Control | Correct | Compensate | Protect
- Functions: Control (motion), Correct (deformity), Compensate (weakness), Protect (healing)
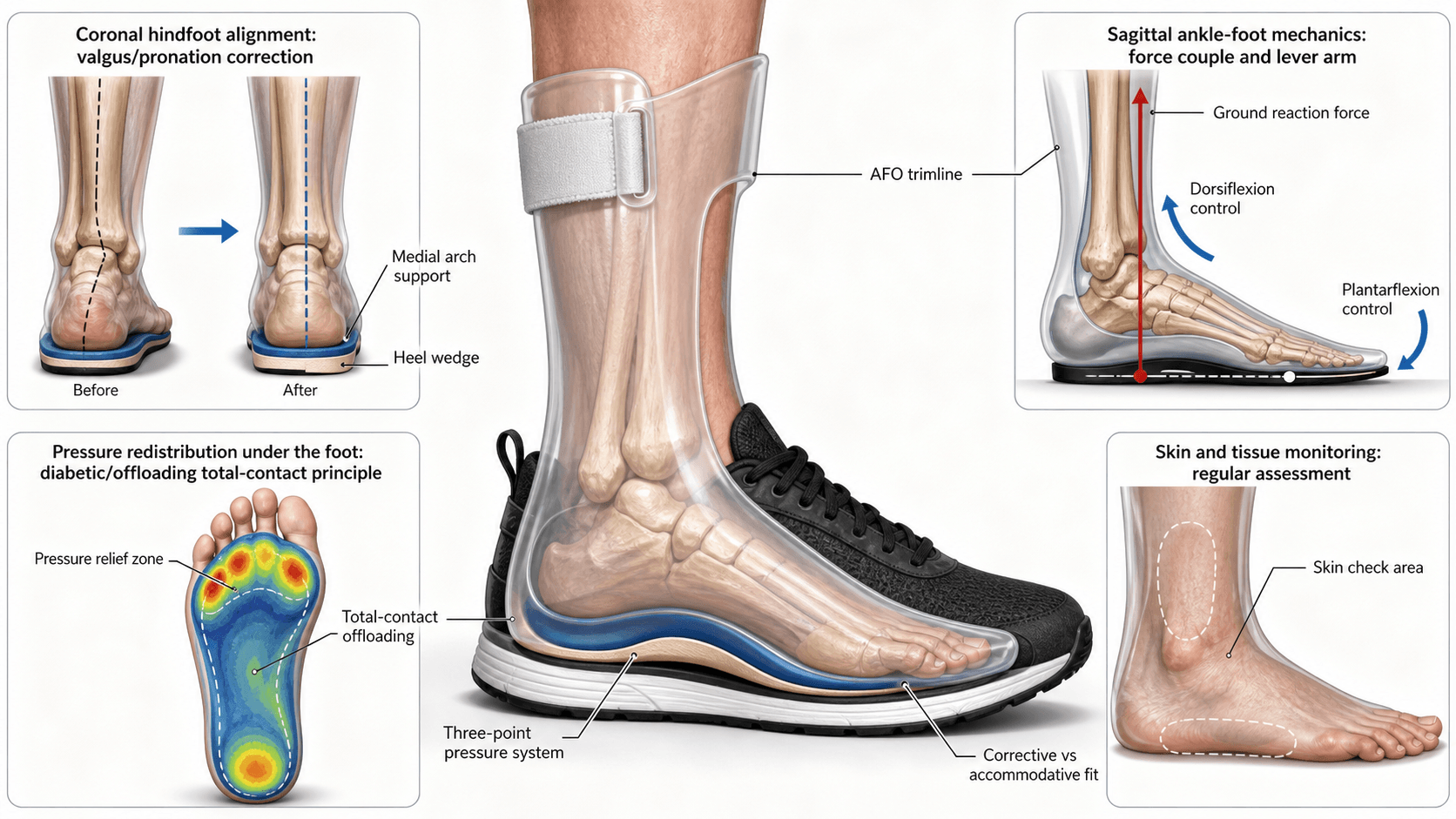
- Three-point pressure = biomechanical basis of all corrective orthoses
- AFO types: Solid (blocks motion), Hinged (allows DF), Ground-reaction (extends knee)
- FRAFO = Floor Reaction AFO - uses ground reaction force to extend knee
- Spinal orthoses named by levels covered (LSO, TLSO, CTLSO)
- “Solid AFO for spastic equinus (blocks plantarflexion)
- “Hinged AFO allows tibial progression in stance (better gait)
- “Ground-reaction AFO for crouch gait (knee extension moment)
- “TLSO for thoracolumbar fractures (T9-L3 coverage)
- “Halo vest = only reliable cervical immobilization (greater than 90%)
Foundation of all corrective orthoses. Central corrective force opposed by two counter-forces creates moment arm. Longer lever arm = greater mechanical advantage. Pressure must be distributed over large area to avoid skin breakdown.
Solid AFO: Blocks all motion - for spasticity, severe instability. Hinged AFO: Allows dorsiflexion - for weak dorsiflexors with intact plantarflexors. Ground-reaction: Creates knee extension - for crouch gait, quad weakness.
TLSO controls T9 to L3 motion effectively. Above T9 requires CTLSO (sternal and clavicular support). Below L3 requires thigh extension for pelvic control. Upper cervical requires halo vest.
Prescription must specify: Diagnosis, joints to control, motion to allow/block, corrective forces needed, material (plastic, metal, carbon fiber), footwear requirements.
4 CsFunctions of Orthoses
Hook:4 Cs = Control, Correct, Compensate, Protect - the four functions of every orthosis!
Overview
Orthoses are externally applied devices used to control, correct, compensate for, or protect musculoskeletal dysfunction. Understanding orthotic prescription is essential for orthopaedic surgeons managing neurological conditions, fractures, deformity correction, and rehabilitation. The fundamental biomechanical principle underlying corrective orthoses is three-point pressure - a central corrective force opposed by two counter-forces creating a moment for correction. Orthoses are named systematically by the joints they cross (AFO, KAFO, TLSO) following ISO 8549 nomenclature. AFO selection depends on the specific gait abnormality: solid AFO blocks spastic plantarflexion, hinged AFO allows controlled dorsiflexion while preventing foot drop, and ground-reaction AFO creates a knee extension moment for crouch gait. Spinal orthoses provide varying degrees of motion restriction based on their extent - LSO controls lumbosacral motion, TLSO extends to thoracolumbar junction, and halo vest provides the most reliable cervical immobilization.
Nomenclature and Classification
ISO 8549 Nomenclature
The International Organization for Standardization (ISO) established a systematic naming convention for orthoses based on the anatomical region and joints crossed.
- FO (Foot Orthosis): Insoles, arch supports, metatarsal pads
- AFO (Ankle-Foot Orthosis): Crosses ankle joint, controls foot position
- KAFO (Knee-Ankle-Foot Orthosis): Extends from thigh to foot, controls knee
- HKAFO (Hip-Knee-Ankle-Foot Orthosis): Includes hip joint control
- KO (Knee Orthosis): Braces for knee instability, unloading
- WHO (Wrist-Hand Orthosis): Wrist splints, resting hand orthoses
- EWHO (Elbow-Wrist-Hand Orthosis): Extends to elbow
- SEWHO (Shoulder-Elbow-Wrist-Hand Orthosis): Full upper limb
- CO (Cervical Orthosis): Soft/rigid collars
- CTO (Cervicothoracic Orthosis): Extends to upper thorax
- CTLSO (Cervicothoracolumbosacral Orthosis): Full spine control
- TLSO (Thoracolumbosacral Orthosis): Thoracolumbar control
- LSO (Lumbosacral Orthosis): Lower lumbar and sacral control
Functional Classification
Orthosis Classification by Function
Material Classification
- Polypropylene: Most common, heat-moldable, durable
- Low-temperature plastics: Custom-molded at lower temperatures
- Carbon fiber composites: Lightweight, energy-storing (athletic use)
- Aluminum: Lightweight, adjustable
- Steel: Heavy-duty, adjustable, traditional KAFOs
- Titanium: Lightweight, strong (specialty applications)
- Neoprene: Compression, warmth, proprioceptive feedback
- Foam: Padding, pressure distribution
- Leather: Traditional, breathable, adjustable
Principles of Orthotic Biomechanics
Three-Point Pressure System
The three-point pressure principle is the fundamental biomechanical concept underlying all corrective orthoses. It creates a bending moment to correct or control deformity.
- Central corrective force: Applied at apex of deformity
- Two counter-forces: Applied proximal and distal to central force
- Moment arm: Distance between forces determines mechanical advantage
- Longer lever arms = greater mechanical advantage
- Force distribution over large surface area prevents pressure ulcers
- Soft tissue tolerance limits maximum corrective force
- TLSO for scoliosis: Lateral pad at curve apex, counter-pads at iliac crest and axilla
- AFO for equinus: Posterior force at calf, anterior force at tibial crest, foot plate
- Knee orthosis for valgus: Lateral force at knee, medial forces at thigh and calf
Ground Reaction Force Manipulation
Floor Reaction AFO (FRAFO) and ground-reaction orthoses manipulate the ground reaction force vector relative to joint centers.
- Ground reaction force (GRF) passes through centre of pressure
- If GRF passes anterior to knee = knee extension moment
- If GRF passes posterior to knee = knee flexion moment
- FRAFO positions GRF anterior to knee, extending the knee in stance
- Crouch gait = excessive knee flexion in stance (common in cerebral palsy)
- Weak quadriceps cannot maintain knee extension
- FRAFO blocks ankle dorsiflexion, moves GRF anterior
- External knee extension moment compensates for weak quads
Lever Arm Considerations
- KAFO controls knee better than short KO
- Full-length thigh cuff provides better rotational control
- Trade-off: Increased weight, reduced function
- Supramalleolar AFO (SMAFO) allows more tibial motion
- Short KAFOs allow easier sitting
- Trade-off: Less control of proximal joints
SHGFAFO Selection Guide
Hook:SHGF = Solid, Hinged, Ground-reaction, FRAFO - know which AFO for which gait problem!
Ankle-Foot Orthoses (AFOs)
Solid Ankle AFO
- Rigid plastic shell from below knee to toes
- Blocks all ankle motion (dorsiflexion and plantarflexion)
- Foot plate extends to metatarsal heads (or toes for spasticity)
- Prevents ankle plantarflexion in swing (clears foot)
- Prevents ankle dorsiflexion in stance (may limit tibial progression)
- Provides mediolateral ankle stability
- Spastic equinus (cerebral palsy, stroke, TBI)
- Severe ankle instability
- Complete foot drop with spasticity
- Fixed equinus contracture (blocks further progression)
- Intact plantarflexors (blocks push-off power)
- Patients requiring squat or stair climbing
- Skin breakdown risk at calf/anterior tibia
- Blocks tibial progression in stance (short step length)
- Reduces push-off power (no plantarflexion for propulsion)
- Compensatory knee hyperextension in mid-stance
Knee-Ankle-Foot Orthoses (KAFOs)
Indications for KAFO
- Quadriceps weakness (polio, muscular dystrophy, SCI)
- Ligamentous instability with neurological impairment
- Knee hyperextension with sensation loss
- Combined quadriceps and dorsiflexor weakness
- Flail limb (complete paralysis below knee)
- Myelomeningocele with high-level paralysis
- Knee flexion contracture (serial casting with KAFO)
- Genu varum/valgum with weakness
- Post-surgical protection
KAFO Components
- Thigh cuff or full-contact thigh shell
- Length determines rotational control
- Medial/lateral uprights connect to knee joint
- Locked knee: Maximum stability, swing-through gait
- Drop-lock: Manual unlock for sitting, locks automatically
- Offset knee joint: Provides hyperextension stability
- Polycentric knee: More anatomical motion
- Stance-control (SCKAFO): Locks in stance, free in swing
- Usually solid ankle or locked dorsiflexion
- May include adjustable ankle joints
- Stirrup connects to shoe or molded foot section
Stance-Control KAFO (SCKAFO)
- Knee joint locks automatically during stance phase
- Unlocks during swing phase for normal knee flexion
- Combines stability with more natural gait pattern
- Weight-activated locking (extends with axial load)
- Ankle-motion triggered (ankle DF triggers knee lock)
- Electronic control (sensors detect gait phase)
- Improved gait pattern (knee flexion in swing)
- Increased walking velocity (consistently demonstrated)
- Better stair climbing and sitting
- Improved cosmesis and patient acceptance
Evidence caveat: While faster, more natural gait is well supported, a reduction in metabolic energy cost compared with locked KAFOs is NOT consistently shown (Davis 2010).
Spinal Orthoses
Cervical Orthoses
- Foam collar, minimal motion restriction
- Proprioceptive reminder, comfort, warmth
- Indications: Whiplash, minor strain, psychological support
- Does NOT immobilize - do not use for unstable injuries
- Two-piece (anterior/posterior) rigid plastic
- Restricts 70-80% flexion/extension, 50% rotation
- Indications: Stable cervical fractures, post-operative, transport
- Does NOT adequately immobilize C0-C2 or C7-T1
- Collar with thoracic extension (sternal and posterior plates)
- Improved control of lower cervical spine (C5-T1)
- Indications: Lower cervical fractures, post-fusion
- Examples: SOMI brace, Minerva orthosis
- Ring fixed to skull with 4 pins, connected to vest
- Most restrictive cervical orthosis available
- Restricts greater than 90% of cervical motion
- Indications: Unstable cervical fractures, C1-C2 injuries, post-odontoid fixation
- Complications: Pin site infection (20%), pin loosening, respiratory compromise
- Flex/Ext
- 5-10%
- Lateral Bend
- 5%
- Rotation
- 5%
- Flex/Ext
- 70-80%
- Lateral Bend
- 50%
- Rotation
- 50%
- Flex/Ext
- 80-90%
- Lateral Bend
- 60%
- Rotation
- 60%
- Flex/Ext
- greater than 95%
- Lateral Bend
- greater than 95%
- Rotation
- greater than 95%
CHT LSSpinal Orthosis Levels
Hook:CHT LS = Collar, Halo, TLSO, LSO, Scoliosis - know which orthosis for which spinal level!
Differential Selection: Matching the Device to the Problem
A frequent exam trap is prescribing the wrong device for a presentation that "looks like foot drop" or "looks like a crouch". The table below contrasts presentations that are easily confused and the discriminating feature that drives device choice.
- discriminator
- Swing-phase only deficit, normal push-off
- device
- Hinged AFO / posterior leaf spring
- wrongChoice
- Solid AFO (loses push-off)
- discriminator
- Stance-phase equinus thrust, high tone (MAS 3-4)
- device
- Solid AFO
- wrongChoice
- Hinged AFO (hinge is overpowered)
- discriminator
- Excess knee flexion in stance, GRF posterior to knee
- device
- Ground-reaction / floor-reaction AFO
- wrongChoice
- Hinged AFO (allows DF, worsens crouch)
- discriminator
- Correctable deformity, normal ankle dorsiflexors
- device
- UCBL or SMO
- wrongChoice
- Solid AFO (over-treats, blocks ankle)
- discriminator
- No posterior tension-band injury, no deficit
- device
- TLSO or early mobilization
- wrongChoice
- Jewett brace (flexion control only)
- discriminator
- Disruption above C2, poorly controlled by collars
- device
- Halo vest or surgical fixation
- wrongChoice
- Rigid collar (inadequate immobilization)
Clinical Relevance: Condition-Specific Prescriptions
Neurological Conditions
- Flaccid phase: Hinged AFO (prevent foot drop, allow DF)
- Spastic phase: Solid AFO if equinus, hinged if mild spasticity
- Consider tone-reducing features (contoured footplate)
- Upper limb: Resting hand splint to prevent contracture
- Spastic diplegia: Ground-reaction AFO for crouch gait
- Spastic hemiplegia: Solid or hinged AFO depending on tone
- Equinus: Solid AFO, consider serial casting first
- KAFO rarely tolerated (high energy cost, poor acceptance)
- Flaccid weakness pattern
- AFO if ankle dorsiflexors weak
- KAFO if quadriceps weak (locked or stance-control)
- Lightweight materials preferred (carbon fiber, aluminum)
- Complete paraplegia: RGO (Reciprocating Gait Orthosis) for therapeutic standing/walking
- Incomplete injury: AFO or KAFO based on muscle power
- High energy cost limits practical ambulation
Fractures
- PTB cast or PTB AFO for protected weight-bearing
- Functional brace (Sarmiento) after initial healing
- Allow knee and ankle motion while protecting tibia
- CAM walker (Controlled Ankle Motion) boot
- Allows protected weight-bearing
- Removable for wound care and physiotherapy
- TLSO for stable burst or compression fractures
- Duration: 8-12 weeks typically
- Custom-molded for unstable patterns
- Jewett brace for anterior column only
- Halo vest for unstable C1-C2 injuries
- Rigid collar for stable subaxial injuries
- Duration: 8-12 weeks for halo
Paediatric Conditions
- Pavlik harness (0-6 months): Hip flexion and abduction
- Abduction orthosis (after Pavlik): Maintain hip position
- Not for exam focus but understand principles
- Denis Browne boots and bar (Ponseti protocol)
- Boots set in external rotation and dorsiflexion
- Maintains correction achieved by casting
- Wear 23 hours/day for 3 months, then night-time
- KAFO with valgus force at knee
- Theoretical benefit in infantile Blount (less than 3 years)
- Limited evidence for efficacy
Orthosis-Tissue Interface: Pressure Tolerance and Skin Protection
Every corrective force an orthosis applies must ultimately be transmitted through skin and soft tissue. Because pressure equals force divided by area, the single most important protective principle is to spread each force over the largest tolerant surface possible and to keep it off bony prominences. Sustained interface pressure that exceeds the skin's capillary perfusion pressure (classically around 32 mmHg at the arteriolar end, the Landis value) causes local ischaemia; if unrelieved this progresses to a pressure ulcer. This is why the topic's recurring warnings about "force distribution" and "skin checks" are not incidental - they are the rate-limiting constraint on how much correction a device can safely deliver.
- Ankle-foot orthoses: medial and lateral malleoli, tibial crest, navicular tuberosity, base of the fifth metatarsal, and the fibular neck, where a poorly contoured proximal trimline or KAFO upright can compress the common peroneal nerve and cause an iatrogenic foot drop.
- KAFOs: femoral condyles, patella, and the proximal thigh cuff.
- Spinal orthoses: iliac crests, anterior superior iliac spines, sternum and pubis (the Jewett three-point pads), and the sacrum.
- Total-contact fitting deliberately maximises contact area so that no single point carries a disproportionate load - the same principle underlying the total-contact cast for the neuropathic foot.
- Insensate skin is the danger case. Patients with diabetic neuropathy, spinal cord injury or spina bifida cannot feel a developing sore, so relief must be engineered into the device and reviewed by inspection, not by symptoms.
- Shear and friction compound direct pressure; a device that pistons or migrates is as dangerous as one that is too tight.
- The practical bedside test is the skin check on removal: blanchable erythema that fades within a few minutes is acceptable, whereas non-blanching erythema persisting beyond 20 to 30 minutes signals excessive local pressure and mandates modification before further wear.
Q: A patient returns two weeks after a new solid AFO with a fixed red mark over the lateral malleolus that does not fade. What does this mean and what do you do? A: Persistent non-blanching erythema over a bony prominence is an impending pressure ulcer - the interface pressure there is exceeding capillary perfusion. Stop wearing the device, inspect for skin breakdown, and return it to the orthotist for relief/padding or re-moulding over the malleolus. Re-examine the fit, trimlines and any pistoning, and be especially vigilant in neuropathic or insensate patients, who will not report the warning discomfort.
Metabolic Energy Cost of Braced Gait
A biomechanically perfect orthosis is useless if the patient will not wear it, and the commonest reason a technically sound brace is abandoned is that walking in it costs too much energy. Energy cost is therefore a core prescription principle, not an afterthought - it explains several statements made elsewhere in this topic (KAFOs being "rarely tolerated" in cerebral palsy, the "high energy cost" that limits practical ambulation after spinal cord injury, and why lightweight carbon-fibre or aluminium components are preferred).
- The more proximal and the more locked the device, the higher the demand. A locked-knee KAFO forces energy-expensive compensations - hip-hitching, circumduction and vaulting - to clear a stiff limb in swing.
- Reciprocating gait orthoses and bilateral KAFOs for thoracic-level paraplegia impose an energy cost so high that most adult users ultimately choose a wheelchair for community distances, reserving the orthosis for therapeutic standing.
- The corollary drives material choice: every gram matters, so carbon-fibre and aluminium are favoured where weight, not durability, is the limiting factor.
- The Physiological Cost Index (PCI) - walking heart rate minus resting heart rate, divided by walking speed - is the common clinic surrogate for oxygen cost when formal calorimetry is unavailable.
- Interpreting device studies through this lens resolves an apparent paradox: stance-control KAFOs reliably increase walking velocity by allowing free knee flexion in swing, yet do not consistently reduce the metabolic cost or PCI of walking compared with a locked KAFO (Davis 2010, verified below). The defensible benefits of an SCKAFO are faster, more natural gait and easier sitting and stair use - not guaranteed energy saving.
- Practically, a device should be prescribed only when the resulting gait cost falls within the patient's cardiopulmonary reserve; otherwise a lighter device, a less restrictive joint, or a wheeled alternative is the honest recommendation.
Q: A young adult with thoracic-level paraplegia has well-fitted KAFOs but uses a wheelchair for everything except therapy. Has the orthosis failed? A: Not biomechanically - it provides the standing stability it was designed for. It has failed the energy-cost test: braced ambulation at this level carries a very high metabolic demand, so the wheelchair is the rational choice for community mobility while the KAFOs retain value for therapeutic standing (bone loading, pressure relief, psychological and physiological benefits). Recognising energy cost as a legitimate prescription endpoint - and choosing the lightest adequate device - is the mature answer.
Guidelines, Registries & Global Practice
Global Epidemiology of Orthotic Need
The major drivers of orthotic demand are common worldwide: stroke (around 12 million new strokes/year, the leading cause of acquired adult foot drop), cerebral palsy (roughly 2 per 1,000 live births, the most common cause of childhood physical disability), diabetic neuropathy and Charcot foot (rising with the global diabetes burden), adolescent idiopathic scoliosis (around 2-3% of adolescents, around 10% of whom need treatment), and osteoporotic and traumatic spinal fractures. Need outstrips supply: the WHO estimates only around 1 in 10 people who need assistive products, including orthoses, currently have access, with the largest gaps in low- and middle-income countries.
Side-by-Side Guidance
- Domain
- AIS bracing
- Key position
- Brace skeletally immature curves around 25-40 degrees (Risser low); target wear time and in-brace correction drive success
- Domain
- Paediatric / CP orthotics
- Key position
- AFO selection matched to gait deviation; bracing as part of multilevel CP management
- Domain
- Stroke rehab, spinal trauma
- Key position
- Offer AFO for persistent foot drop affecting gait; mobilize stable thoracolumbar fractures, brace selectively
- Domain
- Thoracolumbar fractures
- Key position
- Stable AO-A injuries (intact PLC, no deficit) suit non-operative care; bracing optional given equivalence data
- Domain
- Fracture orthotics
- Key position
- Functional bracing principles (Sarmiento) for selected diaphyseal fractures
A recurring theme is convergence on biomechanics with divergence on whether to brace at all for stable spinal injuries, reflecting the Bailey equivalence data.
Standards and Registry Notes
- Orthosis nomenclature follows ISO 8549; device terminology and classification follow ISO 22523. These are the global reference standards regardless of country.
- Most orthoses are regulated as low-risk (Class I) medical devices by national regulators (e.g. FDA in the US, MHRA/UKCA in the UK, CE marking in the EU, TGA in Australia).
- Unlike arthroplasty, orthoses have no large international outcome registry; the evidence base rests on RCTs (BrAIST, Bailey) and gait-laboratory studies rather than registry survival data.
High- versus Limited-Resource Practice
- High-resource settings: custom thermoplastic and carbon-fibre devices, instrumented 3D gait analysis to guide AFO/GRAFO prescription, certified orthotists embedded in MDT clinics, and 3D-printed custom orthoses emerging.
- Limited-resource settings: reliance on prefabricated or locally fabricated devices, limited orthotist availability, and greater use of early mobilization without bracing - directly supported by the Bailey trial showing equivalence of "no orthosis" for stable burst fractures. WHO's GATE initiative promotes a priority assistive products list to widen access.
Controversies & Areas of Uncertainty
The Bailey RCT showed TLSO is equivalent to no orthosis for neurologically intact AO-A3 fractures with an intact PLC. Many surgeons still brace for comfort or where PLC integrity is uncertain. The genuine uncertainty is patient selection, not the biomechanics.
Meta-analyses disagree: a broad analysis (Choo 2021) shows clear speed/ambulation gains, while an RCT-only analysis (Shahabi 2019) found low-quality, non-significant effects on walking speed. Optimal AFO type for a given patient remains unresolved.
Effectiveness is debated. Only around half of children respond; gait-analysis-guided selection (slow gait, weak plantarflexors) improves yield. Whether GRAFOs delay rather than prevent surgery is unsettled.
Stance-control KAFOs reliably improve walking velocity, but the often-quoted energy saving over locked KAFOs is not consistently demonstrated (Davis 2010). Velocity and function, not metabolic cost, are the defensible benefits.
Evidence for LSO/corset in non-specific chronic low back pain is weak; any benefit is likely proprioceptive and short-term. Concern about disuse atrophy with prolonged wear persists but is not well quantified.
Once the gold standard for unstable C-spine, the halo carries significant morbidity (pin-site infection, respiratory and swallowing complications) in older patients, shifting practice toward early surgical stabilization in many centres.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 65-year-old man is 3 months post-stroke with left hemiplegia. He has MRC grade 2 ankle dorsiflexors, grade 3 plantarflexors, and mild ankle spasticity (Modified Ashworth Scale 1+). He is currently walking with a quad cane and foot drop. What orthosis would you prescribe and why?”
“A 55-year-old woman fell from a ladder and sustained an L1 burst fracture. CT shows 40% anterior height loss, 25% canal compromise, intact posterior ligamentous complex (no widening of interspinous distance), and she is neurologically intact. The spine surgeon has decided on conservative management. What orthosis would you prescribe?”
“A 10-year-old boy with spastic diplegic cerebral palsy (GMFCS Level II) presents with progressive crouch gait over the past year. Examination shows bilateral knee flexion of 25 degrees in stance, ankle dorsiflexion to 15 degrees with knee extended, hip extension to neutral, and hamstring tightness (popliteal angle 45 degrees). He currently wears hinged AFOs. How would you approach his orthotic management?”
Nomenclature
- AFO = Ankle-Foot Orthosis
- KAFO = Knee-Ankle-Foot Orthosis
- TLSO = Thoracolumbosacral Orthosis
- Named by joints crossed (ISO 8549)
Functions (4 Cs)
- Control - limit unwanted motion
- Correct - apply corrective forces
- Compensate - replace muscle function
- Protect - allow healing
AFO Selection
- Solid AFO = spastic equinus
- Hinged AFO = foot drop, intact PF
- Ground-reaction = crouch gait
- FRAFO = floor reaction, extends knee
Spinal Levels
- TLSO controls T9-L3 effectively
- Above T9 needs CTLSO (sternal)
- Below L3 needs thigh extension
- Halo vest for C0-C7 (best cervical)
Biomechanics
- Three-point pressure = all correction
- Longer lever arm = greater control
- GRAFO moves GRF anterior to knee
- Force distribution prevents ulcers
Prescription Must Include
- Diagnosis and functional goal
- Joints to control
- Motion to allow/block
- Material and footwear requirements
Evidence Base
BrAIST Trial - Bracing for Adolescent Idiopathic Scoliosis
- Multicentre trial (randomized + preference cohorts, 242 patients analysed) in high-risk AIS
- Treatment success (skeletal maturity without curve reaching 50 degrees): 72% bracing vs 48% observation overall
- Intention-to-treat in randomized cohort: 75% success bracing vs 42% observation (OR 4.11)
- Significant dose-response between hours of brace wear and success (P less than 0.001)
- Trial stopped early for efficacy of bracing
AFO Effectiveness in Stroke - Meta-analysis
- Meta-analysis of 19 studies (434 participants) of AFO use in stroke gait
- AFO improved walking speed (SMD 0.50, 95% CI 0.34-0.66)
- Improved cadence, step length and stride length
- Largest effect on Functional Ambulation Category score (SMD 1.61)
- Improved ankle angle at initial contact; body sway not significantly changed
TLSO versus No Orthosis for Thoracolumbar Burst Fractures (RCT)
- Multicentre randomized equivalence trial, AO Type A3 burst fractures T11-L3, neurologically intact, kyphosis under 35 degrees
- TLSO (n=47) versus no orthosis with early ambulation (n=49)
- Roland-Morris Disability score at 3 months: 6.8 (TLSO) vs 7.7 (no orthosis)
- 95% CI (-1.5 to 3.2) fell within the predefined equivalence margin
- Six patients required later surgical stabilization (similar between groups)