'Dripping Candle Wax' Sclerosing Bone Dysplasia | Sclerotomal Distribution | MAP2K1 Mutation
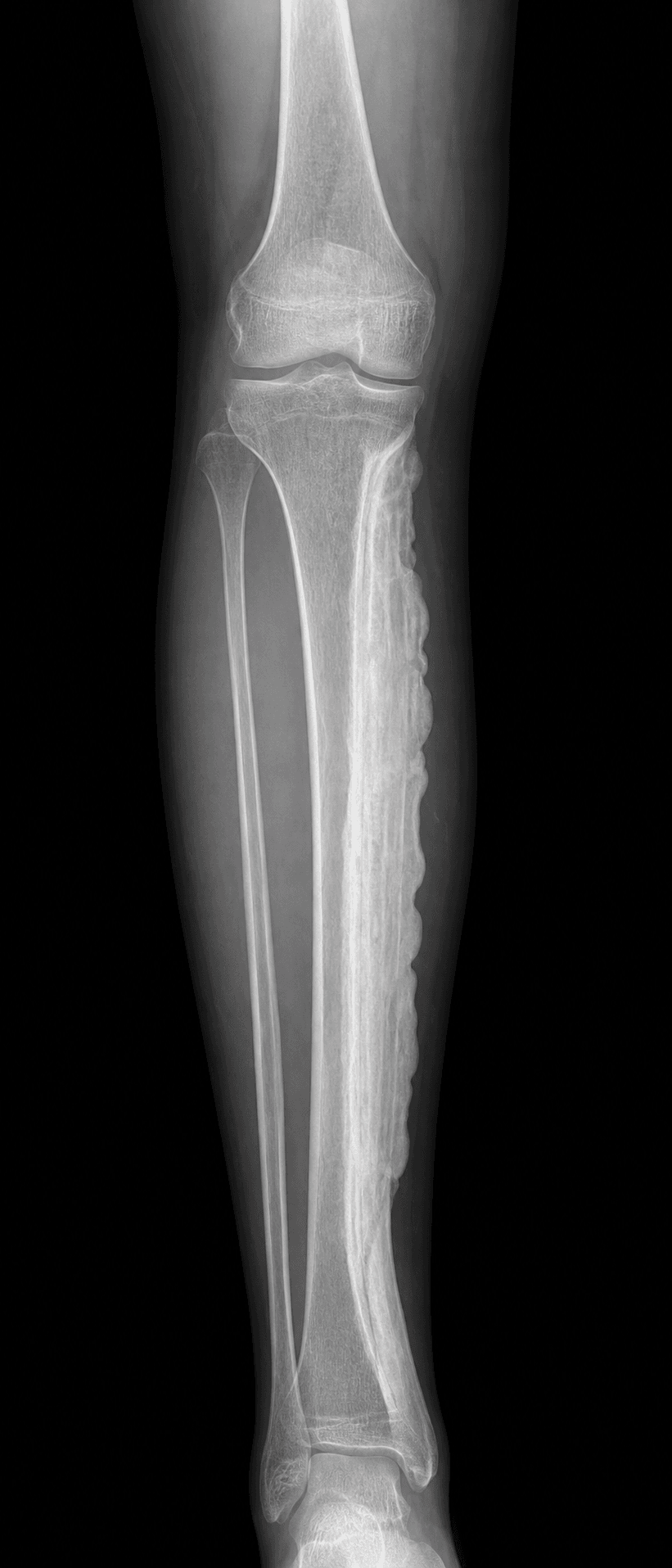
- Dripping candle wax appearance - pathognomonic dense cortical hyperostosis flowing along bone cortex on radiographs
- Sclerotomal distribution - classically follows a single sclerotome (dermatomal equivalent for bone)
- MAP2K1 somatic mutation - identified in approximately 50% of cases, activates MAPK/ERK pathway
- Pain and stiffness - predominant symptoms; contractures from soft tissue involvement
- Surgery has high recurrence - limited surgical role; excision complicated by disease recurrence and joint stiffness
- “Describe the classic radiographic appearance: dense, irregular cortical hyperostosis resembling 'dripping candle wax' flowing down the bone
- “Know the differential diagnosis: osteopoikilosis (round lesions), osteopathia striata (linear striations), parosteal osteosarcoma, myositis ossificans
- “Understand management is primarily conservative: NSAIDs, physiotherapy, bisphosphonates trial; surgery reserved for severe contractures or deformity
- “Surgical complications include high recurrence, stiffness, and incomplete symptom relief
Dripping candle wax appearance - dense, flowing cortical hyperostosis along one side of the bone cortex. This is the hallmark imaging finding and is virtually diagnostic. No other condition produces this exact pattern.
Single sclerotome involvement - the disease classically affects bones, soft tissues, and skin derived from a single somite. This explains the linear, segmental distribution often confined to one limb.
Somatic mosaic mutation in MAP2K1 gene identified in ~50% of cases. This activates MEK1 and the MAPK/ERK signaling pathway, causing osteoblast hyperactivity. This is a post-zygotic mutation (not inherited).
High surgical recurrence rate - disease often recurs after excision. Joint contracture release complicated by recurrent stiffness. Bone excision and soft tissue releases have unpredictable outcomes. Conservative management is first-line.
- Key Features
- Characteristic imaging, no symptoms
- Management
- Observation, reassurance, no treatment
- Exam Pearl
- Many cases are discovered incidentally on imaging
- Key Features
- Symptomatic but functional
- Management
- NSAIDs, physiotherapy, bisphosphonate trial
- Exam Pearl
- Conservative management is first-line for most cases
- Key Features
- Functional impairment, failed conservative Rx
- Management
- Surgical release, osteotomy, or excision
- Exam Pearl
- Warn patient about high recurrence and stiffness risk
Overview and Epidemiology
Melorheostosis (from Greek: melos = limb, rhein = flow, osteon = bone) is a rare, sporadic sclerosing bone dysplasia characterized by dense cortical hyperostosis with a pathognomonic dripping candle wax appearance on radiographs. First described by Leri and Joanny in 1922, it remains one of the rarest bone conditions, with fewer than 500 cases reported in the literature. The 2018 discovery of somatic MAP2K1 mutations (Kang et al.) has transformed understanding of its pathogenesis.
- Incidence: Estimated 1 per 1,000,000 (extremely rare)
- Age: Any age; 50% present before age 20
- Gender: Equal male:female distribution
- Inheritance: Sporadic (somatic mosaic mutation)
- Laterality: Usually unilateral, confined to one limb
- Onset: Childhood to adulthood, insidious
- Progression: Slowly progressive over decades
- Distribution: Follows sclerotomal pattern
- Symptoms: Pain (most common), stiffness, contractures
- Prognosis: Benign but disabling; no malignant transformation
Anatomic Distribution
Melorheostosis shows a characteristic pattern of involvement:
- Lower limb predominance: 70% of cases
- Upper limb: 20% of cases
- Axial skeleton: Rare (10%), usually in combination with limb disease
- Monostotic vs polyostotic: Equal distribution; polyostotic often in adjacent bones
- Sclerotomal pattern: Classically involves bones, muscles, fascia, and skin from a single embryonic somite
The sclerotomal distribution explains why the disease often follows a dermatomal pattern, with skin and soft tissue changes overlying the affected bones.
Pathophysiology and Molecular Genetics
MAP2K1 Somatic Mutation
The landmark 2018 discovery by Kang et al. identified somatic activating mutations in MAP2K1 (encoding MEK1) in melorheostosis lesions. This explains the sporadic, non-inherited nature and mosaic distribution. The mutation activates the RAS-MAPK-ERK signaling pathway, leading to osteoblast hyperactivity and excessive bone formation. Importantly, mutations are found in affected tissue only (not blood), confirming somatic mosaicism.
- Gene: MAP2K1 (mitogen-activated protein kinase kinase 1)
- Protein: MEK1 (dual-specificity kinase)
- Mutation type: Activating, somatic, mosaic
- Pathway: RAS-RAF-MEK-ERK cascade
- Effect: Constitutive ERK activation in osteoblasts
- Osteoblasts: Hyperactive bone formation
- Bone remodeling: Uncoupled, favoring formation
- Soft tissues: Fibroblast activation, fibrosis
- Vasculature: Vascular malformations in some cases
- Skin: Scleroderma-like changes over affected areas
Histopathology
Microscopic examination of affected bone reveals:
- Dense lamellar bone: Mature, well-organized lamellar bone (not woven)
- Haversian system preservation: Normal osteons within sclerotic bone
- Trabecular thickening: Increased trabecular bone mass
- Periosteal new bone: Layers of new bone on cortical surface
- Soft tissue fibrosis: Dense fibrous tissue in adjacent soft tissues
- No inflammatory infiltrate: Distinguishes from chronic osteomyelitis
- No nuclear atypia: Distinguishes from malignancy
Sclerotomal Theory
The classic theory explaining melorheostosis distribution is the sclerotomal hypothesis:
- Sclerotome: Embryonic somite derivative that forms vertebra and associated bones
- Single sclerotome: Disease affects structures from one embryonic segment
- Linear pattern: Explains why disease follows a limb in linear fashion
- Mosaic mutation: Fits with post-zygotic somatic mutation affecting single cell lineage
However, some cases do not fit this pattern, suggesting alternative mechanisms or earlier mutations affecting multiple lineages.
Clinical Presentation
Cardinal Features
The clinical presentation of melorheostosis is highly variable, ranging from incidental discovery to severe disability:
- Pain (50-80%): Dull, aching, often worse with activity
- Stiffness (60-80%): Joint contractures, reduced range of motion
- Deformity (40-60%): Limb length discrepancy, angular deformity
- Skin changes (20-40%): Scleroderma-like hardening over affected areas
- Limb swelling (30%): From bone enlargement and soft tissue involvement
- Quality: Deep, aching, bone pain
- Pattern: Often worse with activity, may have night pain
- Location: Over affected bone segment
- Progression: Slowly worsening over years
- Response to NSAIDs: Variable, often partial relief
- Joints: Adjacent to affected bones
- Mechanism: Soft tissue fibrosis, capsular involvement
- Common sites: Knee, elbow, ankle, fingers
- Severity: Mild limitation to severe fixed contracture
- Progression: Gradually worsening over time
Physical Examination
- Limb asymmetry (affected limb may be shorter or angular)
- Skin changes: thickening, induration, scleroderma-like appearance
- Visible bone enlargement in superficial locations
- Muscle wasting from disuse or direct involvement
- Hard, irregular bone masses along cortical surface
- Non-tender or mildly tender
- Skin may feel indurated, bound down
- Reduced soft tissue mobility over affected areas
- Joint contractures in adjacent joints
- Fixed flexion deformities common
- End-range pain with stretching
- May have limb length discrepancy
Age-Related Presentations
- Limb length discrepancy
- Angular deformity
- Delayed motor milestones
- May be mistaken for developmental conditions
- Pain with increasing activity
- Joint stiffness affecting sports, activities
- Cosmetic concerns
- Peak time for diagnosis
- Progressive pain and stiffness
- Occupational limitations
- May have been symptomatic for decades before diagnosis
- Osteoarthritis in affected joints
STIFFClinical Features
Hook:STIFF - the disease makes joints STIFF! Pain and contractures are the cardinal clinical features.
Imaging and Diagnosis

Radiographic Imaging - Diagnostic Standard
The dripping candle wax appearance is virtually pathognomonic for melorheostosis. This consists of dense, irregular, flowing cortical hyperostosis along one side of the bone, resembling wax that has dripped down and hardened along a candle. The sclerosis typically involves one cortex (eccentric) and may extend across joints to involve adjacent bones in the same sclerotome.
Key Radiographic Features:
- Dense cortical hyperostosis: Markedly increased bone density
- Flowing/dripping pattern: Irregular wavy margins like melted wax
- Eccentric distribution: Usually one side of bone cortex
- Crosses joints: May extend to adjacent bones
- No periosteal reaction: Distinguishes from infection/tumor
- Soft tissue calcification: May see adjacent soft tissue ossification
Radiographic Patterns
Dense cortical hyperostosis flowing along the bone cortex, typically along one side. The outer margin is irregular and wavy, while the inner margin may encroach on the medullary canal. This pattern is pathognomonic.
Focal sclerotic areas within the medullary cavity, resembling osteopoikilosis. May coexist with classic dripping wax pattern. This variant is called melorheostotic variant of mixed sclerosing bone dysplasia.
Linear striations of dense bone, similar to osteopathia striata. May represent overlap syndrome or variant pattern. Less common than classic presentation.
Soft tissue ossification extending from bone, mimicking myositis ossificans or parosteal osteosarcoma. Important to correlate with clinical history (no trauma history) and histology.
CT Imaging
CT provides superior assessment of:
- Cortical extent: Precise delineation of sclerotic bone
- Medullary involvement: Extension into medullary canal
- Joint involvement: Intra-articular extension, osteoarthritis
- Soft tissue ossification: Better detection than radiographs
- Surgical planning: 3D reconstruction for complex cases
MRI - Soft Tissue Assessment
MRI is valuable for evaluating:
- Soft tissue fibrosis: Low signal on T1 and T2
- Muscle involvement: Atrophy, fibrosis, fatty replacement
- Neurovascular compression: Important for surgical planning
- Joint involvement: Synovitis, capsular thickening
- Marrow changes: Usually normal signal in sclerotic areas
- Indication
- Initial diagnosis, surveillance
- Key Findings
- Dripping candle wax, cortical hyperostosis
- Indication
- Surgical planning, cortical detail
- Key Findings
- Precise extent, 3D reconstruction
- Indication
- Soft tissue assessment, nerve evaluation
- Key Findings
- Fibrosis, muscle involvement, neurovascular
Bone Scintigraphy
- Increased uptake: In affected areas on bone scan
- Extent assessment: May show involvement beyond radiographic findings
- Activity monitoring: Intensity may correlate with disease activity
- Limited specificity: Cannot distinguish from other sclerotic conditions
CANDLEDiagnostic Features of Melorheostosis
Hook:CANDLE - think of wax dripping down a candle! The dripping candle wax appearance is the key diagnostic feature.
Differential Diagnosis
Other Sclerosing Bone Dysplasias
- Radiographic Pattern
- Dripping candle wax
- Distribution
- Sclerotomal, unilateral
- Key Distinguishing Feature
- Flowing cortical hyperostosis along one cortex
- Radiographic Pattern
- Multiple round foci (spotted bones)
- Distribution
- Bilateral, symmetric
- Key Distinguishing Feature
- Round/oval sclerotic foci near joints
- Radiographic Pattern
- Linear striations
- Distribution
- Bilateral, symmetric
- Key Distinguishing Feature
- Longitudinal dense lines in metaphyses
- Radiographic Pattern
- Fusiform cortical thickening
- Distribution
- Bilateral, symmetric, diaphyseal
- Key Distinguishing Feature
- Camurati-Engelmann, inherited, systemic symptoms
Osteopoikilosis (spotted bones) consists of multiple small, round, well-defined sclerotic foci clustered near joints - completely different from the flowing, linear dripping wax of melorheostosis. Osteopathia striata shows linear striations but is bilateral and symmetric, unlike the unilateral sclerotomal pattern of melorheostosis.
Mixed Sclerosing Bone Dysplasia
Some patients show features of multiple sclerosing dysplasias:
- Melorheostosis + osteopoikilosis
- Osteopathia striata + osteopoikilosis
- Overlap syndromes suggest common pathogenetic mechanism
This ends the comparison of sclerosing dysplasias.
POMPDifferential Diagnosis
Hook:POMP - think of the POMP and circumstance of diagnosis! These are the key differentials for sclerotic bone lesions.
Management
Conservative Management - First-Line Approach
Conservative management is the mainstay of treatment for melorheostosis. Surgery has unpredictable results with high recurrence rates. Most patients can be managed with a combination of analgesics, physiotherapy, and supportive measures. Surgery is reserved for severe contractures or deformity causing functional impairment.
- NSAIDs: First-line analgesics, often provide partial relief
- Paracetamol: Adjunct for mild pain
- Neuropathic agents: Gabapentin, pregabalin if nerve involvement
- Opioids: Reserved for severe, refractory pain
- Local measures: Heat, ice, TENS
- Goals: Maintain ROM, prevent contracture progression
- Stretching: Regular stretching of affected joints
- Strengthening: Maintain muscle function
- Hydrotherapy: May be beneficial for pain and mobility
- Orthotics: Splints to maintain position, AFOs for drop foot
Bisphosphonates
Bisphosphonates inhibit osteoclast activity and reduce bone turnover. While melorheostosis is primarily an osteoblastic condition, there is some evidence for pain reduction with bisphosphonate therapy.
- Case reports and small series suggest benefit in some patients
- May reduce pain scores in subset of patients
- Effect on bone formation is limited
- Trial of therapy is reasonable for symptomatic patients
- Alendronate 70mg weekly or
- Zoledronic acid 5mg IV annually
- Trial for 6-12 months to assess response
Evidence for bisphosphonate efficacy in melorheostosis is limited to case reports and small case series. Response is variable, with some patients experiencing significant pain relief and others showing no benefit. A therapeutic trial is reasonable but patients should be counseled about uncertain efficacy.
Other Medical Therapies
- Nifedipine: Calcium channel blocker, reported to reduce pain in isolated cases
- MEK inhibitors: Targeted therapy under investigation given MAP2K1 mutation
- Denosumab: RANKL inhibitor, theoretical benefit, case reports only
This section covers the conservative management of melorheostosis.
Two Genetic Routes to Melorheostosis
The MAP2K1 somatic mutation is the topic's focus, but the evidence cards and references (Wordsworth; Hellemans) also invoke LEMD3 without the body ever reconciling the two.
- The common, sporadic form is somatic MAP2K1. Classic isolated melorheostosis is driven by a post-zygotic (mosaic) activating MAP2K1 (MEK1) mutation present in the affected tissue only - so it is not inherited and cannot be passed on. A minority carry related somatic RAS-MAPK changes (KRAS, SMAD3).
- A separate, familial route is germline LEMD3. Germline loss-of-function LEMD3 (MAN1) mutations cause osteopoikilosis and Buschke-Ollendorff syndrome (osteopoikilosis plus connective-tissue naevi), and melorheostosis can arise within these families - the 'osteopoikilosis-associated' or mixed-sclerosing-bone-dysplasia form. LEMD3 normally antagonises TGF-beta/BMP signalling.
- Why it matters. Isolated sporadic disease is a somatic MAP2K1 problem with no inheritance risk, whereas melorheostosis appearing alongside osteopoikilosis or connective-tissue naevi points to a germline LEMD3 disorder that IS autosomal dominant - a distinction that changes family counselling (see the osteopoikilosis topic for the LEMD3 detail).
Q: What are the two genetic routes to melorheostosis?
A: (1) The common sporadic isolated disease is a somatic (post-zygotic, mosaic) activating MAP2K1 (MEK1) mutation in the affected tissue only (Kang 2018) - not inherited (minority: somatic KRAS/SMAD3). (2) The rarer osteopoikilosis-associated / familial form is germline loss-of-function LEMD3 (MAN1), which also causes osteopoikilosis and Buschke-Ollendorff syndrome and is autosomal dominant. So isolated melorheostosis carries no inheritance risk, but melorheostosis with osteopoikilosis or connective-tissue naevi signals a germline LEMD3 disorder - which changes counselling.
Why MEK Inhibitors Are the Rational Targeted Therapy
The topic lists 'MEK inhibitors under investigation' but never explains why they are the logical targeted therapy, nor the mechanistic subtlety the Kang study revealed.
- MEK inhibitors hit the mutated kinase directly. MAP2K1 encodes MEK1; the activating mutation makes MEK1 signal constitutively to ERK. A MEK inhibitor (for example trametinib or selumetinib) blocks that kinase, so it is the rational pathway-directed therapy - the same drug class already established in other RAS-MAPK 'RASopathies' (selumetinib is approved for NF1 plexiform neurofibromas).
- The mechanism is subtler than 'too much bone'. The Kang study showed the mutation increases osteoblast proliferation yet inhibits BMP2-mediated mineralisation and differentiation, producing excess unmineralised osteoid rather than simply more normal bone - which is why merely restraining resorption (bisphosphonates) is only partly helpful and pathway blockade is attractive.
- But it remains investigational. MEK-inhibitor use in melorheostosis is off-label and unproven, so it is not yet standard care - conservative management remains first-line.
Q: Why are MEK inhibitors a rational targeted therapy in melorheostosis?
A: MAP2K1 encodes MEK1; the somatic activating mutation makes MEK1 signal constitutively to ERK, so a MEK inhibitor (trametinib/selumetinib) blocks the mutated kinase directly - the same class already used in other RAS-MAPK 'RASopathies' (selumetinib is approved for NF1 plexiform neurofibromas). Mechanistically the mutation increases osteoblast proliferation but inhibits BMP2-mediated mineralisation (excess unmineralised osteoid), which is why anti-resorptive bisphosphonates only partly help and pathway blockade is attractive. It remains investigational/off-label, so conservative care stays first-line.
Guidelines, Registries & Global Practice
Melorheostosis is too rare for any society (AAOS, BOA, EFORT, AO, IOF) to issue a dedicated guideline, and it has no disease registry. Evidence is confined to case reports and a few retrospective single-centre cohorts (Mayo Clinic n=24; Freyschmidt n=23). The most authoritative reference dataset is the NIH/NIAMS natural-history programme that defined the somatic MAP2K1 basis. The examiner's expectation is therefore that you cite the level of evidence honestly and default to multidisciplinary, predominantly non-operative care.
Global Epidemiology
- Incidence: approximately 1 per 1,000,000 — among the rarest sclerosing bone dysplasias; no geographic clustering reported
- Distribution: lower-limb predominant (about two-thirds), polyostotic more common than monostotic in cohort series; female predominance (up to 4:1) in the Mayo cohort, though earlier series report an equal sex ratio
- Age: any age; most present as young adults, with diagnostic delay of years to decades being typical worldwide
Reference Sources Instead of Guidelines
- Type
- Natural-history + translational
- Contribution
- Established somatic MAP2K1 (and minority RAS-MAPK) genetic basis; phenotype-genotype correlation
- Type
- Retrospective
- Contribution
- Symptom frequencies, interdisciplinary care model
- Type
- Translational
- Contribution
- Rationale for targeted therapy under investigation; no approved indication
Practice Variation by Resource Setting
- Diagnosis
- MRI + CT, lesional genetic testing (MAP2K1), referral to bone-dysplasia/sarcoma MDT; biopsy only if malignancy suspected
- Management
- Analgesia, physiotherapy, selective bisphosphonate trial; complex deformity/contracture surgery at specialist centres; trial access to MEK inhibitors
- Diagnosis
- Diagnosis on plain radiographs alone (dripping candle-wax pattern); genetic testing usually unavailable
- Management
- Conservative analgesia and physiotherapy; surgery reserved for disabling deformity, with realistic counselling about recurrence
Pragmatic Global Principles
- Diagnosis is usually radiographic; reserve biopsy for cases where parosteal osteosarcoma or another malignancy cannot be excluded
- Manage at, or in consultation with, a centre experienced in sclerosing bone dysplasias or musculoskeletal oncology
- Bisphosphonate and MEK-inhibitor use is off-label/investigational everywhere — counsel on uncertain efficacy and document informed consent
- Intensive, sustained physiotherapy is the single most important determinant of a durable result after any contracture surgery, irrespective of health system
Viva Practice Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old woman presents with a 5-year history of progressive right knee stiffness and pain. Radiographs show dense cortical hyperostosis along the medial femur and tibia with a 'dripping candle wax' appearance. How would you assess and manage this patient?”
“You are shown a radiograph demonstrating dense cortical sclerosis along one cortex of the femur. What is your differential diagnosis and how would you distinguish between these conditions?”
“A patient with melorheostosis affecting the knee has a 45-degree fixed flexion contracture despite 12 months of conservative management. They are requesting surgery. How would you counsel them?”
Definition and Key Facts
Molecular Pathogenesis
Clinical Presentation
Radiographic Features
Differential Diagnosis
Management
Exam Pearls
Evidence Base
Somatic activating MAP2K1 mutations cause melorheostosis
- Whole-exome sequencing identified somatic mosaic MAP2K1 mutations in affected (but not unaffected) bone of all 8 unrelated patients studied
- Activating mutations (Q56P, K57E, K57N) cluster tightly in the MEK1 negative regulatory domain, raising p-ERK1/2
- Mosaicism was also detected in skin overlying bone lesions in 4 of 5 patients tested
- Mutations increase osteoblast proliferation yet INHIBIT BMP2-mediated mineralization/differentiation, explaining the excess unmineralized osteoid
- Implicates MEK1 inhibition as a candidate therapeutic avenue
Melorheostosis: a review of 23 cases
- Series of 23 consecutive cases; equal gender ratio, mean age 34 years
- Five distinct radiographic patterns: osteoma-like (n=7), classic candle-wax (n=5), osteopathia striata-like (n=6), mixed (n=4), myositis ossificans-like (n=1)
- NON-classic patterns prevailed — the 'classic' dripping candle-wax was present in only 5/23, so absence does not exclude the diagnosis
- Lower extremity involvement predominated (16/23)
- Author proposes somatic mosaicism (not embryonic sensory-nerve infection) to explain the sporadic, asymmetric segmental pattern
Melorheostosis and its treatment with intravenous zoledronic acid
- Middle-aged man with painful tibial melorheostosis (confirmed on imaging and biopsy)
- Early symptom control after a single infusion of IV zoledronic acid
- Prolonged symptom relief accompanied by sustained suppression of the bone-resorption marker beta-CrossLaps
- Supports a trial of IV bisphosphonate for pain, monitored with resorption markers
- Single case report — efficacy remains anecdotal, no controlled data
Melorheostosis: a retrospective clinical analysis of 24 patients at the Mayo Clinic
- Largest single-institution cohort: 24 patients (1972-2010); female:male ratio 4:1, mean age at presentation 36.5 years
- Lower extremity most commonly affected (66.6%), then upper extremity (33.3%), spine (16.6%)
- Two-thirds had multiple-bone (polyostotic) involvement; one-third monostotic
- Pain was the dominant presenting symptom (83.3%), followed by deformity (54.1%) and limited movement (45.8%); numbness/weakness reflect nerve entrapment
- Supports an interdisciplinary, predominantly non-operative pathway with surgery reserved for selected cases
Melorheostosis and osteopoikilosis: a review of clinical features and pathogenesis
- Most melorheostosis arises from somatic MAP2K1 mutations; a minority involve related RAS-MAPK genes (e.g. KRAS)
- MAP2K1-mutant cases are more likely to show the classic dripping candle-wax appearance
- Osteopoikilosis (germline LEMD3/MAN1, perturbed TGF-beta/BMP signalling) can co-occur, supporting a shared pathway
- Four distinct radiographic patterns are recognised with substantial overlap with mixed sclerosing bone dysplasia
- Bone regrowth after surgery is uncommon, but recurrent soft-tissue contractures are the major surgical problem; RASopathy-directed therapies are a future avenue
A multi-omics approach expands the mutational spectrum of MAP2K1-related melorheostosis
- Confirmed the previously reported K57N and K57E negative-regulatory-domain variants in affected tissue of sporadic patients
- Identified a novel catalytic-domain variant (C121Ser) that also constitutively activates ERK — broadening the MAP2K1 mutational spectrum beyond the regulatory hotspot
- Transcriptomic (RNA-seq) analysis showed upregulation of proliferative pathways in affected tissue
- One patient with classic radiographic features had no detectable variant in MAP2K1, SMAD3, LEMD3 or KRAS, indicating locus heterogeneity
- Reaffirms MAP2K1 as the major cause of melorheostosis
References
- Kang H, Jha S, Deng Z, et al. Somatic activating mutations in MAP2K1 cause melorheostosis. Nature Communications. 2018;9(1):1390. PMID: 29643386.
- Freyschmidt J. Melorheostosis: a review of 23 cases. European Radiology. 2001;11(3):474-479. PMID: 11288855.
- Hollick RJ, Black A, Reid D. Melorheostosis and its treatment with intravenous zoledronic acid. BMJ Case Reports. 2010;2010:bcr0420091757. PMID: 22479293.
- Smith GC, Pingree MJ, Freeman LA, et al. Melorheostosis: a retrospective clinical analysis of 24 patients at the Mayo Clinic. PM&R. 2017;9(3):283-288. PMID: 27485676.
- Wordsworth P, Chan M. Melorheostosis and osteopoikilosis: a review of clinical features and pathogenesis. Calcified Tissue International. 2019;104(5):530-543. PMID: 30989250.
- De Ridder R, Boudin E, Zillikens MC, et al. A multi-omics approach expands the mutational spectrum of MAP2K1-related melorheostosis. Bone. 2020;137:115406. PMID: 32387835.
- Hellemans J, Preobrazhenska O, Willaert A, et al. Loss-of-function mutations in LEMD3 result in osteopoikilosis, Buschke-Ollendorff syndrome and melorheostosis. Nature Genetics. 2004;36(11):1213-1218. PMID: 15489854.