Pediatric Knee | Snapping | Lateral Meniscus
- Definition: A congenital variant where the meniscus is thickened and discoid (saucer) shaped rather than crescentic.
- Presentation: Only symptomatic discoid menisci need treatment. Classic sign is a loud 'clunk' or snap in extension.
- Wrisberg Variant: The most distinct type. It lacks the coronary ligaments (meniscotibial) posteriorly, attached only by the Ligament of Wrisberg (Meniscofemoral). It is hypermobile.
- MRI Sign: The 'Bow-tie' sign is seen on more than 3 consecutive sagittal slices (5mm cuts).
- “Type III (Wrisberg) is the 'Sneaky' one. It looks normal in shape but snaps loudly due to instability.
- “Total meniscectomy is condemned in children due to rapid onset arthritis (Fairbank changes). Preservation is key.
- “Peripheral rim instability is common after saucerization - always probe the rim.
Type III looks normal. On arthroscopy, the shape is crescentic. You might miss the diagnosis if you don't probe the posterior instability.
It Snaps. The lack of posterior tibial attachment causes the meniscus to subluxate into the notch during flexion, causing the clunk.
- Discoid
- Disc / Saucer
- Normal
- Crescent (C-shaped)
- Discoid
- Disorganized
- Normal
- Circumferential (Hoop stress)
- Discoid
- Poor central, Good peripheral
- Normal
- Red-Red / Red-White / White-White
- Discoid
- Poor load distribution
- Normal
- Shock absorber
Definitions
A congenital morphological variant where the lateral meniscus is discoid (disc-shaped) rather than the normal crescent (C-shape), covering a larger portion of the tibial plateau. It is thicker, hypercellular, and has disorganized collagen.
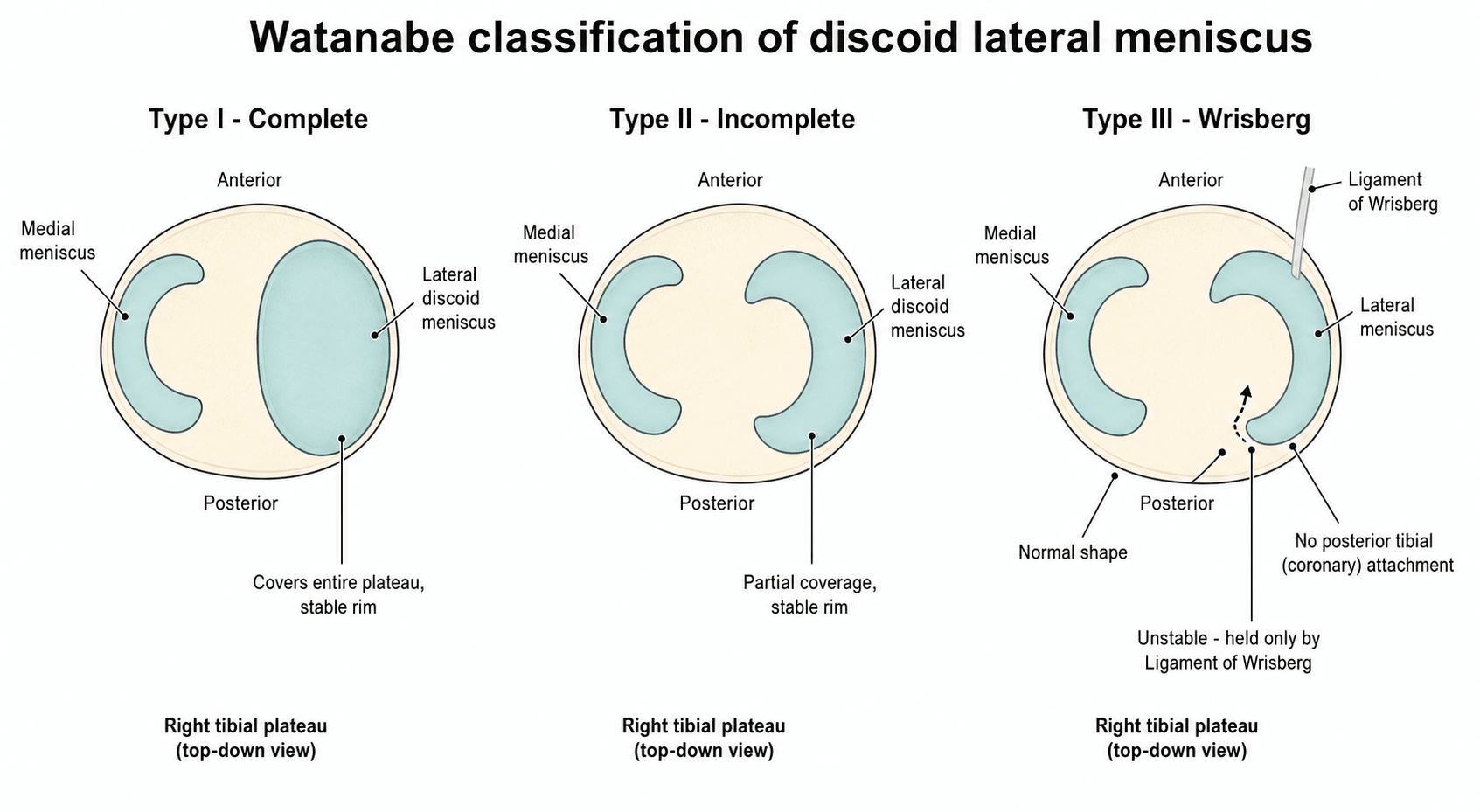
- Type I (Complete): Covers the entire plateau. Block shaped.
- Type II (Incomplete): Covers less than 100% but more than 80% (or significantly wider than normal).
- Type III (Wrisberg): Normal shape but LACKS posterior coronary ligaments. Unstable.
The surgical procedure of resecting the central portion of a discoid meniscus to create a functional peripheral rim (recreating the C-shape).
The Posterior Meniscofemoral Ligament (PMFL). It originates from the posterior horn of the lateral meniscus and inserts on the medial femoral condyle. In Type III discoid meniscus, it is often hypertrophied and acts as the only posterior restraint.
Fibrous bands connecting the inferior edge of the meniscus to the tibial plateau. Their absence defines the Type III variant.
Overview and Epidemiology
Discoid Meniscus is a morphological variant of the meniscus, predominantly affecting the lateral side.
- Etiology Theories:
- Smillie's Theory (1948): Proposed that the meniscus starts as a disc in the embryo and the center resorbs. Failure of resorption = Discoid. (Disproven. Embryonic meniscus is C-shaped from start).
- Kaplan (1955): Suggested absence of posterior attachment causes hypermobility, leading to shape change. (Partially true for Type III).
- Modern View: Genetic congenital malformation. Familial clusters reported.
- Histopathology:
- Disorganized collagen bundles (loss of hoop stress pattern).
- Intrameniscal mutinous degeneration.
- Cyst formation (Parameniscal cysts are common).
- Decreased vascularity in the central portion compared to normal meniscus.
- Familial cases suggested autosomal dominant inheritance with variable penetrance.
- Bilateral cases are more likely in familial presentations.
- Genes involved? Unknown, possibly Collagen type I alpha 2 (COL1A2).
- Fibular hemimelia? (Rare).
- Hypoplasia of the lateral femoral condyle (Result or Cause?).
- High riding fibular head.
Pathophysiology and Mechanisms
-
Normal: C-shaped. Attached to tibia via coronary ligaments. Attached to femur via Meniscofemoral ligaments (Wrisberg/Humphry).
-
Discoid: Block-like. Fills the lateral compartment.
- Thickened (up to 8mm vs normal 3-4mm peripheral height).
- Poor blood supply to the central 'block'.
-
Vascular Zones:
- Red-Red Zone: Peripheral 10-25%. Good healing potential. (Target for repair).
- Red-White Zone: Middle third. Variable healing.
- White-White Zone: Central avascular. No healing. (Target for saucerization).
- In Discoid meniscus, the central "slab" is entirely White-White and prone to degeneration.
- Inferior Lateral Genicular Artery: Supplies the peripheral rim. Preservation of this vessel during dissection for repair is crucial for healing.
- Common Peroneal Nerve (CPN):
- Runs posterior to the Biceps Femoris tendon at the joint line level.
- Risk of injury during Inside-Out suturing if the retractor is not placed correctly (between Biceps and Capsule).
- Risk during Outside-In technique? Less common but possible.
- Saphenous Nerve:
- Risk during medial repairs (not applicable here unless concomitant pathology).
- Coronary Ligaments (Meniscotibial): Connect the inferior edge of the meniscus to the tibia. Prevent superior migration. Absent in Type III.
- Meniscofemoral Ligaments:
- Ligament of Wrisberg: Posterior to PCL. Connects posterior horn of lateral meniscus to medial femoral condyle.
- Ligament of Humphry: Anterior to PCL.
- In Type III, Wrisberg is often hypertrophied and is the ONLY posterior restraint.
Classification
Watanabe Classification (1974)
The gold standard for arthroscopic classification.
-
Type I (Complete):
- Disc covers 100% of the tibial plateau.
- Thick/Block shaped.
- Stable peripheral rim.
-
Type II (Incomplete):
- Disc covers greater than 80%? Partial coverage. still wider than normal.
- Stable peripheral rim.
-
Type III (Wrisberg Variant):
- Normal (C-shaped) or slightly wide.
- Unstable. No posterior meniscotibial attachment.
- Hyper-mobile.
Type III requires repair, not just saucerization.
CIWClassification
Hook:The CIW (Crew) of the ship.
Clinical Assessment
Clinical Features
- Snapping: Loud auditory 'clunk' with flexion/extension.
- Pain: Lateral joint line pain.
- Locking: Inability to fully extend (bucket handle tear of the discoid).
- Giving way: Due to pain inhibition or subluxation.
- Effusion: Usually distinct lack of large effusion (unless acute tear).
- Joint Line Tenderness: Lateral side.
- Clunk: Palpable clunk at 110-30 degrees of flexion.
- McMurray Test: Positive for pain/click.
- Range of Motion: Usually full, unless locked.
A snapping knee in a child can also be:
- Iliotibial Band (ITB) friction.
- Patellar instability.
- Hamstring tendon snapping (Biceps femoris).
- Osteochondroma (snapping muscle over exostosis).
- Features
- Lateral line pain, Clunk in extension
- Age Group
- 3-12 years
- Features
- Snap over femoral condyle, lateral pain
- Age Group
- Adolescent (Runner)
- Features
- Anterior snap, Apprehension +
- Age Group
- Adolescent (Female)
- Features
- Biceps tendon over fibular head
- Age Group
- Adolescent
- Features
- Medial snap, tender plica
- Age Group
- Any age
Differentiation:
- Discoid Clunk: A dull, heavy thud felt and heard at 110-30 degrees of extension. It is the meniscus reducing/subluxing.
- Meniscal Tear Click: A sharp, high pitched click, usually painful.
- Patellar Click: Anterior.
SNAPSymptoms
Hook:The knee goes SNAP.
Investigations
- Description
- Appears as a bow-tie on greater than 3 sagittal slices (5mm cuts)
- Significance
- Diagnostic of discoid shape
- Description
- Meniscal width greater than 14mm or greater than 20% of plateau width
- Significance
- Quantitative measure
- Description
- High signal within the disc
- Significance
- Mucoid degeneration (Not necessarily a tear)
- Description
- Normal shape, but anterior displacement of posterior horn
- Significance
- Hard to diagnose on MRI
Imaging Atlas


Associated Osteochondritis Dissecans
A discoid lateral meniscus is a recognised association of osteochondritis dissecans (OCD) of the lateral femoral condyle - the abnormal thickness, poor load distribution and altered contact mechanics of the disc are thought to predispose the underlying condyle to a subchondral lesion.
- Where to look: the OCD lesion typically sits on the lateral femoral condyle beneath the discoid meniscus - in contrast to the more common medial-side OCD of the non-discoid knee.
- Why it matters: an unrecognised OCD changes the operation - the lesion may need drilling, fixation or grafting at the same arthroscopy, and its presence worsens the long-term prognosis.
- Practical point: scrutinise the lateral femoral condyle on the pre-operative MRI and inspect it arthroscopically once the central disc has been saucerized and the condyle is exposed.
Q: A child with a discoid lateral meniscus also has a focal cartilage/bone lesion - where and what is it likely to be? A: Osteochondritis dissecans of the lateral femoral condyle, a recognised association of discoid lateral meniscus (the abnormal disc alters loading of the underlying condyle). Look for it on MRI and inspect the condyle at arthroscopy after saucerization, addressing the lesion (drilling, fixation or grafting) in the same sitting.
Management Algorithm

The Accidental Finding
- Scenario: MRI done for other reason (or contralateral knee).
- Action: Observe.
- Rationale: Prophylactic surgery is NOT indicated. It may never tear. Surgery induces arthritis risk.
Do not touch asymptomatic discoid menisci.
SAVEManagement
Hook:SAVE the meniscus.
Surgical Technique
Arthroscopic Saucerization
Goal: Resculpt the discoid meniscus into a normal crescent shape (approx 6-8mm rim).
- Diagnostic Scope: Confirm type. Probe rim for instability.
- Resection:
- Use biters / shaver.
- Remove the central "block".
- Leave a stable peripheral rim (6-8mm).
- Probe Again: Crucial step. Often removing the center reveals a hidden peripheral detachment.
- Repair: If unstable rim found, perform Inside-Out or All-Inside repair.
The goal is a stable 6-8mm rim.
Complications
- Detail
- Remaining rim greater than 8mm. Symptoms persist.
- Prevention
- Probe measuring guide.
- Detail
- Rim less than 6mm. Instability/Hoop stress loss.
- Prevention
- Conservative bite.
- Detail
- Failure to diagnose Type III during case.
- Prevention
- Aggressive probing.
- Detail
- Inside-Out needle penetration. (Peroneal/Popliteal)
- Prevention
- Proper retractors. Knee flexion.
- Detail
- Tight lateral compartment in child.
- Prevention
- Use smaller scope (2.7mm). Figure 4 position.
Postoperative Care and Rehabilitation
Protocol
- Goal: Protect Repair. Manage Swelling.
- Weight Bearing:
- Saucerization: Full weight bearing as tolerated.
- Repair: Toe-touch weight bearing (TTWB) or Partial WB in brace.
- Brace:
- Saucerization: None.
- Repair: Range of Motion (ROM) brace locked in extension for walking. Unlocked 0-90 for sitting.
- ROM:
- Saucerization: Full.
- Repair: 0-90 degrees only. Avoid deep flexion (stress on posterior horn).
- Exercises: Straight leg raises, Quad sets.
- Weight Bearing: Progress to Full by week 6 (Repair).
- ROM: Full ROM by week 8.
- Activities:
- Stationary Bike (Seat high to avoid deep flexion).
- Swimming (Flutter kick only, No Breaststroke).
- Elliptical trainer.
- Proprioception (Wobble board).
- Goal: Return to sport.
- Criteria:
- No effusion.
- Full painless ROM.
- Quad strength greater than 90% of contralateral.
- Functional hop tests passing.
- Timeline:
- Saucerization: 3 months.
- Repair: 4-6 months.
Outcomes
Fairbank (1948) described 3 classic signs of post-meniscectomy arthritis:
- Ridge formation: An osteophyte ridge on the femoral condyle.
- Flattening: Squaring of the femoral condyle.
- Narrowing: Loss of joint space.
- Symptomatic Relief: Excellent in the short/medium term.
- Degeneration: Even with saucerization, the remaining meniscus is ultrastructurally abnormal. Long term osteoarthritis rates are higher than normal population, but much lower than total meniscectomy.
- Total Meniscectomy: Results in severe lateral compartment overload and rapid degeneration (Fairbank changes). Avoid at all costs.
- Re-operation Rate: Approximately 10-20% (for recurrent tear or instability).
Salvage of the Meniscus-Deficient Compartment
Some patients - particularly those who had a historical total meniscectomy for a discoid meniscus - present years later with a symptomatic, meniscus-deficient lateral compartment and early lateral overload. For these knees, lateral meniscal allograft transplantation (MAT) is the salvage option.
- Indication: a symptomatic, meniscus-deficient (post-meniscectomy) lateral compartment in a relatively young patient with preserved articular cartilage (no advanced arthritis), normal or corrected alignment and a stable knee.
- Contraindications: advanced osteoarthritis (the cartilage is already lost), uncorrected malalignment and instability - these must be addressed first or the graft will fail.
- Goal: MAT is a pain-relieving, chondroprotective procedure that restores load distribution. It is salvage, not a routine alternative to rim-preserving saucerization, and is the strongest argument for why total meniscectomy must be avoided in the first place.
Q: A young adult had a total lateral meniscectomy for a discoid meniscus as a child and now has lateral pain with early overload but preserved cartilage - what can you offer? A: Lateral meniscal allograft transplantation, the salvage for a symptomatic meniscus-deficient compartment when cartilage is still preserved, alignment is normal or corrected, and the knee is stable. The difficulty of this salvage is exactly why total meniscectomy is condemned in children and rim-preserving saucerization is the standard.
Guidelines, Registries & Global Practice
Global Epidemiology:
- Reported prevalence of lateral discoid meniscus ranges widely (approximately 0.4 to 17%), reflecting differences in study population, imaging, and case definition; medial discoid is rare (approximately 0.1 to 0.3%).
- Markedly higher prevalence is consistently reported in East Asian populations (Japan, Korea, China), with some series exceeding 10 to 13%, versus roughly 3 to 5% in Western series.
- Bilateral involvement occurs in approximately 10 to 20% of cases; the contralateral knee should be examined and imaged if symptomatic.
- It is the most common congenital meniscal anomaly of childhood and the dominant cause of isolated lateral meniscal pathology in children under 13.
Side-by-Side Society Guidance (no single discoid-specific RCT-based guideline exists; recommendations converge):
- Asymptomatic disc
- Observe, no prophylactic surgery
- Operative principle
- Saucerization + repair of unstable rim; preserve a 6 to 8mm rim
- Asymptomatic disc
- Observe; reassure
- Operative principle
- Meniscal preservation; meniscectomy only for irreparable tissue
- Asymptomatic disc
- Observe
- Operative principle
- Saucerization, repair instability, address tear; avoid total meniscectomy
- Asymptomatic disc
- Observe
- Operative principle
- Same preservation paradigm; high case volume drives technique refinement
- No dedicated arthroplasty-style registry tracks discoid meniscus (it is a soft-tissue paediatric condition), so evidence rests on single-institution long-term cohorts rather than national registries.
- The strongest long-term data (minimum 15-year cohort) report durable function but an approximately 44% reoperation rate and no progression to total knee replacement after rim-preserving surgery.
- High-resource settings: Routine MRI for diagnosis and dynamic/two-position MRI to assess rim instability; small-joint arthroscopy with 2.7mm or 4.0mm scopes and all-inside repair devices in young children.
- Limited-resource settings: Diagnosis may rely on clinical clunk plus plain radiographs (widened lateral joint space, squared lateral femoral condyle, cupping of the lateral tibial plateau) when MRI is unavailable; inside-out and outside-in repair with standard sutures remain effective and avoid costly all-inside implants.
- Across all settings the governing principle is identical: never perform total meniscectomy in a child; preserve and stabilise the rim.
- Symptomatic children are best managed by a paediatric orthopaedic or sports-knee surgeon experienced in small-joint arthroscopy.
Controversies & Areas of Uncertainty
- Classification for surgical planning: Watanabe describes shape but not stability. Contemporary work (Yang/Kocher, 2022) shows peripheral-rim STABILITY predicts the need for repair far better than morphology, and proposes a stability/morphology/tear (S/M/T) scheme. Whether this should replace Watanabe in routine practice is unsettled.
- Optimal rim width: A 6 to 8mm residual rim is conventional, but the ideal balance between leaving enough tissue for hoop-stress function and removing enough redundant disc to stop snapping is not defined by high-level evidence.
- Repairing the no-shift complete discoid: How aggressively to probe for and repair occult rim instability in a complete discoid that does not visibly shift is debated; dynamic two-position MRI (Hashimoto, 2022) is promising but not universally available.
- Predicting late osteoarthritis: Even rim-preserving surgery leaves ultrastructurally abnormal tissue, and long-term cohorts show a high reoperation rate (approximately 44% at 15+ years). Which patients will degenerate, and whether earlier repair changes that trajectory, remains unknown.
- Management of the truly asymptomatic disc: Universal observation is standard, but the natural-history risk of an incidental complete discoid eventually tearing has never been quantified prospectively.
MCQ Practice Points
Q: How many sagittal slices (5mm cuts) showing a bow-tie are required to diagnose discoid meniscus? A: Three or more. (Normal meniscus is seen on 2 slices: body and body. 3 implies continuity/width).
Q: What is the most common presenting symptom of Wrisberg type discoid meniscus? A: Snapping (Clunking) knee. Often painless initially.
Q: Which Watanabe type has a normal crescentic shape? A: Type III (Wrisberg). It is defined by its instability (lack of coronary ligaments), not its shape.
Q: What is the treatment for an asymptomatic discoid meniscus found on MRI? A: Observation. No surgery.
Q: What is the long term sequela of total meniscectomy in a child? A: Fairbank changes (Early Osteoarthritis).
Q: Which ligament is hypertrophied in Type III Wrisberg variant? A: The Posterior Meniscofemoral Ligament (Ligament of Wrisberg). It acts as the sole posterior restraint in the absence of coronary ligaments.
Q: Apart from the bow-tie sign, what coronal MRI finding suggests discoid meniscus? A: Meniscal width greater than 14mm or covering greater than 20% of the tibial plateau width.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 10-year-old girl complains of a snapping knee. MRI shows a 'bow-tie' sign on 5 consecutive slices.”
“Intra-operatively, you perform a saucerization. The remaining rim looks stable to the probe. You are about to finish.”
“A 6-year-old presents with a locked knee in 30 degrees of flexion. No trauma.”
Classification (Watanabe)
- Type I: Complete
- Type II: Incomplete
- Type III: Wrisberg (Unstable)
- Type III: Normal shape!
Diagnosis
- Snap / Clunk
- Bow-tie sign greater than 3 slices
- Coronal width greater than 14mm
- Lateral Joint Line Pain
Treatment
- Asymptomatic: Observe
- Symptomatic I/II: Saucerization
- Symptomatic III: Repair
- Avoid Total Meniscectomy
Evidence Base
All evidence below has been verified against the primary record in PubMed. Watanabe's original arthroscopic classification (1974) is the historical reference standard and is cited as a classification source.
Long-Term (Minimum 15-Year) Outcomes After Rim-Preserving Saucerization
- 98 children/adolescents treated arthroscopically for lateral discoid meniscus; mean age at index surgery 10.8 years.
- Mean follow-up 19.5 years (range 16 to 27); patient-reported outcomes favourable (IKDC 77.4, Lysholm 78.6, Tegner 7).
- 44% (11/25 evaluated) underwent subsequent ipsilateral discoid-related surgery (revision saucerization with or without repair).
- No patient progressed to total knee replacement at final follow-up.
Stability- and Tear-Based Surgical Classification (S/M/T System)
- 434 paediatric/adolescent discoid knees reviewed (1991 to 2016).
- Unstable menisci received repair in 93% of cases; instability alone gave 89% sensitivity and 94% specificity for predicting repair.
- Odds of repair were 114 times higher for unstable than stable menisci.
- Proposed S (stability) / M (morphology) / T (tear) scheme outperforms Watanabe morphology alone for surgical planning.
Two-Positioned MRI to Detect Peripheral Rim Instability
- 39 patients with no-shift-type complete discoid lateral meniscus; arthroscopy as reference standard.
- Meniscal shift on full-extension vs deep-flexion MRI predicted overall rim instability with PPV 0.96, sensitivity 0.85, specificity 0.91.
- Anterior shift predicted posterior instability with PPV and specificity of 1.0.
- High agreement (kappa 0.84) between the clinical snapping phenomenon and the MRI shift.
Saucerization Plus Peripheral Repair for the Unstable Discoid
- 18 knees (mean age 11.1 years) with symptomatic unstable discoid meniscus and a peripheral lesion.
- Saucerization combined with inside-out/outside-in repair; mean 3.4 sutures per knee.
- Kaplan-Meier survival 93.7% at 1 year and 85.9% at 2 years; mean Pedi-IKDC 98.3, Lysholm 98.7.
- 18.8% required subsequent subtotal meniscectomy for repair failure.
Discoid vs Non-Discoid Meniscus Outcomes in Adolescents
- 48 discoid and 45 non-discoid adolescent knees treated arthroscopically (2015 to 2021).
- Discoid patients were younger (12.7 vs 15.8 years) with lower BMI.
- Majority in both groups underwent meniscal repair (discoid 73%).
- IKDC and physical-activity scores improved significantly and did not differ between discoid and non-discoid groups at 2 years.
Prevalence and Age-Dependent Imaging Reliability
- 261 arthroscopies for isolated lateral meniscal pathology; 75% were discoid.
- 97% of patients under 13 years with lateral meniscal pathology had a discoid meniscus.
- Standard MRI criteria (3 consecutive sagittal cuts) became unreliable after age 13.
- Complete-to-incomplete discoid ratio approximately 4:3.
Diagnosis and Management Review (AAOS Journal)
- Authoritative review of paediatric discoid meniscus diagnosis and treatment.
- Complete meniscectomy relieves symptoms but causes degenerative change at midterm; now abandoned.
- Current standard is saucerization with peripheral repair when instability is present.
- Short-term results good; degenerative change reported at intermediate follow-up.
Contemporary Narrative Review: Epidemiology and OA Risk
- Reported incidence approximately 0.4 to 17% for lateral and 0.1 to 0.3% for medial discoid meniscus.
- One of the most frequent congenital knee anomalies in childhood; true prevalence unknown as many are asymptomatic.
- Symptomatic discoid should be treated by saucerization, tear repair and stable fixation.
- Osteoarthritis progression risk is higher in operated discoid knees, mandating prolonged follow-up.
Watanabe Arthroscopic Classification (Reference Standard)
- Original arthroscopic classification of discoid lateral meniscus.
- Type I complete and Type II incomplete are stable, peripherally attached.
- Type III (Wrisberg) has a normal/near-normal shape but lacks posterior coronary (meniscotibial) attachment and is unstable.
- Remains the most widely cited descriptive system worldwide.