Chronic, length-dependent peripheral nerve damage from prolonged hyperglycaemia that produces irreversible loss of protective sensation and drives ulceration, Charcot arthropathy and amputation.
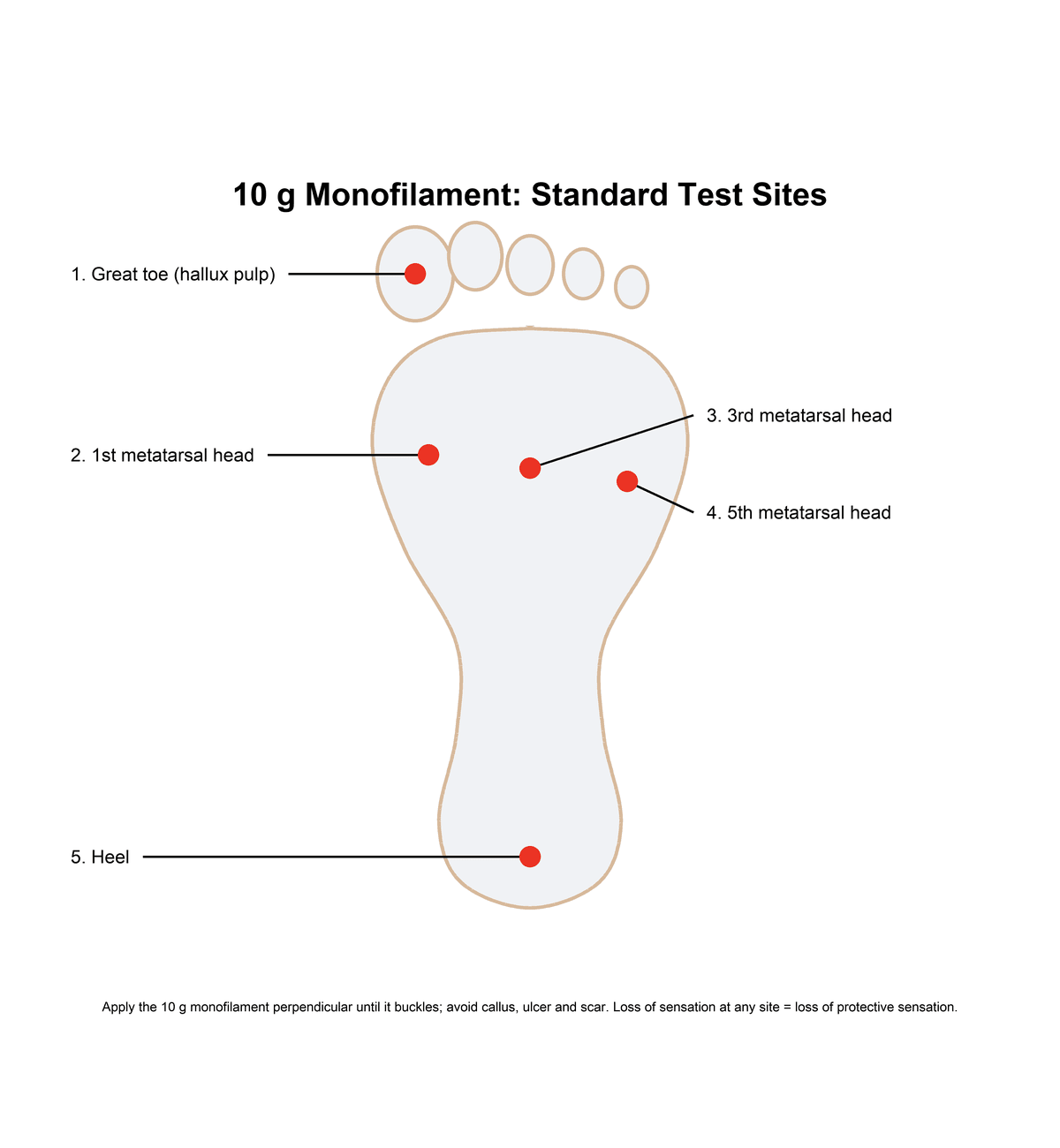
- Screen annually with the 10g Semmes-Weinstein monofilament at 5 plantar sites (1-1-3-5-H) - inability to feel at ANY site equals loss of protective sensation and a 4-7 fold ulcer risk.
- Charcot is hot, swollen and PAINLESS - immobilise in a total contact cast the same day; plain X-rays can be normal in Eichenholtz stage 0, so MRI and skin thermometry guide early diagnosis.
- Neuropathy is irreversible - tight glycaemic control (HbA1c under 7%) prevents progression and cuts risk by 60-70% but cannot restore lost nerve function; the goal is preventing ulcers, infection and amputation.
- “Painless neuropathy is the dangerous phenotype - no symptoms yet complete loss of protective sensation and the highest ulcer and Charcot risk.
- “Probe-to-bone has about 87% sensitivity for osteomyelitis in a diabetic foot ulcer.
- “The Ipswich Touch Test (lightly touch the tips of toes 1, 3 and 5) is the validated equipment-free screen when a monofilament is unavailable.
10g Semmes-Weinstein monofilament at 5 plantar sites (1st toe, 1st/3rd/5th MT heads, heel). Apply perpendicular until buckles, hold 1-2 seconds. Inability to feel at ANY site equals loss of protective sensation and 4-7 fold increased ulcer risk. This is the single most important screening test - MANDATORY annually for all diabetics.
Hot, swollen, PAINLESS foot in diabetic equals Charcot arthropathy until proven otherwise. Temperature difference greater than 2 degrees Celsius between feet is diagnostic. Requires IMMEDIATE total contact casting for minimum 3-6 months. Missed diagnosis leads to progressive fragmentation, rocker-bottom deformity, and recurrent ulceration. DO NOT misdiagnose as cellulitis or DVT.
Charcot arthropathy (acute immobilization critical), Ulceration (total contact cast offloading), Amputation (15-fold increased risk, 85% preceded by ulcer). All three are interconnected and largely preventable through annual screening, patient education, and appropriate footwear delivered within a structured multidisciplinary foot programme.
Established neuropathy is IRREVERSIBLE - nerve damage cannot be reversed even with perfect glycemic control. HbA1c target under 7% prevents progression (60-70% risk reduction) but does not restore lost sensation. Therefore, annual foot screening is MANDATORY for early detection and ulcer prevention, not neuropathy reversal.
Overview and Epidemiology
Diabetic peripheral neuropathy is chronic nerve damage resulting from prolonged hyperglycemia and microvascular complications affecting peripheral nerves. It represents the most common chronic complication of diabetes mellitus and the leading cause of non-traumatic lower extremity amputation in developed countries.
Definition and Clinical Significance
Diabetic neuropathy encompasses a heterogeneous group of nerve disorders, with distal symmetric polyneuropathy being the predominant pattern (95% of cases). The hallmark feature is loss of protective sensation in a stocking-glove distribution, which removes the protective pain response to repetitive trauma and pressure.
The clinical significance lies in three devastating complications:
- Foot ulceration (15-25% lifetime risk in diabetics)
- Charcot neuroarthropathy (0.5-2% of diabetics, progressive joint destruction)
- Lower extremity amputation (15-fold increased risk compared to non-diabetics)
While neuropathy is a medical condition, its orthopaedic consequences are devastating. Loss of protective sensation leads to repetitive microtrauma without pain, causing painless ulceration at pressure points. Motor neuropathy creates biomechanical deformities (claw toes, prominent metatarsal heads) that further increase plantar pressures. Autonomic dysfunction causes dry, cracked skin that serves as infection portal. Together, these create a perfect storm for limb-threatening complications.
Epidemiology
- 50% of diabetic patients develop peripheral neuropathy over their lifetime
- Prevalence increases with diabetes duration (25-year risk approaches 50%)
- Type 1 and Type 2 diabetes have similar long-term neuropathy rates
- Only 20-30% have painful symptoms - majority are painless and more dangerous
- Symptomatic neuropathy affects 10-15% of diabetics at diagnosis
- 60-70% of diabetic foot ulcers have neuropathic component
- Neuropathy present in 80-90% of patients requiring amputation
- 85% of amputations are preceded by preventable foot ulcer
- Leading cause of diabetes-related hospitalization in developed countries
- Economic burden exceeds 10 billion dollars annually in healthcare costs
- 15-fold increased amputation risk compared to non-diabetics
- 50% 5-year mortality following major amputation (worse than many cancers)
- 50% develop contralateral limb ulcer within 5 years of first amputation
- Indigenous populations have 6-fold higher amputation rates
Risk Factors for Neuropathy Development
- Duration of diabetes (strongest predictor)
- Increasing age (cumulative nerve damage)
- Male sex (slightly higher prevalence)
- Height (taller patients have longer nerves at risk)
- Genetic susceptibility (aldose reductase polymorphisms)
- Poor glycemic control (HbA1c greater than 7% - PRIMARY risk factor)
- Smoking (accelerates microvascular damage)
- Hypertension (additional vascular compromise)
- Hyperlipidemia (contributes to nerve ischemia)
- Obesity (insulin resistance, metabolic syndrome)
- Alcohol abuse (direct neurotoxicity)
Every diabetic patient MUST have annual comprehensive foot examination including monofilament testing, pulse examination, and skin inspection. Loss of protective sensation on monofilament testing identifies high-risk patients requiring intensive podiatry management and protective footwear. Structured screening with risk stratification underpins all international guidance (IWGDF, NICE, ADA) and, as part of a multidisciplinary foot service, is associated with reduced amputation rates.
Pathophysiology
Mechanisms of Nerve Damage
Diabetic neuropathy results from multiple interconnected pathophysiologic mechanisms triggered by chronic hyperglycemia. Understanding these pathways explains why tight glycemic control is the only disease-modifying intervention.
1. Metabolic Pathway - Polyol Accumulation
The polyol pathway becomes activated when intracellular glucose concentrations exceed the capacity of normal glycolytic metabolism:
- Aldose reductase enzyme converts excess glucose to sorbitol in nerve cells
- Sorbitol accumulation causes osmotic stress (sorbitol cannot cross cell membranes)
- Depletion of myoinositol and taurine (osmotic pressure draws out essential metabolites)
- Reduced Na-K-ATPase activity impairs nerve membrane potential
- Progressive axonal swelling and eventual degeneration
This pathway explains why intensive glycemic control reduces neuropathy risk by 60-70% - reducing glucose availability prevents polyol pathway activation.
2. Microvascular Pathway - Nerve Ischemia
Chronic hyperglycemia damages the vasa nervorum (blood supply to peripheral nerves):
- Basement membrane thickening of endoneurial capillaries
- Endothelial dysfunction reduces nitric oxide production
- Arteriovenous shunting diverts blood away from nerve capillaries
- Reduced endoneurial blood flow causes chronic nerve hypoxia
- Progressive axonal degeneration from ischemia
Nerve biopsies in diabetic neuropathy demonstrate thickened capillary basement membranes and reduced capillary density in peripheral nerves.
3. Advanced Glycation End Products (AGEs)
Non-enzymatic glycation of nerve proteins creates irreversible damage:
- Glucose binds to amino groups on nerve structural proteins
- Forms irreversible cross-links (AGEs) that accumulate over time
- Impairs nerve structure and function (myelin, neurofilaments, tubulin)
- Triggers inflammatory cascade through RAGE receptors
- Generates reactive oxygen species (oxidative stress)
This mechanism explains why neuropathy is irreversible - AGE accumulation cannot be reversed even with perfect subsequent glycemic control.
4. Oxidative Stress
Chronic hyperglycemia generates free radicals that overwhelm antioxidant defenses:
- Superoxide production from mitochondrial glucose metabolism
- Overwhelms endogenous antioxidants (glutathione, superoxide dismutase)
- Direct nerve membrane lipid peroxidation
- DNA damage in dorsal root ganglion neurons
- Activates inflammatory pathways (NF-kB, protein kinase C)
Pattern of Nerve Fiber Loss
Diabetic neuropathy follows a predictable pattern of fiber loss that explains the clinical progression:
- Unmyelinated C-fibers (pain and temperature sensation) affected first
- Patients report burning pain, hyperesthesia, allodynia
- Loss of temperature discrimination
- Painless injuries as pain fibers degenerate
- May have years of symptoms before large fiber involvement
- Myelinated A-beta fibers (vibration, proprioception, light touch) affected
- Loss of vibration sense (128 Hz tuning fork)
- Impaired proprioception (joint position sense)
- Loss of protective sensation (critical threshold for ulceration)
- Areflexia (ankle reflexes lost)
- "Dying back" neuropathy - longest nerves affected first
- Explains stocking-glove distribution (feet before hands)
- Toes affected before forefoot, forefoot before ankle
- Upper limbs involved only after significant lower limb disease
Motor and Autonomic Involvement
Motor Fiber Degeneration:
Intrinsic foot muscle denervation creates biomechanical derangement:
- Lumbricals and interossei weaken and atrophy
- Loss of flexion at MTP joints, extension at IP joints
- Extrinsic muscles (long flexors, extensors) remain strong
- Imbalance creates claw toe deformity (MTP hyperextension, IP flexion)
- Prominent metatarsal heads from loss of fat pad protection
- Increased plantar pressures (3-4 times normal at MT heads)
- Creates ulceration risk at pressure points
Autonomic Fiber Dysfunction:
Autonomic denervation affects skin integrity and temperature regulation:
- Loss of sudomotor function (sweat glands denervated)
- Dry, anhidrotic skin prone to fissuring
- Fissures serve as infection portals (penetrate to deep tissues)
- Arteriovenous shunting creates warm foot despite neuropathy
- Paradoxically warm foot in neuropathy versus cool foot in ischemia
- Loss of vasomotor control affects wound healing
Biomechanical Consequences
The combination of sensory, motor, and autonomic dysfunction creates a cascade of biomechanical problems:
- Cannot detect minor trauma (foreign objects in shoes, blisters, cuts)
- Repetitive microtrauma accumulates without pain signal
- No protective withdrawal reflex from excessive pressure
- Painless ulceration develops at high-pressure areas
- Threshold for ulceration: inability to feel 10g monofilament
- Intrinsic muscle wasting creates claw toe posture
- Loss of metatarsal fat pad (moves distally with toe clawing)
- Increased plantar pressures at metatarsal heads (3-4 times normal)
- Pressure redistribution to areas of bony prominence
- Callus formation at pressure points (further increases local pressure)
- Non-enzymatic glycosylation of collagen in joint capsules and ligaments
- Stiffening of joints (positive prayer sign in hands)
- Reduced ankle dorsiflexion (equinus contracture)
- Increased forefoot loading during gait
- Higher plantar pressures at metatarsal heads
Once established, diabetic neuropathy is IRREVERSIBLE because of AGE (Advanced Glycation End Product) accumulation and nerve fiber loss. Tight glycemic control prevents progression and reduces risk by 60-70%, but cannot restore lost nerve function. This is why annual screening is critical - we cannot reverse neuropathy, but we can prevent its devastating complications (ulcers, Charcot, amputation) through early detection and protective measures.
Classification Systems
Types of Diabetic Neuropathy
1. Symmetric Polyneuropathy (95% of cases)
- MOST COMMON TYPE - what we mean when we say diabetic neuropathy
- Stocking-glove distribution (feet affected first, hands later)
- Distal to proximal progression (dying back neuropathy)
- Length-dependent (longest nerves affected first)
- Mixed sensory and motor involvement
- Clinically most important for orthopaedic complications
- Loss of vibration sense (128 Hz tuning fork)
- Loss of protective sensation (10g monofilament)
- Reduced pain and temperature discrimination
- Intrinsic muscle wasting (claw toes)
- Ankle areflexia (Achilles reflex lost early)
- May be painless (more dangerous) or painful (burning, shooting)
2. Autonomic Neuropathy (50% of cases)
Affects autonomic nerve fibers controlling non-voluntary functions:
- Loss of sweating (anhidrosis) in feet
- Dry, cracked skin prone to fissuring
- Fissures serve as infection portals
- Contributes to ulceration risk
- Arteriovenous shunting
- Warm foot despite neuropathy
- Bone blood flow alterations (may predispose to Charcot)
- Resting tachycardia
- Orthostatic hypotension
- Perioperative risk factor
3. Focal Neuropathy (5-10% of cases)
Single nerve involvement, often with acute onset:
- Carpal tunnel syndrome (median nerve) - MOST COMMON focal neuropathy
- Ulnar nerve entrapment (cubital tunnel)
- Radial nerve palsy (rare)
- Tarsal tunnel syndrome (tibial nerve behind medial malleolus)
- Peroneal nerve palsy (foot drop)
- Femoral neuropathy (diabetic amyotrophy)
- III, IV, VI (extraocular muscles - diplopia)
- VII (facial nerve - Bell's palsy)
4. Motor Neuropathy
Usually occurs in context of sensorimotor polyneuropathy:
- Lumbricals and interossei atrophy
- First dorsal interosseous wasting (visible on examination)
- Inability to spread toes (interossei weakness)
- Toe extension weakness
- Claw toe deformity (MTP hyperextension, IP flexion)
- Hammer toe deformity (PIP flexion)
- Loss of metatarsal fat pad (moves distally)
- Prominent metatarsal heads (high-pressure ulceration risk)
- Increased plantar pressures (3-4 times normal)
- Acute painful proximal muscle weakness (thigh)
- Weight loss, severe pain
- Usually self-limiting over months
- Rare but dramatic presentation
This section provides comprehensive classification coverage for the exam.
Clinical Assessment
History Taking
- Burning pain (worse at night, disturbs sleep)
- Shooting, lancinating pain (electric shock-like)
- Tingling, pins and needles (paresthesias)
- Hyperesthesia (exaggerated response to stimuli)
- Allodynia (pain from normally non-painful stimuli - bedsheets touching feet)
- Numbness (most common presentation)
- "Walking on cotton wool" or "feet feel dead"
- Loss of temperature sensation
- Painless injuries - noticed cuts, burns, blisters only visually
- Unaware of foot injuries until see blood in shoe
Patients with painful neuropathy often present early for treatment but have preserved protective sensation. Those with painless neuropathy (majority) do not report symptoms, have complete loss of protective sensation, and are at HIGHEST risk for ulceration and Charcot. This is why screening cannot rely on symptoms alone - must actively test with monofilament.
- History of foot ulceration (previous or current)
- Foot deformity awareness
- Difficulty with balance, falls (proprioceptive loss)
- Erectile dysfunction (autonomic - men may volunteer this)
- Gastrointestinal symptoms (gastroparesis, diarrhea - autonomic)
- Diabetes duration (longer equals higher risk)
- Glycemic control history (HbA1c values)
- Previous foot complications (ulcer, infection, Charcot)
- Smoking status (modifiable risk)
- Comorbidities (hypertension, hyperlipidemia, renal disease)
Physical Examination
Step 1: Inspection (Visual Assessment)
- Dry, cracked skin (autonomic neuropathy - anhidrosis)
- Callus formation (indicates high-pressure areas at risk for ulceration)
- Fissures (serve as infection portals - check between toes)
- Previous or current ulceration (plantar surface, pressure points)
- Trophic skin changes (thin, shiny, hairless)
- Color: Warm, pink foot (arteriovenous shunting in neuropathy)
- Claw toes (MTP hyperextension, IP flexion from intrinsic weakness)
- Hammer toes (PIP flexion contractures)
- Prominent metatarsal heads (loss of fat pad protection)
- High arch (pes cavus) or flatfoot (pes planus)
- Charcot foot (rocker-bottom deformity, medial column collapse)
- Intrinsic muscle wasting (first dorsal interosseous atrophy visible)
- Onychomycosis (fungal infection - common in diabetics)
- Ingrown toenails (risk for paronychia)
- Thickened, dystrophic nails (difficult self-care)
Step 2: Monofilament Testing (GOLD STANDARD)
10g Semmes-Weinstein Monofilament Test
- 5.07 gauge monofilament (buckles at 10g force)
- Tests ability to feel pressure that would normally prevent ulceration
- Single most important screening test
- Demonstrate on patient's hand (show what it feels like on dorsum of hand)
- Ask patient to close eyes (eliminates visual cues)
- Apply perpendicular to skin at each test site
- Press until monofilament buckles (10g force)
- Hold for 1-2 seconds (allows sensory processing)
- Ask "Can you feel this?" after each site
- Randomize sites (prevents pattern recognition)
- Do NOT apply over callus, ulcers, or scars (false negatives)
- Plantar aspect of great toe (distal phalanx, avoid nail)
- Plantar 1st metatarsal head (medial forefoot)
- Plantar 3rd metatarsal head (central forefoot - highest pressure)
- Plantar 5th metatarsal head (lateral forefoot)
- Plantar heel (midpoint, avoid thick callus)
- Normal: Can feel at all 5 sites (protective sensation intact)
- Loss of Protective Sensation: Cannot feel at 1 or more sites
- High Risk: Inability to feel at any site equals 4-7 fold increased ulcer risk
- Sensitivity 57-93% for neuropathy detection
- Specificity 75-100%
- Predicts ulcer risk with odds ratio 3.2-4.7
- Best validated bedside screening test
Ipswich Touch Test (Equipment-Free Screening Alternative)
The Ipswich Touch Test (IpTT) is a validated simplified screen for loss of protective sensation designed for use when a monofilament is unavailable or the examiner is a non-specialist (ward nurse, carer or the patient's relative performing self/assisted checks). It requires no equipment.
- Ask the patient to close their eyes and say "yes" when a touch is felt
- The examiner lightly rests the tip of the index finger on the tips of the 1st, 3rd and 5th toes of both feet, in sequence, for 1-2 seconds
- Do NOT push, prod or tap - it is a light static touch, not pressure or movement
- Six toes are tested in total (three per foot)
- Insensate at 2 or more of the 6 toes equals loss of protective sensation (a high-risk foot)
- IpTT shows good agreement with the 10g monofilament and with vibration perception threshold for identifying the at-risk foot
The IpTT does not replace the 10g monofilament in formal annual review, but it is an excellent adjunct and inpatient/community screen that empowers ward staff and families to detect the insensate foot and trigger protective measures.
If asked "how would you screen a diabetic foot when you have no monofilament?", the answer is the Ipswich Touch Test: lightly touch the tips of toes 1, 3 and 5 on each foot for 1-2 seconds (no pushing or tapping); 2 or more insensate toes out of 6 indicates loss of protective sensation. Its strengths are that it needs no equipment and can be taught to relatives and ward staff, making it ideal for inpatient and community case-finding alongside the monofilament gold standard.
Step 3: Additional Sensory Tests
- Strike tuning fork firmly
- Apply base to bony prominence (1st MT head or hallux IP joint)
- Ask patient when vibration stops
- Normal: Perceives vibration greater than 4/8 (of examiner's perception)
- Abnormal: Less than 4/8 predicts ulceration risk
- Large fiber function assessment
- Hold hallux by sides (avoid pressure cues)
- Move toe up/down with patient's eyes closed
- Ask patient to identify direction of movement
- Abnormal: Impaired proprioception indicates advanced neuropathy
- Achilles tendon reflex
- Typically absent in diabetic neuropathy (lost early)
- Non-specific finding but supports diagnosis
Step 4: Motor Examination
- First dorsal interosseous (visible wasting between 1st and 2nd MT)
- Inability to spread toes (interossei weakness)
- Inability to flex toes at MTP while extending IP (lumbrical weakness)
- Claw toe posture (fixed or flexible)
- Can patient extend IP joints actively?
- Assess for rigid contractures (may need surgical correction)
Step 5: Autonomic Testing
- Dry skin (anhidrosis) indicates autonomic dysfunction
- Lack of normal foot moisture
- Fissures from excessive dryness
- Warm foot suggests arteriovenous shunting (autonomic)
- Temperature difference between feet (if greater than 2 degrees Celsius, consider Charcot)
Step 6: Vascular Assessment
- Dorsalis pedis (dorsum of foot, first web space lateral to EHL tendon)
- Posterior tibial (behind medial malleolus)
- Grade: present (bounding/normal/weak) or absent
- Ratio of ankle to brachial systolic pressure
- Normal: 0.9-1.2
- Peripheral arterial disease: Less than 0.9
- Falsely elevated in diabetics: Greater than 1.3 (medial arterial calcification)
- CANNOT rely on ABPI alone in diabetics
- More accurate than ABPI in diabetics
- Toe vessels less affected by medial calcification
- Normal: Greater than 0.7
- PAD: Less than 0.7
- Critical ischemia: Less than 0.3
- Press toenail, release, count seconds to reperfusion
- Normal less than 2 seconds
- Prolonged suggests vascular insufficiency
Step 7: Footwear Assessment
Examine Patient's Current Shoes:
- Inappropriate footwear is a common contributor to diabetic ulcers
- Check for adequate toe box depth (accommodate claw toes)
- Width (avoid lateral pressure)
- Cushioning (reduce plantar pressure)
- Internal seams or rough areas (cause friction blisters)
- Inspect insoles for wear patterns (high-pressure areas)
Differential Diagnosis
Not every distal sensory disturbance in a person with diabetes is diabetic neuropathy, and not every hot swollen foot is Charcot. A length-dependent, symmetrical, predominantly sensory polyneuropathy with normal inflammatory markers favours diabetic peripheral neuropathy, but atypical features (asymmetry, rapid progression, motor predominance, proximal onset) should prompt a search for an alternative or coexistent cause.
- Distinguishing features
- Symmetrical, distal, length-dependent stocking-glove sensory loss; absent ankle reflexes
- Key discriminator
- Diabetes with typical pattern and no atypical red flags
- Distinguishing features
- Distal sensory loss plus dorsal-column signs; may have anaemia; metformin is a risk factor
- Key discriminator
- Low serum B12 / raised methylmalonic acid
- Distinguishing features
- Painful sensory neuropathy, alcohol history, often coexists with diabetes
- Key discriminator
- Alcohol history and thiamine status
- Distinguishing features
- Sensory neuropathy, may include carpal tunnel, other hypothyroid features
- Key discriminator
- Raised TSH
- Distinguishing features
- Motor-predominant, proximal and distal weakness, progressive over weeks
- Key discriminator
- Nerve conduction shows demyelination; raised CSF protein
- Distinguishing features
- Dermatomal/asymmetric sensory loss, back/leg pain, myotomal weakness
- Key discriminator
- Imaging and dermatomal pattern, not stocking distribution
- Distinguishing features
- Painful (rest pain), cool pale foot, absent pulses, dependent rubor
- Key discriminator
- Cool ischaemic foot versus warm neuropathic foot; low toe pressures
- Distinguishing features
- Hot, swollen, often painless foot; temperature difference greater than 2 degrees Celsius
- Key discriminator
- Neuropathy present, no wound portal; MRI marrow oedema
- Distinguishing features
- Hot, swollen, tender foot with systemic signs and a skin breach
- Key discriminator
- Pain, fever and raised inflammatory markers; usually a portal of entry
- Distinguishing features
- Acute monoarticular severe pain, often first MTP joint
- Key discriminator
- Severe pain, raised urate, crystals on aspiration
- Distinguishing features
- Unilateral calf and leg swelling, pain
- Key discriminator
- Doppler ultrasound; calf rather than forefoot focus
Investigations
Clinical Diagnosis
Diabetic neuropathy is primarily a CLINICAL diagnosis based on:
- History of diabetes with duration and control
- Symptoms (or lack of symptoms in painless neuropathy)
- Monofilament testing (loss of protective sensation)
- Exclusion of other causes (B12 deficiency, hypothyroidism, alcohol)
Investigations serve to:
- Confirm the diagnosis
- Exclude alternative diagnoses
- Assess glycemic control and cardiovascular risk
- Evaluate complications (osteomyelitis, Charcot)
Neurophysiology (Rarely Needed)
- Reduced conduction velocity (demyelination)
- Reduced amplitude (axonal loss)
- Confirms polyneuropathy pattern (length-dependent)
- Excludes focal entrapment (CTS, tarsal tunnel)
- NOT routinely needed for diagnosis in typical diabetic neuropathy
- Atypical presentation (acute onset, asymmetric, rapid progression)
- Proximal greater than distal involvement
- Suspected superimposed focal neuropathy
- Motor predominant neuropathy
- Thermal thresholds (warm, cool detection)
- Vibration perception thresholds
- Pressure pain thresholds
- Not used clinically (research and clinical trials only)
Metabolic and Hematologic Screen
- HbA1c (target less than 7% or 53 mmol per L for prevention)
- Reflects average glycemia over 3 months
- Fasting glucose (daily control assessment)
- Continuous glucose monitoring data if available
- Vitamin B12 level (metformin users at high risk for B12 deficiency)
- Thyroid function (TSH) - hypothyroidism causes neuropathy
- Serum protein electrophoresis (if atypical - exclude paraproteinemia)
- Folate level
- Renal function (creatinine, eGFR) - diabetic nephropathy common
- Lipid profile (cardiovascular risk stratification)
- Liver function (if considering certain medications)
- FBC (white cell count, neutrophilia)
- CRP (elevated in infection, Charcot)
- Blood cultures (if systemically unwell)
- Deep tissue swab or bone biopsy (for osteomyelitis - NOT superficial swab)
Vascular Studies
- ABPI measurement (unreliable in diabetics if greater than 1.3)
- Toe pressures (more accurate in diabetics)
- Toe-Brachial Index (TBI greater than 0.7 adequate, less than 0.7 PAD)
- Arterial waveform analysis (triphasic normal, biphasic/monophasic abnormal)
- Measures tissue oxygen availability
- Greater than 30 mmHg predicts healing
- Less than 30 mmHg impaired healing, consider revascularization
- Indicated if revascularization being considered
- Anatomical mapping for bypass or angioplasty planning
- Assesses inflow, target vessels, runoff
Imaging for Complications
- Current foot ulcer (exclude osteomyelitis)
- Hot, swollen foot (exclude Charcot)
- Foot deformity assessment
- AP, lateral, oblique foot (weight-bearing if possible)
- Ankle views if hindfoot Charcot suspected
- Osteomyelitis: Bone destruction, cortical erosion, periosteal reaction
- Charcot: Fragmentation (stage 1), coalescence (stage 2), consolidation (stage 3)
- Gas in soft tissues: Necrotizing infection (SURGICAL EMERGENCY)
- Deformity assessment (Meary's angle, talo-first MT angle)
- Suspected osteomyelitis (probe-to-bone positive)
- Early Charcot (stage 0 - X-ray normal)
- Pre-operative planning for Charcot reconstruction
- Differentiate soft tissue infection from bone involvement
- T1-weighted (anatomy, marrow signal)
- T2-weighted fat-suppressed or STIR (edema detection)
- T1 post-gadolinium (enhancement indicates infection/inflammation)
- Osteomyelitis: Marrow edema (T2 bright), cortical destruction, enhancement
- Charcot stage 0: Bone marrow edema, joint effusion, soft tissue edema
- Ulcer tracking: Depth of penetration, sinus tracts to bone
- Osteomyelitis: Sensitivity 90%, Specificity 80%
- Superior to plain X-rays for early detection
- Sensitive but NOT specific (infection and Charcot both show uptake)
- Cannot differentiate osteomyelitis from Charcot
- Rarely used now (MRI superior)
- More specific for infection
- Combined with bone scan (triple-phase)
- Still less accurate than MRI in diabetic foot
The probe-to-bone test is the most practical bedside investigation for osteomyelitis. Insert sterile probe through ulcer base - if hard bone contacted, sensitivity 87%, specificity 83% for osteomyelitis. Positive test mandates MRI confirmation and 6-12 weeks antibiotics. More practical than X-ray (which may be normal early) and available immediately in clinic.

Medical Management
Pharmacological Management of Painful Neuropathy
Only 20-30% of patients with diabetic neuropathy experience pain. When present, it significantly impacts quality of life and sleep. Treatment focuses on symptom control as nerve damage is irreversible.
First-Line Agents
1. Tricyclic Antidepressants (TCAs)
Amitriptyline (most evidence):
- Starting dose: 10-25 mg nocte (start low in elderly)
- Titration: Increase by 10-25 mg weekly
- Target dose: 75-150 mg nocte (therapeutic range)
- Number Needed to Treat (NNT): 3-4 (excellent efficacy)
- Onset: 2-4 weeks for pain relief
Inhibits reuptake of serotonin and norepinephrine, blocks sodium channels
- Dry mouth, constipation (anticholinergic)
- Drowsiness (use nocte dosing - beneficial for sleep)
- Orthostatic hypotension (caution in elderly)
- Weight gain
- Urinary retention (caution in men with BPH)
- Recent MI or unstable angina
- Cardiac conduction defects (prolonged QT, bundle branch block)
- Severe liver disease
- Angle-closure glaucoma
Nortriptyline (fewer anticholinergic effects), Imipramine
2. Gabapentinoids
Pregabalin (Lyrica):
- Starting dose: 75 mg twice daily
- Titration: Increase to 150 mg BD after 1 week if tolerated
- Maximum: 300 mg BD (most patients respond at 150-300 mg BD)
- NNT: 5-7
- Onset: 1-2 weeks
Gabapentin (cheaper alternative):
- Starting dose: 300 mg nocte
- Titration: Increase to 300 mg TDS, then 600 mg TDS, up to 900 mg TDS
- Maximum: 3600 mg daily (divided TDS)
- NNT: 5-7
- Onset: 2-4 weeks
Binds alpha-2-delta subunit of voltage-gated calcium channels, reduces neurotransmitter release
- Dizziness, somnolence (dose at night initially)
- Peripheral edema
- Weight gain (common, warn patients)
- Gait instability (fall risk in elderly)
- No cardiac effects (safe in heart disease)
- Dose adjustmen in renal impairment needed (renally excreted)
3. Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)
Duloxetine (Cymbalta):
- Dose: 60 mg daily (can start 30 mg for tolerability)
- NNT: 5-6
- Onset: 2-4 weeks
- No titration needed (fixed dose)
Inhibits serotonin and norepinephrine reuptake centrally
- Nausea (most common - take with food)
- Dry mouth
- Constipation
- Dizziness
- Sexual dysfunction
- Severe liver disease
- Uncontrolled hypertension
- Concurrent MAOI use
- Once daily dosing (good compliance)
- No weight gain
- May help comorbid depression
Second-Line Agents
- Dose: 50-100 mg up to QDS (maximum 400 mg daily)
- NNT: 4-5
- Reserve for patients unresponsive to first-line
- Risks: Addiction potential, tolerance, falls in elderly
- Caution: Serotonin syndrome if combined with SNRI/SSRI
- Applied to affected area TDS-QDS
- Depletes substance P from nerve endings
- Burning sensation on initial application (improves with continued use)
- Minimal systemic absorption
- May be used as adjunct
- Applied to localized painful areas
- Up to 3 patches for 12 hours daily
- Minimal systemic absorption
- Expensive, limited evidence in diabetic neuropathy
Combination Therapy
If monotherapy insufficient:
- Amitriptyline plus Pregabalin (different mechanisms)
- Duloxetine plus Pregabalin
- Add topical agent to oral medication
Ineffective Treatments (Avoid)
- NSAIDs (ineffective for neuropathic pain)
- Paracetamol (ineffective monotherapy)
- Long-term opioids (addiction risk, limited evidence, no superiority over other agents)
Non-Pharmacological Approaches
- Limited evidence but safe
- May provide adjunctive benefit
- Patient-controlled
- Limited evidence
- May be tried if patient interested
- Helps with pain coping strategies
- Addresses sleep disturbance
- Useful for chronic pain management
This comprehensive pharmacological approach ensures exam readiness.
Management Algorithm
- 1
- 2
- 3
- 4
- 5
Management Principles
Diabetic neuropathy management follows a hierarchical approach:
1. Primary Prevention (prevent neuropathy development)
- Tight glycemic control (HbA1c less than 7%)
- Cardiovascular risk modification
2. Secondary Prevention (prevent complications in established neuropathy)
- Annual screening (monofilament testing)
- Patient education
- Protective footwear
- Regular podiatry
3. Complication Management (treat active problems)
- Ulcer offloading and wound care
- Charcot immobilization
- Infection control
- Surgical intervention if needed
Complications Management
Diabetic Foot Ulcer Management
Comprehensive Ulcer Assessment
- Size: Measure length, width, depth (photograph for serial comparison)
- Location: Plantar MT heads (neuropathic), toes/heel (ischemic), between toes (fungal/moisture)
- Depth: Superficial (skin only) vs deep (tendon, bone exposed)
- Probe to bone: Insert sterile probe - if touches bone, 87% sensitive for osteomyelitis
- Appearance: Granulation tissue (healing), slough (needs debridement), necrotic tissue (poor perfusion)
- Discharge: Serous (normal), purulent (infected), malodorous (anaerobes, necrotizing infection)
- Callus: Indicates high pressure (requires debridement)
- Cellulitis: Erythema extent (mark with pen, track daily)
- Undermining or sinus tracts: Track with probe (may communicate with bone)
- Skin temperature: Hot suggests infection or Charcot, cool suggests ischemia
- 10g monofilament: Will be abnormal in neuropathic ulcer
- Pain: Neuropathic ulcers typically painless (ischemic ulcers painful)
- Pulses: Dorsalis pedis, posterior tibial
- ABPI: Unreliable if greater than 1.3 (medial calcification in diabetics)
- Toe-Brachial Index (TBI): More reliable (toe vessels less calcified)
- TBI greater than 0.7: Adequate perfusion for healing
- TBI less than 0.5: Revascularization may be needed
- TBI less than 0.3: Critical ischemia, urgent vascular referral
- No infection: No purulence, erythema, warmth, or systemic signs
- Mild infection: Erythema less than 2 cm from ulcer edge, superficial
- Moderate infection: Erythema greater than 2 cm OR deep tissue involvement
- Severe infection: Systemic signs (fever, rigors, hypotension) OR necrotizing fasciitis
- Grade 0: No open lesion (high-risk foot)
- Grade 1: Superficial ulcer
- Grade 2: Deep ulcer (tendon, bone, joint)
- Grade 3: Deep ulcer with abscess or osteomyelitis
- Grade 4: Forefoot gangrene (partial amputation salvageable)
- Grade 5: Whole foot gangrene (major amputation needed)
This assessment guides treatment planning.
Charcot Neuroarthropathy Management
Acute Charcot Management (Eichenholtz Stage 0-1)
- Hot, swollen, painless foot in diabetic with neuropathy
- May have minor trauma history (often forgotten or trivial)
- Temperature difference greater than 2 degrees Celsius between feet
- Erythema, edema (often misdiagnosed as cellulitis or DVT)
- NO PAIN despite significant swelling (hallmark of Charcot)
- Infrared thermometry: Affected foot 3-5 degrees Celsius warmer than contralateral
- Monofilament testing abnormal (neuropathy prerequisite)
- May have palpable bony crepitus if advanced
- X-ray initially: May be NORMAL in stage 0 (pre-fragmentation)
- MRI gold standard early: Bone marrow edema, joint effusion before X-ray changes
- Serial X-rays: Monthly to monitor progression or coalescence
- Cellulitis: Would expect pain, systemic signs (fever)
- DVT: Would expect calf involvement, positive D-dimer
- Gout: Would expect severe pain, monoarticular, tophi
- Osteomyelitis: Requires wound/ulcer as source
- Total Contact Cast application SAME DAY
- Non-weight-bearing initially (crutches or wheelchair)
- OR protected weight-bearing in TCC (distributes forces)
- Prevents progressive fragmentation and collapse
- Cast changes weekly initially (swelling reduces rapidly)
- Then every 2-3 weeks once stable
- Monitor temperature weekly with infrared thermometry
- Temperature difference guides treatment duration
- Minimum 3-6 months in acute phase
- Continue until temperature normalized (difference less than 2 degrees Celsius for 2-4 consecutive weeks)
- Some patients require 6-12 months
- Do NOT remove cast prematurely (causes recurrence)
- Weekly temperature checks (infrared thermometry both feet)
- Monthly X-rays (monitor fragmentation stage 1, coalescence stage 2)
- Clinical assessment (swelling, erythema)
- Optimize glycemic control (HbA1c less than 7-8%)
- Calcium and Vitamin D supplementation
- Bisphosphonates (Pamidronate 90 mg IV monthly for 3-6 months) - CONTROVERSIAL, limited evidence but may reduce duration
- Mechanism: Reduce osteoclastic bone resorption
- Progressive bone fragmentation (stage 1)
- Joint subluxation and dislocation
- Rocker-bottom deformity (midfoot collapse)
- Bony prominences develop
- Recurrent ulceration over prominences
- Osteomyelitis, infection
- Amputation
This immediate response prevents devastating outcomes.
Surgical Technique
Surgical Interventions for Diabetic Neuropathy
- Symptomatic diabetic peripheral neuropathy
- Failed conservative management (6-12 months)
- Demonstrable nerve compression at anatomical tunnels
- Preserved motor function (best candidates)
- Tarsal tunnel (tibial nerve)
- Common peroneal nerve at fibular neck
- Deep peroneal nerve on dorsum foot
- Medial/lateral plantar nerves in tarsal tunnel
- Release fascial and fibro-osseous tunnels
- Decompress swollen, ischemic nerves
- Allow improved perfusion and function
- Non-healing ulcer with extensive gangrene
- Unreconstructable vascular disease
- Life-threatening sepsis (necrotizing fasciitis)
- Extensive osteomyelitis not amenable to resection
- Non-functional limb with severe deformity
- Toe amputation - single/multiple toes
- Ray amputation - metatarsal and toe
- Transmetatarsal - midfoot level
- Symes - ankle disarticulation
- Below-knee (BKA) - most common major amputation
- Above-knee (AKA) - if BKA healing unlikely
Tarsal Tunnel Decompression
- Curvilinear incision posterior to medial malleolus
- Identify and protect posterior tibial artery and veins
- Release flexor retinaculum completely
- Decompress tibial nerve and all branches
- Release medial and lateral plantar nerve tunnels
- Inspect for fibrous bands, lipomas, or other compressive lesions
- Careful hemostasis and closure
- Full release of all compartments critical
- Internal neurolysis generally not required
- Epineurotomy may be performed for visibly swollen nerves
- Careful handling of posterior tibial vessels
Exam Viva Point: "What is the role of nerve decompression in diabetic neuropathy?" Answer: Controversial but may benefit selected patients with compressive neuropathy at anatomical tunnels. Not first-line - reserve for patients with demonstrable compression and failed conservative treatment. Evidence is limited but some studies show improvement in sensation and pain.
Surgical treatment for diabetic neuropathy focuses on managing complications rather than treating the neuropathy itself.
Postoperative Care
Postoperative Management Principles
- Higher infection risk - meticulous sterile technique
- Impaired healing - protect wounds longer
- Regular wound inspection (patient may not feel problems)
- Keep wounds clean and dry
- Avoid tight dressings that impair perfusion
- Day 2: First inspection, dry dressing
- Daily wound checks for signs of infection
- Suture/staple removal: 3-4 weeks (vs 2 weeks in non-diabetics)
- Longer immobilization for bone healing
- Target glucose 6-10 mmol/L (not tight control for major surgery)
- Insulin sliding scale or infusion if required
- Avoid hypoglycemia (can cause falls, arrhythmia)
- Check HbA1c if unknown (guides long-term management)
- Stress response causes hyperglycemia
- Resume usual diabetes medications when eating
- Endocrinology input for poorly controlled patients
- Healing impaired if glucose persistently greater than 12 mmol/L
Offloading and Weight-Bearing
- Non-weight-bearing on residual limb initially
- Soft dressing and elevation to reduce edema
- Monitor for wound dehiscence, hematoma
- Early physio for conditioning, transfers, mobility aids
- Prosthetic assessment when wound healed and stump matured
- Total contact cast or removable cast walker
- Non-weight-bearing or protected weight-bearing
- Continue offloading until fully epithelialized
- Transition to therapeutic footwear
Exam Viva Point: "What are the key postoperative considerations in diabetic foot surgery?" Answer: Prolonged healing time - leave sutures in 3-4 weeks. Strict offloading essential. Glycemic control (target 6-10 mmol/L). Daily wound inspection as patient has impaired sensation. Higher infection risk - low threshold for antibiotic treatment.
Meticulous wound care and strict offloading are essential for successful outcomes in diabetic foot surgery.
Outcomes
Outcomes in Diabetic Neuropathy and Foot Disease
Ulcer Healing Outcomes
- Good Prognosis
- HbA1c less than 8%
- Poor Prognosis
- HbA1c greater than 10%
- Good Prognosis
- ABI greater than 0.9, palpable pulses
- Poor Prognosis
- ABI less than 0.5, critical ischemia
- Good Prognosis
- Superficial, no bone exposure
- Poor Prognosis
- Deep, probe-to-bone positive
- Good Prognosis
- No infection or superficial only
- Poor Prognosis
- Osteomyelitis, deep tissue infection
- Good Prognosis
- Total contact cast or strictly non-WB
- Poor Prognosis
- Poor compliance, continued walking
- Good Prognosis
- Albumin greater than 30 g/L
- Poor Prognosis
- Hypoalbuminemia, malnutrition
Ulcer Healing Rates:
- Superficial ulcer, no infection: 80-90% healing at 12 weeks
- Deep ulcer, no osteomyelitis: 60-70% healing at 12 weeks
- Ulcer with osteomyelitis: 40-60% healing with antibiotics and offloading
- Ischemic ulcer without revascularization: less than 30% healing
Exam Viva Point: "What determines diabetic ulcer healing outcomes?" Answer: Vascular status is the most critical factor. Ischemic ulcers won't heal without revascularization. Other factors: glycemic control (HbA1c less than 8%), infection control, strict offloading, and nutrition. Probe-to-bone positive indicates osteomyelitis and worse prognosis.
Healing outcomes depend on vascular status, glycemic control, infection management, and offloading compliance.
Prevention and Screening
Primary Prevention - Glycemic Control
Target HbA1c less than 7% (53 mmol per L):
The DCCT/EDIC trials (Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications) provided definitive evidence:
- Intensive glycemic control reduces neuropathy risk by 60-70% in Type 1 diabetes
- 1% reduction in HbA1c equals 40% reduction in microvascular complications
- Benefit persists even after relaxation of control (metabolic memory)
- Similar benefits demonstrated in Type 2 diabetes (UKPDS trial)
- Frequent blood glucose monitoring
- Adjust insulin or oral hypoglycemics to achieve targets
- Continuous glucose monitoring in selected patients
- Diabetes educator involvement
- Balance tight control with hypoglycemia risk (especially elderly)
- Smoking cessation (CRITICAL - accelerates all diabetic complications)
- Blood pressure control (target less than 140 over 90 mmHg)
- Lipid management (statin therapy for most diabetics)
- Regular exercise (improves insulin sensitivity)
- Weight loss if obese (improves glycemic control)
Tight glycemic control prevents development and slows progression of diabetic neuropathy but CANNOT reverse established nerve damage. AGE (Advanced Glycation End Product) accumulation and nerve fiber loss are permanent. Therefore, prevention through early intensive glycemic control is paramount. Once neuropathy is established, focus shifts to preventing complications (ulcers, Charcot, amputation).
Secondary Prevention - Screening Program
Annual Diabetic Foot Screening (MANDATORY):
Every diabetic patient requires annual comprehensive foot examination:
Dorsalis pedis and posterior tibial palpation U - Ulcers: Inspect all pressure points (plantar MT heads, heel, toes, between toes) L - Loss of sensation: 10g monofilament test at 5 sites S - Skin: Dry, cracked, callus, fissures, nail problems E - Examination of footwear: Appropriate shoes, internal damage
- Intact protective sensation (normal monofilament)
- Palpable pulses
- No deformity
- Management: Annual screening, patient education, glycemic control
- Loss of protective sensation OR absent pulses OR deformity
- No history of ulceration
- Management: 3-6 monthly podiatry review, protective footwear, intensive education
- Loss of protective sensation AND deformity
- OR previous ulceration
- OR previous amputation
- OR Charcot foot
- Management: Specialist multidisciplinary foot clinic (3 monthly), custom footwear, intensive monitoring
- Current ulceration
- Active Charcot
- Infected foot
- Management: Urgent specialist review, may require admission
Patient Education
Education improves foot-care knowledge and self-care behaviour and is a core component of multidisciplinary prevention (note: high-quality evidence that education alone reduces ulceration is limited - Dorresteijn Cochrane review):
- Use mirror to visualize plantar surface
- Check for cuts, blisters, redness, swelling, nail problems
- Between toes (fungal infection, fissures)
- Report any injuries immediately
- NEVER walk barefoot (indoors or outdoors)
- Check inside shoes before putting on (shake out foreign objects)
- Avoid high heels, pointed toes, or tight shoes
- New shoes: break in gradually (wear 1-2 hours daily initially)
- Replace worn shoes promptly
- Wash feet daily with lukewarm water (test temperature with elbow)
- Dry thoroughly, especially between toes
- Moisturize dry skin (avoid between toes - fungal infection risk)
- Do NOT use heating pads or hot water bottles (burn risk with sensory loss)
- Trim toenails straight across (avoid ingrown nails)
- Podiatry for nail care if vision poor or cannot reach feet
- Any foot wound, blister, or cut
- Redness, warmth, or swelling
- Change in foot shape
- Pain in legs or feet
- Ingrown toenail with redness
Protective Footwear
- Wide, deep toe box (accommodate claw toes without pressure)
- Adequate length (half thumb width beyond longest toe)
- Cushioned, shock-absorbing sole (reduce plantar pressure)
- No internal seams or rough areas (cause friction blisters)
- Lace-up or Velcro closure (allows adjustment for swelling)
- Breathable materials (reduce moisture, fungal risk)
- Foot deformity (claw toes, prominent MT heads)
- Previous ulceration (pressure redistribution required)
- Charcot foot (total contact insole in custom shoe)
- High plantar pressures on assessment
- Mold to exact shape of plantar foot
- Distribute pressure over entire plantar surface
- Reduce peak pressures at MT heads
- Accommodate deformities
- Require specialist orthotist for fabrication
- For chronic Charcot foot with fixed deformity
- Rigid ankle-foot orthosis with total contact
- Lifelong requirement after Charcot episode
- Prevents recurrent breakdown
Podiatry Services
- Nail care (trim nails, treat onychomycosis, remove ingrown nails)
- Callus debridement (reduce plantar pressure, prevent underlying ulceration)
- Footwear assessment and advice
- Orthotic prescription and fitting
- Early detection of pre-ulcerative lesions
- Education reinforcement
- Low risk: Annual (can coincide with medical review)
- Moderate risk: 3-6 monthly
- High risk: 1-3 monthly
- Very high risk: Weekly (during ulcer treatment)
Guidelines, Registries & Global Practice
Global Epidemiology
Diabetic foot disease is a worldwide burden, but prevalence varies markedly by region. A systematic review and meta-analysis (Zhang P et al, Annals of Medicine 2016) reported a global diabetic foot ulcer prevalence of 6.3% (95% CI 5.4-7.3), higher in men than women and higher in type 2 (6.4%) than type 1 (5.5%) diabetes.
- North America: 13.0% (95% CI 10.0-15.9) - the highest regional prevalence
- Africa: 7.2% (95% CI 5.1-9.3)
- Asia: 5.5% (95% CI 4.6-6.4)
- Europe: 5.1% (95% CI 4.1-6.0)
- Oceania: 3.0% (95% CI 0.9-5.0) - the lowest regional prevalence
The standard global review of natural history (Armstrong DG, Boulton AJM, Bus SA, New England Journal of Medicine 2017) frames the diabetic foot ulcer as a chronic, recurrent disease: a substantial proportion of people with diabetes develop a foot ulcer in their lifetime, and recurrence after healing is common, which is why post-healing remission care and lifelong surveillance are emphasised internationally.
Major Guidelines, Side by Side
Recommendations are broadly concordant on annual screening, the 10g monofilament, risk stratification and total contact casting, with differences mainly in screening frequency for higher-risk feet and in how strongly nerve decompression and adjuncts are endorsed.
- Screening / key recommendation
- Annual foot screening for all; more frequent (1-6 monthly) by risk stratification; 10g monofilament for loss of protective sensation
- Offloading
- Non-removable knee-high offloading device first-line for plantar forefoot/midfoot ulcers
- Stance / evidence emphasis
- GRADE-based; the most widely adopted global standard
- Screening / key recommendation
- Annual assessment, risk stratify (low/moderate/high/active); rapid referral to multidisciplinary foot service for active disease (within 1 working day)
- Offloading
- Non-removable casting for non-infected, non-ischaemic plantar ulcers
- Stance / evidence emphasis
- Strong emphasis on pathways and timely MDT referral
- Screening / key recommendation
- Annual comprehensive foot exam with 10g monofilament plus one other test; more frequent if high-risk
- Offloading
- Offloading central to ulcer healing
- Stance / evidence emphasis
- Aligns with IWGDF; integrated into annual diabetes standards
- Screening / key recommendation
- Recognise acute Charcot as inflammatory; clinical diagnosis, MRI when radiographs normal
- Offloading
- Total contact cast mainstay until inflammation resolves
- Stance / evidence emphasis
- Expert consensus; limited/uncertain role for bisphosphonates and surgery
Global Practice Variation
- Resource setting drives outcomes. Multidisciplinary high-risk foot services, total contact casting expertise, vascular intervention and advanced wound therapies are concentrated in high-resource systems; in limited-resource settings barefoot walking, delayed presentation and limited revascularisation contribute to higher amputation rates.
- Access models differ. Specialist podiatry is free at the point of care in some systems (e.g. NHS) and insurance- or subsidy-dependent in others; this influences screening frequency and footwear provision.
- Indigenous, remote and rural populations carry a disproportionate burden worldwide, with earlier diabetes onset, higher lower-limb amputation rates, remoteness, access barriers and comorbid renal disease repeatedly reported across underserved populations. Targeted responses include outreach podiatry, telehealth foot clinics, culturally safe community health-worker involvement and footwear-access programmes aimed at narrowing these gaps.
Multidisciplinary Foot Service (Universal Principle)
Across all guidelines the strongest structural recommendation is a coordinated multidisciplinary high-risk foot service - typically vascular surgery, endocrinology, podiatry, orthopaedic/foot-and-ankle surgery, infectious diseases and specialist wound nursing - with rapid access for acute Charcot and infected or ischaemic ulcers. Establishment of such services is consistently associated with reduced major amputation rates.
MCQ Practice Points
Q: What is the most common pattern of diabetic peripheral neuropathy and its clinical features?
A: Distal symmetric polyneuropathy (DSPN) is the most common pattern (75%), presenting as a "stocking-glove" distribution. Features: Sensory predominant (numbness, tingling, burning pain); Begins distally in feet, progresses proximally; Loss of vibration and position sense first; Ankle reflexes lost early; Motor involvement late. Key orthopaedic significance: Loss of protective sensation leads to neuropathic ulcers, Charcot arthropathy, and unrecognized trauma.
Q: How do you screen for diabetic neuropathy and what clinical tests are most reliable?
A: Standard screening: 10g monofilament testing (4-10 sites on plantar foot) - inability to detect indicates loss of protective sensation; 128 Hz tuning fork for vibration at great toe; Ankle reflexes. Additional tests: Semmes-Weinstein monofilaments (5.07 threshold for protective sensation); Ipswich Touch Test (simplified screening). Combination of abnormal monofilament + absent ankle reflex has highest sensitivity. Annual screening recommended for all diabetics.
Q: What is the pathophysiology of diabetic neuropathy?
A: Multifactorial mechanisms: (1) Metabolic - hyperglycemia activates polyol pathway (sorbitol accumulation), advanced glycation end-products (AGEs), oxidative stress; (2) Microvascular - endoneurial hypoxia from vasa nervorum disease; (3) Inflammatory - cytokine-mediated nerve damage. Result: Axonal degeneration (predominantly small unmyelinated fibers first, then large myelinated fibers) and segmental demyelination. Duration and degree of hyperglycemia are primary risk factors.
Q: What is the difference between diabetic neuropathy and Charcot neuroarthropathy?
A: Diabetic neuropathy: Nerve damage causing sensory/motor/autonomic dysfunction; Precedes and predisposes to Charcot. Charcot neuroarthropathy: Destructive arthropathy due to repetitive trauma in insensate foot + autonomic dysfunction (increased blood flow, osteoclast activation); Presents as acute red, hot, swollen foot; Progresses through Eichenholtz stages (fragmentation, coalescence, remodeling). Not all neuropathic patients develop Charcot (approximately 0.1-0.5% of diabetics).
Q: How does diabetic neuropathy influence surgical planning in foot/ankle surgery?
A: Key considerations: (1) Wound healing - increased infection risk, poor soft tissue healing; (2) Bone quality - often osteopenic, affects fixation; (3) Protected weight-bearing - patient may not feel pain warnings, requires extended immobilization; (4) Hardware considerations - may need larger, more robust constructs; (5) Vascular assessment - often coexistent PVD, check ABI preoperatively; (6) Glycemic control - optimize HbA1c (less than 8%) before elective surgery to reduce SSI risk.
At a Glance
Diabetic neuropathy affects 50% of diabetics, causing irreversible loss of protective sensation in a stocking-glove distribution due to metabolic and microvascular nerve damage. The 10g Semmes-Weinstein monofilament test at 5 plantar sites (1st toe, 1st/3rd/5th MT heads, heel) is the gold standard screening tool—inability to feel at any site indicates 4-7 fold increased ulcer risk. Three major complications are Charcot arthropathy (hot, swollen, PAINLESS foot requiring urgent total contact casting for 3-6 months), ulceration (15-25% lifetime risk, managed with offloading), and amputation (15-fold increased risk, 85% preceded by preventable ulcer). Annual foot screening is mandatory; tight glycemic control (HbA1c under 7%) prevents progression but cannot reverse established neuropathy.
PULSEDiabetic Foot Screening - PULSE
Hook:Check patient's PULSE - comprehensive diabetic foot assessment in every clinic visit
CUAThree Major Complications - CUA
Hook:CUA reminds you of the three devastating orthopaedic complications requiring aggressive prevention
1-1-3-5-HMonofilament Test Sites - 1-1-3-5-H
Hook:Remember 1-1-3-5-H for the five standard monofilament testing sites - inability to feel at ANY site equals high risk
ODIMUlcer Management Pillars - ODIM
Hook:ODIM - the four pillars of diabetic foot ulcer management, with Offloading being most critical
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are running a diabetes clinic. A 58-year-old man with Type 2 diabetes for 10 years (HbA1c 8.2%) attends for annual review. How would you screen for diabetic neuropathy and foot complications?”
“A 62-year-old diabetic presents to ED with a hot, swollen right foot for 3 days. No history of trauma. The foot is not painful. X-ray shows subtle midfoot changes. What is your differential diagnosis and immediate management?”
“A 68-year-old diabetic presents with a 3cm plantar ulcer under the 3rd metatarsal head present for 8 weeks. How would you assess and manage this comprehensively?”
EPIDEMIOLOGY
- 50% of diabetics develop neuropathy (duration-dependent)
- Distal symmetric polyneuropathy MOST COMMON (95% of cases)
- 15-fold increased amputation risk compared to non-diabetics
- 85% of amputations preceded by preventable foot ulcer
PATHOPHYSIOLOGY
- Polyol pathway: aldose reductase converts glucose to sorbitol (osmotic damage)
- Microvascular ischemia: basement membrane thickening, reduced endoneurial blood flow
- Advanced glycation end products (AGEs): irreversible protein cross-links
- Oxidative stress: free radical generation, membrane lipid peroxidation
- IRREVERSIBLE once established - cannot reverse with glycemic control
MONOFILAMENT TEST (GOLD STANDARD)
- 10g Semmes-Weinstein monofilament - MANDATORY annual screening
- Five sites (1-1-3-5-H): 1st toe, 1st/3rd/5th MT heads, heel
- Apply perpendicular until buckles, hold 1-2 seconds, ask "Can you feel this?"
- Inability to feel at ANY site equals loss of protective sensation
- Predicts ulcer risk with OR 4-7 (sensitivity 57-93%, specificity 75-100%)
THREE MAJOR COMPLICATIONS (CUA)
- Charcot: Hot, swollen, painless foot - urgent TCC for 3-6 months
- Ulceration: Painless plantar ulcers (15-25% lifetime risk)
- Amputation: 15-fold increased risk, 85% preceded by ulcer
ULCER MANAGEMENT (ODIM - FOUR PILLARS)
- Offloading: Total Contact Cast gold standard (reduces pressure 30-50%, 80-90% healing at 12 weeks)
- Debridement: Sharp debridement weekly (reduces bacterial load, stimulates healing)
- Infection: Antibiotics ONLY if infected (avoid resistance). Probe-to-bone 87% sensitive for osteomyelitis
- Moisture: Hydrocolloid dressings for moist wound healing, change 2-3 times weekly
CHARCOT MANAGEMENT
- Hot, swollen, PAINLESS foot equals Charcot until proven otherwise
- Temperature difference greater than 2°C diagnostic (infrared thermometry)
- MRI detects early (stage 0 - bone marrow edema) before X-ray abnormal
- Immediate total contact cast for minimum 3-6 months until temperature normalizes
- Monitor temperature weekly, X-ray monthly, transition to CROW boot when quiescent
PREVENTION STRATEGY
- Primary: HbA1c less than 7% (60-70% neuropathy risk reduction - DCCT trial)
- Annual screening: PULSE (Pulses, Ulcers, Loss of sensation, Skin, Examination of footwear)
- Patient education: Daily inspection, never barefoot, appropriate footwear (core part of multidisciplinary prevention)
- Protective footwear: Wide toe box, cushioned sole, custom orthotics if deformity
- Podiatry frequency: Low risk annual, moderate 3-6 monthly, high 1-3 monthly
VASCULAR ASSESSMENT
- Pulses: Dorsalis pedis (1st web space), posterior tibial (behind medial malleolus)
- ABPI unreliable in diabetics if greater than 1.3 (medial arterial calcification)
- Toe-Brachial Index (TBI) more accurate: greater than 0.7 adequate, less than 0.5 consider revascularization
- TcPO2 greater than 30mmHg predicts healing, less than 30mmHg impaired
NEUROPATHIC PAIN MANAGEMENT
- First-line: Amitriptyline (10-75mg nocte, NNT 3-4) OR Pregabalin (75-300mg BD, NNT 5-7) OR Duloxetine (60mg daily, NNT 5-6)
- Second-line: Tramadol (opioid - use with caution), topical capsaicin
- AVOID: NSAIDs (ineffective for neuropathic pain), long-term opioids
- Glycemic control slows progression but does NOT reverse established neuropathy
EXAM TRAPS TO AVOID
- Not knowing 5 monofilament sites (1st toe, 1st/3rd/5th MT, heel)
- Misdiagnosing Charcot as cellulitis (hot swollen PAINLESS is Charcot)
- Relying on ABPI alone in diabetics (use TBI - more reliable)
- Not offloading ulcers adequately (TCC mandatory, not just advice)
- Removing Charcot cast too early (need temperature normalized for 2-4 weeks)
Evidence Base
- 1441 patients with type 1 diabetes randomised to intensive versus conventional insulin therapy, mean follow-up 6.5 years
- Intensive therapy reduced the development of clinical neuropathy by 60% (95% CI 38-74)
- Risk of retinopathy reduced by 76% and microalbuminuria by 39% in the combined cohorts
- Chief harm was a two- to three-fold increase in severe hypoglycaemia
- Long-term follow-up (EDIC) showed benefit persisted after glycaemic separation narrowed - the metabolic memory phenomenon
- 3867 newly diagnosed patients with type 2 diabetes randomised to intensive (sulphonylurea or insulin) versus conventional glucose control
- Over 10 years HbA1c was 7.0% (intensive) versus 7.9% (conventional) - an 11% relative reduction
- Intensive control reduced microvascular endpoints by 25% (95% CI 7-40, p=0.0099)
- Any diabetes-related endpoint fell by 12%; macrovascular disease was not significantly reduced
- Intensive treatment increased hypoglycaemia and weight gain
- Systematic review of 30 studies (8365 patients); 4 studies compared the monofilament directly against nerve conduction studies as the reference standard
- Sensitivity ranged from 57% (95% CI 44-68) to 93% (95% CI 77-99) for detecting diabetic peripheral neuropathy
- Specificity ranged from 75% (95% CI 64-84) to 100% (95% CI 63-100)
- Authors recommend a three-site test (plantar great toe, third and fifth metatarsal heads) to maximise diagnostic value
- Wide variation in reported accuracy is driven by differing methodology and testing thresholds
- 14 RCTs (709 participants) of pressure-relieving offloading devices
- Non-removable casts healed significantly more ulcers than removable devices (RR 1.17, 95% CI 1.01-1.36)
- Non-removable casts also outperformed dressings alone
- Achilles tendon lengthening plus non-removable cast healed more forefoot ulcers than cast alone (RR 2.23, 95% CI 1.32-3.76)
- Key advantage of irremovable devices is enforced adherence - patients cannot offload themselves
- International task force convened by the American Diabetes Association and American Podiatric Medical Association
- Reframes acute Charcot as an inflammatory syndrome driven by neuropathy, trauma and disturbed bone metabolism
- Offloading with a total contact cast is the mainstay of acute-phase treatment, continued until inflammation settles
- Diagnosis is clinical; MRI detects early disease when radiographs are still normal
- Bisphosphonates have a limited and unproven role; evidence for surgery is low-quality
- 12 RCTs assessed patient education for preventing diabetic foot ulcers; only 5 reported ulceration or amputation endpoints
- One trial in high-risk patients reported reduced ulceration (RR 0.31, 95% CI 0.14-0.66) and amputation (RR 0.33, 95% CI 0.15-0.76) after a single group education session
- A similar, lower-risk-of-bias trial found no benefit (ulceration RR 1.00; amputation RR 0.98)
- Foot-care knowledge and self-reported self-care improved in the short term in most trials
- Authors conclude there is insufficient robust evidence that education alone reduces ulcers or amputations
- Global diabetic foot ulcer prevalence 6.3% (95% CI 5.4-7.3)
- Higher in type 2 (6.4%) than type 1 (5.5%) diabetes, and higher in men than women
- Highest in North America (13.0%) and lowest in Oceania (3.0%); Africa 7.2%, Asia 5.5%, Europe 5.1%
- Ulcer patients were older, had longer diabetes duration and more hypertension, retinopathy and smoking
- Marked regional variation underscores the need for region-specific prevention strategies
- Reframes the diabetic foot ulcer as a chronic, relapsing disease rather than a single acute event
- A large proportion of people with diabetes develop a foot ulcer over their lifetime
- Recurrence after healing is common, so healed patients are in remission rather than cured
- Loss of protective sensation, deformity and prior ulceration are the dominant recurrence risk factors
- Lifelong surveillance, offloading footwear and self-monitoring are central to maintaining remission