "popcorn") is the radiographic fingerprint of a chondroid matrix - its presence on radiograph or CT essentially confirms that a lesion is a cartilage tumour.
- Why this pattern: cartilage lobules are avascular, so mineralization (enchondral ossification) occurs at the periphery and septa of the lobules, ringing each lobule - producing the rings-and-arcs appearance.
- Why CMF is different: CMF's matrix is myxoid (myxochondroid) rather than mature hyaline cartilage, so it shows little or no mineralization - identified radiographically in only about 13% of the Mayo series and, when present, faint and amorphous rather than well-formed rings. The relative absence of organised chondroid calcification in an eccentric metaphyseal chondroid lesion is itself a clue toward CMF over enchondroma.
- Reading malignancy into the matrix: dense, organised rings-and-arcs favour a benign or low-grade cartilage tumour; destruction of previously visible calcification, a new lytic area, deep endosteal scalloping (more than two thirds of the cortex), or a soft-tissue mass signal chondrosarcomatous behaviour.
"Rings and arcs" (and punctate/popcorn) calcification is the radiographic signature of a chondroid matrix - mineralization at the periphery of avascular cartilage lobules. CMF is the cartilage tumour that characteristically lacks it (myxoid, not hyaline, matrix), so an eccentric metaphyseal chondroid lesion with little or only amorphous calcification in a young adult fits CMF. Conversely, dense rings-and-arcs that become destroyed alongside a new lytic area and soft-tissue mass point to chondrosarcoma.
Reading Aggressiveness: Lodwick-Madewell Margins and Zone of Transition
The body grades CMF as "geographic", "well-defined with a sclerotic rim" and contrasts the "permeative" pattern of chondrosarcoma - these are the terms of the Lodwick-Madewell classification, the standard framework for judging how aggressive a lytic bone lesion looks.
- Geographic (Lodwick grade I) - a single, well-defined lytic area implying slow growth: IA = with a sclerotic rim (most indolent - the classic CMF pattern), IB = well-defined without a sclerotic rim, IC = a partly ill-defined margin.
- Moth-eaten (grade II) - multiple confluent lucencies, and permeative (grade III) - ill-defined tiny lucencies infiltrating between trabeculae: both imply a rapid, aggressive or malignant process.
- The unifying concept is the zone of transition - the width of the border between lesion and normal bone. A narrow zone (a sharp, often sclerotic edge) means slow, benign growth; a wide zone (no clear line where the lesion ends) means rapid, aggressive growth. CMF's sclerotic rim is a narrow zone of transition; loss of that rim with a widening zone of transition is a red flag for chondrosarcoma.
Grade a lytic bone lesion by its margin: geographic with a sclerotic rim (Lodwick IA, narrow zone of transition) = benign and slow (CMF's pattern), whereas moth-eaten or permeative (wide zone of transition) = aggressive or malignant. The zone of transition is the single most useful plain-film discriminator of benign versus aggressive bone lesions.
CT Imaging
CT provides superior assessment of:
- Cortical integrity: Precise delineation of cortical thinning vs breakthrough
- Matrix calcification: Better detection of subtle calcifications than X-ray
- Sclerotic margins: Quantification of reactive sclerosis
- Bone destruction: Pattern of bone involvement (geographic vs permeative)
- Surgical planning: 3D reconstruction for complex anatomy (pelvis, spine)
- Eccentric, lobulated, expansile mass
- Endosteal scalloping with cortical thinning
- Sclerotic rim at margins
- No or minimal internal calcification
- No periosteal reaction (unless fractured)
- No soft tissue mass (unless aggressive)
CT advantages: Calcification detection, cortical bone detail MRI advantages: Soft tissue extent, cartilage cap assessment, intramedullary involvement Best practice: Both modalities complement for complete assessment
MRI - Gold Standard for Soft Tissue Assessment
MRI is superior for evaluating:
- Intramedullary extent: Marrow involvement
- Soft tissue extension: Mass beyond cortex
- Neurovascular structures: Proximity to nerves/vessels
- Signal characteristics: Heterogeneous signal reflecting lobular myxoid composition
- Signal Intensity
- Low to intermediate signal
- Interpretation
- Reflects myxoid and cartilaginous matrix
- Signal Intensity
- Very high signal (bright)
- Interpretation
- Myxoid matrix has high water content, bright on T2
- Signal Intensity
- Heterogeneous enhancement
- Interpretation
- Peripheral lobular enhancement, septal enhancement
Both CMF and low-grade chondrosarcoma show similar MRI features: high T2 signal, lobulated margins, and heterogeneous enhancement. Clinical correlation (age, symptoms) and histology are essential. Key differences favoring CMF: younger age (10-30 vs over 40), eccentric location, sclerotic rim on X-ray, and lack of soft tissue mass. Biopsy is always required.
Nuclear Medicine
Bone scan (Tc-99m MDP):
- Uptake pattern: Moderate to marked uptake in CMF
- Utility: Limited for diagnosis but useful for detecting multifocal disease or metastatic survey
- PET-CT: Not routinely used; CMF can show FDG uptake, complicating interpretation
Biopsy - Essential for Diagnosis
Image-guided core needle biopsy is preferred over open biopsy for initial diagnosis:
- Multiple cores (3-5) to sample lobular architecture
- Avoid biopsy tract contamination of neurovascular structures
- CT or fluoro guidance for deep lesions (pelvis, spine)
- Send fresh tissue for cytogenetics if available
Expert musculoskeletal pathology review mandatory:
- CMF is rare and easily misdiagnosed
- High-volume center reduces misdiagnosis as chondrosarcoma
- Correlation with radiology essential
- Consider second opinion for any atypical features
Small core biopsies may sample only the hypercellular peripheral zone of CMF lobules, leading to misdiagnosis as chondrosarcoma. The pathologist must recognize the lobular architecture and low-power pattern. Correlation with imaging (showing benign features like sclerotic rim, eccentric location) and clinical context (young age) is essential. If doubt exists, open biopsy with larger sample size may be warranted before proceeding with ablative surgery.
MYXOIDDiagnostic Features of Chondromyxoid Fibroma
Hook:MYXOID - the name tells you it has MYXOID matrix! Think rare, eccentric metaphyseal, scalloped lesion in young adult.
Differential Diagnosis
Cartilaginous Lesion Differentials
- Age
- 10-30 years
- Location
- Eccentric metaphysis
- Imaging
- Scalloped, sclerotic rim
- Histology
- Lobules, myxoid, hypercellular periphery
- Age
- 10-20 years (younger)
- Location
- Epiphysis/apophysis
- Imaging
- Lytic, rim sclerosis, ABC component
- Histology
- Chondroblasts, chicken-wire calcification, giant cells
- Age
- 20-40 years
- Location
- Central medullary (hands common)
- Imaging
- Ring-and-arc calcification
- Histology
- Hyaline cartilage lobules, no atypia
- Age
- Over 40 years (older)
- Location
- Medullary or surface
- Imaging
- Permeative, cortical thickening
- Histology
- Permeation, nuclear atypia, myxoid change
Both CMF and chondroblastoma occur in young patients and can have giant cells on histology. Key differences: (1) Location - chondroblastoma is epiphyseal/apophyseal, CMF is metaphyseal; (2) Age - chondroblastoma peaks at 10-20 years (before physeal closure), CMF at 20-30 years (after closure); (3) Histology - chondroblastoma has uniform chondroblasts with chicken-wire calcification, CMF has lobular myxoid pattern; (4) Imaging - chondroblastoma is more central, CMF is eccentric and cortically based.
Distinguishing CMF from low-grade chondrosarcoma is the most important clinical challenge and has enormous treatment implications (curettage vs amputation or wide resection). Favoring CMF: age under 30, eccentric cortical location, sclerotic rim, no soft tissue mass, lobular histology with bland cytology. Favoring chondrosarcoma: age over 40, central medullary or surface location, permeative pattern, cortical thickening, true nuclear atypia with permeative growth. When in doubt, seek expert pathology review and consider multidisciplinary tumor board discussion.
There are no additional paragraphs needed for this tab closure.
SCALLOPDifferential Diagnosis
Hook:Think SCALLOP for the scalloped endosteal margin! Run through differentials of eccentric metaphyseal lesions.
Management Algorithm
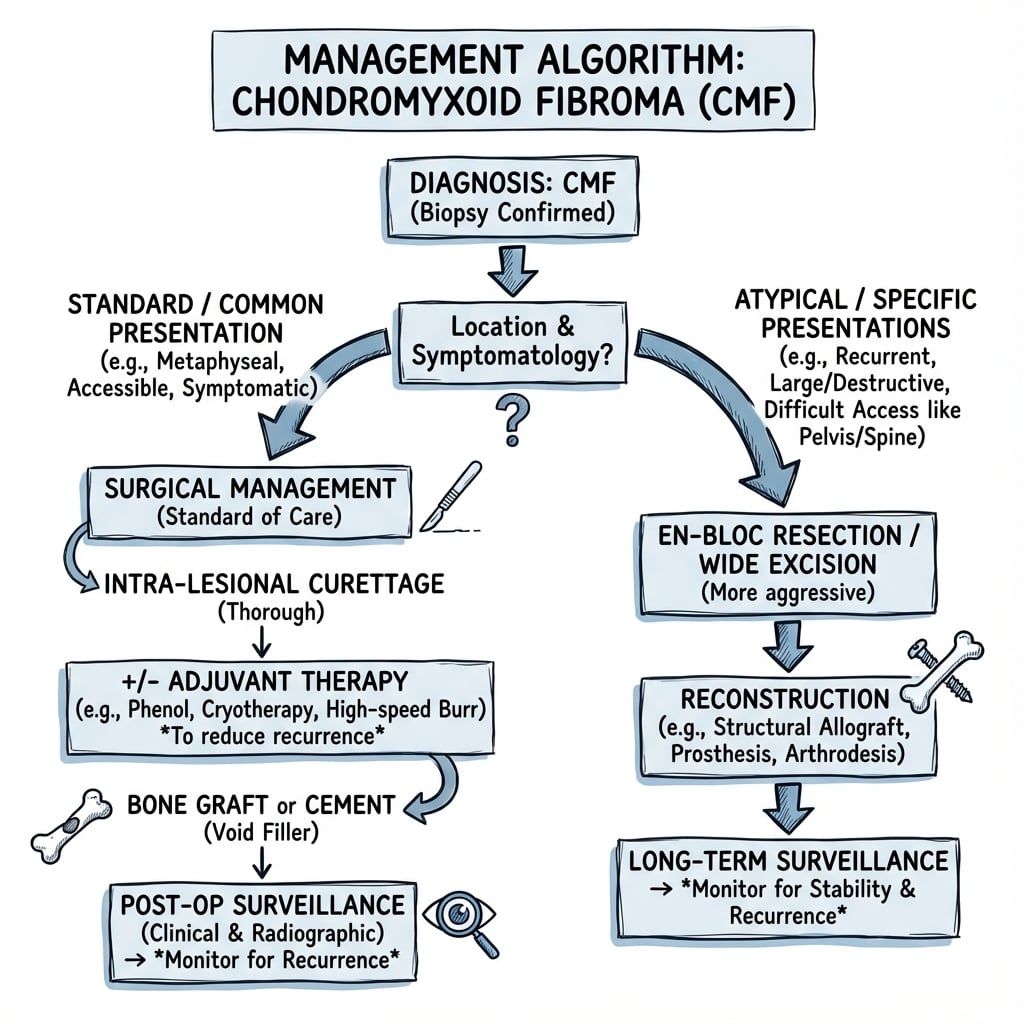
Treatment Decision Pathway
Obtain tissue diagnosis via image-guided core needle biopsy. Ensure expert musculoskeletal pathology review with radiologic correlation. Confirm diagnosis as CMF with lobular myxoid pattern before proceeding with definitive treatment.
Complete imaging: plain X-ray, MRI (or CT if MRI contraindicated). Assess cortical integrity, intramedullary extent, soft tissue extension, proximity to neurovascular structures. Enneking staging: CMF is benign (Stage 3 if aggressive features).
Choose treatment based on: lesion size, location, symptoms, cortical involvement, patient age, and functional demands. Options: observation, extended curettage with adjuvants, wide excision, or en bloc resection.
Serial imaging: X-ray every 3-6 months for first 2 years, then annually for 5 years. Recurrence typically occurs within 2 years. MRI if clinical or radiographic concern for recurrence.
Non-Operative Management
- Small, asymptomatic, incidental finding
- Lesion in stable phase (no growth on serial imaging)
- Patient unwilling to undergo surgery
- High surgical risk (medical comorbidities)
- Elderly patient with limited life expectancy
- Clinical exam: Every 3-6 months for 2 years
- X-ray: Every 6 months for 2 years, then annually
- MRI: If symptoms change or X-ray shows growth
- Proceed to surgery if: lesion enlarges, symptoms worsen, cortical breakthrough develops
Most CMF cases warrant surgical treatment due to risk of continued growth, pathological fracture, and diagnostic uncertainty. Observation is suitable only for truly asymptomatic, stable, small lesions in low-risk locations where biopsy has definitively confirmed the diagnosis. Given the rarity of CMF and potential for misdiagnosis, most surgeons advocate curettage both for treatment and to obtain adequate tissue for definitive histologic diagnosis.
Operative Management - Curettage with Adjuvants
Extended intralesional curettage with local adjuvants is the gold standard treatment for most CMF cases. The goals are: (1) remove all tumor tissue, (2) destroy residual microscopic disease with adjuvants, (3) fill defect to restore structural integrity, and (4) minimize morbidity compared to wide excision. Technique involves creating cortical window, aggressive curettage of all lobular tissue, high-speed burr of cavity walls, and application of local adjuvant (phenol, liquid nitrogen, argon beam, or PMMA).
Extended Curettage Procedure
Pre-operative Planning
- Review all imaging (X-ray, CT, MRI) to plan cortical window location
- Identify neurovascular structures at risk
- Determine need for reconstruction (bone graft vs PMMA vs allograft)
- Consent for possible pathological fracture during curettage
Surgical Steps
1. Exposure and Window Creation
- Incision directly over lesion (avoid placing over weight-bearing surface)
- Subperiosteal dissection preserving periosteum for closure
- Create cortical window with osteotomes or saw (preserve window as autograft)
- Size window to allow access to entire lesion (visualize all margins)
2. Intralesional Curettage
- Use large curettes to remove all visible tumor in piecemeal fashion
- Confirm lobular, gelatinous appearance consistent with CMF
- Send multiple samples for histology (confirm diagnosis on frozen section if first surgery)
- Curettage must reach healthy bone margins circumferentially
3. Extended Curettage with High-Speed Burr
- Use high-speed pneumatic burr to remove additional 1-2mm of cavity walls
- Burr creates smooth walls and removes microscopic residual tumor
- Ensure 360-degree burred surface (floor, walls, ceiling of cavity)
- Irrigate copiously to remove bone debris
4. Local Adjuvant Application
- Phenol: Apply with pledgets to cavity walls for 2 minutes, then irrigate with alcohol and saline
- Liquid nitrogen: Cryoprobe technique with two freeze-thaw cycles
- Argon beam: Coagulate cavity surface at high setting
- PMMA cement: Exothermic polymerization provides thermal adjuvant effect
5. Cavity Filling and Reconstruction
- Choose filler based on cavity size, location, and load-bearing needs:
- Small cavities (under 3cm): cancellous autograft or allograft chips
- Large cavities: PMMA cement (immediate weight-bearing) or structural allograft
- Metaphyseal cavities near joint: consider cancellous graft to preserve future arthroplasty options
- Fill cavity completely to prevent hematoma and provide structural support
6. Closure
- Replace cortical window (if preserved) as autograft
- Close periosteum over window if possible (enhances healing)
- Layered closure of subcutaneous tissue and skin
- Drain placement optional (some surgeons use for large cavities)
Post-operative Immobilization
- Upper extremity: Sling for comfort, early active ROM encouraged
- Lower extremity (non-weight bearing bones): Protected weight-bearing 6 weeks
- Lower extremity (weight-bearing bones): Non-weight bearing until X-ray shows graft incorporation (6-12 weeks)
- Pathological fracture risk: Consider prophylactic plate fixation if cortex extensively thinned
This section describes the complete surgical approach for CMF treatment.
Wide Excision or En Bloc Resection
En bloc resection with wide margins is reserved for specific scenarios:
- Recurrent disease: After failed curettage, especially multiple recurrences
- Aggressive features: Soft tissue extension, cortical destruction, pathological fracture
- Expendable bone: Fibula, rib, distal ulna where excision has minimal morbidity
- Uncertainty of diagnosis: Concern for low-grade chondrosarcoma on imaging or biopsy
- Failed adjuvant therapy: Multiple recurrences despite adjuvants suggest need for wide excision
Wide excision carries significantly higher morbidity (loss of bone, need for reconstruction, functional deficit) but provides lowest recurrence risk (under 5%).
- Surgical Approach
- Excise fibula segment with margins
- Reconstruction
- None (non-essential bone)
- Functional Outcome
- Excellent, protect peroneal nerve
- Surgical Approach
- En bloc pelvic resection
- Reconstruction
- Depends on extent (may not reconstruct)
- Functional Outcome
- Good for Type I resection, limp possible
- Surgical Approach
- Segmental tibial resection
- Reconstruction
- Intercalary allograft or vascularized fibula
- Functional Outcome
- Fair to good, prolonged protected weight-bearing
Management of Recurrent CMF
Recurrence Management Algorithm
Identify recurrence on serial X-ray (new lysis, loss of trabecular pattern) or MRI (soft tissue mass, high T2 signal). Biopsy if imaging unclear. Most recurrences occur within 24 months of initial curettage.
Repeat extended curettage with more aggressive adjuvant (e.g., cryotherapy if phenol was used initially). Send fresh tissue to confirm diagnosis (rule out malignant transformation). Use alternative adjuvant strategy.
Consider en bloc resection after second recurrence, especially if bone is expendable or if there is concern for diagnostic uncertainty. Multiple recurrences may indicate sampling error with underlying low-grade chondrosarcoma.
Exceedingly rare but reported. If biopsy of recurrence shows chondrosarcoma, proceed with wide resection with margins. This likely represents initial misdiagnosis rather than true transformation.
Surgical Technique
Extended Curettage Technique
Surgical Steps
Position according to lesion location. Tourniquet for extremity lesions. Direct approach over lesion using cortical window - extend window to visualize entire cavity. Preserve surrounding soft tissue.
Systematic removal of all tumor tissue using curettes of varying sizes. Start with large curettes, progress to small. Extend curettage 1-2mm beyond visible tumor margin. Send tissue for frozen section to confirm diagnosis.
High-speed burr entire cavity wall to extend margin (reduces recurrence 25% to 10%). Optional additional adjuvants: phenol (3 minutes), liquid nitrogen (cryotherapy), or argon beam coagulation.
Bone graft cavity: allograft cancellous chips, autograft iliac crest, or synthetic bone substitute. Large cavities near joints may require structural support - cortical strut or plate fixation.
Key Technical Points
- Size: Large enough to visualize and curette entire lesion
- Location: Directly over lesion, through thinnest cortex
- Preserve: Avoid physeal injury in skeletally immature patients
- High-speed burr: Standard adjuvant, low complication rate
- Phenol: Effective, requires meticulous irrigation after
- Cryotherapy: Most effective but highest fracture risk
- Combination: May be used for high-risk lesions
Extended curettage with high-speed burr reduces recurrence from 25% to approximately 10%. Adding phenol or cryotherapy further decreases recurrence but increases complication risk (pathological fracture, wound healing issues).
Complications
Surgical Complications
- Incidence
- 25% curettage alone, 10% with adjuvant
- Prevention
- Extended curettage, adjuvant use, adequate margins
- Management
- Repeat curettage or wide excision
- Incidence
- 5-10% (higher with cryotherapy)
- Prevention
- Assess cortical integrity pre-op, prophylactic fixation
- Management
- ORIF with plate/screws, bone grafting
- Incidence
- 2-5%
- Prevention
- Perioperative antibiotics, sterile technique
- Management
- Antibiotics, debridement if deep
- Incidence
- Under 2%
- Prevention
- Careful dissection, identify structures, avoid phenol spill
- Management
- Immediate exploration and repair if recognized
- Incidence
- 10-20% (iliac crest harvest)
- Prevention
- Limit harvest size, preserve outer table, good closure
- Management
- Pain management, physical therapy
- Incidence
- Under 5%
- Prevention
- Adequate graft fill, protected weight-bearing, avoid NSAIDs
- Management
- Revision grafting, consider BMP
Adjuvant-Specific Complications
- Chemical burn: Soft tissue necrosis if spills
- Neurotoxicity: Nerve damage if contacts major nerve
- Systemic toxicity: Rare with local use (metabolic acidosis)
- Prevention: Protect soft tissues with moist pads, avoid contact with nerves, limit volume
- Pathological fracture: Up to 10-15% due to bone necrosis
- Nerve injury: Cold injury to adjacent nerves (peroneal nerve at proximal tibia)
- Skin necrosis: If cryoprobe too close to skin
- Prevention: Prophylactic fixation in weight-bearing bones, identify nerves, monitor freezing
- Thermal necrosis: Exothermic heat (60-80°C) can damage soft tissues, nerves
- Precludes arthroplasty: Difficult cement removal if future joint replacement needed
- Cement extravasation: Into joint or soft tissues
- Prevention: Vent heat, protect soft tissues, avoid in young patients near joints
- Graft resorption: Especially allograft
- Fracture through graft: If inadequate incorporation or premature loading
- Infection: Higher with allograft (0.5-1%)
- Prevention: Adequate fill, protected weight-bearing, antibiotics for allograft
Long-Term Complications
Some patients experience chronic pain or reduced function after surgery, especially in weight-bearing locations:
- Stiffness: Prolonged immobilization or adhesions
- Weakness: Muscle atrophy during non-weight bearing
- Pain: Altered biomechanics, hardware irritation
- Limb length discrepancy: Premature physeal closure in skeletally immature patients
Management: Aggressive physical therapy, pain management, hardware removal if symptomatic, osteotomy for limb length inequality.
Malignant Transformation - Extremely Rare
Malignant transformation of CMF is exceedingly rare, with fewer than 10 reported cases in literature. When it occurs, it is unclear whether it represents:
- True malignant transformation of benign CMF
- Initial misdiagnosis with underlying low-grade chondrosarcoma
- Radiation-induced sarcoma (if prior radiation was given)
Most experts believe cases of "malignant CMF" are sampling errors with initial diagnosis, highlighting the importance of adequate tissue sampling and expert pathology review.
Postoperative Care and Rehabilitation
Immediate Post-operative Period (0-2 weeks)
- Sterile dressing for 48-72 hours
- Remove drain (if placed) when output under 30mL/24hr
- Suture or staple removal at 10-14 days
- Monitor for signs of infection (erythema, drainage, fever)
- Multimodal analgesia (acetaminophen, opioids prn)
- Avoid NSAIDs (impair bone healing) for first 6 weeks
- Ice and elevation for swelling
- Regional anesthesia (nerve block) for upper extremity
Mobilization and Weight-Bearing Protocol
- Graft Type
- Autograft or allograft
- Initial Status
- Sling for comfort, early ROM
- Full Weight-Bearing
- Immediate for ADLs, avoid heavy lifting 6 weeks
- Graft Type
- Any
- Initial Status
- Weight-bearing as tolerated
- Full Weight-Bearing
- Immediate
- Graft Type
- Cancellous autograft
- Initial Status
- Touch-down weight-bearing (10-20 lbs)
- Full Weight-Bearing
- 6-12 weeks (when X-ray shows incorporation)
- Graft Type
- PMMA cement
- Initial Status
- Weight-bearing as tolerated immediately
- Full Weight-Bearing
- Immediate (cement provides structural support)
- Graft Type
- Intercalary allograft
- Initial Status
- Non-weight bearing 6 weeks, then progressive
- Full Weight-Bearing
- 12-24 weeks (slower incorporation)
Rehabilitation Timeline
Rehabilitation Phases
Goals: Wound healing, minimize swelling, maintain adjacent joint ROM
- Upper extremity: Pendulum exercises (shoulder), elbow/wrist ROM, grip strengthening
- Lower extremity: Ankle pumps, quad sets, hip/knee ROM (non-weight bearing)
- Restrictions: No weight-bearing (unless PMMA), no resistance training
Goals: Progress weight-bearing, restore ROM, initiate strengthening
- Criteria: X-ray shows trabecular bridging, no pain with protected weight-bearing
- Exercises: Progressive resistance, proprioception training, gait training
- Weight-bearing: Advance from touch-down to partial (50%) to full
Goals: Full ROM, normal strength, return to activities
- Exercises: Functional training, sport-specific drills, endurance building
- Criteria for progression: Pain-free full ROM, strength 80% of contralateral side
- Return to sport: Unrestricted at 6 months if criteria met
Goals: Optimize function, prevent recurrence of symptoms
- Continue: Home exercise program, activity modifications as needed
- Monitor: Annual X-ray for first 5 years (detect recurrence)
Surveillance Protocol
CMF has a 25% recurrence rate after curettage, with most recurrences occurring within 24 months. Lifelong surveillance is recommended, with most intensive monitoring in first 5 years.
- Clinical Exam
- Every 3 months
- Radiographs
- Every 3-6 months
- MRI Indications
- Any pain, swelling, or X-ray concern
- Clinical Exam
- Every 6 months
- Radiographs
- Every 6-12 months
- MRI Indications
- Clinical symptoms or radiographic changes
- Clinical Exam
- Annually
- Radiographs
- Annually
- MRI Indications
- New symptoms only
Radiographic Signs of Recurrence
- New lysis: Lucency within previously grafted area
- Loss of trabeculation: Disappearance of bone graft trabecular pattern
- Cortical erosion: Scalloping or thinning of cortex
- Soft tissue mass: Visible soft tissue swelling
- High T2 signal: Myxoid recurrent tumor (very bright)
- Lobulated mass: Characteristic lobular pattern
- Cortical breach: Extension beyond original cavity
- Soft tissue extension: Extra-osseous component
Early post-operative X-rays may show apparent lysis due to graft resorption during creeping substitution - this is normal healing, not recurrence. Key differences: (1) Timing - normal resorption occurs at 6-12 weeks, recurrence typically after 6 months; (2) Pattern - normal resorption is diffuse throughout graft, recurrence is focal lucency; (3) Stability - normal resorption stabilizes then remodels, recurrence progressively enlarges; (4) Symptoms - normal healing is painless, recurrence may cause pain. When in doubt, MRI or biopsy to distinguish.
Prognosis and Outcomes
Overall Prognosis - Excellent
CMF is a benign tumor with excellent prognosis. There are no cases of metastasis, and malignant transformation is exceedingly rare (likely representing misdiagnosis). The primary concern is local recurrence, which can be managed with repeat curettage or wide excision without impact on survival.
Factors Affecting Recurrence Risk
- Low Risk (under 10%)
- Extended curettage with adjuvant
- High Risk (over 25%)
- Simple curettage alone
- Low Risk (under 10%)
- Cryotherapy or PMMA
- High Risk (over 25%)
- No adjuvant
- Low Risk (under 10%)
- Expendable bones (fibula, rib)
- High Risk (over 25%)
- Complex anatomy (pelvis, spine)
- Low Risk (under 10%)
- Under 3cm diameter
- High Risk (over 25%)
- Over 5cm diameter
- Low Risk (under 10%)
- Intact cortex with window
- High Risk (over 25%)
- Pathological fracture, extensive destruction
Functional Outcomes
- Upper extremity: Near-normal function after healing
- Fibula: No functional deficit if peroneal nerve preserved
- Small lesions: Full return to pre-morbid activity level
- Young patients: Excellent bone remodeling and adaptation
- Large metaphyseal lesions: May have residual stiffness or weakness
- Pathological fracture: Prolonged recovery, possible chronic pain
- Multiple recurrences: Cumulative surgical morbidity
- Wide excision: Loss of bone, reconstruction-related issues
Long-Term Studies and Evidence
Limited long-term studies exist due to rarity of CMF, but available evidence shows:
- 10-year tumor-free survival: 90-95% with curettage and adjuvant
- Functional scores: MSTS (Musculoskeletal Tumor Society) scores average 25-28/30 (excellent)
- Return to sport: Most patients return to pre-injury activity level by 6-12 months
- Quality of life: Comparable to general population after successful treatment
Largest Clinicopathologic Series (Mayo Clinic, 278 cases)
- Largest single-institution series; slight male predominance, peak in the second decade
- Almost half involved long bones; ilium and small bones also common sites
- Eccentric metaphyseal lucent lesion with thinned, expanded cortex; soft-tissue extension uncommon
- Approximately one quarter of patients developed local recurrence after conservative surgical removal
Treatment Experience at the Istituto Ortopedico Rizzoli
- Surgical series correlating treatment modality (curettage vs resection) with local recurrence
- Recurrence concentrated in lesions treated by intralesional curettage alone
- Marginal/wide excision associated with lower recurrence than simple curettage
- Supports extended curettage with adjuvants or marginal excision over intralesional curettage alone
Guidelines, Registries & Global Practice
Global Epidemiology
Chondromyxoid fibroma is genuinely rare worldwide. According to PubMed, in the Mayo Clinic series of 278 cases (Wu CT et al., Hum Pathol 1998 — DOI) CMF accounted for well under 1% of all primary bone tumours, with a slight male predominance and a peak in the second decade. Almost half of lesions arose in the long bones (classically around the knee), with the ilium and the small bones of the hands and feet as other characteristic sites. These distribution and demographic patterns are consistent across North American, European (Rizzoli — Gherlinzoni F et al., J Bone Joint Surg Am 1983 — DOI) and other international series, so the same diagnostic and surgical principles apply globally rather than being region-specific.
Because any individual surgeon sees very few cases, the single most important global practice point is referral to a specialist bone-and-soft-tissue sarcoma/musculoskeletal oncology centre before biopsy or definitive surgery. This mirrors the principle behind national sarcoma networks (e.g. UK sarcoma "diagnostic and treatment" centres under NICE NG10/IOG guidance, US NCCN-affiliated sarcoma centres, and ISG/EORTC referral pathways in Europe).
Guidelines and Standards — Side-by-Side
CMF is too rare to have a dedicated single-disease guideline; it is managed within broader bone-tumour/sarcoma frameworks. The table summarises how the major bodies converge on the same core message — refer, biopsy correctly, avoid radiotherapy.
- Relevant Guidance
- NG10 / Improving Outcomes for Sarcoma (IOG)
- Position Relevant to CMF
- Suspected bone tumours referred to a designated bone sarcoma centre; biopsy only at the treating centre
- Evidence Basis
- Guideline / expert consensus
- Relevant Guidance
- BOAST: Suspected bone tumour & metastatic bone disease
- Position Relevant to CMF
- Do not perform definitive surgery or biopsy a likely primary bone tumour outside a specialist unit
- Evidence Basis
- Standard of care / consensus
- Relevant Guidance
- Bone sarcoma clinical practice guidelines
- Position Relevant to CMF
- Multidisciplinary diagnosis; image-guided core biopsy planned with the surgeon; expert bone pathology review
- Evidence Basis
- Level III-IV, expert consensus
- Relevant Guidance
- Bone Cancer guidelines (benign/borderline pathways)
- Position Relevant to CMF
- Curettage with adjuvants for benign aggressive lesions; wide excision reserved for diagnostic doubt
- Evidence Basis
- Category 2A consensus
- Relevant Guidance
- Classification of Tumours: Soft Tissue and Bone, 5th ed (2020)
- Position Relevant to CMF
- CMF defined as a benign cartilaginous tumour; GRM1 rearrangement now recognised as the molecular hallmark
- Evidence Basis
- Reference standard
Across all frameworks, radiotherapy is not recommended for CMF. The Zillmer & Dorfman series (Hum Pathol 1989 — DOI) documented a radiation-associated sarcoma arising after irradiation of a benign CMF. Radiotherapy is reserved only for genuinely unresectable lesions in critical locations after multidisciplinary discussion.
Registry and Practice Variation
- No dedicated CMF registry exists in any country; arthroplasty registries (NJR, AJRR, AOANJRR, SHAR, NZJR) do not capture primary benign bone tumours
- Epidemiology is therefore derived from single-institution pathology archives (Mayo Clinic, Rizzoli, Memorial Sloan Kettering) and national bone-tumour databases
- Recommendation: enter cases into local/national bone-tumour or rare-cancer registries to improve population-level data
- Adjuvant choice varies by availability: phenol and high-speed burr near-universal; cryotherapy and argon-beam more common in well-resourced units
- Observation of small asymptomatic lesions is emerging but not yet standard (Butler Z et al., Cureus 2026 — DOI)
- GRM1 IHC/FISH access varies; where available it materially reduces CMF-versus-chondrosarcoma misdiagnosis
Perioperative Medication Principles (Generic, Globally Applicable)
- Multimodal analgesia: paracetamol plus short-course opioid as required
- Avoid NSAIDs during the bone-healing phase (first ~6 weeks) where graft incorporation is required
- Use locally available agents per national formularies
- Single-dose first-generation cephalosporin (e.g. cefazolin) at induction is the international standard for clean orthopaedic surgery
- Follow local antimicrobial stewardship guidelines for choice and duration
- Consider antibiotic-loaded cement/graft for larger reconstructions per unit protocol
Return to Function (Surgery-Driven, Not Jurisdiction-Driven)
Return-to-activity timelines depend on reconstruction type and weight-bearing status rather than any specific health or compensation system:
- Sedentary work / desk-based activity: approximately 2-4 weeks (upper limb), 6-8 weeks (lower limb)
- Light manual work: approximately 6-12 weeks, guided by radiographic graft incorporation
- Heavy manual / impact loading: approximately 3-6 months, after radiographic union and adequate graft incorporation
MCQ Practice Points
High-Yield MCQ Topics
- Rarest benign cartilage tumor (under 1% of bone tumors)
- Peak age 10-30 years (slightly older than chondroblastoma)
- Male predominance 2:1
- Most common site: proximal tibia (25-30%)
- Classic triad: eccentric metaphyseal, scalloped margin, sclerotic rim
- Very high T2 signal on MRI (myxoid matrix)
- Minimal or absent calcification (unlike enchondroma)
- Cannot distinguish from chondrosarcoma on imaging alone
- Lobular architecture with fibrous septa (pathognomonic)
- Hypocellular myxoid center, hypercellular periphery
- S100 positive, low Ki-67 (under 5%)
- Reverse pattern compared to chondrosarcoma
- Standard: curettage with adjuvant (phenol, cryo, or PMMA)
- Recurrence: 25% without adjuvant, 10-15% with adjuvant
- Wide excision for recurrent or expendable bones
- Prognosis: excellent, no metastases
Classic Exam Vignettes
"A 22-year-old male presents with knee pain. X-ray shows an eccentric, lytic lesion in the proximal tibia with endosteal scalloping and sclerotic rim. Biopsy shows lobules with myxoid matrix and hypercellular periphery. What is the diagnosis?"Answer: Chondromyxoid fibroma (lobular architecture with myxoid matrix is pathognomonic)
"Which feature BEST distinguishes chondromyxoid fibroma from chondroblastoma?"Answer: Chondroblastoma is epiphyseal/apophyseal, CMF is metaphyseal (or: chondroblastoma has chicken-wire calcification, CMF has myxoid matrix)
"What is the recurrence rate after simple curettage alone for CMF?"Answer: 25-30% (versus 10-15% with adjuvant)
"Core needle biopsy of a proximal tibial lesion shows hypercellular cartilaginous tissue. The pathologist is concerned about chondrosarcoma. What feature would favor CMF?"Answer: Lobular architecture with hypocellular myxoid centers (CMF has reverse pattern - hypocellular center, hypercellular periphery; chondrosarcoma has permeative pattern with nuclear atypia throughout)
"A 25-year-old has an eccentric metaphyseal lesion with very high T2 signal on MRI. Differential diagnosis includes CMF and low-grade chondrosarcoma. Which clinical feature most favors CMF?"Answer: Age under 30 years (chondrosarcoma typically over 40 years)
Common Examiner Questions
-
Why is CMF easily misdiagnosed as chondrosarcoma?
- Hypercellular peripheral zones can mimic malignancy on small biopsies
- Both show high T2 signal on MRI
- Expert pathology review essential
-
What is the significance of the lobular architecture?
- Pathognomonic feature of CMF
- Lobules separated by fibrous septa
- Central myxoid zone, peripheral hypercellular zone
-
How do you reduce recurrence risk?
- Extended curettage (not simple curettage)
- High-speed burr to remove 1-2mm of cavity walls
- Local adjuvant (phenol, cryotherapy, or PMMA)
- Complete filling of defect with bone graft
-
When would you recommend wide excision over curettage?
- Recurrent disease (especially second recurrence)
- Expendable bone (fibula, rib)
- Diagnostic uncertainty with concern for chondrosarcoma
- Patient preference for lower recurrence risk
-
What is the prognosis?
- Excellent (benign tumor)
- 100% 5-year survival
- No metastatic potential
- Recurrence does not affect survival
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old male presents with a 6-month history of mild knee pain. X-ray shows an eccentric, lytic lesion in the proximal tibial metaphysis with endosteal scalloping and a sclerotic rim. MRI demonstrates a lobulated mass with very high T2 signal and cortical thinning without breakthrough. Describe your approach.”
“A 28-year-old female presents with deep pelvic pain. CT shows a 6cm expansile, lytic lesion in the iliac wing with cortical thinning and minimal internal calcification. Core needle biopsy shows hypercellular cartilaginous tissue with focal myxoid areas. The reporting pathologist suggests 'low-grade chondrosarcoma cannot be excluded.' How do you proceed?”
“A 25-year-old returns 18 months after extended curettage (with phenol and bone grafting) for proximal tibial CMF. He reports new onset of pain and swelling. X-ray shows a lucent area in the previously grafted site with loss of trabecular pattern. MRI demonstrates a 3cm lobulated mass with high T2 signal in the proximal tibia metaphysis. How do you manage this recurrence?”
Key Epidemiology
- **Rarest benign cartilage tumor** - under 1% of all bone tumors
- Peak age **10-30 years**, male:female 2:1
- **Proximal tibia 25-30%**, distal femur 15%, pelvis 15%
- Metaphyseal location (eccentric, cortical-based)
Classic Imaging Triad
- **Eccentric metaphyseal** location
- **Endosteal scalloping** with cortical expansion
- **Sclerotic rim** at margins (benign feature)
- MRI: very high T2 signal (myxoid matrix), lobulated
Pathognomonic Histology
- **Lobular architecture** with fibrous septa separating lobules
- **Myxoid matrix** centrally in lobules (hypocellular)
- **Hypercellular periphery** with spindle cells, giant cells
- **S100 positive**, Ki-67 under 5%, no nuclear atypia
Key Differentials
- **Chondroblastoma**: epiphyseal, younger age (10-20), chicken-wire calcification
- **Low-grade chondrosarcoma**: older age (over 40), permeative pattern, true atypia
- **Enchondroma**: central medullary, ring-and-arc calcification
- **ABC**: fluid-fluid levels, blood-filled spaces, no lobules
Standard Treatment
- **Extended curettage** with cortical window
- **High-speed burr** to remove 1-2mm of cavity walls
- **Local adjuvant**: phenol (most common), cryotherapy (lowest recurrence), or PMMA
- **Bone grafting**: cancellous autograft or allograft chips
Recurrence and Outcomes
- **25-30% recurrence** after curettage alone
- **10-15% recurrence** with curettage plus adjuvant
- **Under 5% recurrence** after wide excision
- **Excellent prognosis**: no metastases, 100% survival
Management of Recurrence
- **Always biopsy** to confirm and rule out malignancy
- **First recurrence**: repeat curettage with different adjuvant (e.g., cryotherapy)
- **Second recurrence**: strong consideration for wide excision
- **Prophylactic fixation** if cryotherapy used in weight-bearing bone
Exam Pearls
- **Most important distinction**: CMF vs low-grade chondrosarcoma (requires expert pathology)
- **Lobular pattern is pathognomonic** - fibrous septa, myxoid centers
- **Reverse cellular pattern**: hypocellular center, hypercellular periphery (opposite of chondrosarcoma)
- **Cannot diagnose on imaging alone** - biopsy mandatory despite typical appearance
Evidence Base and Guidelines
Characteristic Radiographic Appearance (38 cases + literature review)
- CMF has a characteristic but not specific radiographic appearance and often mimics commoner tumours
- Can occur anywhere in the skeleton, but almost half of cases occur around the knee
- Consider CMF for a focal lesion with geographic bone destruction, sclerotic rim, lobulated margins and septation
- Diagnosis most likely when the patient is in the second decade of life
Clinicopathologic Correlation Including Aggressive Variants (36 cases)
- Long-bone lesions appeared benign radiographically; vertebral lesions showed aggressive bone destruction
- Pseudolobulated tumour with myxoid and chondroid regions; cells occasionally bizarre/binucleate but rarely mitotic
- Majority of recurrences occurred in patients treated by curettage alone
- No malignant transformation; one radiation-associated sarcoma, cautioning against radiotherapy
GRM1 Immunohistochemistry Distinguishes CMF From Mimics
- GRM1 immunohistochemistry positive in 97% of CMF specimens (34/35), usually diffuse
- GRM1 negative in chondrosarcoma, enchondroma, chondroblastoma, GCT, fibrous dysplasia and other mimics
- Acid decalcification can reduce staining intensity - interpret with care
- Serves as a sensitive surrogate marker for the defining GRM1 gene rearrangement
Molecular Basis: GRM1 Gene Rearrangement
- GRM1 (metabotropic glutamate receptor 1) is recurrently rearranged and up-regulated in CMF via promoter swapping
- GRM1 break-apart FISH detected rearrangement in ~75% of testable cases (9/12)
- GRM1 protein overexpression by immunohistochemistry detected in 13/13 cases - the most sensitive method
- Targeted RNA sequencing did not reliably detect the fusion, so it is not yet a standalone diagnostic test
Contemporary Treatment Outcomes and Role of Observation
- Eight patients managed by en bloc resection (n=2), intralesional curettage with adjuvants (n=4) or serial imaging (n=2)
- All surgically treated patients remained free of local recurrence
- Two en bloc resections (25%) had complications requiring revision arthroplasty
- First report to document successful non-operative management with serial imaging in selected asymptomatic patients
Expert Recommendations and Guidelines
The WHO Soft Tissue and Bone Tumour Classification and Musculoskeletal Tumor Society guidelines recommend:
- Diagnosis: Image-guided biopsy with expert musculoskeletal pathology review
- Standard treatment: Extended intralesional curettage with local adjuvant and bone grafting
- Adjuvant selection: Phenol or cryotherapy based on surgeon preference and location
- Wide excision: Reserved for recurrent disease, expendable bones, or diagnostic uncertainty
- Surveillance: Serial imaging every 3-6 months for 2 years, then annually for 5 years
Controversial Areas and Research Needs
- Optimal adjuvant (phenol vs cryotherapy vs PMMA)
- Role of denosumab or bisphosphonates as adjuvants
- Genetic markers to predict recurrence risk
- Long-term outcomes (over 20 years) data lacking
- Molecular characterization (identify driver mutations)
- Less invasive techniques (radiofrequency ablation, MRI-guided focused ultrasound)
- Targeted therapies if molecular targets identified
- International registry for rare tumor outcomes tracking
References
-
Jaffe HL, Lichtenstein L. Chondromyxoid fibroma of bone: a distinctive benign tumor likely to be mistaken especially for chondrosarcoma. Arch Pathol. 1948;45:541-551.
-
Wu CT, Inwards CY, O'Laughlin S, et al. Chondromyxoid fibroma of bone: a clinicopathologic review of 278 cases. Hum Pathol. 1998;29(5):438-446. PMID:9596266. doi:10.1016/s0046-8177(98)90058-2
-
Rahimi A, Beabout JW, Ivins JC, Dahlin DC. Chondromyxoid fibroma: a clinicopathologic study of 76 cases. Cancer. 1972;30(3):726-736.
-
Gherlinzoni F, Rock M, Picci P. Chondromyxoid fibroma. The experience at the Istituto Ortopedico Rizzoli. J Bone Joint Surg Am. 1983;65(2):198-204. PMID:6337162. doi:10.2106/00004623-198365020-00008
-
Wilson AJ, Kyriakos M, Ackerman LV. Chondromyxoid fibroma: radiographic appearance in 38 cases and in a review of the literature. Radiology. 1991;179(2):513-518. PMID:2014302. doi:10.1148/radiology.179.2.2014302
-
Schajowicz F, Gallardo H. Chondromyxoid fibroma (fibromyxoid chondroma) of bone. A clinico-pathological study of thirty-two cases. J Bone Joint Surg Br. 1971;53(2):198-216.
-
Zillmer DA, Dorfman HD. Chondromyxoid fibroma of bone: thirty-six cases with clinicopathologic correlation. Hum Pathol. 1989;20(10):952-964. PMID:2793160. doi:10.1016/0046-8177(89)90267-0
-
WHO Classification of Tumours Editorial Board. Soft Tissue and Bone Tumours. 5th ed. Lyon: International Agency for Research on Cancer; 2020.
-
Xu H, Nugent D, Monforte HL, et al. Chondromyxoid fibroma of bone: a retrospective study of 107 cases. Clin Orthop Relat Res. 2015;473(3):1097-1104. doi:10.1007/s11999-014-4066-7
-
Marcove RC, Kambolis C, Bullough PG, Jaffe HL. Fibromyxoma of bone. A report of 23 cases. Clin Orthop Relat Res. 1976;(118):156-162.
-
Bloem JL, Mulder JD. Chondromyxoid fibroma: a clinical and radiological study of 76 cases. Skeletal Radiol. 1985;14(1):7-13. doi:10.1007/bf00361194
-
Springfield DS, Rosenberg AE, Mankin HJ, Mindell ER. Relationship between osteofibrous dysplasia and adamantinoma. Clin Orthop Relat Res. 1994;(309):234-244.
-
Huvos AG. Bone Tumors: Diagnosis, Treatment, and Prognosis. 2nd ed. Philadelphia: WB Saunders; 1991:283-294.
-
Unni KK, Inwards CY. Dahlin's Bone Tumors: General Aspects and Data on 10,165 Cases. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2010:91-98.
-
Murphey MD, Walker EA, Wilson AJ, Kransdorf MJ, Temple HT, Gannon FH. From the archives of the AFIP: imaging of primary chondrosarcoma: radiologic-pathologic correlation. Radiographics. 2003;23(5):1245-1278. doi:10.1148/rg.235035134
-
Kilpatrick SE, Wenger DE, Gilchrist GS, et al. Langerhans' cell histiocytosis (histiocytosis X) of bone. A clinicopathologic analysis of 263 pediatric and adult cases. Cancer. 1995;76(12):2471-2484.
-
Bertoni F, Unni KK, Beabout JW, Sim FH. Chondrosarcomas of the synovium. Cancer. 1991;67(1):155-162.
-
Fletcher CDM, Bridge JA, Hogendoorn PCW, Mertens F, eds. WHO Classification of Tumours of Soft Tissue and Bone. 4th ed. Lyon: IARC Press; 2013.
-
Douis H, Saifuddin A. The imaging of cartilaginous bone tumours. I. Benign lesions. Skeletal Radiol. 2012;41(10):1195-1212. doi:10.1007/s00256-012-1427-0
-
Giudici MA, Moser RP Jr, Kransdorf MJ. Cartilaginous bone tumors. Radiol Clin North Am. 1993;31(2):237-259.