Angular Knee Deformities | Physiological vs Pathological | Blount Disease | Guided Growth
- Physiological evolution: Birth varus (10-15°) → neutral (18-24mo) → peak valgus (3-4yrs, 10-15°) → adult alignment (7yrs, 5-7° valgus)
- Red flags for pathology: Asymmetry, rapid progression, extreme angle, short stature, onset after walking established
- Blount disease: Tibia vara from disrupted medial proximal tibial physis. Infantile (1-3yrs) vs adolescent types
- Rickets: Systemic cause of angular deformity - nutritional or renal. Bilateral, symmetric, physeal widening
- Guided growth: Hemiepiphysiodesis with 8-plates to correct angular deformity in skeletally immature patients
- “Measure intercondylar distance (varus) or intermalleolar distance (valgus) clinically
- “Mechanical axis deviation on standing long leg X-ray is the gold standard
- “Metaphyseal-diaphyseal (Drennan) angle greater than 16° suggests Blount disease (original cut-off was 11°)
- “Always check calcium, phosphate, vitamin D, ALP in bilateral deformity
Normal evolution: Babies born with 10-15° varus (bowlegs). Straightens by 18-24 months. Peaks at valgus 10-15° (knock-knees) by age 3-4. Gradually corrects to adult alignment (5-7° valgus) by age 7. Symmetric, follows expected pattern.
Suspect pathology if: Asymmetric deformity, rapid progression beyond expected pattern, extreme angles (varus greater than 15° after age 2, valgus greater than 15° after age 5), short stature, lateral thrust in gait, persisting/worsening after expected correction age.
Tibia vara from medial proximal tibial physis disorder. Infantile (1-3yrs, often bilateral) vs Adolescent (greater than 10yrs, unilateral, obese). Drennan MDA greater than 16° diagnostic. Infantile may respond to bracing; adolescent requires surgery.
Hemiepiphysiodesis with tension-band plating (8-plate). Applied to convex side of physis to retard growth and allow correction. Requires at least 2 years growth remaining. Correct approximately 1°/month. Remove hardware after correction achieved.
- Physiological Varus
- Less than 2 yrs, resolving
- Blount Disease
- Infantile: 1-3yrs, progressive
- Rickets
- Any age, often bilateral
- Physiological Varus
- Symmetric
- Blount Disease
- Often bilateral but may be asymmetric
- Rickets
- Symmetric
- Physiological Varus
- Normal physes
- Blount Disease
- Medial tibial beaking, MDA greater than 16°
- Rickets
- Physeal widening, cupping, fraying
- Physiological Varus
- None
- Blount Disease
- Lateral thrust, internal tibial torsion
- Rickets
- Short stature, rachitic rosary, bowing
- Physiological Varus
- Observation
- Blount Disease
- Brace (early) or surgery
- Rickets
- Vitamin D/phosphate, guided growth
ALIGNALIGN - Approach to Angular Deformity
Hook:ALIGN the approach - check age, look for thrust, investigate appropriately, and consider growth.
BLOUNTBLOUNT - Blount Disease Features
Hook:BLOUNT affects the proximal tibia physis, causing Beaking on X-ray and Lateral thrust.
RICKETSRICKETS - Features of Rickets
Hook:RICKETS is systemic - look for rosary, cupping, short stature, and treat the metabolic cause.
Overview and Epidemiology
Angular knee deformities are common presenting concerns in pediatric orthopaedics. Understanding the normal physiological development is essential to differentiate benign patterns from pathological conditions requiring intervention.
Definitions:
- Genu varum: "Bowlegs" - tibiofemoral angle in varus, knees apart when ankles together
- Genu valgum: "Knock-knees" - tibiofemoral angle in valgus, ankles apart when knees together
Birth to adult pattern: Newborns have 10-15° varus (intrauterine positioning). This straightens by 18-24 months to neutral. Maximum valgus (10-15°) occurs at age 3-4 years. Gradual correction to adult alignment (5-7° valgus) by age 6-7 years.
Epidemiology:
- Physiological angular deformity is extremely common and usually normal
- Infantile Blount disease: more common in African descent, early walkers, obese
- Rickets: nutritional form rare in developed countries; renal osteodystrophy in chronic kidney disease
Pathophysiology and Mechanisms
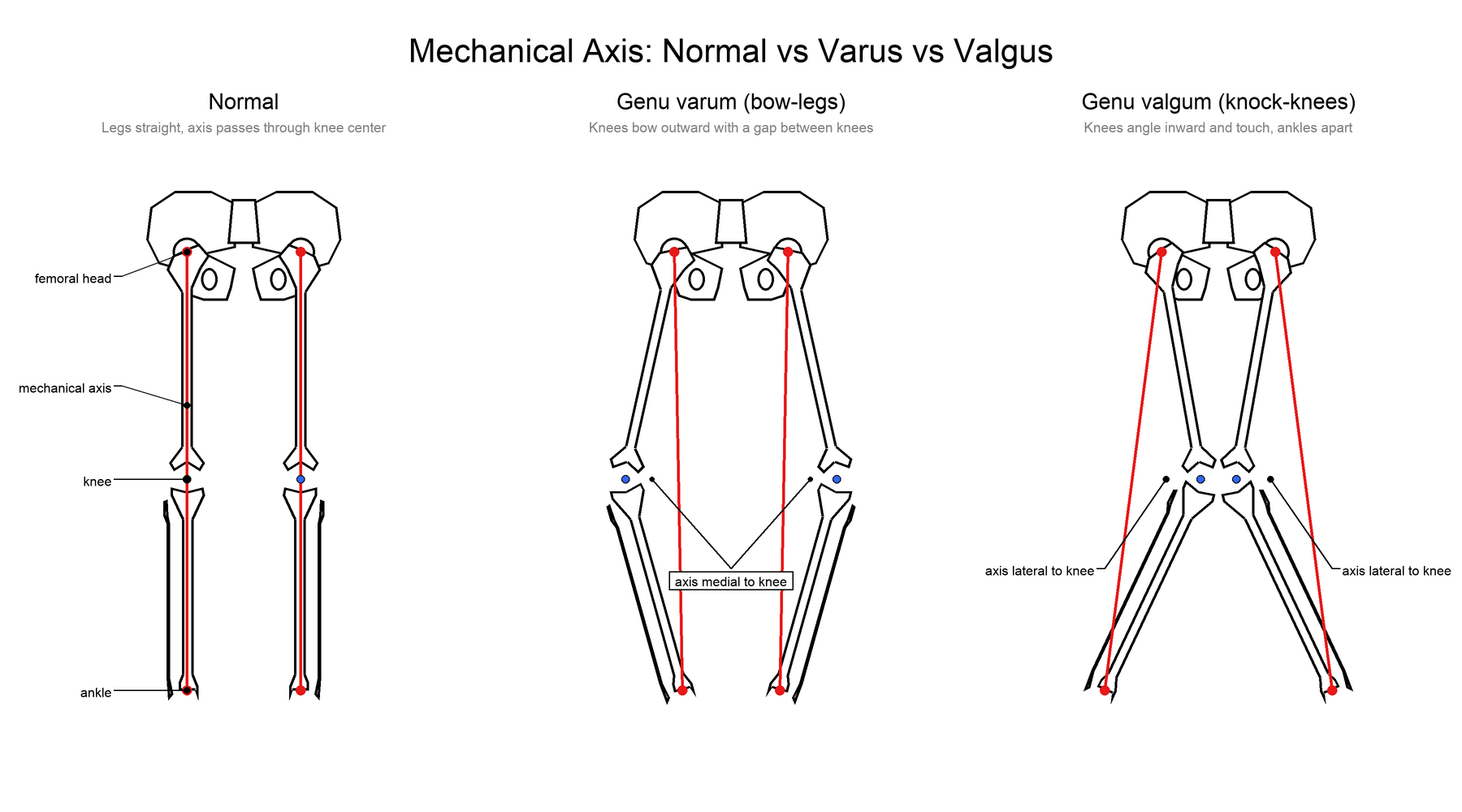
Lower Limb Mechanical Axis
- Definition
- Center of femoral head to center of ankle
- Normal Value
- Passes through or just medial to knee center
- Definition
- Femoral and tibial diaphyseal axes
- Normal Value
- 5-7° valgus tibiofemoral angle
- Definition
- Medial proximal tibial angle
- Normal Value
- 85-90°
- Definition
- Lateral distal femoral angle
- Normal Value
- 85-90°
Physeal Growth and Correction
- Proximal tibia: 55% of tibial growth
- Distal femur: 70% of femoral growth, 37% of leg length
- Asymmetric loading affects physeal growth
- Hueter-Volkmann law: compression retards, tension stimulates growth
- Hemiepiphysiodesis: Retard growth on one side
- 8-plate creates tension band effect
- Screw/staple methods also used
- Correct approximately 1°/month at distal femur
- Need at least 2 years growth remaining
Distal femur contributes more to angular correction than proximal tibia due to faster growth rate. Consider site of maximum deformity (CORA - center of rotation of angulation) when planning surgery. Overcorrection is a risk if hardware not removed promptly.
Classification Systems
Etiology-Based Classification
- Examples
- Normal developmental pattern
- Management Approach
- Observation, reassurance
- Examples
- Infantile tibia vara, adolescent tibia vara
- Management Approach
- Bracing (infantile), surgery
- Examples
- Rickets (nutritional, X-linked hypophosphatemic, renal)
- Management Approach
- Treat metabolic cause, then guided growth
- Examples
- Achondroplasia, multiple epiphyseal dysplasia
- Management Approach
- Manage deformity, often complex
- Examples
- Physeal injury, malunion
- Management Approach
- Depends on growth remaining
- Examples
- Post-septic physeal damage
- Management Approach
- May need surgical correction
Identifying the cause is essential for appropriate management.
The classic acquired cause of childhood genu valgum is the Cozen phenomenon: a proximal tibial metaphyseal fracture (often a minimally displaced greenstick injury in a child around 2-8 years) is followed weeks to months later by a progressive valgus deformity of that tibia. The mechanism is asymmetric medial overgrowth / physeal stimulation rather than malunion, so it occurs even after an anatomically reduced fracture. The crucial examinable point is the natural history: the valgus usually peaks at 12-18 months and then spontaneously remodels and largely corrects over several years - so management is observation and parental counselling, not acute osteotomy (early osteotomy tends to recur). Persistent severe deformity in an older child with little growth remaining is the exception that may need guided growth (medial hemiepiphysiodesis). Warn parents at the time of the original fracture that valgus may develop and is usually self-correcting.
Clinical Assessment
Systematic Examination
- Age of onset: When parents first noticed deformity
- Progression: Improving, stable, worsening
- Walking age: Early walkers at risk for Blount
- Family history: Skeletal dysplasia, rickets
- Diet/sun exposure: Vitamin D intake, risk for nutritional rickets
- Medical history: Renal disease, GI malabsorption
- Lateral thrust: Knee appears to "pop out" laterally in stance
- This is pathological and suggests significant varus
- In-toeing or out-toeing: May coexist with angular deformity
- Assess overall gait pattern and foot progression angle
- Intercondylar distance (ICD): Measure with ankles together (varus)
- Intermalleolar distance (IMD): Measure with knees together (valgus)
- Symmetry: Compare both sides
- Rotational profile: May coexist tibial internal torsion
- Height: Short stature suggests skeletal dysplasia or rickets
- Wrist exam: Physeal widening in rickets
- Rachitic rosary: Costochondral swelling
- Dysmorphic features: Skeletal dysplasia
A lateral thrust during gait is NEVER physiological. It indicates significant varus with medial collateral laxity or tibial vara. This finding warrants investigation and likely treatment.
Investigations
X-ray if: Asymmetric deformity, extreme angles, not following physiological pattern, lateral thrust, short stature, or clinical concern. Request standing AP long leg X-ray for accurate mechanical axis assessment.
- When Used
- Angular deformity requiring assessment
- What to Look For
- Mechanical axis deviation, site of deformity
- When Used
- Initial assessment, Blount diagnosis
- What to Look For
- Physeal changes, metaphyseal beaking, MDA
- When Used
- Suspected rickets
- What to Look For
- Physeal widening, cupping, fraying
- When Used
- Bilateral deformity, suspected metabolic cause
- What to Look For
- Low Ca/PO4/Vit D, high ALP in rickets
- When Used
- Physeal bar suspected, Blount assessment
- What to Look For
- Physeal status, bar extent
Key Radiographic Measurements:
- Mechanical axis deviation (MAD): Distance from mechanical axis to knee center
- Metaphyseal-diaphyseal angle (MDA): Described by Levine and Drennan (original threshold over 11°); the higher cut-off of over 16° popularised by Feldman and Schoenecker is the modern working value suggesting Blount disease, with an indeterminate grey zone between 9° and 16°
- Tibial metaphyseal angle: Assesses tibia vara severity
- Epiphyseal-metaphyseal angle (Gordon): Adjunct that may improve early discrimination of Blount disease from physiological bowing
Focal fibrocartilaginous dysplasia (FFCD) is an under-recognised cause of unilateral infantile tibia vara that mimics infantile Blount disease. It is caused by an abnormal focal fibrocartilaginous lesion at the insertion of the pes anserinus on the medial proximal tibial metaphysis, which tethers medial growth. The radiographic clue separates it from Blount: FFCD shows a sharply marginated, sclerotic cortical defect or radiolucency at the medial metaphyseal-diaphyseal junction (often an abrupt "step" or beak with focal angulation) rather than the medial physeal and epiphyseal beaking/depression of Blount, and the proximal tibial physis itself looks normal. The examinable point is the benign natural history: most FFCD spontaneously resolves with growth over 1-3 years, so management is usually observation, with corrective osteotomy reserved for the minority with progressive or non-resolving deformity. Consider it whenever an apparent unilateral "infantile Blount" has a focal metaphyseal lesion but a normal physis.
Management Algorithm
Conservative Management
- Most common presentation
- Follows expected pattern for age
- No lateral thrust, symmetric
- Reassurance and education
- Clinical follow-up every 6-12 months
- Serial clinical photos to document
- X-rays rarely needed if following typical pattern
- Expect correction by age 6-7 for valgus, earlier for varus
No bracing or orthotics required for true physiological deformity. They do not hasten correction.
Surgical Technique
Tension-Band Plating (8-Plate)
Standard guided growth technique for angular deformity.
Surgical Steps
- Standing long leg X-ray to assess mechanical axis
- Identify site(s) of deformity (CORA)
- Decide distal femur vs proximal tibia vs both
- Supine on radiolucent table
- Affected side accessible
- Image intensifier available
- Small (2-3cm) incision over physis
- On convex side of deformity
- For valgus: lateral distal femur
- For varus: medial proximal tibia
- Identify physis with fluoroscopy
- Extraperiosteal placement of 8-plate
- One screw in epiphysis, one in metaphysis
- Screws parallel, with plate on tension side
- Confirm position with imaging
- Close in layers
- No immobilization required
Technical Points:
- Screws must be parallel for tension-band effect
- Plate should sit flush on bone
- Do not violate physis with plate, only screws cross it
Post-operative: Weight-bear as tolerated; follow-up X-rays every 3 months.
Complications
- Incidence
- Common if hardware not removed
- Prevention/Management
- Regular monitoring, prompt removal
- Incidence
- Variable
- Prevention/Management
- Ensure adequate growth remaining
- Incidence
- Blount: significant if growth remaining
- Prevention/Management
- Address physeal bar, consider osteotomy
- Incidence
- Common (8-plate)
- Prevention/Management
- May need removal after correction
- Incidence
- Rare with 8-plate
- Prevention/Management
- Proper technique, avoid physeal damage
- Incidence
- Rare but serious
- Prevention/Management
- Prophylactic fasciotomy for large corrections
Overcorrection is common if 8-plates are not removed promptly. Follow patients closely (every 3 months) and remove hardware as soon as correction is achieved. Correcting past neutral is easy but creates opposite deformity.
Postoperative Care and Rehabilitation
Post-Guided Growth Protocol
- Wound care
- Weight-bearing as tolerated immediately
- No immobilization needed
- Discharge day 0-1
- Normal activities resume quickly
- First follow-up X-ray at 6-8 weeks
- Assess early correction
- Clinical and radiographic assessment
- Measure mechanical axis on long leg films
- Continue until correction achieved
- Once alignment normalized or slightly overcorrected
- Remove 8-plate as day surgery
- May rebound slightly after removal
- Post-removal X-ray at 3-6 months
Post-Osteotomy Rehabilitation:
- Protected weight-bearing for 6-8 weeks
- Knee ROM exercises
- Progress to full weight-bearing and activity
Outcomes
Near-universal spontaneous resolution; no intervention needed in the vast majority.
High success rate in appropriate candidates with predictable correction, low morbidity, and reversibility if overcorrection occurs.
Infantile disease has a better prognosis when treated early; adolescent disease shows higher recurrence and often needs osteotomy. Residual malalignment carries a long-term risk of medial compartment osteoarthritis.
Guidelines, Registries & Global Practice
Global Epidemiology:
- Physiological angular variation is near-universal in toddlers and is the single commonest reason for paediatric orthopaedic referral for "bent legs"; the vast majority require only reassurance.
- Infantile Blount disease shows a higher reported prevalence in populations of African ancestry, in early walkers, and with rising childhood obesity; late-onset (adolescent) Blount tracks closely with the global obesity epidemic.
- Nutritional rickets remains an important and preventable cause worldwide, concentrated in infants with darker skin, limited sun exposure, exclusive prolonged breastfeeding without supplementation, and low dietary calcium; X-linked hypophosphataemic rickets and renal osteodystrophy are the main non-nutritional metabolic causes.
Guidelines, Side by Side:
- Focus
- Nutritional rickets
- Key Position
- Defines diagnosis (biochemistry plus physeal change); universal infant vitamin D supplementation and food fortification to prevent and eradicate rickets
- Focus
- Angular deformity work-up
- Key Position
- Standing long-leg alignment film as the reference standard; guided growth favoured while physis is open
- Focus
- Referral and observation
- Key Position
- Reassure and observe physiological patterns; refer red-flag features (asymmetry, lateral thrust, short stature, extreme angle)
- Focus
- Vitamin D prophylaxis
- Key Position
- Routine infant vitamin D supplementation to prevent rickets-related deformity
There is broad international agreement on the principles (observe physiological deformity, screen for metabolic causes in bilateral deformity, prefer guided growth while the physis is open) and no major society-level disagreement on the core algorithm — the genuine debates are technical (thresholds, timing) rather than national.
- There is no dedicated paediatric angular-deformity arthroplasty registry; evidence is from institutional series and multicentre study groups rather than national joint registries.
- Long-term registry-style follow-up matters because residual malalignment is a recognised risk factor for early medial compartment osteoarthritis, linking childhood correction to adult arthroplasty burden captured in national joint registries.
- Well-resourced settings: standing long-leg radiographs, MRI for physeal-bar assessment, tension-band plating and computer-assisted/hexapod external fixators are routinely available.
- Limited-resource settings: the priority shifts to public-health prevention of nutritional rickets (supplementation, fortification), clinical screening without long-leg films, and definitive osteotomy where staged guided growth or repeat hardware procedures are impractical.
- Parental concern is often driven by cultural norms about leg shape; clear reassurance about the physiological arc prevents unnecessary imaging and intervention everywhere.
Controversies and Areas of Uncertainty
Angular knee deformity is a high-volume but evidence-thin area: most data are retrospective single-centre series, and several practical questions remain genuinely unsettled. Examiners reward a candidate who can state what is established versus what is debated.
The original Drennan threshold (over 11°) over-calls Blount disease; the over 16° cut-off improves specificity but leaves a 9–16° grey zone where physiological bowing and early Blount overlap. Serial measurement and adjunct angles (e.g. Gordon epiphyseal-metaphyseal angle) are more reliable than any single number.
Reported bracing success in early infantile tibia vara is confounded by the fact that many young, low-stage cases would resolve spontaneously. There is no randomised evidence; brace type, dose and the true threshold for abandoning bracing remain debated.
Guided growth is attractive but has a higher failure and recurrence rate in advanced Blount disease (Langenskiöld IV+) and obese adolescents, where many surgeons favour acute or gradual osteotomy. The optimal crossover point is not defined by high-level evidence.
Rebound after plate removal is common (over 40% of segments in long-term series). Whether to deliberately overcorrect, when to remove hardware, and whether to leave the plate in situ in younger children are all unresolved trade-offs against iatrogenic deformity.
State the principle, acknowledge the uncertainty, then commit to a defensible plan: "The evidence base is largely retrospective. I would use the MDA alongside serial clinical assessment rather than a single cut-off, reserve osteotomy for advanced or adolescent Blount disease, and counsel families that rebound is common and follow-up to maturity is mandatory."
MCQ Practice Points
Q: At what age is peak physiological genu valgum expected? A: Age 3-4 years, with approximately 10-15° valgus. This corrects to adult alignment (5-7° valgus) by age 7.
Q: What metaphyseal-diaphyseal (Drennan) angle suggests Blount disease? A: The original Drennan threshold was over 11°; the modern working value (Feldman and Schoenecker) of over 16° is more specific, with a 9–16° grey zone overlapping physiological bowing.
Q: Where is an 8-plate placed for genu valgum and what is its correction rate? A: On the medial side of the distal femur (convex side) to retard medial growth; expect roughly 1° per month, slightly slower at the proximal tibia.
Medicolegal Considerations
- Age, height, and clinical measurements (ICD/IMD)
- Gait assessment including lateral thrust
- Family history and dietary assessment
- Radiographic findings and measurements
- Need for hardware removal after correction
- Risk of overcorrection or undercorrection
- May need additional surgery (recurrence, other side)
- Osteotomy risks: compartment syndrome, nerve injury
Missing follow-up after 8-plate insertion can lead to overcorrection. Emphasize the importance of regular monitoring and document the follow-up plan clearly.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A mother brings her 18-month-old child concerned about 'bowlegs'. The child started walking at 11 months and the mother feels the legs are bowed.”
“A 2.5-year-old child presents with progressive bowlegs. They have been walking since 10 months. On examination, there is a noticeable lateral thrust during gait, and the varus appears worse on the right side.”
“A 9-year-old child presents with bilateral knock-knees that have been present for several years. The parents are concerned it is getting worse. The child is otherwise well and of normal height.”
Physiological Pattern
- Birth: 10-15° varus (bowlegs)
- 18-24 months: Neutral
- 3-4 years: Peak valgus (10-15°)
- 7 years: Adult alignment (5-7° valgus)
Red Flags for Pathology
- Lateral thrust during gait
- Asymmetry between sides
- Extreme angle beyond expected
- Short stature or systemic features
Blount Disease
- Tibia vara from medial proximal tibial physis
- Infantile (1-3yrs) vs Adolescent (greater than 10yrs)
- MDA greater than 16° diagnostic
- Langenskiöld staging determines treatment
Guided Growth (8-Plate)
- On convex side of deformity
- Valgus: medial distal femur
- Varus: lateral proximal tibia
- Correct approximately 1°/month
- Remove promptly after correction
Key Numbers
- MDA greater than 16° = Blount disease
- 5-7° = Normal adult tibiofemoral angle
- 1°/month = 8-plate correction rate
- At least 2 years growth needed for guided growth
Evidence Base
Salenius & Vankka — Natural History of the Tibiofemoral Angle
- Defined the developmental arc of the tibiofemoral angle from birth to maturity
- Maximal physiological varus in infancy, transitioning to peak valgus at approximately 3 years
- Spontaneous correction toward the adult value of mild valgus by around 7 years
- Wide spread of normal values reinforces that single measurements should be interpreted with age
Levine & Drennan — Metaphyseal-Diaphyseal Angle
- Introduced the metaphyseal-diaphyseal (Drennan) angle to quantify proximal tibial bowing
- 29 of 30 limbs with an angle over 11 degrees later developed radiographic tibia vara
- Only 3 of 58 limbs with an angle of 11 degrees or less progressed
- Approximately 60% of deformity in tibia vara arises in the proximal metaphysis versus around 20% in physiological bowing
Feldman & Schoenecker — Refining the MDA Threshold
- Mean MDA was 9 degrees in physiological bowing versus 19 degrees in Blount disease (p less than 0.0000001)
- An angle between 9 and 16 degrees carried over 5% risk of false-positive and false-negative classification
- 37% of physiological limbs exceeded 11 degrees, exposing the limitation of the original cut-off
- A threshold of 16 degrees better separates Blount disease from physiological bowing