Glucocerebrosidase Deficiency
- Glucocerebrosidase deficiency: Lipid accumulates in macrophages (Gaucher cells)
- Bone crises: Severe pain, fever - mimics osteomyelitis but culture negative
- AVN: Hip and shoulder common, may require arthroplasty
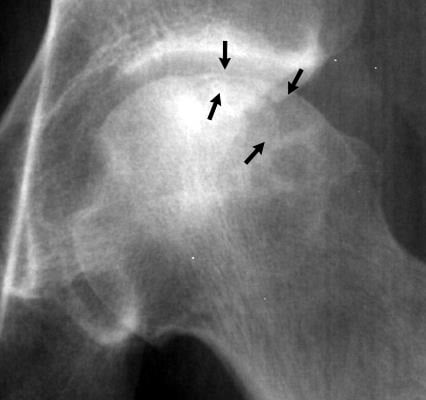
- Erlenmeyer flask deformity: Failure of distal femur remodeling
- ERT (Enzyme Replacement Therapy): First-line treatment, transformed prognosis
- “Erlenmeyer flask = failed metaphyseal remodeling
- “Bone crises are NOT infection - do not treat with antibiotics
- “ERT is mainstay of treatment
- “Autosomal recessive, high in Ashkenazi Jews
Key Concepts
Mimics osteomyelitis perfectly. Severe bone pain, fever, swelling, and elevated inflammatory markers (ESR/CRP). MRI shows marrow edema.
Culture Negative. Blood cultures and bone aspirate are sterile. This is an ischemic event (infarction), not an infection.
Do NOT treat with antibiotics. Antibiotics are ineffective and mask true infection if it develops later. Treat with aggressive analgesia, hydration, and steroids.
Epidemiology and Genetics
Gaucher disease is the most common lysosomal storage disorder.
- General population: 1 in 40,000-60,000
- Ashkenazi Jewish population: approximately 1 in 800 (carrier frequency around 1:15)
- In the ICGG Gaucher Registry (1698 patients, 38 countries), 94% had type 1, fewer than 1% type 2, and 5% type 3
- Autosomal recessive inheritance
- GBA gene mutation (chromosome 1q21)
- Encodes glucocerebrosidase (acid beta-glucosidase)
- Over 400 mutations identified
- Most common alleles in the Registry: N370S (53%), L444P (18%), 84GG (7%), IVS2+1 (2%)
- N370S is associated with the type 1 (non-neuronopathic) phenotype; L444P homozygosity is associated with more severe, often neuronopathic disease
- Genotype influences age at diagnosis (mean 27 years for N370S/N370S vs around 2 years for L444P/L444P)
Pathophysiology

- Glucocerebrosidase deficiency → glucocerebroside (glucosylceramide) cannot be degraded
- Substrate accumulates within macrophages, forming Gaucher cells
- Gaucher cells infiltrate bone marrow, spleen, liver, and lymph nodes
- Macrophages engorged with glucocerebroside
- "Crinkled tissue paper" or "wrinkled silk" cytoplasm
- Found in bone marrow, spleen, liver, lymph nodes
- Histiocytes 20-100 microns in diameter
-
Marrow Infiltration
- Gaucher cells replace normal marrow
- Decreased hematopoiesis → cytopenias
- Marrow expansion → cortical thinning
-
Vascular Compromise
- Marrow infiltration → ischemia
- Bone infarcts and bone crises
- AVN of femoral head, humeral head
-
Bone Remodeling Failure
- Interference with osteoclast/osteoblast function
- Failed metaphyseal remodeling → Erlenmeyer flask
- Osteopenia and pathological fractures
Classification
- Type 1
- Non-neuronopathic
- Type 2
- Acute neuronopathic
- Type 3
- Chronic neuronopathic
- Type 1
- 95% of cases
- Type 2
- Rare
- Type 3
- Rare
- Type 1
- Childhood to adult
- Type 2
- Infancy (under 2 years)
- Type 3
- Childhood
- Type 1
- None
- Type 2
- Severe, progressive
- Type 3
- Moderate, variable
- Type 1
- Common
- Type 2
- Not relevant (die early)
- Type 3
- Common
- Type 1
- Good with ERT
- Type 2
- Death in infancy
- Type 3
- Variable
The three classical types are distinguished by the presence and tempo of central nervous system involvement; skeletal disease is the dominant orthopaedic burden in Types 1 and 3.
Clinical Presentation
- Severe bone pain, often femur or tibia
- Fever, malaise
- Elevated ESR, CRP
- Mimics osteomyelitis - critical differential
- Caused by acute marrow ischemia/infarction
- May last days to weeks
- Treatment: analgesia, hydration, steroids
- Femoral head most common (40% of Type 1)
- Humeral head also affected
- Chronic marrow infiltration → vascular compromise
- May progress despite ERT if established
- Often requires arthroplasty
- Failure of metaphyseal remodeling
- Classic at distal femur
- Wide metaphysis, narrow diaphysis
- "Flask" shape on X-ray
- Bilateral and symmetric
- Does not cause symptoms directly
- Osteopenia from marrow expansion
- Cortical thinning
- Vertebral compression fractures
- Long bone fractures (often minimal trauma)
- Healing may be delayed
- Bone infarcts (medullary)
- Osteonecrosis of vertebrae
- Growth retardation in children
- Chronic bone pain
Investigations
- Glucocerebrosidase enzyme activity (leukocytes or fibroblasts)
- Under 15% of normal is diagnostic
- Genetic testing - GBA gene mutations
- Confirms diagnosis
- Allows family screening
- Chitotriosidase: Markedly elevated (biomarker)
- Acid phosphatase: Elevated
- Ferritin: Elevated
- CBC: Anemia, thrombocytopenia
- Coagulation: May be abnormal
- Plain X-rays: Erlenmeyer flask, osteopenia, lytic lesions
- MRI: Gold standard for bone assessment
- T1: Low signal (fatty marrow replacement)
- Bone marrow burden score
- AVN detection
- Bone infarcts
- CT: Hepatosplenomegaly assessment
- DXA: Bone mineral density
Gaucher-like ("pseudo-Gaucher") cells are NOT specific to Gaucher disease. Identical lipid-laden macrophages with crinkled cytoplasm appear in chronic myeloid leukaemia and other myeloproliferative/myelodysplastic disorders, thalassaemia and other haemoglobinopathies, multiple myeloma, and some chronic infections (for example mycobacterial). They reflect a high cell-turnover load on macrophages, not glucocerebrosidase deficiency. So a marrow reported as containing "Gaucher cells" must NOT be equated with Gaucher disease - the diagnosis is confirmed by low glucocerebrosidase (acid beta-glucosidase) enzyme activity in leukocytes, supported by GBA genotyping. It also follows that a bone marrow biopsy is not required to diagnose Gaucher disease.

Bone Marrow Burden Assessment
MRI Bone Marrow Burden Score:
- Quantifies severity of marrow infiltration
- Used to monitor treatment response
- Correlates with risk of bone complications
Severity Scoring:
- Points
- 0-8
- Points
- 0-8
- Points
- Additional points
Interpretation:
- Used to guide treatment intensity
- Monitor response to ERT
- Predict fracture risk
Paediatric Skeletal Disease and the Case for Early Treatment
Bone involvement frequently begins in childhood and adolescence, and the growing skeleton has features the adult does not - examiners testing the paediatric angle expect these:
- Growth failure and delayed bone age: marrow infiltration and the chronic metabolic burden retard linear growth and skeletal maturation, so many untreated children fall below their genetic height potential and have delayed puberty.
- Childhood bone crises and osteonecrosis: acute bone crises and AVN (hip, shoulder, proximal tibia) occur in children and adolescents, not only adults; a crisis in a child is again culture-negative infarction, not infection.
- Modelling failure during growth: because remodelling failure happens while the bone is still growing, the Erlenmeyer flask deformity and generalised osteopenia are established in childhood.
- Early enzyme replacement therapy is growth- and bone-protective: starting ERT early in symptomatic children can restore growth velocity, normalise bone age, and reduce the risk of irreversible AVN and pathological fracture. This is the strongest argument for prompt diagnosis and treatment in the paediatric patient - once AVN has occurred it does not reverse, so the window is before structural damage.
This is why paediatric Gaucher disease is managed by a metabolic team with growth, puberty and skeletal monitoring, and why there should be a low threshold for the diagnostic enzyme assay in a child with unexplained splenomegaly, cytopenia or bone pain.
Systemic Features
- Anemia (Gaucher cell marrow replacement)
- Thrombocytopenia (splenic sequestration)
- Bleeding tendency (both platelet and coagulation defects)
- Leukopenia (less common)
- Massive splenomegaly (25x normal)
- Hepatomegaly (2-3x normal)
- Hypersplenism → cytopenias
- May cause abdominal discomfort
- Growth retardation
- Delayed puberty
- Pulmonary involvement (rare)
- Increased malignancy risk (myeloma, lymphoma)
Pre-operative assessment for Gaucher patients:
- Platelet count and function (may need transfusion)
- Coagulation studies
- Liaise with hematology
- Increased bleeding risk at surgery
- Delayed bone healing
- Higher infection risk
Management

Enzyme Replacement Therapy
Recombinant glucocerebrosidase administered IV
- Imiglucerase (Cerezyme) - first ERT
- Velaglucerase alfa (VPRIV)
- Taliglucerase alfa (Elelyso) - plant-derived
- 30-60 units/kg every 2 weeks (IV infusion)
- Lifelong treatment
- Higher doses for severe bone disease
- Reduces hepatosplenomegaly within months
- Improves hematological parameters
- Prevents new bone disease
- Limited effect on established AVN
- Does NOT cross blood-brain barrier (no effect on neurological Type 2/3)
- Regular MRI for bone marrow burden
- CBC, liver function
- Biomarkers (chitotriosidase)
ERT remains the gold standard for moderate-severe disease.
ERT does NOT:
- Cross the blood-brain barrier (no neurological benefit)
- Reverse established AVN
- Completely prevent bone complications in all patients
- Replace need for surgical management when indicated
Surgical Management
-
Early AVN (Pre-collapse):
- Core decompression
- Limited evidence in Gaucher-related AVN
- May slow progression
- Coordinate with hematology
-
Advanced AVN (Collapse/Arthritis):
- Total hip arthroplasty
- Total shoulder arthroplasty
- Higher complication rate than primary OA
- Increased bleeding risk
- Platelet transfusion may be needed (target greater than 50,000)
- Cement may be preferable (poor bone quality)
- Extended prophylaxis (increased VTE risk)
- Consider tranexamic acid
- Liaise with hematology pre-operatively
- Surgical fixation when indicated
- Delayed healing expected
- May require bone grafting
- Internal fixation may be challenging (soft bone)
- Rarely needed with ERT
- May worsen bone disease (increased bone marrow infiltration)
- Only for massive, symptomatic splenomegaly
- Partial splenectomy preferred
Complications
- Progressive AVN requiring arthroplasty
- Chronic bone pain
- Multiple pathological fractures
- Vertebral collapse
- Growth retardation
- Severe anemia requiring transfusion
- Bleeding complications
- Hypersplenism
- Pulmonary hypertension
- Increased malignancy risk (myeloma, lymphoma)
- Parkinsonism (associated with GBA mutations, including heterozygotes)
- Increased bleeding (platelet and coagulation defects) → pre-operative hematology consultation, platelet transfusion if needed, meticulous hemostasis, consider tranexamic acid
- Delayed bone healing → protected weight bearing, longer follow-up
- Higher infection risk → standard prophylaxis, vigilance
- Implant loosening (poor bone quality) → consider cement fixation
- Prolonged recovery → optimise ERT dosing perioperatively
Outcomes and Prognosis
- Life expectancy near-normal for Type 1
- Dramatic reduction in splenectomy rates
- Prevention of new bone complications
- Quality of life greatly improved
- Established AVN often progresses despite ERT
- New bone crises reduced on ERT
- Bone density improves slowly
- Pathological fractures less common with treatment
- Good functional results
- Higher complication rate than primary OA
- May need earlier revision
- Coordinate perioperative care with hematology
Guidelines, Registries & Global Practice
Global Epidemiology:
- Pan-ethnic but markedly enriched in Ashkenazi Jewish populations (carrier frequency around 1:15; affected approximately 1:800)
- General population prevalence approximately 1:40,000 to 1:60,000
- The international ICGG Gaucher Registry remains the largest natural-history dataset; many countries maintain national registries to monitor long-term treatment outcomes
Side-by-Side Guidance:
- Emphasis
- Achievable treatment goals; structured monitoring; avoid splenectomy; semi-quantitative bone MRI
- Emphasis
- Diagnostic confirmation by enzyme assay plus genotyping; lifelong specialist follow-up
- Emphasis
- Newborn and high-risk screening; SRT (eliglustat) as oral first-line option in eligible type 1 adults
- Imiglucerase, velaglucerase alfa, and taliglucerase alfa (ERT) and eliglustat / miglustat (SRT) are high-cost orphan drugs; most health systems restrict access to confirmed disease prescribed through specialist metabolic services
- High-resource settings: ready access to ERT/SRT, MRI monitoring, and multidisciplinary metabolic-orthopaedic-haematology teams
- Limited-resource settings: diagnosis may be delayed; ERT access constrained by cost; greater reliance on supportive care, with higher rates of advanced AVN and splenectomy
- Patients requiring joint replacement, fracture fixation, or spinal surgery must be co-managed with haematology and metabolic medicine, with perioperative platelet and bleeding-risk optimisation
MCQ Practice Points
Q: What enzyme is deficient in Gaucher disease and what accumulates?
A: Glucocerebrosidase (beta-glucosidase) deficiency leads to accumulation of glucocerebroside in macrophages. These lipid-laden macrophages are called Gaucher cells and accumulate in bone marrow, spleen, and liver. GBA gene mutation on chromosome 1 causes the deficiency.
Q: What is the Erlenmeyer flask deformity and what causes it?
A: Failure of distal femoral metaphyseal remodeling due to Gaucher cell infiltration of the marrow, resulting in a flask-shaped appearance. The normal metaphyseal flaring persists because marrow expansion prevents normal cortical remodeling during growth. Also seen in distal tibia.
Q: The Erlenmeyer flask deformity is NOT specific to Gaucher. What else causes it?
A: A classic radiology viva list - remember "LEGS-NOP": Lead (heavy-metal) poisoning, Erlenmeyer in haemoglobinopathies (thalassaemia, sickle cell), Gaucher disease, Spondyloepiphyseal/other storage disorders; plus Niemann-Pick, Osteopetrosis, and Pyle disease / craniometaphyseal dysplasia (the inherited metaphyseal dysplasias). In an exam, name Gaucher first but show you know the deformity reflects any process that blocks normal metaphyseal "tubulation".
Q: A patient with Gaucher disease presents with severe bone pain, fever, and elevated inflammatory markers. Blood cultures are negative. What is the diagnosis?
A: Bone crisis - severe pain episode mimicking osteomyelitis but cultures are NEGATIVE. Caused by bone infarction from marrow infiltration with Gaucher cells. Treatment is supportive (analgesia, hydration), NOT antibiotics. ERT reduces frequency of crises.
Q: What is the inheritance pattern of Gaucher disease and which population has highest prevalence?
A: Autosomal recessive inheritance. Highest prevalence in Ashkenazi Jewish population (1:800 carrier frequency, 1:40,000 affected). Type 1 (non-neuronopathic) is most common and has best prognosis with ERT. Types 2 and 3 have neuronopathic features.
Self-Assessment Quiz
At a Glance
Gaucher disease is an autosomal recessive lysosomal storage disorder caused by glucocerebrosidase deficiency, leading to glucocerebroside accumulation in macrophages (Gaucher cells with "crinkled tissue paper" cytoplasm). Type 1 (non-neuronopathic) accounts for 95% of cases and is most common in Ashkenazi Jewish populations (1:800 prevalence). Key orthopaedic manifestations include bone crises (severe pain and fever mimicking osteomyelitis but culture-negative—do NOT treat with antibiotics), AVN of the hip and shoulder, pathological fractures, and Erlenmeyer flask deformity (failure of distal femur metaphyseal remodeling). Enzyme replacement therapy (ERT) with imiglucerase has transformed outcomes and is first-line treatment.
GAUCHERGaucher Features - GAUCHER
Hook:GAUCHER: Glucocerebrosidase, AVN, Unusual cells, Crises, Hepatosplenomegaly, Erlenmeyer, Recessive
BLEEDSurgical Precautions - BLEED
Hook:BLEED: Bleeding, Liaise, ERT, Expect delayed healing, DVT prophylaxis
123Gaucher Types - 1-2-3
Hook:1 = No neuro (good), 2 = Die by 2 (bad), 3 = Chronic neuro (variable)
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old man with known Gaucher Type 1 on ERT presents to ED with severe right thigh pain, fever, and inability to weight bear. X-ray shows Erlenmeyer flask deformity. His GP has started IV antibiotics for presumed osteomyelitis. What is your assessment?”
“A 35-year-old woman with Type 1 Gaucher disease presents with bilateral hip pain worse on the left. MRI shows Ficat Stage 4 AVN of the left femoral head and Stage 2 on the right. She is on ERT. How would you manage her?”
“A 45-year-old man with Type 1 Gaucher disease on ERT falls and sustains a distal femur fracture. X-ray shows Erlenmeyer flask deformity and an AO 33-A2 fracture. Describe your management.”
GENETICS
- GBA gene (chromosome 1)
- Glucocerebrosidase deficiency
- Autosomal recessive
- 1:800 Ashkenazi Jews
- Gaucher cells = lipid-laden macrophages
TYPES
- Type 1: Non-neuro, 95%, good prognosis
- Type 2: Acute neuro, infantile death
- Type 3: Chronic neuro, variable
BONE MANIFESTATIONS
- Erlenmeyer flask deformity
- Bone crises (mimic osteomyelitis)
- AVN (hip 40%)
- Pathological fractures
- Osteopenia
BONE CRISIS
- NOT infection
- Culture negative
- Analgesia, hydration, steroids
- Do NOT give antibiotics unless proven
TREATMENT
- ERT: Imiglucerase, velaglucerase
- SRT: Eliglustat (oral)
- Does NOT cross BBB
- Cannot reverse established AVN
SURGICAL PRECAUTIONS
- Bleeding risk - check platelets
- Liaise with hematology
- Delayed bone healing
- Cement fixation for arthroplasty
- Extended VTE prophylaxis
Evidence Base
- Largest cohort: 1698 patients across 38 countries before ERT
- 94% type 1, fewer than 1% type 2, 5% type 3; N370S (53%) and L444P (18%) most common alleles
- Bone pain in 63% and radiological bone disease in 94% of patients
- Bone disease more likely in asplenic patients
- Authoritative review of phenotype, diagnosis, and treatment
- ERT inhibits or reverses visceral and hematological disease
- Bone disease may progress despite treatment
- Substrate reduction and chaperone strategies emerging
- 1028 type 1 patients followed 2 to 5 years on ERT
- Hemoglobin normalised within 6 to 12 months; organomegaly markedly reduced
- Of patients with prior bone pain, 52% became pain-free at 2 years
- 94% of those with prior bone crises reported no further crises
- Phase 3 RCT of oral eliglustat vs placebo in treatment-naive type 1 patients
- Spleen volume fell 27.8% vs placebo (absolute difference -30%, P less than .001)
- Hemoglobin rose 1.22 g/dL and platelet count rose 41% vs placebo
- No serious adverse events; established oral substrate reduction therapy
- Consensus treatment goals and monitoring guidelines
- Recommended semi-quantitative MRI assessment of marrow infiltration
- Guidance on splenectomy, bisphosphonates, biomarkers, and pregnancy
- Splenectomy should be avoided where possible (worsens bone disease)
- 48 Gaucher patients with 54 hip implants for osteonecrosis-related arthrosis
- 15-year implant survival 60%; mean implant life 12.8 years
- Cementless ceramic-on-ceramic bearings outperformed other constructs
- Cement use and genotype did not affect longevity