Subtle Diagnosis | Myerson Classification | ORIF vs Primary Arthrodesis
- Fleck sign = avulsion of Lisfranc ligament from base of 2nd MT (pathognomonic)
- No bony columns align normally on AP, oblique, and lateral views
- 2mm diastasis between 1st and 2nd MT bases = absolute surgical indication
- Primary arthrodesis superior to ORIF for purely ligamentous injuries
- Weight-bearing CT gold standard for subtle injuries in high-suspicion cases
- “Piano key test: pain with dorsoplantar force on metatarsal heads
- “ALWAYS check medial column alignment on lateral X-ray (1st TMT joint)
- “Purely ligamentous injuries have worse outcomes than fracture-dislocations
- “Primary arthrodesis of medial 3 TMTs shown superior to ORIF in RCTs

20% are missed initially. High index of suspicion for midfoot pain after trauma. Fleck sign on AP X-ray (avulsion of Lisfranc ligament from 2nd MT base) is pathognomonic. Weight-bearing views mandatory if stable; weight-bearing CT if high suspicion but normal X-rays.
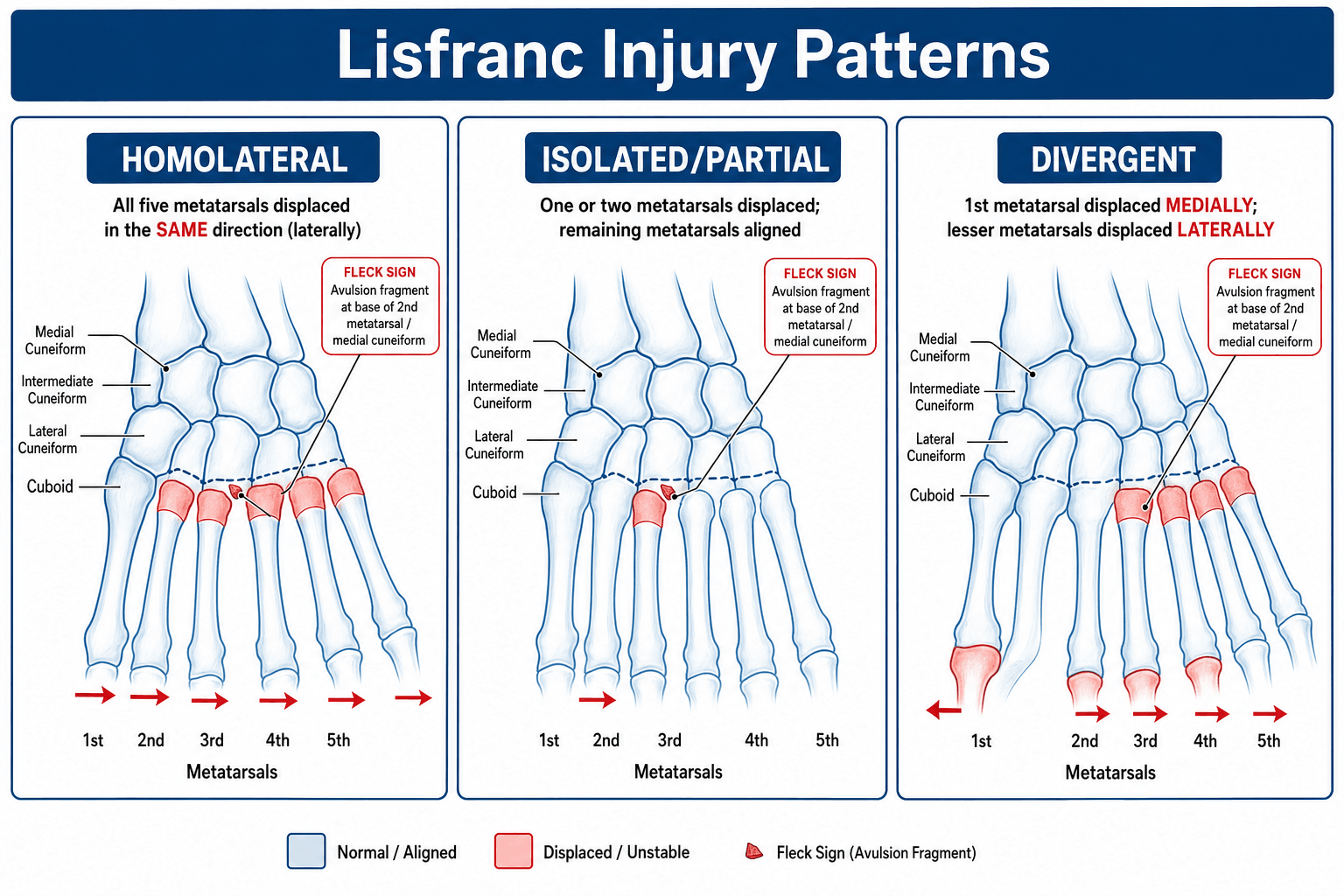
Type A = total incongruity (all 5 TMTs). Type B = partial (B1 medial, B2 lateral). Type C = divergent (1st ray medial, 2-5 lateral). Classification guides fixation: screw medial column, K-wire lateral.
Purely ligamentous injuries do poorly with ORIF alone. Primary arthrodesis of medial 3 TMTs (1st, 2nd, 3rd) shown superior in RCTs. ORIF acceptable for fracture-dislocations with good bone reduction. Preserve mobility of 4th-5th TMTs.
Medial column (1st-2nd-3rd TMTs) = rigid, screw fixation or fuse. Lateral column (4th-5th TMTs) = mobile, temporary K-wires. Anatomic reduction critical - even 2mm residual diastasis leads to arthritis. Remove hardware at 4-6 months if ORIF.
- Myerson Type
- Suspected ligamentous
- Treatment
- Weight-bearing X-rays or CT
- Key Pearl
- Greater than 2mm diastasis on WB views = surgery
- Myerson Type
- Type A or B
- Treatment
- Primary arthrodesis 1st-3rd TMTs
- Key Pearl
- ORIF alone has 50% poor outcomes
- Myerson Type
- Type A, B, or C
- Treatment
- ORIF with screws medial, K-wires lateral
- Key Pearl
- Anatomic reduction critical, hardware removal at 4-6 months
- Myerson Type
- Type B2 or C
- Treatment
- Bridge plating or external fixation
- Key Pearl
- Stage to primary arthrodesis once soft tissues heal
Overview and Epidemiology

Lisfranc injuries are easily missed (20% on initial presentation) but devastatingly disabling if untreated. The tarsometatarsal (TMT) joint complex is critical for foot stability and push-off power. Even subtle ligamentous injuries lead to progressive deformity and post-traumatic arthritis in over 90% if not recognized and treated. High index of suspicion is essential for midfoot pain after trauma.
- Fall with foot plantar-flexed and twisted
- Motor vehicle accident (foot on brake pedal)
- Sporting injuries (football, basketball)
- Peak age 30-40 years
- Motor vehicle collisions
- Fall from height
- Industrial crush injuries
- Associated with other foot/ankle fractures (39%)
- Progressive midfoot collapse (90%)
- Post-traumatic arthritis (90%)
- Chronic pain and disability
- Loss of push-off power
- Secondary forefoot deformities
- Worse outcomes than acute treatment
- Often requires salvage arthrodesis
Anatomy and Biomechanics
The Lisfranc ligament (oblique ligament) is the strongest ligament in the TMT complex, running from the lateral plantar aspect of the medial cuneiform to the medial base of the 2nd metatarsal. It consists of three bundles: dorsal (weakest), interosseous (strongest), and plantar (second strongest). The 2nd MT base is recessed 2-3mm proximally, creating a "Roman arch" configuration. There is NO ligamentous connection between the 1st and 2nd metatarsal bases - the Lisfranc ligament is the sole stabilizer.


- TMT Joints
- 1st-2nd-3rd TMTs
- Mobility
- Minimal (2-3°)
- Fixation Strategy
- Screw fixation or primary arthrodesis
- TMT Joints
- 4th-5th TMTs
- Mobility
- Significant (10-15°)
- Fixation Strategy
- Temporary K-wires only (preserve motion)
- Medial 1st MT = medial 1st cuneiform
- Medial 2nd MT = medial 2nd cuneiform
- Medial 4th MT = medial cuboid
- Medial 3rd MT = medial 3rd cuneiform
- Lateral 4th MT = lateral cuboid
- Dorsal 1st MT = dorsal 1st cuneiform (often missed!)
- Medial column: rigid lever for push-off
- Lateral column: flexible adaptation to terrain
- Transverse arch maintained by Lisfranc complex
- Loss of transverse arch (progressive collapse)
- Medial column instability (loss of push-off)
- Forefoot abduction deformity
CLIMBLisfranc Ligament Anatomy
Hook:CLIMB the Roman arch - the 2nd MT is recessed like a keystone, held by the strongest Lisfranc ligament from medial cuneiform!
Pathophysiology and Injury Mechanism
Lisfranc injuries occur via two primary mechanisms: direct (crush injury) and indirect (rotational/axial loading). The indirect mechanism is more common and involves hyperplantar flexion with axial load, causing the Lisfranc ligament to fail. Understanding the mechanism helps predict associated injuries and guides treatment.
Mechanism of Injury
- Industrial crush injury
- Heavy object dropped on midfoot
- Motor vehicle collision with direct impact
- Results in significant soft tissue damage
- Higher rate of open injuries and compartment syndrome
- Axial load on plantarflexed foot (e.g., driver's foot on brake during collision)
- Rotational force with foot fixed to ground (sporting injuries)
- Fall from height onto plantarflexed foot
- Hyperabduction or hyperadduction with fixed forefoot
Sequence of Ligamentous Failure
Sequential Failure of Stabilizers
The dorsal TMT ligaments are weakest and fail first under dorsiflexion-abduction stress.
The interosseous portion of the Lisfranc ligament (strongest component) fails next, allowing dorsal-lateral displacement of the metatarsals.
Complete failure of plantar ligaments allows full TMT dislocation. Associated fractures may occur (2nd MT base avulsion, cuneiform fractures).
Why Injuries Progress Without Treatment
- Loss of the "Roman arch" configuration
- Progressive diastasis between 1st and 2nd metatarsals
- Medial column instability → loss of push-off power
- Lateral column adaptive changes → forefoot abduction
- Transverse arch collapse → midfoot arthritis
- Greater than 2mm diastasis between 1st and 2nd MT bases indicates ligamentous incompetence
- Even minimal displacement leads to increased joint contact pressures
- Articular cartilage degeneration begins within weeks
- 90%+ develop post-traumatic arthritis if untreated
The Lisfranc ligament is the sole connection between the 1st and 2nd metatarsal bases - there is NO direct ligament between them. When the Lisfranc ligament fails, the medial column can separate from the middle column, causing progressive deformity and instability.
FLECKRadiographic Signs of Lisfranc Injury
Hook:FLECK sign is the key - if you see the tiny avulsion fracture from the 2nd MT base, you've found your Lisfranc injury!
Classification Systems
Myerson Classification (Most Used)
Based on direction and pattern of displacement at TMT joints. Guides treatment strategy.
- Pattern
- All 5 TMTs displaced same direction
- Key Features
- Lateral or dorsomedial (most common)
- Treatment Approach
- ORIF all columns
- Pattern
- 1st-2nd TMTs involved
- Key Features
- Medial column instability
- Treatment Approach
- ORIF medial, assess lateral
- Pattern
- 3rd-4th-5th TMTs involved
- Key Features
- Lateral column injury
- Treatment Approach
- ORIF or K-wire lateral column
- Pattern
- 1st ray medial, 2-5 lateral
- Key Features
- High energy, worst outcomes
- Treatment Approach
- ORIF both columns, consider staging
Myerson added subtypes: A1/B1/C1 = total incongruity, A2/B2/C2 = partial incongruity. However, most surgeons use the simpler A/B1/B2/C system. Type C (divergent) has the highest energy, most soft tissue damage, and worst prognosis.
ABCMyerson Classification of Lisfranc Injuries
Hook:ABC = All together, Broken in parts, Completely divergent - remember B has two subtypes (B1 medial, B2 lateral)!
Nunley-Vertullo Classification (Athletic Midfoot Sprains)
The Myerson and Quenu-Kuss systems describe the high-energy fracture-dislocation. They do not capture the subtle, low-energy athletic midfoot (Lisfranc) sprain, which spans a spectrum from a stable ligament sprain to frank diastasis and needs its own staging because treatment differs. Nunley and Vertullo (2002) staged these injuries using weight-bearing radiographs (the original description also used bone scintigraphy to detect the radiographically occult sprain), and reported excellent results in 93% of athletes managed by this scheme.
- Diastasis (1st-2nd ray)
- None (positive bone scan or MRI, normal radiographic alignment)
- Arch height (lateral view)
- Preserved
- Treatment
- Non-operative: non-weight-bearing cast, then progressive return to activity
- Diastasis (1st-2nd ray)
- Diastasis present (approximately 1 to 5 mm)
- Arch height (lateral view)
- Preserved (no flattening)
- Treatment
- Anatomic reduction and internal fixation
- Diastasis (1st-2nd ray)
- Diastasis present
- Arch height (lateral view)
- LOST (arch flattening on the lateral view)
- Treatment
- Anatomic reduction and internal fixation
The Myerson system describes the high-energy fracture-dislocation, but the subtle low-energy athletic midfoot sprain has its own staging (Nunley and Vertullo). Stage I is a sprain with no diastasis and a normal arch - the radiographs look aligned and the diagnosis rests on a positive bone scan or MRI - and is treated non-operatively. Stage II has 1st-2nd ray diastasis with a preserved arch; Stage III has diastasis WITH loss of arch height on the lateral view. The operative line falls between Stage I and Stage II: ANY diastasis (II or III) needs anatomic reduction and fixation, whereas a true Stage I is managed in a non-weight-bearing cast with a graded return. Weight-bearing radiographs are the key diagnostic step.
Clinical Assessment
- Low-energy: Fall on plantar-flexed foot, twisting injury
- High-energy: MVA with foot on brake, crush, fall from height
- Unable to weight-bear immediately after injury
- Midfoot pain and swelling (dorsal and plantar)
- Unable to push off or walk normally
- Pain worse with weight-bearing
- "Just a sprain" - most common misdiagnosis
- Delayed presentation (days to weeks) with persistent pain
- Midfoot ecchymosis (dorsal and plantar - highly specific)
- Diffuse swelling over TMT joints
- Forefoot abduction deformity (if severe)
- Point tenderness over TMT joints (especially 1st-2nd)
- Palpable step-off or gap
- Piano key test: pain with dorsoplantar force on MT heads
- Passive abduction stress painful
- Unable to single-leg heel rise
Up to 20% of Lisfranc injuries are missed on initial presentation. High index of suspicion required for:
- Midfoot pain after twisting injury, even if X-rays appear "normal"
- Unable to weight-bear or push off despite "normal" static X-rays
- Plantar ecchymosis (pathognomonic - always suspect Lisfranc)
If high suspicion but normal static X-rays: obtain weight-bearing views (patient stands on injured foot). If still normal but high suspicion, proceed to weight-bearing CT (gold standard for subtle injuries).
- Distinguishing Features
- Plantar ecchymosis, pain on piano-key / abduction stress, fleck sign, 1st-2nd MT diastasis
- Key Investigation
- Weight-bearing radiographs; weight-bearing CT if normal
- Distinguishing Features
- Tenderness without diastasis or malalignment, able to weight-bear, stable on stress
- Key Investigation
- Weight-bearing radiographs normal; consider Nunley-Vertullo stage I
- Distinguishing Features
- Focal tenderness over a single MT base, no TMT diastasis or incongruity
- Key Investigation
- Plain radiographs; CT if intra-articular
- Distinguishing Features
- Tenderness more proximal/medial, midfoot bony tenderness
- Key Investigation
- Plain radiographs; CT for occult fracture
- Distinguishing Features
- Swollen, warm, often painless insensate foot; may lack clear trauma history
- Key Investigation
- Radiographs (fragmentation/collapse), inflammatory markers, MRI
Investigations
Imaging Protocol for Suspected Lisfranc Injury
- AP: Check medial column alignment (1st MT to 1st cuneiform, 2nd MT to 2nd cuneiform)
- Oblique: Check 3rd MT to 3rd cuneiform, 4th MT to cuboid
- Lateral: Check dorsal alignment (often forgotten but critical)
- Fleck sign (avulsion from 2nd MT base - pathognomonic)
- Diastasis greater than 2mm between 1st-2nd MT bases
- Step-off at any TMT joint
- Fractures of cuneiforms or MT bases

This imaging protocol provides comprehensive evaluation for Lisfranc injuries.
Sagittal CT imaging is valuable for assessing:
- Dorsal subluxation of metatarsal bases
- Soft tissue swelling patterns
- Associated cuneiform fractures

Sagittal plane assessment helps evaluate instability patterns.
Suspected Lisfranc but normal non-weight-bearing X-rays
- Patient stands on injured foot (bilateral comparison views)
- AP and lateral views most useful
- Diastasis greater than 2mm between 1st-2nd MT bases on AP
- Loss of medial column alignment on lateral (1st TMT joint)
- Greater than 2mm difference compared to contralateral side
Weight-bearing views are critical for detecting subtle instability.
- High clinical suspicion but normal weight-bearing X-rays
- Subtle ligamentous injuries
- Pre-operative planning for complex injuries
- Detects subtle diastasis (under 2mm)
- Identifies occult fractures
- 3D reconstruction for surgical planning
- Bilateral comparison possible
Sensitivity 94%, Specificity 99% for Lisfranc injuries
This advanced imaging modality is invaluable for challenging cases.
Less commonly used but can identify:
- Lisfranc ligament disruption directly
- Bone marrow edema pattern
- Soft tissue injuries
Limitations:
- Non-weight-bearing (may miss subtle instability)
- More expensive and time-consuming than CT
MRI can complement other imaging but is not typically first-line for Lisfranc injuries.

Management Algorithm

Conservative Management Criteria
Indications (RARE):
- No diastasis on weight-bearing X-rays (under 2mm)
- No loss of alignment on AP, oblique, lateral views
- Stable on clinical examination
- Low-energy mechanism
Protocol:
Non-Operative Treatment
- Non-weight-bearing in short leg cast or boot
- Strict compliance critical
- Weekly X-rays first 3 weeks to detect displacement
- Transition to weight-bearing in boot if X-rays stable
- Gradual progression over 6 weeks
- Continue weekly X-rays
- Wean from boot
- Physiotherapy for gait retraining
- Avoid high-impact until 4-6 months
Conservative management requires close monitoring and patient compliance.
Even "stable" Lisfranc injuries have high failure rates with non-operative treatment. Any displacement on follow-up X-rays mandates surgical intervention. Many surgeons advocate early surgical fixation even for minimally displaced injuries to prevent late collapse.
SAFETreatment Algorithm for Lisfranc Injuries
Hook:Keep it SAFE - Screws medially, Anatomic reduction, Flexible laterally, Early fusion for ligamentous!
Surgical Technique
Pre-operative Preparation
- Infection: 2-5% superficial, 1-2% deep
- Nerve injury: Superficial peroneal, deep peroneal (1-2%)
- Malunion/loss of reduction: 10-20% with ORIF
- Post-traumatic arthritis: 30-50% despite treatment
- Hardware removal: Required at 4-6 months if ORIF
- Need for revision/arthrodesis: 20% with ORIF
- Compartment syndrome: Rare but possible (high-energy)
Comprehensive consent ensures patient understanding of risks.
- Implants: 3.5mm or 4.0mm screws for medial column, 1.6mm K-wires for lateral
- Power: Drill, small fragment set
- Imaging: C-arm with AP, oblique, lateral capability
- Reduction aids: Pointed reduction clamps, bone hooks, K-wires
- Arthrodesis set: If planning primary fusion (curettes, reamers, bone graft)
- External fixator: If staged approach for high-energy injuries
Proper equipment preparation is essential for successful surgery.
Surgical Decision Tree:
- Purely ligamentous → Primary arthrodesis 1st-2nd-3rd TMTs
- Fracture-dislocation, acute → ORIF with screws medial, K-wires lateral
- High-energy, soft tissue compromise → Temporary K-wires or external fixation, stage to definitive fixation/arthrodesis at 7-14 days
- Chronic (greater than 6 weeks) → Primary arthrodesis 1st-2nd-3rd TMTs
This decision tree guides optimal surgical approach based on injury characteristics.



Choice of Fixation Construct
When ORIF is chosen, the construct matters. The traditional construct is the transarticular screw, but each screw crossing the tarsometatarsal joint violates articular cartilage and fatigues across the joint, so a dorsal bridge plate (extra-articular, cartilage-sparing) and a suture-button / flexible device (allowing physiological micromotion) are alternatives. No single construct is proven universally superior; selection follows the injury pattern, the degree of comminution, and the wish to avoid joint violation.
- How it works
- Rigid screws crossing the TMT joints (medial three columns)
- Advantages and trade-offs
- Strong, well-studied, the traditional default; but they damage articular cartilage and fatigue across the joint - planned removal at 4 to 6 months, risk of breakage
- How it works
- Plate spanning the joint with screws in the metatarsal and cuneiform (not crossing the joint)
- Advantages and trade-offs
- Extra-articular, so it spares cartilage; comparative data trend in its favour over transarticular screws (pooled AOFAS approximately 79 vs 74); useful with comminution or dorsal bone loss; usually still removed
- How it works
- Cortical button-and-suture across the medial cuneiform to the 2nd metatarsal base, giving dynamic stabilisation
- Advantages and trade-offs
- Allows physiological micromotion, no routine removal operation, spares cartilage; attractive for isolated ligamentous instability; limited comparative data and a risk of incomplete reduction
The traditional Lisfranc construct is the transarticular screw, but every transarticular screw damages tarsometatarsal articular cartilage and fatigues across the joint, so it must be removed at 4 to 6 months and can break. A dorsal bridge plate avoids crossing the joint (extra-articular and cartilage-sparing), and the comparative evidence trends in its favour over transarticular screws (Philpott meta-analysis: AOFAS approximately 79 vs 74, with a pooled effect favouring the plate). Suture-button (flexible) fixation allows physiological micromotion and avoids a removal operation, and is attractive for isolated ligamentous instability, although comparative data are limited. No single construct is proven universally superior - match it to the injury pattern and the wish to avoid joint violation.
Complications
- Incidence
- 30-50% overall
- Risk Factors
- Residual displacement, high-energy injury, cartilage damage
- Management
- Activity modification, orthotics, NSAIDs; salvage arthrodesis if severe
- Incidence
- 10-30%
- Risk Factors
- Purely ligamentous injury, inadequate fixation, early weight-bearing
- Management
- Revision ORIF or convert to primary arthrodesis
- Incidence
- 20-30%
- Risk Factors
- Screw heads not countersunk, thin soft tissue dorsum of foot
- Management
- Hardware removal at 4-6 months (planned)
- Incidence
- 5-10%
- Risk Factors
- High-energy injury, soft tissue damage, diabetes, smoking
- Management
- Wound care, antibiotics; may require debridement or flap
- Incidence
- 2-5%
- Risk Factors
- Iatrogenic during approach, traction injury
- Management
- Usually neuropraxia; observe, most recover in 3-6 months
- Incidence
- 5-10%
- Risk Factors
- Smoking, diabetes, inadequate fixation, bone loss
- Management
- Revision arthrodesis with bone graft and supplemental fixation
- Incidence
- Under 5%
- Risk Factors
- High-energy injury, crush mechanism
- Management
- Emergency fasciotomy (4 compartments of foot)
Even with perfect reduction and fixation, 30-50% of patients develop symptomatic post-traumatic arthritis at the TMT joints. High-energy injuries and cartilage damage at time of injury are major risk factors. Counsel patients that salvage arthrodesis may be needed in the future. Some surgeons advocate primary arthrodesis to eliminate this risk (especially for ligamentous injuries).
Postoperative Care and Rehabilitation

Rehabilitation After ORIF
- Non-weight-bearing in short leg splint
- Elevation above heart level (reduce swelling)
- DVT prophylaxis (aspirin or LMWH per protocol)
- Wound check at 2 weeks, transition to cast/boot
- Non-weight-bearing in short leg cast or boot
- Weekly X-rays first 3 weeks to detect loss of reduction
- Remove lateral column K-wires at 6 weeks (in clinic)
- Transition to weight-bearing in boot (10-20% per week)
- Continue in boot full-time
- Radiographs at 8, 12 weeks
- Start gentle ROM exercises at 8 weeks
- Wean from boot
- Supportive shoes with rigid sole
- Physiotherapy for gait retraining
- Custom orthotics if arch collapse
- Remove medial column screws at 4-6 months (mandatory to prevent hardware failure)
- Brief period non-weight-bearing (1-2 weeks) after hardware removal
- Return to full activity at 6 months
Structured rehabilitation optimizes functional recovery.
Screws crossing the TMT joints are subject to repetitive cyclical loading during gait. They WILL eventually break or loosen (30-50% by 1 year). Planned removal at 4-6 months after bony healing prevents this complication and allows the patient to transition to full activity without risk of hardware failure.
- Low-impact activities: 4-6 months
- High-impact sports: 6-9 months
- Return to competition: 9-12 months
- Severity of initial injury
- Type of surgery (ORIF vs arthrodesis)
- Sport demands
- Presence of arthritis
Many athletes never return to pre-injury level (30-40% in high-impact sports)
Realistic expectations are important for patient satisfaction.
- 2, 6, 12 weeks post-op (X-rays)
- 6, 12, 24 months (clinical and X-ray)
- Annual review if symptomatic
- Progressive arthritis
- Hardware failure (if ORIF)
- Midfoot collapse
- Transfer metatarsalgia
- Custom orthotics
- Rigid-sole shoes
Ongoing monitoring helps identify and address late complications.
Outcomes and Prognosis
- Patient Population
- Acute, good bone quality
- Outcomes
- 70-80% good/excellent, most return to activity
- Complications
- 20-30% loss of reduction, hardware removal required
- Patient Population
- No fractures, ligament only
- Outcomes
- 50% poor outcomes, high revision rate
- Complications
- 30% loss of reduction, 20% conversion to arthrodesis
- Patient Population
- No fractures, or chronic
- Outcomes
- 85% good/excellent, better than ORIF for this group
- Complications
- 5-10% nonunion, eliminates arthritis risk
- Patient Population
- Truly non-displaced, compliant
- Outcomes
- High failure rate, most end up needing surgery
- Complications
- Progressive deformity, arthritis
- High-energy mechanism: Worse outcomes than low-energy injuries
- Purely ligamentous injuries: 50% poor outcomes with ORIF (need primary arthrodesis)
- Delayed diagnosis: Greater than 6 weeks from injury significantly worsens prognosis
- Residual displacement: Even 2mm diastasis leads to progressive arthritis (90%)
- Associated injuries: Navicular or cuneiform fractures worsen overall outcome
- Smoking and diabetes: Increase risk of complications and poor healing
Guidelines, Registries & Global Practice
Lisfranc injuries are uncommon but high-morbidity, and are misdiagnosed in approximately 20% of cases on initial radiographs across health systems. They are caused by both high-energy (motor vehicle, fall from height, crush) and low-energy (athletic, twisting plantar-flexed foot) mechanisms, and should be considered in any patient with midfoot pain, swelling or ecchymosis after a foot injury. Missed or inadequately reduced injuries lead to chronic pain, deformity and post-traumatic arthritis, which is why prompt diagnosis and anatomic reduction are emphasised worldwide.
- Recommendation
- Weight-bearing radiographs, then CT (weight-bearing CT increasingly preferred)
- Evidence / Source
- Systematic reviews and emergency-medicine reviews (Level III-IV)
- Recommendation
- Most studies use diastasis of 2 mm (range 1-3 mm) or any TMT incongruity
- Evidence / Source
- Pearsall 2023 systematic review of operative indications (Level IV)
- Recommendation
- Primary arthrodesis of medial 2-3 rays favoured over ORIF
- Evidence / Source
- Ly & Coetzee RCT (Level I)
- Recommendation
- Anatomic reduction with stable fixation (screws or bridge plate); avoid fusing all 5 joints
- Evidence / Source
- Myerson 1986; Mulier 2002; Philpott 2021 meta-analysis
- Classification used: Nunley-Vertullo for subtle athletic sprains; Myerson for fracture-dislocations (most cited operative-indication systems, Pearsall 2023).
- Fixation construct: transarticular screws vs dorsal bridge plating; some evidence favours bridge plating, but no construct is proven universally superior (Philpott 2021).
- Suture-button / flexible fixation: used in some centres for isolated ligamentous instability; promising single-study results, limited comparative data.
- Weight-bearing CT availability drives how often subtle injuries are detected (resource-dependent).
- No dedicated joint registry captures Lisfranc injuries (national joint registries such as NJR, AJRR, AOANJRR track arthroplasty, not TMT trauma); evidence is from trials, cohorts and systematic reviews.
- Diabetic / neuropathic patients: higher rate of delayed diagnosis and progression to Charcot neuroarthropathy; consider extended fixation and lower threshold for surgery (Levitt 2013).
- Paediatric / adolescent: rare and easily missed (about 20% missed); satisfactory outcomes if adequately reduced (Kushare 2020).
Across emergency and orthopaedic literature, the recurring reasons for a missed Lisfranc injury are: accepting a "normal" radiology report without personally reviewing the films, not obtaining weight-bearing or CT imaging when suspicion is high, missing a subtle fleck sign, and dismissing the injury as a simple midfoot sprain. Document the mechanism, weight-bearing status, plantar ecchymosis, neurovascular examination, the specific radiographic lines checked, and the measured 1st-2nd metatarsal diastasis. If treated non-operatively, repeat weight-bearing radiographs to detect late displacement.
MCQ Practice Points
Q: What is the Lisfranc ligament and where does it attach?
A: The Lisfranc ligament (oblique ligament) is the strongest ligament of the TMT complex. It runs from the lateral plantar aspect of the medial cuneiform to the medial base of the 2nd metatarsal. It has three bundles: dorsal (weakest), interosseous (strongest), and plantar. Critically, there is NO ligament between the 1st and 2nd metatarsal bases - the Lisfranc ligament from the medial cuneiform is the sole stabilizer of this interval.
Q: Describe the Myerson classification of Lisfranc injuries.
A: Type A = total incongruity (all 5 TMTs displaced in same direction, homolateral). Type B = partial incongruity (B1 = medial column involved, 1st-2nd TMTs; B2 = lateral column involved, 3rd-4th-5th TMTs). Type C = divergent (1st ray displaced medially, 2nd-5th rays displaced laterally; highest energy, worst prognosis). Classification guides fixation: screws for medial column, K-wires for lateral column.
Q: What is the fleck sign and what is its significance?
A: The fleck sign is a small avulsion fracture at the base of the 2nd metatarsal, best seen on AP radiograph. It represents avulsion of the Lisfranc ligament insertion. The fleck sign is pathognomonic for Lisfranc injury (93% sensitivity, 100% specificity). Its presence mandates surgical exploration even if no other radiographic abnormalities are apparent. Average size is 2-3mm, so it can be easily missed on cursory review.
Q: What is the key difference in outcomes between ORIF and primary arthrodesis for purely ligamentous Lisfranc injuries?
A: Purely ligamentous Lisfranc injuries (no fractures, ligament disruption only) have 50% poor outcomes with ORIF due to progressive loss of reduction. Primary arthrodesis of the medial 3 TMTs shows 85% good/excellent outcomes with only 5% revision rate (Ly & Coetzee, JBJS 2006). This represents an evidence-based shift in practice over the last 15 years. ORIF remains acceptable for fracture-dislocations where bone provides stability.
Q: Why are screws used for the medial column but only K-wires for the lateral column in Lisfranc ORIF?
A: The medial column (1st-2nd-3rd TMTs) is rigid with minimal physiologic motion (2-3°), serving as a stable lever for push-off. Screw fixation provides necessary stability. The lateral column (4th-5th TMTs) is mobile with 10-15° of physiologic motion, essential for foot adaptation to terrain. Rigid screw fixation of the lateral column destroys this motion, leading to overload of the medial column and accelerated arthritis. Temporary K-wires maintain reduction during healing but are removed at 6 weeks to restore motion.
Q: What is the incidence of post-traumatic arthritis after Lisfranc injury and what are the risk factors?
A: 30-50% of patients develop symptomatic post-traumatic arthritis despite optimal treatment. Risk factors include: high-energy mechanism, cartilage damage at time of injury, residual displacement (even 2mm leads to 90% arthritis rate), associated navicular or cuneiform fractures, and delayed diagnosis. Many patients eventually require salvage arthrodesis of affected TMT joints. This high arthritis rate is why some surgeons advocate primary arthrodesis to eliminate this risk.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old footballer presents to emergency department after twisting his midfoot during a tackle. He has midfoot swelling and is unable to weight-bear. X-rays are reported as 'normal' by the emergency physician. How would you assess and manage this patient?”
“You are taking a 35-year-old patient to theatre for ORIF of an acute Lisfranc fracture-dislocation (Myerson Type A). Walk me through your surgical approach and fixation strategy.”
“You have a 32-year-old high-demand manual laborer with a purely ligamentous Lisfranc injury (no fractures, 4mm diastasis on weight-bearing CT). Your colleague suggests ORIF. What is your management and what evidence guides your decision?”
Key Anatomy
- Lisfranc ligament = medial cuneiform to 2nd MT base (strongest TMT ligament)
- NO ligament between 1st-2nd MT bases (Lisfranc ligament is sole stabilizer)
- 2nd MT recessed 2-3mm (keystone of Roman arch configuration)
- Medial column (1st-2nd-3rd TMTs) = rigid, minimal motion
- Lateral column (4th-5th TMTs) = mobile, 10-15° motion
Classification - Myerson
- Type A = total incongruity (all TMTs same direction)
- Type B1 = partial medial (1st-2nd TMTs)
- Type B2 = partial lateral (3rd-4th-5th TMTs)
- Type C = divergent (1st medial, 2-5 lateral, worst prognosis)
Diagnosis - FLECK Mnemonic
- Fleck sign = avulsion 2nd MT base (pathognomonic, 93% sensitivity)
- Line disruption = 1st MT to 1st cuneiform on AP
- Extra space = greater than 2mm between 1st-2nd MTs (surgical indication)
- Column disruption = 2nd MT to 2nd cuneiform on AP (most critical)
- K-sign = 4th MT to cuboid on oblique
- Weight-bearing CT = gold standard if X-rays normal (94% sensitivity)
Treatment Algorithm
- Purely ligamentous injury → Primary arthrodesis 1st-2nd-3rd TMTs (85% good outcomes)
- Fracture-dislocation → ORIF (screws medial 3, K-wires lateral 2)
- Greater than 2mm diastasis = absolute surgical indication
- Hardware removal mandatory at 4-6 months after ORIF (prevent screw breakage)
- Non-weight-bearing 6 weeks → progressive weight-bearing 6-12 weeks
Surgical Pearls
- Dorsal double-incision approach (medial + lateral)
- Protect deep peroneal nerve (medial) and superficial peroneal (lateral)
- Reduction sequence: 1st TMT → 2nd TMT keystone → 3rd TMT → lateral column
- Screw 2nd MT into medial cuneiform (NOT 2nd cuneiform - poor purchase)
- K-wires only for lateral column (preserve motion)
- Anatomic reduction critical - even 2mm residual leads to 90% arthritis
Evidence Base and Key Trials
Primary Arthrodesis vs ORIF for Primarily Ligamentous Lisfranc Injuries (Landmark RCT)
- Prospective randomised trial: 41 patients with isolated primarily ligamentous Lisfranc injuries (20 ORIF, 21 primary arthrodesis of medial 2-3 rays), mean follow-up 42.5 months
- Mean AOFAS Midfoot score at 2 years: 88 (arthrodesis) vs 68.6 (ORIF), p less than 0.005
- Patient-estimated activity level: 92% of pre-injury (arthrodesis) vs 65% (ORIF), p less than 0.005
- 5 of 20 ORIF patients developed deformity or osteoarthrosis and were eventually treated with arthrodesis
- Anatomic initial reduction obtained in 18 of 20 (ORIF) and 20 of 21 (arthrodesis)
Myerson Classification: Fracture-Dislocations of the Tarsometatarsal Joints (Defining Paper)
- Series of 76 tarsometatarsal fracture-dislocations in 72 patients; introduced the type A (total incongruity), B (partial incongruity) and C (divergent) classification still used today
- Only 27 of 55 feet (49%) achieved an excellent or good result at mean 4.2-year follow-up
- Quality of the initial reduction was the major determinant of outcome
- Direct crush injuries did poorly (1 of 8 good or excellent)
- Recommended open reduction for displacement greater than 2 mm or talometatarsal angle greater than 15 degrees after closed reduction