Mechanical Overload | Plantar Plate Pathology | Load Redistribution
- Second metatarsal most commonly affected - longest MT, most fixed at Lisfranc joint
- Plantar plate pathology underlies many cases - drawer test assesses integrity
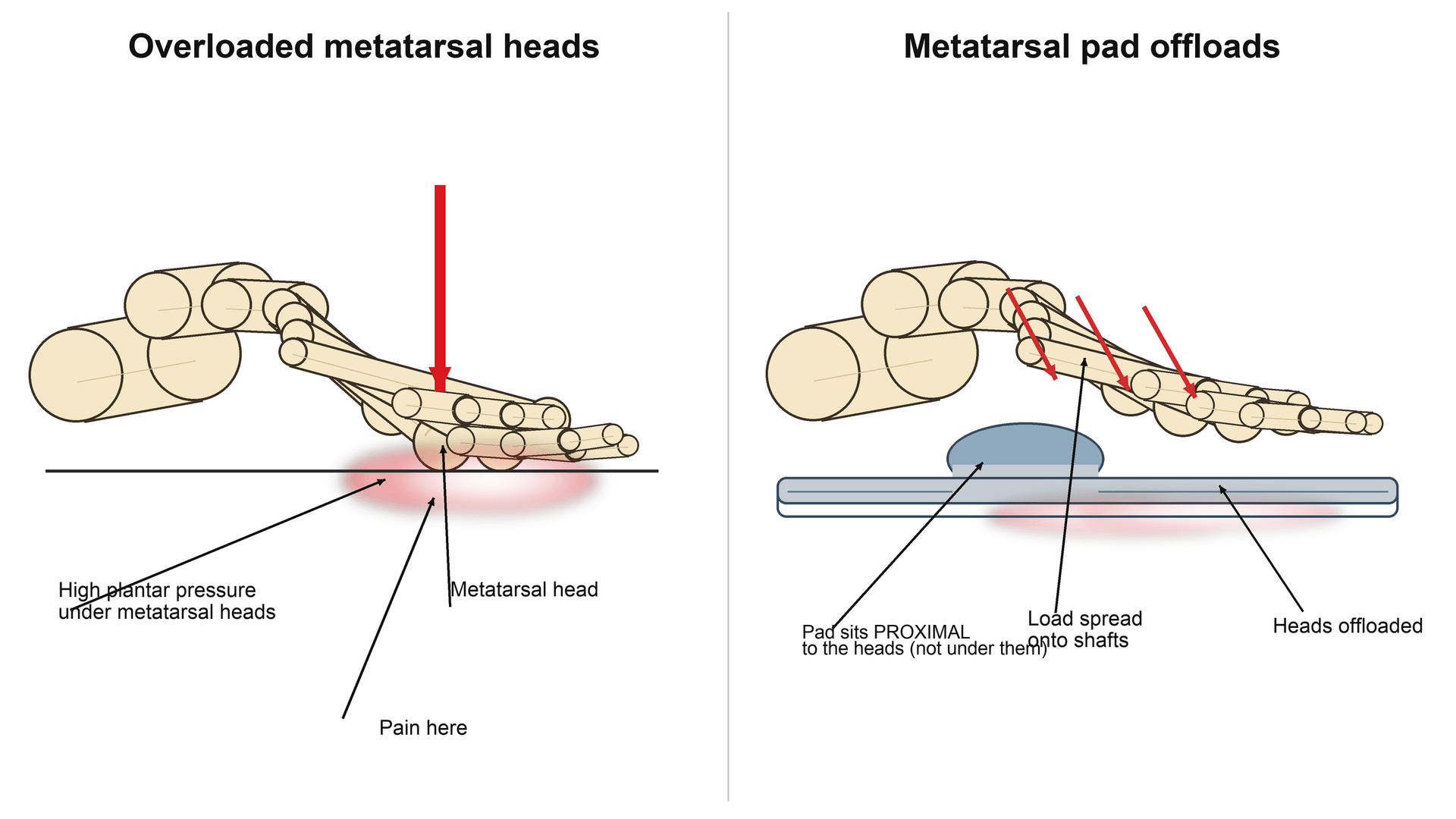
- Conservative management successful in 80% - metatarsal pad PROXIMAL to MT heads
- Weil osteotomy shortens MT 2-4mm to unload - risks transfer metatarsalgia and floating toe
- First ray insufficiency (HV, hypermobility) is common cause - must be addressed
- “Long second MT (Greek foot/Morton's foot) predisposes to overload
- “Plantar plate tear causes crossover toe (toe drifts medially over hallux)
- “Drawer test: excessive dorsal toe translation indicates plantar plate rupture
- “Weil osteotomy: oblique cut parallel to weightbearing surface, shorten 2-4mm
- “Transfer metatarsalgia prevented by cascade shortening and limiting shortening amount
The second metatarsal is most commonly affected because it is typically the longest metatarsal and has the most rigid articulation at Lisfranc joint (no movement). Combined with its position adjacent to the first ray, it is vulnerable to overload when first ray function is impaired by hallux valgus, hypermobility, or prior surgery.
Plantar plate degeneration or rupture underlies many cases of metatarsalgia. The plantar plate is a thick fibrocartilaginous structure that stabilizes the MTP joint. Tear leads to dorsal subluxation, crossover toe (medial drift), and pain directly under MT head. Drawer test assesses integrity - positive if excessive dorsal translation.
80% respond to conservative management: Metatarsal dome or pad placed PROXIMAL to MT heads (not directly under). Stiff-soled shoes to reduce MTP bending. Achilles stretching to reduce forefoot overload. Activity modification. Custom orthotics. Corticosteroid injection with caution (can rupture plantar plate).
Weil osteotomy risks: Transfer metatarsalgia (10-15%) from load shift to adjacent MT. Floating toe (15-30%) where toe loses ground contact. MTP stiffness. Prevention: Limit shortening to 2-4mm. Cascade shortening of adjacent MTs. Address first ray insufficiency. Careful preoperative planning of relative MT lengths.
Overview and Epidemiology
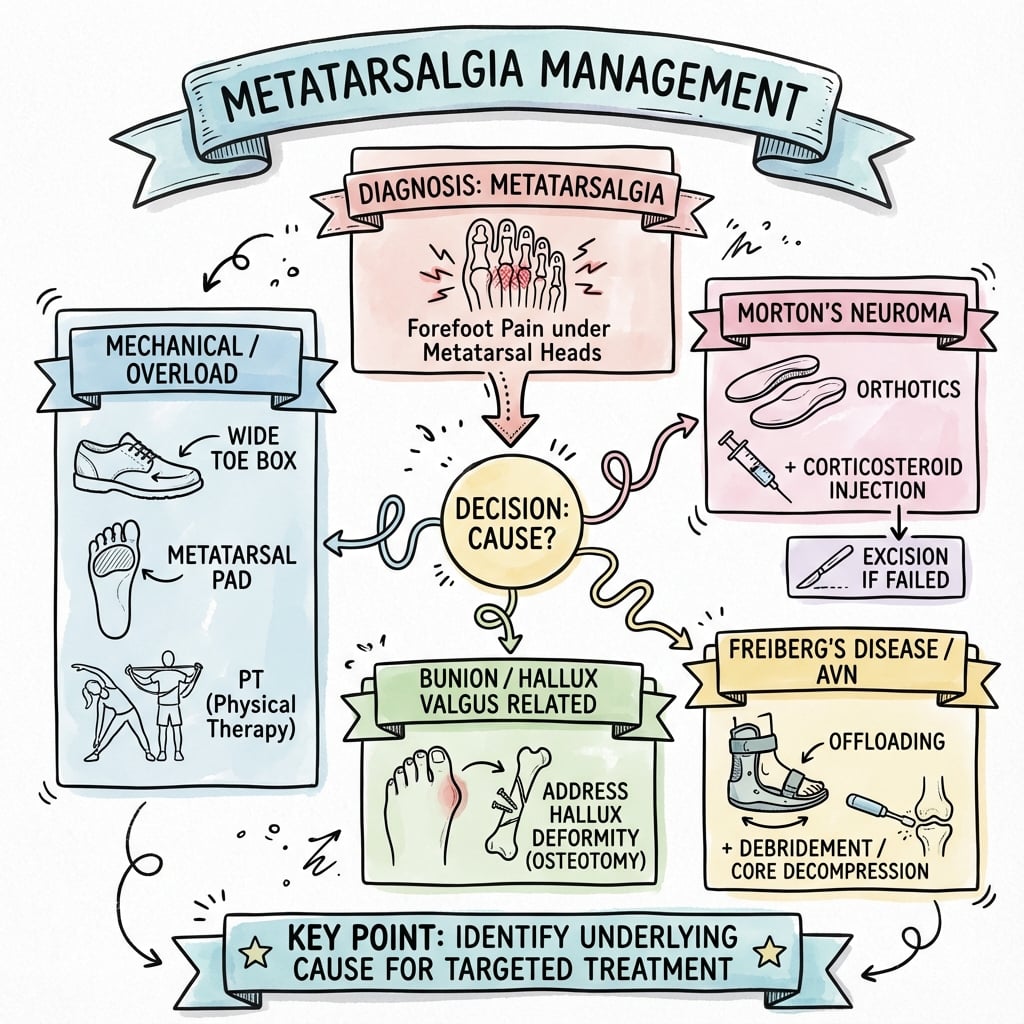
Metatarsalgia is a symptom complex, not a diagnosis. It represents forefoot pain localized to the plantar metatarsal head region from mechanical overload of the lesser metatarsals. Understanding the underlying biomechanical cause is essential for effective treatment. The second metatarsal is most commonly affected due to its typical length (longest) and fixed articulation at the Lisfranc joint.
Definition and Terminology
Metatarsalgia: Pain localized to the plantar aspect of the metatarsal heads, typically involving the lesser metatarsals (second through fifth). The term describes a symptom, not a specific diagnosis.
Key concept: Metatarsalgia is the end result of abnormal load distribution across the forefoot. Identifying and correcting the underlying mechanical or pathologic cause is the goal of treatment.
Epidemiology
Prevalence: One of the most common foot complaints in orthopaedic and podiatric practice. Affects approximately 10-15% of the general population at some point in life.
Demographics:
- Female predominance: 3:1 ratio (high heels, narrow shoes)
- Peak age: 40-60 years
- Athletes: Higher incidence in runners, dancers, sports with repetitive forefoot loading
Metatarsal involvement frequency:
- Second MT: 65-70% of cases (most common)
- Third MT: 20-25%
- Fourth MT: 5-10%
- Multiple MTs: 10-15% involve more than one metatarsal
Why Second MT Most Common?
The second metatarsal is predisposed to overload for several anatomical and biomechanical reasons:
- Longest metatarsal: In approximately 60% of the population (Greek or Morton's foot), the second MT is longer than the first
- Rigid Lisfranc articulation: The second MT has the most fixed tarsometatarsal joint with no movement, unlike the mobile first and fifth rays
- Adjacent to first ray: When first ray function is impaired (hallux valgus, hypermobility, prior surgery), load transfers to the second MT
- Central position: Bears significant load during toe-off phase of gait
Pathophysiology
Forefoot Anatomy
Metatarsals: Five long bones of the forefoot. First metatarsal is shortest and thickest. Second metatarsal is typically longest and most fixed at Lisfranc joint.
Plantar plate: Thick fibrocartilaginous structure on plantar aspect of each MTP joint. Functions include:
- Stabilizes MTP joint in sagittal and transverse planes
- Attachment site for plantar fascia
- Protects metatarsal head from excessive load
- Prevents dorsal subluxation of toe
First ray: Comprises the first metatarsal and medial cuneiform. Normally bears approximately 50% of forefoot load during toe-off.
Normal Load Distribution
Weightbearing distribution:
- First ray: 50% of forefoot load
- Second MT: 15-20%
- Third MT: 10-15%
- Fourth MT: 5-10%
- Fifth MT: 5-10%
Gait cycle: During toe-off, load shifts anteriorly and concentrates on metatarsal heads. Plantar plates and intrinsic muscles stabilize MTP joints.
Pathophysiology of Metatarsalgia
- Pathophysiology
- Excessive load on longest MT head
- Clinical Example
- Greek foot (2nd MT longer than 1st)
- Treatment Approach
- Weil osteotomy to shorten and unload
- Pathophysiology
- First ray fails to bear normal 50% load, transfers to 2nd MT
- Clinical Example
- Hallux valgus, first MT hypermobility, prior HV surgery
- Treatment Approach
- Address first ray pathology
- Pathophysiology
- Loss of MTP stabilization, dorsal subluxation, direct MT head overload
- Clinical Example
- Crossover toe, drawer test positive
- Treatment Approach
- Plantar plate repair plus Weil osteotomy
- Pathophysiology
- Increases forefoot loading during gait
- Clinical Example
- Isolated gastrocnemius contracture
- Treatment Approach
- Achilles stretching or gastrocnemius recession
- Pathophysiology
- Fixed forefoot equinus concentrates load on MT heads
- Clinical Example
- High-arched rigid foot
- Treatment Approach
- Cavus correction if severe, orthotics
- Pathophysiology
- Excessive first MT elevation or shortening shifts load to 2nd MT
- Clinical Example
- After aggressive hallux valgus repair
- Treatment Approach
- Revision osteotomy, first MT plantarflexion
Plantar Plate Pathology
Structure: Fibrocartilaginous plate analogous to the meniscus. Approximately 1-2mm thick. Inserts on plantar base of proximal phalanx and metatarsal neck.
Pathologic changes:
- Degeneration: Chronic repetitive stress causes fibrocartilage breakdown
- Attenuation: Thinning and weakening
- Partial tear: Usually originates at lateral insertion (second MTP)
- Complete rupture: Loss of all stabilization
Clinical consequences of plantar plate failure:
- Dorsal subluxation of toe on MT head
- Medial deviation (crossover toe) - second toe drifts over hallux
- MTP joint instability
- Direct pain under MT head (loss of protective cushioning)
- Positive drawer test (excessive dorsal translation)
Corticosteroid injection for metatarsalgia must be used with caution. Repeated steroid injections can accelerate plantar plate degeneration and precipitate rupture. While steroids may provide short-term symptomatic relief from MTP synovitis, they do not address the underlying mechanical problem and may worsen structural pathology. Maximum 2-3 injections, consider other treatments first.
Secondary Causes
Freiberg's disease: Avascular necrosis of MT head, typically second MT. Affects adolescent females. Presents with pain, limited motion, radiographic changes (flattening, sclerosis, fragmentation).
Morton's neuroma: Interdigital neuroma (perineural fibrosis) between MT heads. Web space pain radiating to toes. Mulder's click pathognomonic.
Rheumatoid arthritis: Systemic inflammatory arthropathy. MTP synovitis, erosions, subluxation. Multiple joints involved bilaterally.
Stress fracture: Acute onset pain. Bony tenderness over MT shaft (not plantar MT head). Second or third MT most common.
Sesamoiditis: Pain under first MT head at sesamoid bones. Distinct from lesser MT metatarsalgia.
Classification Systems
Classification by Etiology
- Subcategory
- Structural anatomic abnormality
- Examples
- Long 2nd MT, cavus foot, first ray hypermobility
- Management Principle
- Correct mechanical abnormality
- Subcategory
- Underlying disease process
- Examples
- RA, Freiberg's, Morton's neuroma, sesamoiditis
- Management Principle
- Treat primary pathology
- Subcategory
- Post-surgical load redistribution
- Examples
- After HV repair, first MT osteotomy, excessive MT shortening
- Management Principle
- Revision surgery to rebalance
This classification guides the treatment approach - primary mechanical causes require structural correction, secondary causes need treatment of underlying pathology, and iatrogenic causes may require revision surgery.
Understanding the etiology helps direct appropriate treatment strategies.
Clinical Assessment
History
Location: Plantar forefoot under MT heads - patient can point to specific MT head
Quality: Aching, burning, sharp with weight-bearing
Aggravating factors:
- Prolonged standing or walking
- High heels (shifts load anteriorly)
- Hard surfaces
- Barefoot walking
- Thin-soled shoes
Relieving factors:
- Rest
- Removing shoes
- Massaging forefoot
Timing: Worse at end of day after cumulative loading
Numbness or burning: Suggests Morton's neuroma (web space, radiates to toes)
Toe deformity: Crossover toe indicates plantar plate rupture
Callus formation: Under specific MT head confirms overload pattern
Instability: Feeling of toe "giving way" suggests plantar plate insufficiency
Swelling: Prominent dorsal MTP swelling suggests synovitis or arthropathy
Night pain: Red flag for tumor, infection (not typical mechanical metatarsalgia)
Physical Examination
Systematic Examination Approach
Standing position: Observe weightbearing alignment
- Foot type: Cavus (high arch), planus (flat), neutral
- First ray position: Hallux valgus, first MT elevation
- Lesser toe alignment: Crossover toe (second over hallux), hammer toes, claw toes
Seated examination:
- Callus pattern: Location and severity indicate specific MT overload
- Swelling: Dorsal MTP swelling (synovitis, arthropathy)
- Skin changes: Ulceration (diabetes, RA), color changes
Inspection provides immediate clues to underlying mechanical problem.
Plantar MT head tenderness: Palpate each MT head individually to localize pain precisely
- Second MT head most commonly tender
- Note which specific MT heads are symptomatic
- Assess for plantar plate prominence (thickening)
Web space compression: Squeeze between MT heads to assess for Morton's neuroma
- Mulder's click: Lateral MT compression while pressing web space
- 3rd web space most common for neuroma
Dorsal MTP palpation: Assess for synovitis, osteophytes, joint swelling
Palpation distinguishes metatarsalgia (MT head tenderness) from neuroma (web space tenderness).
Drawer test (essential for every case):
- Stabilize MT head with one hand
- With other hand, dorsally translate toe on MT head
- Positive: Excessive dorsal translation compared to normal
- Indicates plantar plate tear
- Compare to adjacent toes and contralateral foot
First ray assessment:
- Dorsal mobility test: Dorsally translate first MT on medial cuneiform
- Excessive mobility (hypermobility) predisposes to transfer metatarsalgia
- Assess for hallux valgus deformity
Achilles tightness (Silfverskiold test):
- Measure ankle dorsiflexion with knee extended (gastrocnemius tight if limited)
- Repeat with knee flexed (if improves, isolated gastrocnemius contracture)
- Tight Achilles increases forefoot loading
Range of motion: Assess MTP joint dorsiflexion and plantarflexion. Limited ROM suggests arthropathy or Freiberg's disease.
Special tests identify specific pathology and guide treatment.
Observe walking:
- Antalgic gait (painful, shortened stance phase)
- Early heel-off (avoids toe-off on painful forefoot)
- Toe-walking (Achilles contracture)
Toe-off phase: Normal load shift to forefoot during push-off. Painful toe-off confirms forefoot pathology.
Gait observation confirms functional impact and severity.
The drawer test is the single most important special test for metatarsalgia. Technique: Stabilize the metatarsal head firmly with one hand. With the other hand, grasp the toe and apply dorsally directed force to translate the toe on the MT head. A positive test shows excessive translation (more than 2-3mm) compared to adjacent toes and the contralateral foot. This indicates plantar plate tear or severe attenuation. Always perform bilaterally and compare to establish what is abnormal for that patient. A positive drawer test changes management - plantar plate repair should be considered if surgical treatment is pursued.
A positive drawer test is graded, and the grade drives the operation. The clinical MTP instability grade (from the drawer / "vertical Lachman" test) runs: Grade 0 stable; Grade 1 mild laxity (under half subluxation); Grade 2 moderate (over half subluxation); Grade 3 dislocatable joint; Grade 4 fixed dislocation with rigid deformity. This maps onto the anatomic (Nery-Coughlin) plantar plate grading seen at surgery or on MRI: Grade 0 intact or attenuated; Grade I transverse distal tear involving less than half the plate; Grade II transverse tear of more than half; Grade III extensive tear (often with a longitudinal component); Grade IV complete tear or buttonhole with retraction (frequently with collateral involvement). The practical message: a low grade may settle with a metatarsal pad/offloading or a Weil osteotomy that indirectly relaxes the plate, whereas higher grades (true subluxation, crossover toe) need direct plantar plate repair combined with the Weil, and a fixed Grade 4 may need joint salvage rather than repair.
Red Flags Requiring Urgent Assessment
Seek alternative diagnosis if:
- Night pain or rest pain: Consider tumor, infection, complex regional pain syndrome
- Acute traumatic onset: Rule out Lisfranc injury, MT fracture, plantar plate rupture
- Constitutional symptoms: Fever, weight loss, malaise suggest infection or systemic disease
- Rapidly progressive deformity: May indicate inflammatory arthropathy, tumor
- Neurological symptoms: Widespread numbness, weakness suggest peripheral neuropathy or nerve compression
- Vascular insufficiency: Poor pulses, skin changes, ulceration require vascular assessment before any intervention
These features are atypical for simple mechanical metatarsalgia and require comprehensive workup.
Investigations
Imaging Protocol
Investigation Algorithm
Standard views: AP, lateral, oblique of foot. Must be WEIGHT-BEARING.
Assessment:
- MT length: Identify long second MT (Greek foot). Measure relative MT lengths using parabola method or direct measurement
- MT alignment: Check for MT elevation, depression, or rotation
- MTP joint space: Assess for arthropathy, erosions (RA), flattening (Freiberg's)
- First ray position: Hallux valgus angle, first MT elevation
- Sesamoid position: Lateral displacement with hallux valgus
Specific findings:
- Normal: Second MT typically 1-2mm shorter to equal length compared to first
- Pathologic: Second MT significantly longer than first (greater than 3mm predisposes to overload)
- Cavus foot: High calcaneal pitch angle (greater than 30 degrees)
Weight-bearing radiographs are essential initial investigation.
Indications:
- Positive drawer test (assess plantar plate tear)
- Suspected neuroma
- Rule out stress fracture
- Freiberg's disease staging
- Preoperative planning
Protocol: Foot MRI with dedicated coils. Sagittal, coronal, and axial images.
Plantar plate assessment (key finding):
- Normal: Low signal structure on all sequences, uniform thickness 1-2mm
- Partial tear: High signal on T2/STIR at insertion (usually lateral), thinning
- Complete rupture: Discontinuity, high signal, MTP joint subluxation
- Best seen on sagittal and coronal images
Other findings:
- Morton's neuroma: Low signal on T1/T2, between MT heads
- Stress fracture: Bone marrow edema, possible fracture line
- Freiberg's: MT head edema, fragmentation, subchondral changes
MRI is gold standard for soft tissue pathology assessment.
Advantages: Dynamic assessment, real-time, lower cost than MRI, no radiation
Uses:
- Morton's neuroma detection (hypoechoic mass between MT heads)
- Plantar plate tears (less sensitive than MRI)
- Guide injections
Limitations: Operator-dependent, less detailed than MRI for plantar plate
Ultrasound is useful but MRI preferred for comprehensive assessment.
Limited role in metatarsalgia assessment. Mainly for:
- Subtle MT fractures not visible on X-ray
- Lisfranc injury
- Freiberg's disease staging
Not routinely required for typical metatarsalgia.
Laboratory Studies
Generally not required for primary mechanical metatarsalgia.
Indicated if secondary cause suspected:
- Rheumatoid factor, anti-CCP: If bilateral MTP synovitis, systemic symptoms
- Uric acid: If acute monoarticular MTP pain (gout)
- ESR, CRP: If infection or inflammatory arthropathy suspected
- HbA1c: Diabetic patients with neuropathy or at-risk foot
Differential Diagnosis
- Pain Location
- Plantar MT head (specific MT)
- Key Clinical Features
- Plantar callus, drawer test positive if plate torn
- Diagnostic Test
- Clinical diagnosis, X-ray shows MT length
- Pain Location
- Web space (between MT heads)
- Key Clinical Features
- Burning, radiates to toes, Mulder's click
- Diagnostic Test
- Ultrasound or MRI shows neuroma
- Pain Location
- Dorsal and plantar second MT head
- Key Clinical Features
- Limited MTP motion, adolescent female
- Diagnostic Test
- X-ray shows MT head flattening, sclerosis
- Pain Location
- MT shaft (not plantar head)
- Key Clinical Features
- Acute onset, bony shaft tenderness
- Diagnostic Test
- MRI shows fracture line and edema
- Pain Location
- Multiple MTP joints bilaterally
- Key Clinical Features
- Systemic disease, synovitis, erosions
- Diagnostic Test
- Positive RF/anti-CCP, X-ray erosions
- Pain Location
- Under first MT head (sesamoids)
- Key Clinical Features
- Hallux pain, not lesser MTs
- Diagnostic Test
- X-ray/MRI shows sesamoid pathology
Key distinguishing features:
- Location of maximal tenderness is most helpful - MT head vs web space vs MT shaft
- Drawer test distinguishes plantar plate pathology (positive) from other causes
- Mulder's click is pathognomonic for Morton's neuroma
- Imaging confirms diagnosis when clinical examination unclear
Management
- 1
Clinical diagnosis of metatarsalgia (plantar MT head pain). Obtain weight-bearing X-rays to assess MT length and alignment. Proceed to conservative management trial for 3-6 months.
- 2
Conservative management includes metatarsal pad proximal to MT heads, stiff-soled shoes, and Achilles stretching. Approximately 80% of patients improve with conservative measures. If adequate relief achieved, continue conservative measures long-term. If symptoms persist, proceed to advanced options.
- 3
For persistent symptoms after 3-6 months conservative trial, obtain MRI to assess plantar plate integrity and rule out neuroma or stress fracture. Plan surgical approach based on MRI findings.
- 4
Surgical indications include failed conservative management, plantar plate tear, or structural abnormality. Perform Weil osteotomy (shorten MT 2-4mm) plus plantar plate repair if torn. Address first ray pathology if insufficiency is present.
Non-Operative Treatment
Conservative management is successful in approximately 80% of cases and should be the first-line approach for all patients with metatarsalgia.
Metatarsal pad or dome:
- Placed PROXIMAL to MT heads (not directly under)
- Typically 1cm proximal to point of maximal tenderness
- Redistributes load away from affected MT heads
- Can use adhesive gel pad or built into custom orthotic
Mechanism: Elevates MT shafts to transfer load proximally, unloading MT heads
Fitting: Must be precisely positioned - too distal is ineffective, too proximal is uncomfortable
Proper MT pad placement is the single most effective conservative intervention.
Stiff-soled shoes (rigid rocker sole):
- Reduces MTP joint dorsiflexion during toe-off
- Decreases load on MT heads
- Morton's extension or carbon fiber plate in shoe
Low heels (under 2-3cm):
- High heels transfer load anteriorly to forefoot
- Low heels maintain more even load distribution
Wide toe box:
- Accommodates any toe deformity
- Prevents lateral compression
Well-cushioned: Shock absorption reduces impact loading
Appropriate footwear is essential for load reduction.
Activity modification:
- Avoid prolonged standing when possible
- Reduce high-impact activities (running, jumping) during acute phase
- Swimming, cycling as alternative exercises
- NOT complete rest - maintain general fitness
Achilles stretching protocol:
- If Silfverskiold test positive (tight Achilles)
- Wall stretches: Knee straight (gastrocnemius), knee bent (soleus)
- Hold 30 seconds, repeat 3-5 times, perform 2-3 times daily
- Reduces forefoot loading by improving ankle dorsiflexion
Custom orthotics:
- Incorporate MT pad at correct position
- Arch support if first ray hypermobility or pes planus
- May include first MT cutout if first ray elevation
- Typically fabricated by podiatrist or orthotist
Taping:
- Plantar plate taping: Plantarflexes and supports toe
- Temporary measure, useful to assess if would benefit from orthotic
NSAIDs:
- Short-term use for acute flare-up
- Addresses MTP synovitis component
- Not curative, symptomatic only
Corticosteroid Injection
Indications: MTP synovitis with conservative failure. Use with caution.
Technique: Inject into MTP joint space (dorsal approach, avoid plantar plate). 1ml 40mg methylprednisolone plus 1ml local anesthetic.
Cautions:
- Can accelerate plantar plate degeneration
- May precipitate plantar plate rupture with repeated injections
- Maximum 2-3 injections per joint
- Avoid if drawer test already positive (plate already compromised)
Alternative: Consider if significant inflammatory component, but recognize risks.
Expected Conservative Outcomes
Success rate: 80% achieve adequate symptom control to avoid surgery
Timeframe: Expect gradual improvement over 3-6 months. Initial improvement within 4-6 weeks if will respond.
Factors predicting success:
- Mild symptoms
- Recent onset (under 6 months)
- Good compliance with offloading
- No structural deformity
- Negative drawer test
Failure predictors:
- Chronic symptoms (over 12 months)
- Positive drawer test (plantar plate rupture)
- Significant structural abnormality (long MT, severe first ray pathology)
- Crossover toe deformity
Adequate conservative trial (minimum 3-6 months) is essential before surgical consideration.
Complications
Transfer metatarsalgia occurs in 10-15% of patients after Weil osteotomy. Mechanism: Shortening one metatarsal reduces load on that MT but increases load on adjacent MTs. The third MT is most commonly affected after second MT osteotomy. Prevention is key: (1) Limit shortening to 2-4mm, (2) Consider cascade shortening of adjacent MTs if multiple need addressing, (3) Address first ray insufficiency so load doesn't transfer to lesser MTs, (4) Careful preoperative planning of relative MT lengths using weightbearing X-rays. Treatment: Conservative initially with MT pads and orthotics. If severe and refractory, may require adjacent MT osteotomy - but beware creating cascade of transfer issues.
Complications by Category
Intraoperative:
- Neurovascular injury: Digital nerve or vessel damage during dissection (under 5%). Prevention: careful dissection, identify structures
- Malposition of osteotomy: Incorrect angle causes dorsal or plantar step-off. Prevention: parallel to weightbearing surface
- Excessive shortening: Greater than 4mm increases transfer risk. Prevention: measure and plan carefully
- Inadequate fixation: Screw strips or K-wire bends. Prevention: proper technique, appropriate size implants
Early postoperative (under 6 weeks):
- Infection: Under 2% (typically superficial). Management: antibiotics, wound care
- Hematoma: Collection causing painful swelling. Management: usually resolves, aspiration if large
- Wound dehiscence: Poor healing (diabetes, smoking). Management: local wound care, rarely revision
- Fixation failure: Screw loosening, displacement. Management: may need revision fixation if symptomatic
Late complications (over 6 weeks):
- Delayed union: Visible on X-ray at 3-6 months. Usually asymptomatic and progresses to union
- Nonunion: Persistent gap, no bridging callus. Rate under 5%. May need revision if painful
- Malunion: Heals in abnormal position. Can cause persistent pain or deformity
- Hardware prominence: Screw head palpable. May need removal if symptomatic
- Complex regional pain syndrome: Rare. Disproportionate pain, swelling, vasomotor changes
Recognition and appropriate management of these complications is essential for optimal outcomes.
Minimizing Complications
Preoperative:
- Careful patient selection
- Adequate conservative trial
- Realistic expectation setting
- Address all contributing pathology (first ray, Achilles)
Intraoperative:
- Precise osteotomy technique
- Appropriate shortening amount (2-4mm typically)
- Consider cascade shortening
- Solid fixation
- Capsular repair
Postoperative:
- Toe plantarflexion strapping
- Early appropriate mobilization
- Physiotherapy for range of motion
- Patient education and compliance
Guidelines, Registries & Global Practice
Metatarsalgia is a worldwide forefoot complaint with no single dedicated national-society guideline; practice is driven by foot-and-ankle literature and the closely related conditions of hallux valgus and lesser-toe instability. The principles below are consistent across UK (BOFAS/BOA), US (AAOS/AOFAS), European (EFAS/EFORT) and AO Foundation teaching.
Global Epidemiology
- Evidence
- Hallux valgus - a major driver of first-ray insufficiency and lesser-MT overload - has a pooled prevalence of 23% in adults aged 18-65 and 36% in adults over 65 (systematic review/meta-analysis)
- Source
- Nix 2010 (J Foot Ankle Res), PMID 20868524
- Evidence
- Hallux valgus and related forefoot deformity are markedly more common in women than men, consistent with the female predominance seen in metatarsalgia and crossover toe
- Source
- Nix 2010, PMID 20868524
- Evidence
- The second MTP joint is the most commonly affected by plantar plate failure (63% in a prospective surgical series)
- Source
- Nery 2012 (Foot Ankle Int), PMID 22735202
Guidance and Consensus, Side by Side
- Position
- Identify and treat the specific cause; staged grade-matched plantar plate protocol (shrinkage / direct repair / tendon transfer) combined with Weil osteotomy
- Evidence basis
- Level IV-V (expert review and prospective series): Espinosa 2008, Nery 2014
- Position
- Exhaust structured non-operative care (offloading orthoses, rocker/stiff sole, footwear advice) before surgery; reserve osteotomy for refractory mechanical overload
- Evidence basis
- Consensus / Level V - aligned with 80% non-operative success in reviews
- Position
- Distal oblique (Weil) osteotomy is the best-evaluated lesser-MT osteotomy; limit shortening and consider cascade balancing to minimise transfer metatarsalgia and floating toe
- Evidence basis
- Level III: Trnka 1999 (Weil superior to Helal); Highlander 2011 (complication profile)
Registry & Pooled Evidence
No national joint registry captures lesser-metatarsal osteotomy (registries focus on arthroplasty). The best population-level evidence is therefore pooled review data: across 1131 Weil osteotomies, floating toe occurred in 36%, recurrence in 15%, transfer metatarsalgia in 7%, and delayed/non-/malunion in 3% (Highlander 2011, PMID 21490179). These figures should frame consent worldwide.
Practice Variation
First-line conservative management (metatarsal pad placed proximal to the heads, stiff/rocker sole, footwear modification, Achilles stretching) is universal, succeeding in around 80% of cases. Threshold for surgery varies by health system and access to podiatry/orthotics rather than by any difference in the underlying evidence.
The Weil osteotomy is the global default for refractory mechanical overload. Minimally invasive distal metatarsal metaphyseal osteotomy (DMMO) is increasingly used in some European centres but has a recognised learning curve. Choice is largely surgeon- and resource-dependent, not guideline-mandated.
Consent and Documentation (Universal Principles)
- Document an adequate conservative trial (3-6 months of specific offloading and footwear measures) before offering surgery - inadequate trial is a recurrent source of dissatisfaction and litigation.
- Quantify complication risk at consent: floating toe (reported up to 36% in pooled data), transfer metatarsalgia (7-15%), expected MTP stiffness (10-20 degrees), and the possibility of further surgery.
- Record the planned and achieved shortening (target 2-4mm); excessive shortening is the principal avoidable cause of transfer metatarsalgia.
- Assess and document first ray pathology (hallux valgus, hypermobility) and whether it was addressed - failure to do so is a common cause of recurrence.
MCQ Practice Points
Q: What is the most common cause of metatarsalgia related to hallux valgus correction?
A: Transfer metatarsalgia - excessive shortening or elevation of first ray transfers load to lesser metatarsals. Occurs after over-aggressive first MT shortening, dorsal malunion, or first MTP fusion in excessive dorsiflexion. Prevention: Maintain first ray length and plantar position. Treatment: Metatarsal osteotomy to offload affected rays.
Q: What is the Weil osteotomy and its indication?
A: Oblique distal metatarsal head osteotomy cut roughly parallel to the weightbearing surface (from dorsal-distal to plantar-proximal) for metatarsalgia with a relatively long metatarsal. The head fragment slides proximally to shorten the metatarsal with inherent stability. Fix with 1-2 screws. Indicated for intractable metatarsalgia, subluxed/dislocated MTP joint, and crossover toe deformity.
Q: What is the clinical significance of plantar plate tears in metatarsalgia?
A: Plantar plate attenuation/tear causes MTP joint instability leading to hammer toe, crossover toe, and metatarsalgia. Drawer test positive (greater than 2mm dorsal translation or greater than 50% compared to contralateral). MRI shows plantar plate disruption. Treatment: Direct plantar plate repair through dorsal approach + Weil osteotomy. Grade II-III tears require repair.
Q: How do you differentiate Morton's neuroma from primary metatarsalgia?
A: Morton's neuroma: Burning, electrical pain in 3rd webspace (sometimes 2nd), Mulder's click positive, sensory changes in adjacent toes, pain relieved by removing shoes. Primary metatarsalgia: Aching pain under metatarsal heads, callus formation, worsened by weightbearing. Morton's: Webspace injection diagnostic and therapeutic; metatarsalgia: Offloading insoles first-line.
Q: What is the relative metatarsal length formula and its clinical relevance?
A: Ideal formula: first metatarsal longest, then decreasing 2, 3, 4, 5 (or first equals second). Abnormally long 2nd metatarsal predisposes to metatarsalgia under 2nd MT head. Index-minus foot (short first MT) transfers stress to lesser metatarsals. Relative overlength guides which metatarsals require shortening osteotomy.
At a Glance
Metatarsalgia is forefoot pain under the metatarsal heads, with the second metatarsal most commonly affected due to its length and rigid Lisfranc articulation. Plantar plate pathology (degeneration or rupture) is a common underlying cause, assessed by the drawer test which demonstrates excessive dorsal toe translation. Primary causes include long second MT (Greek foot), first ray insufficiency, and Achilles tightness. Conservative management (metatarsal pad placed PROXIMAL to MT heads, stiff-soled shoes) is successful in 80%. Surgical options include Weil osteotomy (shortening 2-4mm) with risks of transfer metatarsalgia (10-15%) and floating toe (15-30%).
PLANTARPrimary Causes of Metatarsalgia
Hook:PLANTAR causes make the PLANTAR surface of the forefoot hurt! Remember to examine for all seven causes.
DRAWERDrawer Test for Plantar Plate
Hook:DRAWER test opens the drawer to check the plantar plate integrity - essential examination for every metatarsalgia case!
PADSConservative Management Steps
Hook:PADS offload the metatarsal heads and allow healing in 80% of cases!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old woman presents with 6 months of right forefoot pain under the ball of her foot, worse with prolonged standing and wearing heels. She points to the area under her second metatarsal head. Examination shows plantar tenderness under the second MT head, and you perform a drawer test which shows some increased translation compared to the other toes. How do you approach this patient?”
“A 60-year-old woman presents with progressive second toe deformity - the toe is now drifting medially over her hallux. She has pain under the second metatarsal head. On examination, the second toe is deviated medially and when you perform a drawer test, the toe subluxates dorsally very easily. How do you manage this patient?”
“You see a 52-year-old patient in clinic who underwent Weil osteotomy of the second metatarsal 6 months ago for metatarsalgia. The second MT pain has resolved, but she now has significant pain under the third metatarsal head that wasn't present before surgery. Weight-bearing X-rays show the second MT has been shortened by approximately 6mm. What has happened and how do you manage this complication?”
Key Anatomy
- Second MT: Longest (60% population), most fixed at Lisfranc joint, most commonly affected (65-70%)
- Plantar plate: Fibrocartilaginous structure 1-2mm thick, stabilizes MTP joint, prevents dorsal subluxation
- First ray: Should bear 50% of forefoot load - if insufficient, transfers to second MT
- Load distribution: 1st ray 50%, 2nd MT 15-20%, 3rd MT 10-15%, 4th and 5th MT 5-10% each
Clinical Diagnosis
- Pain: Plantar MT head (patient can point to specific MT), worse with standing/walking
- Drawer test: Dorsally translate toe on MT head - positive if excessive translation (plantar plate tear)
- Crossover toe: Second toe drifts medially over hallux - indicates plantar plate rupture
- First ray exam: Check for hallux valgus, hypermobility, prior surgery (causes second MT overload)
- Achilles tightness: Silfverskiold test - increases forefoot loading if positive
Causes (PLANTAR)
- P - Plantar plate pathology (tear causes crossover toe, positive drawer)
- L - Long second MT (Greek/Morton's foot - mechanical overload)
- A - Achilles tightness (increases forefoot loading)
- N - Neuroma Morton's (web space pain - differential)
- T - Transfer lesion (after HV surgery, first MT osteotomy)
- A - Arthritis (RA, Freiberg's disease - secondary causes)
- R - Rigid cavus foot (fixed forefoot equinus)
Conservative Management (PADS) - 80% Success
- P - Pad placement PROXIMAL to MT heads (1cm proximal to pain point)
- A - Activity modification (avoid standing, walking, heels)
- D - Dense-soled (stiff) shoes reduce MTP bending
- S - Stretching Achilles tendon if tight
- Trial 3-6 months before considering surgery
Weil Osteotomy Technique
- Indication: Failed 3-6 months conservative, structural abnormality
- Approach: Dorsal longitudinal incision between extensor tendons
- Osteotomy: Oblique cut parallel to weightbearing surface (25-30 degrees to shaft)
- Shortening: 2-4mm (6mm or more is excessive - high transfer risk)
- Fixation: 2.0-2.4mm screw dorsal distal to plantar proximal
- Concurrent: Plantar plate repair if drawer positive, address first ray if HV/hypermobility
Complications
- Transfer metatarsalgia: 10-15% (load shifts to adjacent MT from excessive shortening)
- Floating toe: 15-30% (toe loses ground contact - usually not functionally limiting)
- MTP stiffness: 20-40% (10-20 degree dorsiflexion loss - expected)
- Recurrent pain: 5-10% (inadequate shortening, plate not addressed)
- Prevention: Limit shortening 2-4mm, cascade planning, address first ray, plate repair if torn
Evidence Base and Key Trials
Current Concept Review: Metatarsalgia
- Metatarsalgia is a symptom, not a diagnosis - the underlying cause must be identified
- Primary metatarsalgia arises from intrinsic anatomic factors (long lesser metatarsal, plantarflexed metatarsal, first ray insufficiency)
- Secondary metatarsalgia is driven by systemic or local pathology (RA, Freiberg's disease, interdigital neuroma)
- Iatrogenic (transfer) metatarsalgia follows first ray surgery that alters load distribution
- Treatment must be directed at the specific mechanical or pathologic cause, not just the symptom
Complications of the Weil Osteotomy
- Literature review pooling 1131 Weil osteotomies from 17 studies
- Floating toe was the most common complication - reported in 233 cases, overall occurrence 36%
- Recurrence of deformity/symptoms reported in 15% of cases
- Transfer metatarsalgia reported in 7% of cases
- Delayed union, non-union and malunion collectively reported in 3% of cases
Lesser MTP Instability: Prospective Evaluation and Repair of Plantar Plate and Capsular Insufficiency
- 22 patients (40 MTP joints) treated by direct plantar plate repair through a dorsal approach combined with Weil osteotomy
- The second MTP joint was the most commonly affected (63%); Grade III tears were the most frequent type
- Mean AOFAS score improved from 52 preoperatively to 92 postoperatively
- Direct anatomic repair corrected medial/dorsal/dorsomedial toe deviation and restored MTP alignment
- Plain radiographs, MRI and MTP arthroscopy were correlated with the anatomic grading of the tear
Comparison of Weil and Helal Osteotomies for Metatarsalgia Secondary to Lesser MTP Dislocation
- 30 patients (47 metatarsals) compared - 15 Weil osteotomy vs 15 Helal osteotomy
- Transfer lesions: 0% after Weil vs 41% after Helal (significant)
- Recurrent metatarsalgia: 0% after Weil vs 27% after Helal
- Radiographic reduction maintained in 84% of Weil vs 36% of Helal joints
- No malunion or pseudarthrosis in the Weil group; 5 malunions and 3 pseudarthroses with Helal
Prospective Evaluation of a Protocol for Surgical Treatment of Lesser MTP Plantar Plate Tears
- 68 patients (100 MTP joints) graded by the anatomic plantar plate tear classification and treated by a grade-matched protocol
- Grades 0-I: thermal shrinkage; Grades II-III: direct reinsertion; Grade IV: flexor-to-extensor transfer - all combined with a Weil osteotomy
- All grades improved significantly in VAS and AOFAS scores after surgery (P less than .0001)
- Grade IV tears had the poorest outcome (fair AOFAS average of 72 points)
- Grades I, III and IV had less stable joints and poorer toe purchase/ground touch than grades 0 and II