X-Linked Dystrophinopathy | Progressive Weakness
- Genetics: X-linked recessive. Dystrophin gene mutation. Boys affected.
- Pathophysiology: Absent dystrophin leads to muscle fiber necrosis, fibrosis, weakness.
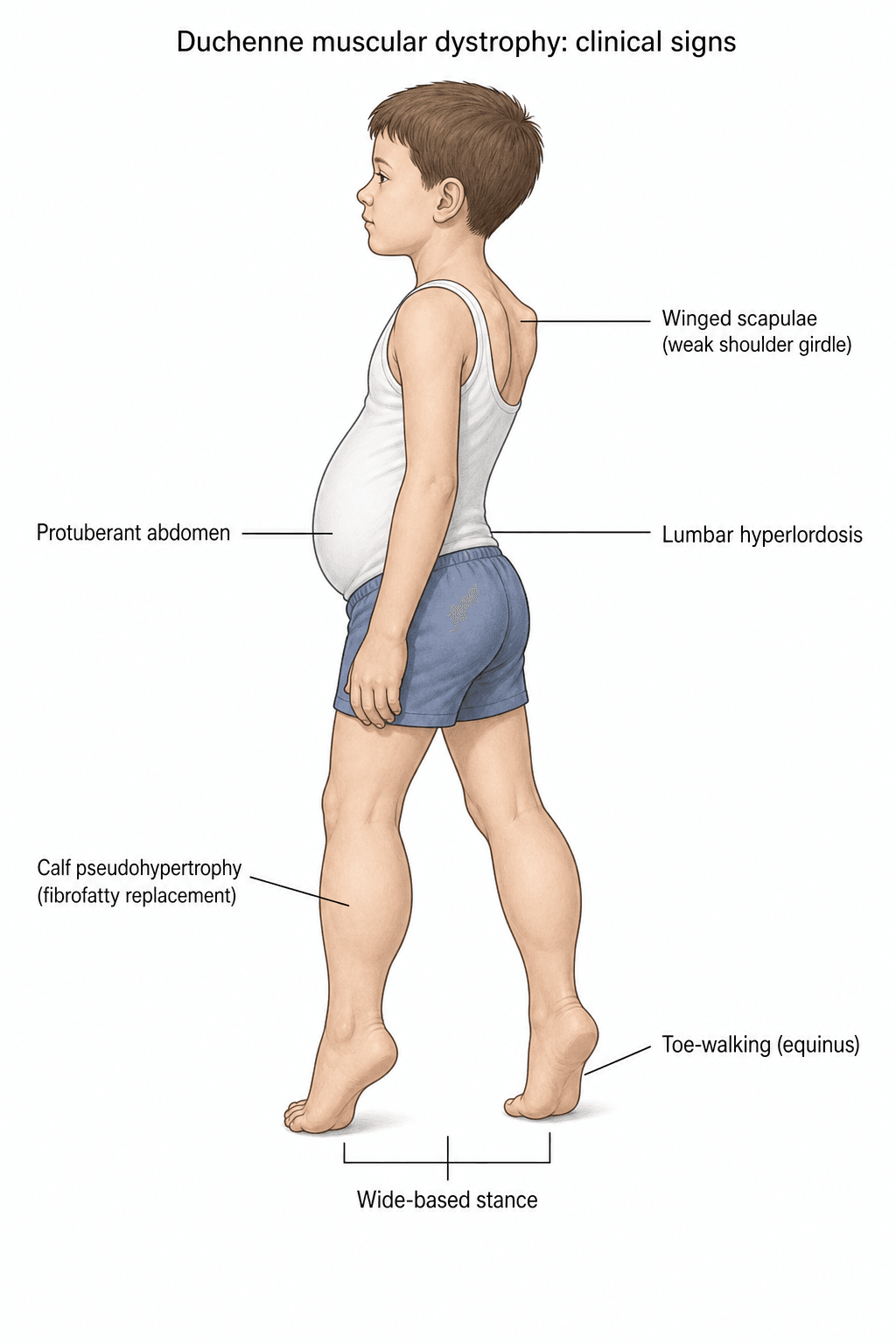
- Presentation: Proximal weakness (3-5 yo), Gowers' sign, Pseudohypertrophy (calves).
- Scoliosis: Inevitable after loss of ambulation. Spinal fusion indicated if rapid progression.
- Steroids: Prednisolone/Deflazacort prolongs ambulation and delays scoliosis.
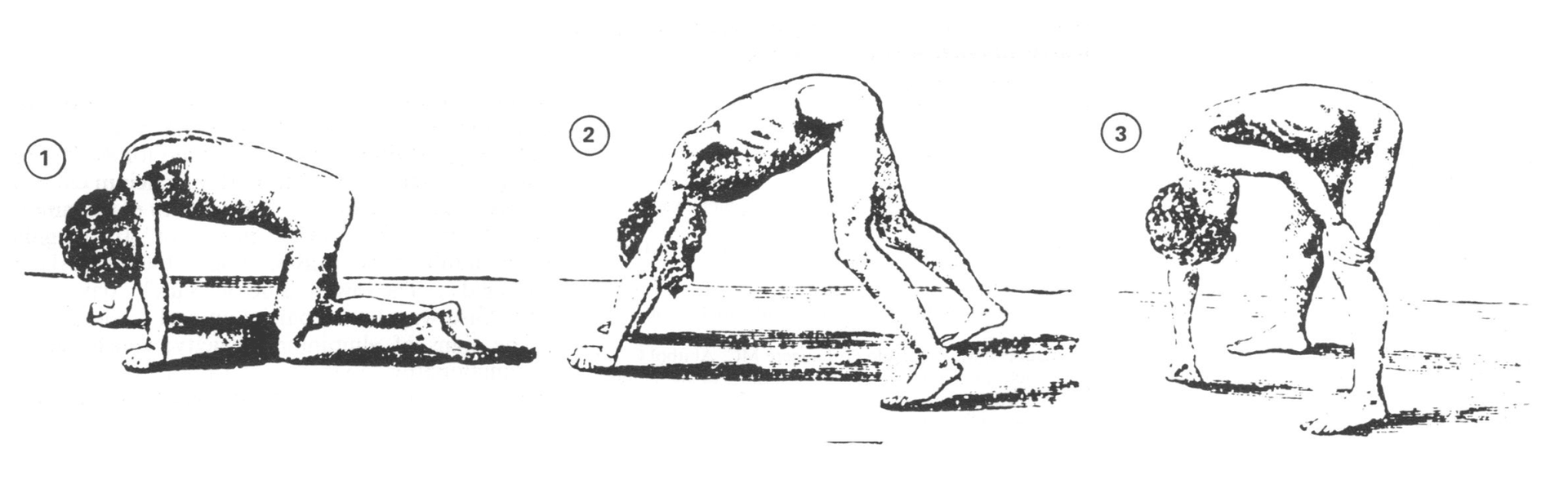
- “Gowers' sign = Proximal weakness (uses arms to 'climb up' legs to stand).
- “Pseudohypertrophy of calves (fatty/fibrous infiltration).
- “CK is MASSIVELY elevated (10-100x normal) - useful screening test.
- “Scoliosis progresses after loss of ambulation. Fuse before severe.
Anesthetic Risk. DMD patients are at risk. Avoid succinylcholine and volatile agents. Use TIVA.
Cardiomyopathy. All DMD patients develop cardiomyopathy. Cardiac clearance before any surgery.
Pulmonary Function. Progressive respiratory muscle weakness. Assess FVC before scoliosis surgery.
Osteoporosis. Steroid use + Immobility = Fractures. Lower limb fractures can end ambulation.
- Duchenne (DMD)
- ABSENT
- Becker (BMD)
- REDUCED (partial function)
- Duchenne (DMD)
- 3-5 years
- Becker (BMD)
- Adolescence / Adult
- Duchenne (DMD)
- Severe
- Becker (BMD)
- Milder
- Duchenne (DMD)
- By 12 years
- Becker (BMD)
- May ambulate into adulthood
- Duchenne (DMD)
- 20-30 years
- Becker (BMD)
- 40-50+ years
DUCHENNEDMD Features
Hook:Key features of DMD.
CLIMBGowers' Sign
Hook:Gowers' = Proximal weakness.
Overview and Epidemiology
Duchenne Muscular Dystrophy (DMD) is a severe X-linked recessive disorder caused by mutations in the dystrophin gene (Xp21). It results in absent dystrophin protein, leading to progressive muscle degeneration.
- Incidence: ~1 in 3500-5000 male births.
- Inheritance: X-linked recessive. Males affected. Females are carriers.
- New Mutations: ~1/3 are sporadic (new mutation).
- Age 3-5: Symptom onset (delayed walking, difficulty climbing stairs).
- Age 5-10: Progressive weakness. Gowers' sign. Toe walking.
- Age 10-12: Loss of ambulation. Wheelchair-bound.
- Age 15+: Scoliosis progression. Respiratory decline. Cardiomyopathy.
- Age 20-30: Death (usually respiratory or cardiac failure).
Genetics and Pathophysiology
- Gene: Dystrophin (DMD gene) on Xp21.
- Mutation Types: Deletions (60%), Duplications (5-10%), Point mutations (30%).
- Result: Complete absence of dystrophin protein.
- Dystrophin: Links cytoskeleton to ECM. Stabilizes sarcolemma during contraction.
- Absence: Membrane fragility. Increased calcium influx. Muscle fiber necrosis.
- Progression: Repeated cycles of necrosis and regeneration. Eventually, fibrosis and fatty replacement.
- CK Elevation: Leakage from damaged muscle fibers.
- Same gene, but in-frame mutations that allow partial dystrophin function.
- Milder phenotype. Later onset. Longer survival.
The Reading-Frame Rule (Genotype-Phenotype)
The single principle that unifies DMD genetics, the Duchenne-versus-Becker distinction and modern antisense therapy is the reading-frame (Monaco) rule.
- Out-of-frame (frameshift) mutations shift the triplet reading frame, generate a premature stop codon and abolish dystrophin - producing the severe Duchenne phenotype.
- In-frame mutations delete whole codons but preserve the downstream frame, producing a shortened but partly functional dystrophin - producing the milder Becker phenotype.
- The rule holds in roughly 90 percent of cases; exceptions exist (for example, large in-frame deletions disrupting critical actin-binding or dystroglycan-binding domains can still behave like Duchenne), so genotype is strongly correlated with, but not absolutely predictive of, phenotype.
Therapeutic corollary - exon skipping: antisense oligonucleotides (such as eteplirsen for exon-51-amenable deletions) mask a neighbouring exon during splicing so the mutated transcript is read back in frame, converting a Duchenne-type out-of-frame defect into a Becker-like in-frame product with partial dystrophin restoration.
Q: Two boys each have a dystrophin gene deletion - one has Duchenne and one has Becker. What genetic principle explains the difference? A: The reading-frame rule: a frameshifting (out-of-frame) deletion abolishes dystrophin and causes Duchenne, whereas an in-frame deletion yields a truncated but partly functional protein and causes the milder Becker phenotype. Exon-skipping therapy exploits this by restoring the reading frame to convert a Duchenne-type defect toward a Becker-like one.
Pathophysiology: Musculoskeletal Mechanisms
Why weakness becomes deformity: The orthopaedic burden of DMD is a direct downstream consequence of progressive, asymmetric muscle weakness acting across growing joints and a growing spine.
- Contractures: Antigravity muscles (gastrocnemius-soleus, hip flexors, iliotibial band) retain relative strength longer than their antagonists (tibialis anterior, hip extensors). The resulting muscle imbalance, combined with prolonged sitting once ambulation is lost, drives fixed equinus, hip flexion contracture and ITB tightness.
- Equinus gait compensation: While still ambulant, boys adopt toe-walking and a lordotic, wide-based stance to keep the ground-reaction force anterior to the knee and posterior to the hip, stabilising both joints despite quadriceps and gluteal weakness. Aggressive Achilles lengthening that destroys this equinus "lock" can precipitate loss of ambulation.
- Neuromuscular scoliosis: Once truncal and paraspinal muscles can no longer balance the seated spine, a long C-shaped collapsing curve with pelvic obliquity develops. Unlike idiopathic scoliosis, it progresses even after skeletal maturity and through the wheelchair years.
- Fragility bone: Disuse osteoporosis (immobility) plus glucocorticoid-induced bone loss produces a fracture-prone skeleton. Vertebral compression fractures and low-energy long-bone fractures (especially distal femur) are common; a femoral fracture in a marginal ambulator frequently ends walking permanently.
Classification Systems
DMD is staged by functional ambulatory status, which drives the timing of every orthopaedic decision. The Brooke (upper limb) and Vignos (lower limb) scales remain the classic clinical grading tools.
The North Star Ambulatory Assessment (NSAA) and the 6-minute walk test are the validated trial outcome measures, but day-to-day staging follows five clinical phases:
- Presymptomatic: Diagnosis on raised CK or family history; may have mild delay only.
- Early ambulatory: Gowers' sign, waddling gait, toe-walking, trouble with stairs and running.
- Late ambulatory: Increasingly laboured gait, frequent falls, struggling to rise from floor.
- Early non-ambulatory: Wheelchair for distance, then full-time; able to self-propel; scoliosis begins.
- Late non-ambulatory: Upper-limb and trunk function declining; respiratory and cardiac support needed.
Clinical Assessment
- Developmental: Delayed walking (18+ months). Difficulty running, climbing, jumping.
- Family History: X-linked pattern. Carrier mother. Affected uncles/brothers.
- Gowers' Sign: Uses hands on thighs to stand from floor (proximal weakness).
- Pseudohypertrophy: Calves appear large (fibrofatty replacement).
- Lordosis: Lumbar hyperlordosis (weak hip extensors).
- Toe Walking: Equinus contracture.
- Shoulder Weakness: Weak scapular fixators ('winging').
- Contractures: Equinus, Hip flexion, Iliotibial band.
- Scoliosis: After loss of ambulation.
- Contractures: Equinus (most common), Hip flexion, ITB tightness.
- Scoliosis: Progressive neuromuscular scoliosis after wheelchair.
- Fractures: Fragility fractures (osteoporosis from steroids + immobility).
Investigations
- Serum CK: Massively elevated (10-100x normal). Screening test.
- Genetic Testing: Confirms mutation. Multiplex PCR, MLPA, Sequencing.
- Muscle Biopsy: Absent dystrophin on immunohistochemistry. Now less used (genetic testing is gold standard).
- Spine X-ray: AP and Lateral for scoliosis. Measure Cobb angle.
- Whole Spine MRI: If planning fusion.
- Pulmonary Function (FVC): Essential before scoliosis surgery.
- Cardiac Assessment: Echo, ECG. Cardiomyopathy is universal.
- DEXA: Bone density assessment.

Carrier Females and Genetic Counselling
"Females are carriers" is an over-simplification examiners probe.
- Manifesting carriers: because of skewed X-inactivation (lyonisation) a minority of female carriers have skeletal-muscle symptoms - calf hypertrophy, cramps, mild-to-moderate proximal weakness and a raised CK. The most severe female presentations occur with Turner syndrome (45,X) or an X-autosome translocation that disrupts the dystrophin gene.
- Carrier cardiomyopathy: carriers are at risk of dilated cardiomyopathy even when they have no skeletal-muscle weakness, so every confirmed or obligate carrier needs baseline and periodic cardiac surveillance (ECG and echocardiography) regardless of muscle symptoms.
- Germline mosaicism in counselling: about one-third of cases are apparently "new" mutations, but a mother whose blood test is negative is not guaranteed a zero recurrence risk, because the mutation may be present in a subset of her oocytes (gonadal/germline mosaicism, giving a recurrence risk of the order of 10 percent). Prenatal or preimplantation genetic diagnosis should therefore still be offered.
Q: A boy is diagnosed with Duchenne muscular dystrophy. Besides carrier testing, what must his mother be offered? A: Cardiac surveillance. Female carriers can develop dilated cardiomyopathy even without skeletal-muscle weakness, so baseline and periodic ECG/echocardiography are recommended. She also needs genetic counselling that accounts for germline mosaicism - a negative maternal blood test does not eliminate the recurrence risk in future pregnancies, so prenatal/preimplantation diagnosis is still offered.
Differential Diagnosis
The classic triad of a young boy with proximal weakness, a positive Gowers' sign and a markedly raised CK has a focused differential. Distinguishing features are exam favourites.
- Distinguishing Features
- Same gene; in-frame mutation, later onset, milder, longer ambulation
- Key Test
- Dystrophin reduced (not absent); genetics
- Distinguishing Features
- Autosomal; affects both sexes; calf pseudohypertrophy possible
- Key Test
- Gene panel; dystrophin normal
- Distinguishing Features
- Tongue fasciculations, areflexia, distal involvement, normal/mildly raised CK
- Key Test
- SMN1 deletion testing
- Distinguishing Features
- Subacute, rash (dermatomyositis), tender muscles
- Key Test
- EMG, MRI, biopsy, autoantibodies
- Distinguishing Features
- Hypotonia/weakness from birth, slowly progressive, normal/low CK
- Key Test
- Muscle biopsy; gene panel
- Distinguishing Features
- Isolated equinus, normal strength and CK, no Gowers'
- Key Test
- Normal CK reassures; observe
Any boy with delayed walking, toe-walking or a "clumsy" gait should have a serum CK checked before an orthopaedic procedure such as Achilles lengthening. Operating on an undiagnosed dystrophinopathy without anaesthetic precautions risks succinylcholine-induced hyperkalaemic cardiac arrest.
Management Algorithm
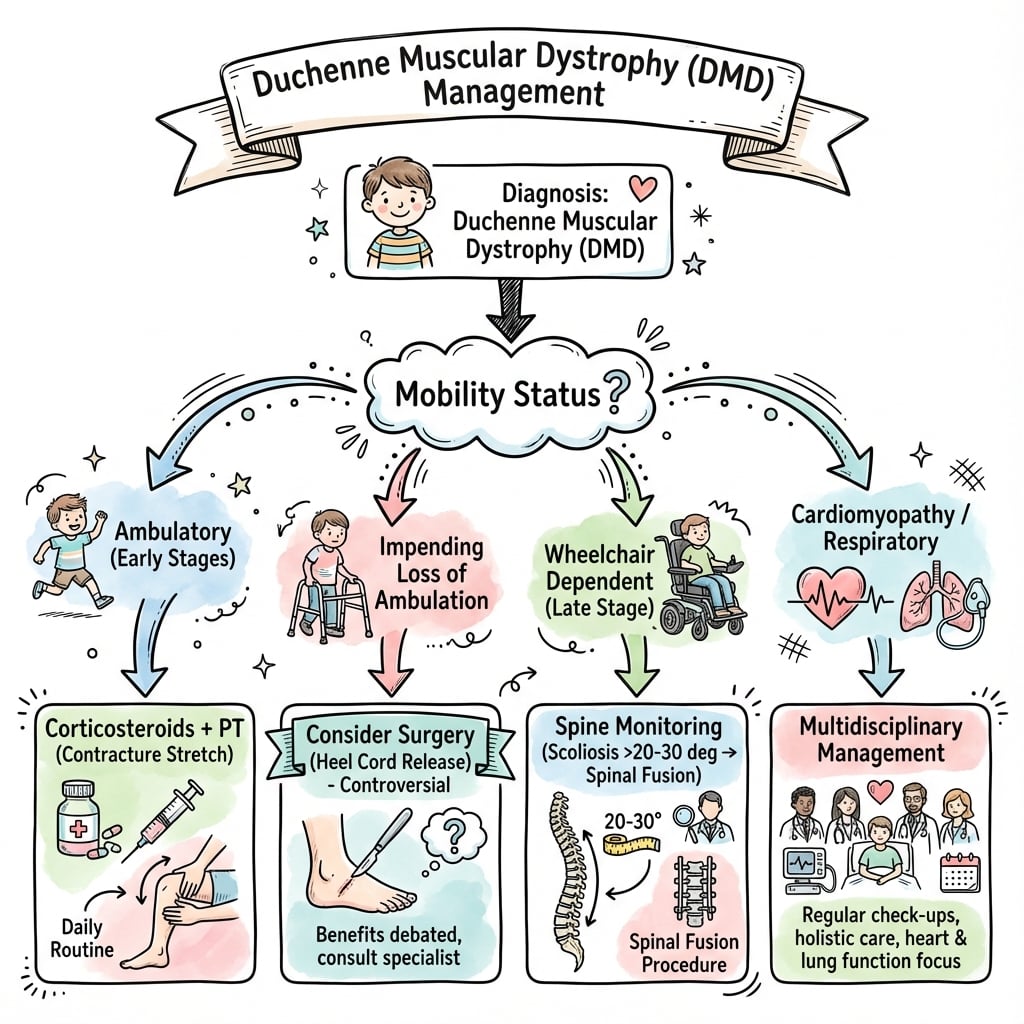
Ambulatory Phase (Age 5-12)
Goal: Prolong Ambulation.
- Steroids: Prednisolone or Deflazacort.
- Prolongs ambulation by ~2 years.
- Delays scoliosis onset.
- Side effects: Weight gain, Osteoporosis, Cataracts.
- Physiotherapy: Stretching (Equinus, Hip flexors, ITB).
- Orthotics: Night AFOs for equinus. KAFOs occasionally.
- Surgery (Ambulatory):
- Achilles Lengthening: For fixed equinus.
- ITB Release: For hip abduction contracture.
- Fracture Prevention: Calcium, Vitamin D. Bisphosphonates if osteoporosis.
Scoliosis Management
- Scoliosis develops in nearly 100% of DMD patients after loss of ambulation.
- Progression is rapid (~15-20 degrees/year).
- Cobb angle greater than 20-30 degrees AND progressing.
- FVC greater than 35% (some say greater than 30%) - Below this, perioperative risk is very high.
- Posterior Spinal Fusion (PSF): T2/T3 to Pelvis (Iliac or S1 Alar-Iliac screws).
- Instrumentation: Segmental pedicle screws.
- No Anterior Release: Usually not needed.
- Anesthesia: TIVA (Total Intravenous Anesthesia). Avoid succinylcholine and volatiles (MH risk).
- Blood Loss: Expect significant. Cell salvage, Tranexamic acid.
- ICU: Often require post-op ICU. May need prolonged NIV.
- Halts scoliosis progression.
- Maintains sitting balance.
- May improve respiratory function or slow decline.
20/20Scoliosis Decision
Hook:Fuse early in DMD scoliosis.
Surgical Technique
Posterior Spinal Fusion for DMD Scoliosis
- Pre-op: Optimize cardiac/respiratory. FVC assessment. Cardiac echo. MDT planning.
- Anesthesia: TIVA (Propofol, Remifentanil). Avoid Succinylcholine/Volatiles.
- Positioning: Prone on Jackson frame.
- Exposure: Midline incision T2 to Pelvis.
- Instrumentation:
- Pedicle screws T3-L5.
- Iliac screws or S2 Alar-Iliac screws.
- Cobalt-chrome rods.
- Correction: Cantilever, Rod rotation.
- Fusion: Decorticate, Bone graft.
- Closure: Layered. Drain.
- Post-op: ICU. Early mobilization. NIV if needed.
Complications
- Risk Factor
- Low FVC, Post-op
- Management
- NIV, ICU care
- Risk Factor
- Cardiomyopathy
- Management
- Cardiology involvement
- Risk Factor
- Anesthetic
- Management
- TIVA protocol
- Risk Factor
- Spinal surgery
- Management
- Cell salvage, TXA
- Risk Factor
- Steroids, Immobility
- Management
- Conservative care
- Risk Factor
- Poor healing
- Management
- Optimize nutrition
Postoperative Care
- ICU admission (often 24-48 hours).
- NIV if respiratory compromise.
- Early mobilization to wheelchair (Day 2-3).
- Wound care.
- No brace required (rigid instrumentation).
- Cast 4-6 weeks.
- AFOs after cast removal.
- Intensive physiotherapy.
Outcomes
- With Modern Care: Life expectancy now 20-30 years (previously teens).
- Steroids: Prolong ambulation ~2 years. Delay scoliosis.
- Spinal Fusion: Halts scoliosis progression. Maintains sitting posture. May improve QOL.
Guidelines, Registries & Global Practice
Global epidemiology:
- Birth incidence approximately 1 in 3,500-5,000 live male births; one of the most common lethal childhood genetic disorders worldwide.
- Roughly one-third of cases arise from de novo mutations with no family history.
- With contemporary multidisciplinary care (daily steroids, cardiac and respiratory support, spinal surgery), median survival has risen from the teens into the late 20s-30s.
Side-by-side guidance:
- Focus
- Whole-of-disease MDT care
- Key Recommendation
- Daily glucocorticoids; anticipatory cardiac, respiratory, bone and orthopaedic surveillance across the lifespan
- Focus
- Pharmacological therapy
- Key Recommendation
- Corticosteroids improve strength and function and should be offered (practice parameter, since superseded by care considerations)
- Focus
- Service organisation
- Key Recommendation
- Care through specialist neuromuscular MDT hubs; structured transition to adult services
- Focus
- Cardiomyopathy
- Key Recommendation
- Baseline and surveillance cardiac imaging; early ACE inhibitor/ARB +/- beta-blocker even before symptomatic dysfunction
- National and international DMD registries (e.g. TREAT-NMD network, the UK NorthStar database, US MD STARnet surveillance) track ambulation, scoliosis surgery rates, cardiac and respiratory milestones and feed trial recruitment.
- Registry data document the falling incidence of spinal fusion in the daily-steroid era and the rising age at loss of ambulation.
- Well-resourced settings: genetic confirmation, daily steroids, non-invasive ventilation, cardiac pharmacotherapy, posterior spinal fusion with segmental instrumentation, and access (variably) to exon-skipping or gene therapy.
- Limited-resource settings: diagnosis may rely on CK and clinical phenotype with limited genetic testing; steroids and bracing remain the mainstay; ventilatory and spinal-surgery access may be constrained, shifting emphasis toward seating, contracture prevention and palliative goals.
Controversies & Areas of Uncertainty
- Glucocorticoid regimen: The FOR-DMD randomised trial showed daily prednisone and daily deflazacort both outperform the 10-days-on/10-days-off intermittent regimen, with no significant difference between the two daily drugs. Deflazacort causes less weight gain and fewer behavioural effects but worse growth and more cataracts. Vamorolone (a dissociative steroid) is an emerging alternative with a potentially better bone/growth profile. The "best" regimen remains individualised.
- Should the pelvis always be fused? Long constructs to the pelvis control pelvic obliquity but increase operative time, blood loss and implant prominence. Some series of early, limited instrumentation in low curves (correcting before pelvic obliquity is fixed) report good seating with shorter, lower-morbidity surgery. Threshold of pelvic obliquity at which pelvic fixation becomes mandatory is debated.
- Has steroid use changed the scoliosis equation? Daily glucocorticoids dramatically reduce the incidence and severity of scoliosis, so far fewer steroid-treated boys now require spinal fusion than in the pre-steroid era. The classic teaching of near-universal, rapidly progressive scoliosis largely predates routine daily steroids.
- Are volatile anaesthetics absolutely contraindicated? Succinylcholine is unequivocally contraindicated (hyperkalaemic arrest). The risk from modern volatile agents (rhabdomyolysis/hyperkalaemia) is real but lower; many centres still use total intravenous anaesthesia as the safest default, while acknowledging the volatile-agent recommendation is less absolute.
- Disease-modifying genetic therapy: Exon-skipping antisense oligonucleotides (eteplirsen for exon 51-amenable mutations and related agents) and micro-dystrophin gene therapy (delandistrogene moxeparvovec) are approved in some regions but produce only partial dystrophin restoration; durable functional benefit, cost and access remain uncertain. They supplement, not replace, multidisciplinary musculoskeletal care.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is your diagnosis and approach?”
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is your management?”
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Discuss the key points.”
MCQ Practice Points
Q: What is the inheritance pattern of Duchenne Muscular Dystrophy? A: X-linked recessive. Affects males. Females are carriers.
Q: What does Gowers' sign indicate? A: Proximal muscle weakness (hip extensors, gluteals). The child uses their hands on thighs to 'climb up' themselves to stand from the floor.
Q: What is the typical CK level in DMD? A: Massively elevated - 10-100 times normal (often greater than 10,000 U/L).
Q: When is spinal fusion indicated in DMD scoliosis? A: Cobb angle greater than 20-30 degrees and progressing, with FVC greater than 30-35%.
Q: What anesthetic agents should be avoided in DMD? A: Succinylcholine (causes hyperkalemic cardiac arrest) and Volatile anesthetics (risk of rhabdomyolysis/MH-like reaction). Use TIVA.
Key Features
- X-linked recessive
- Dystrophin absent
- CK 10-100x elevated
- Gowers' sign
- Calf pseudohypertrophy
Natural History
- Onset 3-5 years
- Wheelchair ~12 years
- Scoliosis after WC
- Life exp 20-30 years
Orthopaedic Rx
- Steroids (prolong amb)
- Stretching/AFOs
- Achilles length (equinus)
- Spine fusion (scoliosis)
Anesthesia
- AVOID Succinylcholine
- AVOID Volatiles
- USE TIVA
- Pre-op Cardiac Echo
Evidence Base
FOR-DMD: Optimal Steroid Regimen (RCT)
- Double-blind RCT, 196 steroid-naive boys aged 4-7, 5 countries, 3-year follow-up.
- Daily prednisone and daily deflazacort both superior to intermittent (10-on/10-off) prednisone on a composite of rise-from-floor velocity, FVC and treatment satisfaction.
- No significant difference between the two daily regimens.
DMD Care Considerations: Orthopaedic & Systemic Management
- International consensus on respiratory, cardiac, bone-health and orthopaedic/surgical care.
- Daily glucocorticoids have reduced scoliosis incidence and altered natural history.
- Multidisciplinary, anticipatory care underpins improved survival and quality of life.
Spinal Stabilisation Preserves Respiratory Function & Survival
- Comparative study: 32 operated vs 23 who refused spinal stabilisation.
- Non-operated FVC fell ~8% per year; operated FVC static for 36 months.
- Scoliosis progressed 37 to 89 degrees in non-operated vs improved 47 to 34 degrees operated; survival significantly better after stabilisation.
Anaesthesia in Dystrophinopathy: Succinylcholine is Lethal
- Retrospective review of 117 anaesthetic exposures in 47 DMD/BMD patients.
- One patient given succinylcholine developed rhabdomyolysis and hyperkalaemic cardiac arrest.
- Volatile agents were used 66 times without attributable MH-type events, supporting that the volatile contraindication is less absolute than for succinylcholine.
Early Limited Instrumentation for DMD Scoliosis
- Retrospective cohort of 41 DMD patients with single-rod, limited posterior fusion.
- Mean Cobb improved 24.3 to 15.6 degrees; pelvic obliquity 7 to 5 degrees; no perioperative mortality.
- Operating early on smaller curves gave satisfactory seating with low morbidity (mean blood loss 2.3 L, ICU 41 h).
Eteplirsen: Exon-Skipping Dystrophin Restoration (Landmark)
- Double-blind placebo-controlled trial in boys with exon 51-skippable deletions.
- Dystrophin-positive fibres rose to ~52% of normal by week 48; treatment increase driven by duration more than dose.
- Eteplirsen-treated patients showed a 67.3 m benefit on the 6-minute walk test vs placebo/delayed.
Deflazacort vs Prednisone: Comparative Profile
- Synthesis of RCT and prospective data on the two standard-of-care steroids.
- Deflazacort: similar or slower functional decline, less weight gain and fewer behavioural effects.
- Deflazacort: worse growth, bone health and more cataracts than prednisone/prednisolone.