Pes Planus | Physiological | Jack's Test
- Natural History: Most infants have flat feet. The arch develops spontaneously within the first decade of life. 90% resolve by age 10.
- Physiological vs Pathological: Flexible, painless flatfoot is physiological. Painful or rigid flatfoot is pathological.
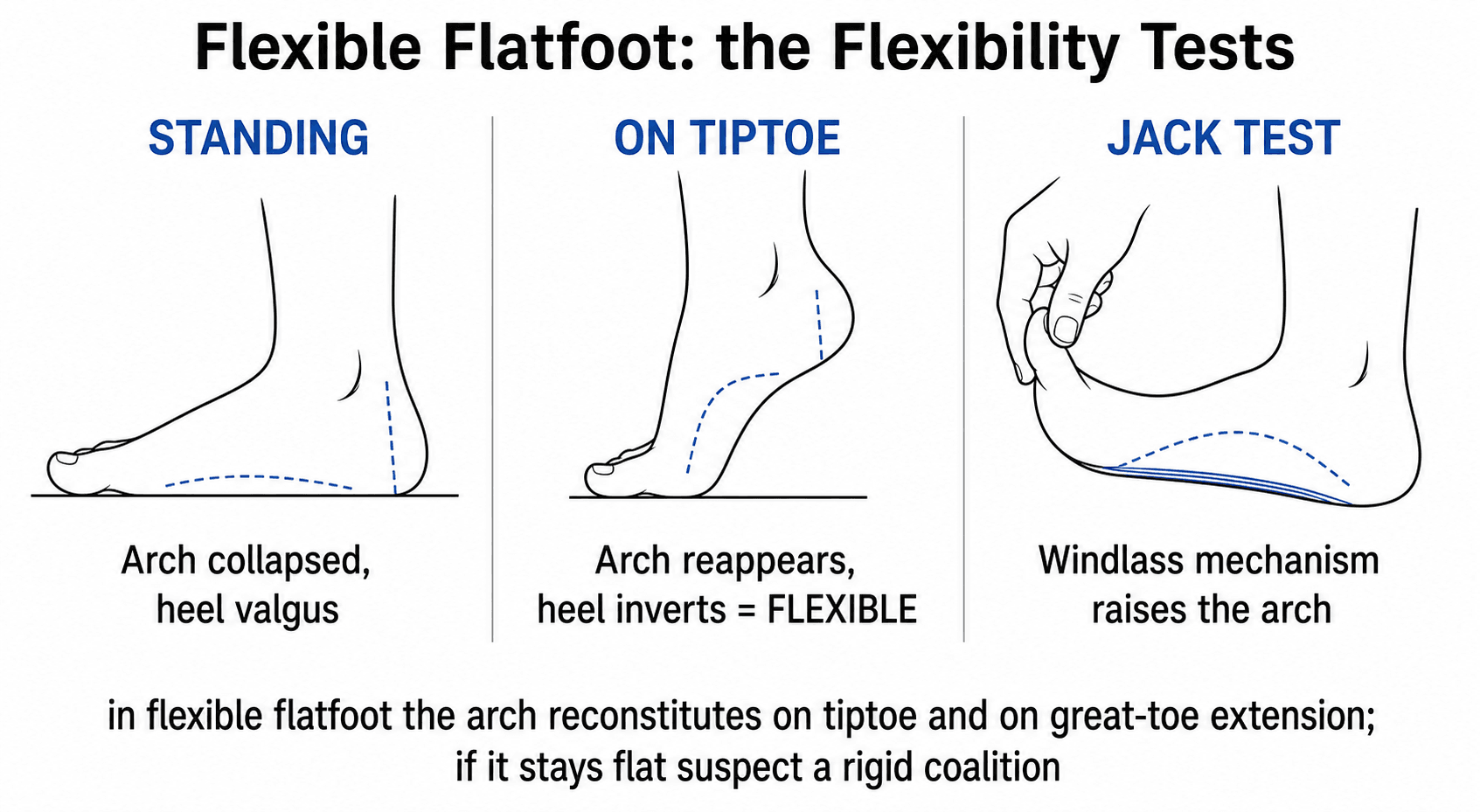
- Jack's Test: Passive extension of the big toe engages the Windlass mechanism. If the arch reconstitutes, it is flexible.
- Treatment: Asymptomatic flexible flatfoot requires NO treatment (no orthotics). Symptomatic cases start with calf stretching.
- “Look at the parents' feet. It is often familial.
- “Always check the shoes for wear patterns. Uneven medial wear suggests significant pronation.
- “Don't forget to assess generalized ligamentous laxity (Beighton Score).
It's not flexible. If the arch stays flat on toe-raise, suspect Tarsal Coalition. Look for peroneal spasm ("Peroneal Spastic Flatfoot").
Rocker Bottom. In congenital vertical talus (CVT), the foot is rigid and the sole is convex. This is NOT a flexible flatfoot.
- Flexible
- Arch Reappears
- Rigid (Coalition/CVT)
- Flat remains
- Flexible
- Arch Reappears
- Rigid (Coalition/CVT)
- Flat remains
- Flexible
- Normal / Hypermobile
- Rigid (Coalition/CVT)
- Restricted / Absent
- Flexible
- Usually Painless
- Rigid (Coalition/CVT)
- Often Painful
PAINRed Flags
Hook:PAIN is not normal.
Definitions
Flat foot. Technically defined as valgus of the hindfoot, abduction of the forefoot, and depression of the medial longitudinal arch.
Emphasizes the valgus component of the heel.
The deformity is reducible. The joints (Subtalar, TN, CC) are mobile.
A lateral column lengthening procedure. The "Workhorse" for severe flatfoot correction.
"To prop up". Surgical limitation of joint motion (without fusion) using an implant.
Overview and Epidemiology
Flexible Flatfoot (Pes Planus) is the most common reason for referral to a pediatric orthopaedic clinic.
- Definition: Loss of the medial longitudinal arch that is present only during weight bearing, and resolves when non-weight bearing or during the Windlass maneuver.
- Natural History:
- The arch is naturally flat in neonates due to a fat pad and laxity.
- As the neuromuscular system matures, the arch develops.
- Morley (1964) showed 97% of 2-year-olds are flat, but only 4% of 10-year-olds.
- Therefore, spontaneous resolution is the rule.
Etiology:
- Ligamentous Laxity: Generalized (Ehlers-Danlos, Marfan, Down Syndrome) or isolated familial laxity.
- Obesity: Increases load on the arch.
- W-sitting: Associated with femoral anteversion and external tibial torsion ("Miserable Malalignment").
Pathophysiology and Mechanisms
The Talonavicular joint is the keystone of the arch. In flatfoot, the talus head uncovers medially and plantarward (Peritalar subluxation).
- Hindfoot Valgus: The calcaneus goes into valgus.
- Forefoot Abduction: The midfoot breaks, and forefoot abducts relative to hindfoot.
- Achilles Tension: With the hindfoot in valgus, the Achilles tendon becomes a DEFORMING force (it is now lateral to the axis of the subtalar joint), acting as an evertor.
- Medial Column: The Spring Ligament (Calcaneonavicular) and Tibialis Posterior stretch out.
- Spring Ligament:
- Superomedial band: The most important stabilizer.
- Inferoplantar band: Supports the head of talus.
- Tibialis Posterior:
- Primary dynamic stabilizer of the arch.
- Inserts on the Navicular tuberosity + slips to cuneiforms/cuboid/metatarsals (2,3,4).
- Failure leads to flatfoot (Adult Acquired), but in kids, it's usually laxity not rupture.
- Spring Ligament:
- Lateral Column: Theoretically shortened relative to the medial column in flatfoot (hence lengthening corrects it).
- Heel Strike: Calcaneus everts (unlocking subtalar joint) for shock absorption.
- Mid-Stance: Subtalar joint inverts (locking MTJ) to create a rigid lever for push-off.
- In Flatfoot, the foot remains everted and unlocked throughout stance, leading to inefficient gait.
- Extending the Hallux pulls the Plantar Aponeurosis.
- This shortens the distance between calcaneus and metatarsal heads.
- This elevates the arch and inverts the hindfoot.
- In Flexible Flatfoot, this mechanism is INTACT.
- In Rigid Flatfoot, it is blocked.
Classification
Harris and Beath (1947)
Classified based on talo-calcaneal overlap on weight bearing footprint (Harris Mat).
- Type I: Arch present.
- Type II: Arch absent, heel valgus. (Flexible).
- Type III: Rigid flatfoot (Coalition).
Most flexible feet are Type II.
Clinical Assessment
Clinical Flow
- Pain: Where? (Sinus tarsi impinging vs Medial strain).
- Activity: "Tired legs", "Refuses to walk distances".
- History: Prematurity? Developmental delay? Family history.
- Too Many Toes Sign: Viewed from behind. Seeing greater than 1.5 toes laterally suggests forefoot abduction.
- Heel Valgus: Assess relationship of heel to leg.
- Arch: Is it absent?
- Toe Raise Test: Ask child to stand on tiptoes. Heel should invert (varus) and arch usually appears.
- Jack's Test: Passively extend big toe in standing. Arch should rise.
- Gait: Check for antalgic gait or internal rotation.
- Silfverskiold Test: Differentiate Gastroc vs Soleus tightness. (Dorsiflexion with knee straight vs bent).
- Subtalar ROM: Must be free.
- Correction: Can you passively correct the foot to neutral?
A tight Achilles (Gastrocnemius) is the most common cause of Symptomatic flexible flatfoot. The tight triceps surae prevents dorsiflexion at the ankle, so the midfoot "breaks" (dorsiflexes) to allow the foot to clear the ground, worsening the flatfoot.
JACKAssessment Steps
Hook:Know JACK about flat feet.
Investigations
X-rays (Weight Bearing): Usually not needed for physiologic flatfoot, but indicated for pain or rigidity.
- Views: AP and Lateral Weight Bearing. Harris (Saltzman) view for hindfoot alignment.
- Normal
- 0 degrees (Straight line)
- Flatfoot
- Convex downwards (Sag)
- Normal
- 20-30 degrees
- Flatfoot
- Decreased (less than 15 even negative)
- Normal
- Aligned
- Flatfoot
- Lateral subluxation of Navicular


CT/MRI:
- Only if suspecting coalition (CT) or tendon pathology (MRI). Not routine.
Differential Diagnosis
The key clinical task is separating benign physiological flexible flatfoot from the pathological mimics that share a "flat" appearance. Flexibility (arch restores on toe-raise/Jack's test) and painlessness are the great discriminators.
- Flexibility
- Flexible, painless
- Key Discriminator
- Arch restores on tiptoe; normal subtalar motion; often familial
- Action
- Reassurance, no imaging
- Flexibility
- Flexible but symptomatic
- Key Discriminator
- Positive Silfverskiold; midfoot break on dorsiflexion
- Action
- Calf stretching first line
- Flexibility
- Rigid
- Key Discriminator
- Loss of subtalar motion, peroneal spasm, C-sign on lateral X-ray, age 8-12
- Action
- CT to characterise bar
- Flexibility
- Rigid (neonatal)
- Key Discriminator
- Rocker-bottom sole, vertical talus on forced-plantarflexion lateral film, dorsal navicular dislocation
- Action
- Reverse-Ponseti +/- surgery
- Flexibility
- Often flexible early
- Key Discriminator
- Medial prominence and tenderness over navicular; single-heel-raise weakness in adolescents
- Action
- Imaging, immobilisation, selective surgery
- Flexibility
- Variable
- Key Discriminator
- Spasticity, equinus, asymmetry, global motor signs
- Action
- Treat underlying condition; bony correction if disabling
- Flexibility
- Flexible
- Key Discriminator
- Forefoot adduction with hindfoot valgus (S-shaped lateral border)
- Action
- Distinguish before any lengthening
Tarsal Coalition: the Rigid-Flatfoot Mimic
The most important pathological cause of a rigid flatfoot is a tarsal coalition - an abnormal fibrous, cartilaginous or bony bridge between two tarsal bones that restricts subtalar/midtarsal motion. It is the classic cause of the "peroneal spastic flatfoot," in which the peroneal muscles spasm to splint a painful, stiff hindfoot.
The two common types (about 90% of coalitions):
- Calcaneonavicular (CN)
- 8-12 years (ossifies earlier)
- Talocalcaneal (TC)
- 12-16 years (ossifies later)
- Calcaneonavicular (CN)
- 45-degree oblique foot
- Talocalcaneal (TC)
- Lateral and Harris axial
- Calcaneonavicular (CN)
- 'Anteater nose' (elongated anterior calcaneal process)
- Talocalcaneal (TC)
- 'C-sign' and talar beaking on lateral; middle-facet obliquity
- Calcaneonavicular (CN)
- CT (MRI for a fibrous bar)
- Talocalcaneal (TC)
- CT (defines the middle-facet bar)
Management:
- First-line is non-operative (activity modification, a period of cast/boot immobilisation for a painful flare, orthoses).
- For refractory symptoms, resection of the bar with interposition (extensor digitorum brevis or fat for CN coalitions) preserves motion and is favoured in the young foot when there is little subtalar arthrosis.
- A large talocalcaneal coalition (involving more than about half of the joint) or established subtalar arthrosis is better treated by arthrodesis than resection.
A rigid, painful flatfoot with restricted subtalar motion and peroneal spasm in a child of 8-16 is a tarsal coalition until proven otherwise. Look for the anteater nose sign (calcaneonavicular, ~8-12 y, oblique film) or the C-sign / talar beak (talocalcaneal, ~12-16 y, lateral film); confirm and characterise with CT.
Management Algorithm
The Painless Flatfoot
- Reassurance: Explain natural history.
- Education: "The arch is like height - some are tall, some are short. Flat is just a variant."
- No Orthotics: Evidence shows orthotics do NOT change the shape of the foot or arch development (Wenger et al 1989). They are expensive and uncomfortable.
- Shoe Wear: Supportive heel counter shoes are fine, but barefoot walking is also healthy.
Do not treat X-rays.
Surgical Technique
Surgery aims to realign the foot. It is often a "A la carte" menu depending on the deformity.
Joint Sparing Osteotomies (Preferred)
Realigns anatomy without fusing joints.
-
Calcaneal Lengthening (Evans):
- Concept: Lengthens the lateral column. Pushes the navicular (and forefoot) medially, reducing abduction.
- Technique: Osteotomy 1.5cm proximal to CC joint. Insert trapezoidal bone graft.
- Effect: Corrects Forefoot Abduction AND Hindfoot Valgus.
- Risk: CC joint arthritis (increased pressure).
-
Medial Slide (Koutsogiannis):
- Concept: Translates posterior calcanues medially. Changes the pull of Achilles from evertor to invertor.
- Effect: Corrects Hindfoot Valgus only. Little effect on arch height.
-
Cotton Osteotomy:
- Concept: Opening wedge plantarflexion osteotomy of the Medial Cuneiform.
- Effect: Restores the medial column height (Arch).
- Indication: Persistent forefoot varus (supination) AFTER the heel is corrected. If you fix the heel and the big toe creates a "tripod" effect off the ground, you need to bring the ray down (Cotton).
- Graft: Use a wedge (Allograft or Autograft). Fix with a staple or plate.
-
Mosca Procedure:
- Combination of Evans + Soft tissue plication.
- Gold standard for severe deformity.
- Steps:
- Approach lateral calcaneus.
- Osteotomy and graft (Evans).
- Medial approach.
- Plication of Talonavicular capsule (advancing the spring ligament).
- TAL (Percutaneous).
CALMSurgical Options
Hook:CALM the painful foot.
Complications
- Specific Risk
- CC Joint Arthritis / Dorsal Subluxation
- Prevention
- Don't over-stuff the graft.
- Specific Risk
- Sural Nerve Injury
- Prevention
- Careful dissection laterally.
- Specific Risk
- Sinus Tarsi Pain
- Prevention
- Remove implant.
- Specific Risk
- Under-correction
- Prevention
- Address both limited Equinus and Valgus.
Postoperative Care and Rehabilitation
Protocol (Osteotomy)
- Non-Weight Bearing (NWB): Cast applied.
- Elevation: Critical for swelling control.
- X-ray: Check graft healing at 6 weeks.
- Aircast Boot: Weight bearing as tolerated (guided by X-ray).
- ROM: Start Ankle and Subtalar ROM.
- Transition: Into supportive runners.
- Physio: Gait training, calf stretching (prevent recurrence of equinus).
- Return to Play: When fusion solid and strength regained.
- Plyometrics: Hopping, skipping to recruit peroneals and tib post.
- Orthotics?: Generally NOT needed post-op, but some surgeons use arch supports for transition.
- Exercise
- Wall Stretch / Night Splint
- Rationale
- Corrects Equinus driver
- Exercise
- Heel Raises with Ball squeeze
- Rationale
- Dynamic arch support
- Exercise
- Towel gather / Marble pick-up
- Rationale
- Core strength of foot
- Exercise
- Balance Board
- Rationale
- Ankle stability
Outcomes
- Pain Relief: Reported as 90% good/excellent in long term studies (Mosca).
- Deformity Correction: Excellent restoration of arch and alignment.
- Complications:
- Calcaneocuboid OA: Due to increased joint pressure from the graft. Often asymptomatic.
- Lateral column pain: Hardware prominence or graft non-union.
- Under-correction: If the Equinus is not addressed (TAL).
- Asymptomatic flexible flatfoot does NOT lead to disability in adulthood.
- It is a variant of normal.
Guidelines, Registries & Global Practice
Global Epidemiology:
- One of the commonest reasons for paediatric orthopaedic referral worldwide; the great majority are physiological.
- Prevalence is strongly age-dependent: ~44% at ages 3-6 falling to ~24% by age 6 (Pfeiffer, Pediatrics 2006), and only a few percent of 10-year-olds retain a flat arch as the medial arch matures through the first decade.
- Higher prevalence with male sex, overweight/obesity, and generalised ligamentous laxity; pathological (rigid) flatfoot accounts for under 1%.
- Often presents as "grandmother concern" — a normal-looking variant raised by an anxious family member rather than a symptomatic child.
Side-by-Side Society Guidance:
- Imaging stance
- No imaging for painless flexible foot
- Orthotics / shoes
- Not to alter arch; symptom relief only
- Surgery threshold
- Reserved for pain refractory to non-op care
- Imaging stance
- Weight-bearing films only if pain or rigidity
- Orthotics / shoes
- Reassurance first; insoles for symptoms
- Surgery threshold
- Symptomatic, flexible, failed conservative Rx
- Imaging stance
- Do NOT X-ray painless flexible feet
- Orthotics / shoes
- Do NOT prescribe to asymptomatic children
- Surgery threshold
- Refer only if rigid, painful or atypical
- Imaging stance
- Selective imaging
- Orthotics / shoes
- More liberal use of arthroereisis in some centres
- Surgery threshold
- Earlier surgical interest in selected cases
The major point of genuine international divergence is subtalar arthroereisis: relatively popular in parts of continental Europe, but viewed with caution in the UK, North America and Australasia given low-level evidence and removal rates of roughly 7-19% (Metcalfe, Foot Ankle Int 2011).
- There is no dedicated implant registry for paediatric flatfoot. Arthroereisis "spacers" are device implants, so where national implant or device registries exist (e.g. orthopaedic device tracking schemes), outcomes and removal events should be captured the same way as any implant; the absence of long-term registry data is itself a reason for caution.
- High-resource settings: Risk is over-investigation and over-treatment (unnecessary X-rays, custom orthoses, premature surgery) for what is usually a normal variant; ethical counselling — "we treat the child, not the radiograph" — is the priority.
- Limited-resource settings: Custom orthoses and elective reconstruction may be unaffordable; emphasis falls on examination-based diagnosis, reassurance, simple calf-stretching programmes, and reserving theatre time for genuinely disabling or rigid deformity.
- Rigid foot or absent subtalar motion (suspect tarsal coalition or congenital vertical talus).
- Unilateral or asymmetric deformity.
- Pain or callosity limiting walking/sport.
- Failure of a supervised calf-stretching programme over roughly 6 months.
Controversies & Areas of Uncertainty
There is no robust evidence that an asymptomatic flexible flatfoot in childhood causes pain, osteoarthritis or disability in adulthood. Anchoring treatment to a feared future is not supported.
Persistent international divide. Proponents cite minimally invasive correction during growth; critics cite low-level evidence and removal rates of ~7-19% (Metcalfe 2011). No controlled trial shows benefit over natural history.
For the (uncommon) symptomatic child, expensive custom devices have not been shown to outperform simple supportive footwear or off-the-shelf insoles for symptom relief; neither alters the arch.
No agreed radiographic cut-off triggers surgery. Decisions are symptom-led, with debate over how long to persist with stretching and whether to operate before or after skeletal maturity.
Unresolved questions for higher-level study:
- Lack of validated, disease-specific paediatric patient-reported outcome measures hampers comparison across procedures.
- The relative contribution of each "a la carte" component (lengthening vs medial column vs soft tissue vs gastrocnemius recession) is poorly isolated because procedures are usually combined.
- Optimal management of the borderline symptomatic adolescent (mild pain, very flexible foot) remains opinion-based.
MCQ Practice Points
Q: What is the most common potential complication of a lateral column lengthening (Evans)? A: Calcaneocuboid joint arthritis (due to increased joint pressure) or Dorsal subluxation of the CC joint.
Q: At what age do most flexible flat feet resolve? A: By age 10 years. The arch development curve plateaus at this age. If it hasn't formed by 10, it likely won't.
Q: What mechanism is tested by passive extension of the hallux? A: The Windlass Mechanism (Shortening of plantar fascia elevates the arch).
Q: If the arch does NOT reconstitute on toe standing, what is the likely diagnosis? A: Rigid Flatfoot (Tarsal Coalition or Vertical Talus).
Q: What soft tissue contracture is most strongly associated with symptomatic flatfoot? A: Gastrocnemius-Soleus complex (Achilles) tightness. Always test with the knee straight (Gastroc) and bent (Soleus) - Silfverskiold Test.
Q: How do you clinically differentiate Oblique Talus (Severe Flatfoot) from Vertical Talus (CVT)? A: In CVT, the foot is rigid and the hindfoot is in valgus but the forefoot is dorsiflexed (Rocker Bottom). You can palpate the head of the talus in the sole. In flexible/oblique talus, the deformity reduces.
Q: Which nerve is at risk during the lateral approach for a Medial Slide calcaneal osteotomy? A: The Sural Nerve. It runs with the small saphenous vein posterior to the lateral malleolus.
Q: What is the 'C-Sign' on a lateral foot X-ray indicative of? A: Talocalcaneal coalition. It represents a bony bridge between the talus and calcaneus.
Q: What happens to the calcaneal pitch angle in flatfoot? A: It decreases (flattens), often becoming less than 15 degrees or even negative (rocker bottom).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A worried mother brings her 2-year-old son. He has flat feet. 'His dad has flat feet too'. He runs and plays without pain.”
“A 12-year-old boy has painful flat feet. Medial arch pain. Short calf muscles. Flexible on exam.”
“Discuss the role of Arthroereisis (Subtalar screw).”
Diagnosis
- Flexible: Arch restores on tiptoe
- Rigid: Arch stays flat (Coalition)
- Physiological: Painless
- Pathological: Painful / Rigid
- Vertical Talus: Rocker Bottom
Assessment
- Jack's Test (Windlass)
- Toe Raise Test
- Silfverskiold (Equinus)
- General Laxity (Beighton)
- Too Many Toes Sign
Management
- Asymptomatic: Reassurance
- Symptomatic: Stretch & Orthotics
- Surgery: Evans Osteotomy
- Always lengthen Achilles
- Avoid Arthroereisis (Risk)
Evidence Base
Evidence below verified against PubMed. DOIs link to the primary record where one exists.
Corrective Shoes/Inserts Do Not Change Natural History (Landmark RCT)
- Prospective RCT of 129 children with radiographic flatfoot randomised to controls, corrective orthopaedic shoes, Helfet heel-cup, or custom-molded insert; 98 completed minimum 3 years of treatment.
- Radiographs improved significantly in ALL groups including untreated controls (p less than 0.01).
- NO significant difference between controls and any treated group (p greater than 0.4).
- Wearing corrective shoes or inserts for 3 years does not influence the course of flexible flatfoot.
Calcaneal Lengthening for Symptomatic Hindfoot Valgus
- 31 severe symptomatic valgus feet (flatfoot/skewfoot) in 20 children corrected with a modified Evans calcaneal lengthening osteotomy.
- Satisfactory clinical and radiographic correction of all components in all but the two most severely deformed feet.
- Pain and plantar callus resolved; subtalar motion preserved (avoiding arthrodesis).
- Medial cuneiform opening-wedge osteotomy added for forefoot supination in skewfeet.
Subtalar Arthroereisis - Critical Review
- Critical review of 76 studies of arthroereisis for paediatric flexible flatfoot.
- Most radiographic parameters improved; calcaneal inclination changed least.
- Complication rates 4.8% to 18.6%; unplanned implant removal rates 7.1% to 19.3% across device types.
- All evidence is consecutive case series or case reports - no controlled comparison with natural history.
Flatfoot Prevalence, Age, Sex and Weight
- 835 children aged 3-6 assessed by laser surface scanning.
- Flexible flatfoot prevalence 44% overall, falling from 54% at age 3 to 24% at age 6; pathological flatfoot under 1%.
- Boys affected more than girls (52% vs 36%); significant association with overweight/obesity.
- Over 90% of treatments given (10% wore arch supports) were judged unnecessary.
Original Lateral Column Lengthening (Calcaneo-valgus)
- Original description: in calcaneo-valgus the lateral column is short relative to the medial column.
- Cortical tibial bone graft inserted to elongate the anterior calcaneus, equalising column lengths.
- Elongating the lateral column swings the forefoot medially, correcting valgus, abduction and sag.
- Conceptual basis for the modern Evans/Mosca lengthening.
Addressing Equinus Improves Flatfoot Surgery Outcomes
- 34 symptomatic flexible flatfeet in 20 children treated with gastrocnemius recession plus subtalar arthroereisis.
- Mean AOFAS Ankle-Hindfoot score improved 21.3 points (67.7 to 89, p less than 0.0001).
- Authors emphasise correcting the underlying equinus deformity as key to optimising outcomes.
- Subjective pain, function, cosmesis and shoe wear all improved.