Lateral Ankle Pain | PB More Common | Debridement vs Reconstruction
- Peroneus brevis tears more commonly than peroneus longus (PB subjected to higher friction against fibula)
- 80% association with lateral ankle instability - always assess and repair ATFL/CFL concomitantly
- Longitudinal split tears most common pattern (within tendon substance, parallel to fibers)
- Under 50% debride, over 50% reconstruct - critical threshold for preserving function
- SPR (superior peroneal retinaculum) injury allows subluxation - must repair if torn
- “PB compressed between PL and fibula at retromalleolar groove - highest stress zone
- “Low-lying PB muscle belly extends into retromalleolar groove - anatomical variant predisposing to tears
- “Painful arc sign: Pain at fibula tip with active eversion through range = peroneal pathology
- “MRI: highly specific but only moderately sensitive for PB tears (Park 2012: sensitivity ~44-50%, specificity ~99%) - a normal scan does not exclude a tear
PB runs anterior to PL at retromalleolar groove behind lateral malleolus. PB is compressed between PL (posterior) and fibula (anterior) = high friction zone = most common tear location. Low-lying PB muscle belly variant increases compression.
Longitudinal split tears within tendon substance, parallel to fibers. Unlike Achilles (usually transverse rupture), peroneal tears are degenerative splits from chronic friction and compression. PB tears more common than PL.
80% of peroneal tears have lateral ankle instability (ATFL/CFL insufficiency). Chronic instability → increased peroneal load → tears. Must repair lateral ligaments concomitantly with tendon surgery.
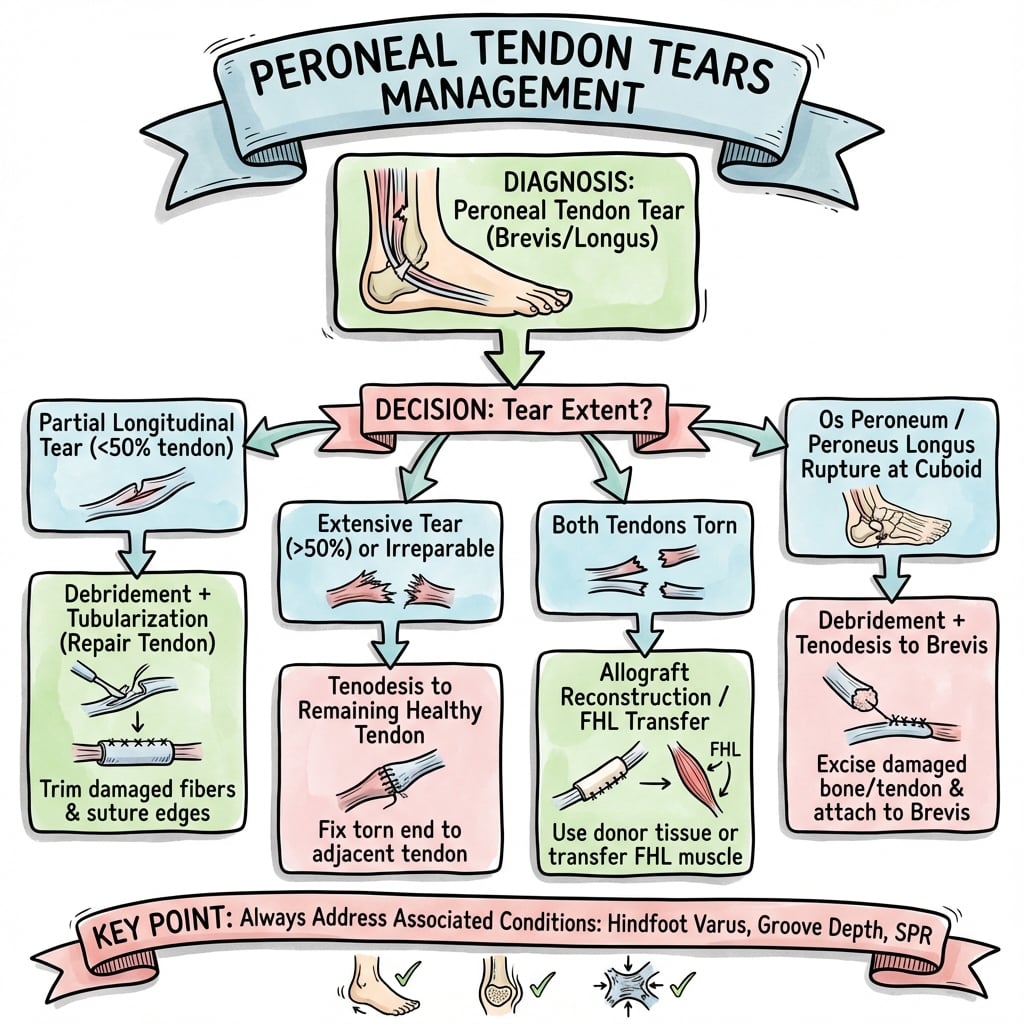
Under 50% tear: Debridement alone preserves function. Over 50% tear: Reconstruction required (tubularization, allograft, or tenodesis to PL). Critical threshold determines surgery type.
- Clinical Presentation
- Lateral ankle pain, mild weakness, palpable tender PB
- Procedure
- Debridement or tubularization
- Key Pearl
- Preserve tendon bulk - debride only diseased tissue
- Clinical Presentation
- Significant weakness, instability feeling, thickened PB
- Procedure
- Tubularization or allograft reconstruction
- Key Pearl
- Under 50% healthy tendon remaining - reconstruct required
- Clinical Presentation
- Severe weakness, cannot perform eversion against resistance
- Procedure
- Tenodesis to PL or allograft interpositional graft
- Key Pearl
- Retracted tear - direct repair impossible
- Clinical Presentation
- Inversion ankle sprains, giving way, positive anterior drawer
- Procedure
- Peroneal surgery + ATFL/CFL reconstruction
- Key Pearl
- MUST address instability - 80% association, recurrent tears if not fixed
- Clinical Presentation
- Peroneal tendons pop anteriorly over fibula with eversion
- Procedure
- Peroneal repair + SPR reconstruction ± fibular groove deepening
- Key Pearl
- SPR (superior peroneal retinaculum) must be repaired or tendons sublux
PB FRONTPeroneal Anatomy at Lateral Ankle
Hook:PB is in FRONT (anterior) and takes the most damage from friction!
Overview and Epidemiology
Peroneal tendon tears are a commonly missed cause of lateral ankle pain, often misdiagnosed as chronic ankle sprain. The tendons are critical for hindfoot eversion and lateral ankle stability. Untreated tears lead to progressive weakness, recurrent instability, and functional limitation. Early recognition and appropriate surgical treatment (debridement for minor tears, reconstruction for major tears) achieves 80-90% good outcomes and prevents chronic disability.
- Incidence: 11-37% of chronic lateral ankle pain cases
- Age: 30-40 years (active adults)
- Gender: Equal distribution (contrast to PTTD which is female-predominant)
- Bilateral: 10-15% have contralateral involvement
- Association: 80% have lateral ankle instability (ATFL/CFL insufficiency)
- Chronic lateral ankle instability (most significant risk)
- Recurrent inversion ankle sprains
- High-level sports (basketball, soccer, tennis)
- Steroid injections (degenerative effect on tendon)
- Low-lying peroneus brevis muscle belly (anatomical variant)
- Shallow retromalleolar groove (less fibular containment)
- Cavovarus hindfoot alignment (increased peroneal load)
Pathophysiology and Mechanisms
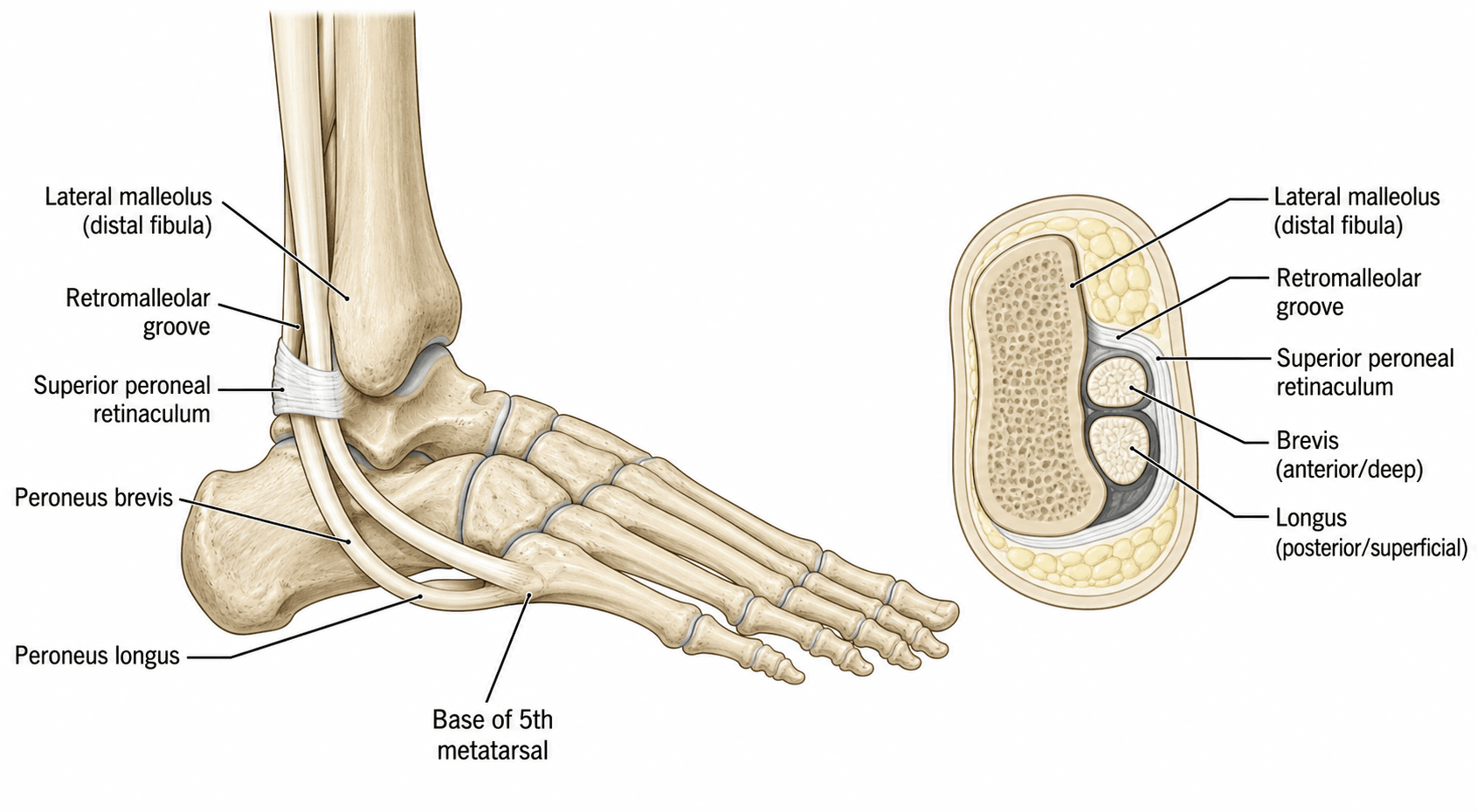
At the retromalleolar groove (behind lateral malleolus), the peroneus brevis runs anterior to peroneus longus. PB is compressed between the fibula (anteriorly) and PL (posteriorly), creating a high-friction zone. This compression, combined with the tendon's excursion during hindfoot inversion-eversion, leads to degenerative tears within the substance of PB. This is why PB tears are far more common than PL tears.
- Anatomical Detail
- Origin: Distal 2/3 lateral fibula. Insertion: Styloid 5th MT base. Position: ANTERIOR at retromalleolar groove.
- Clinical Significance
- Most commonly torn tendon (compressed between PL and fibula). Insertion avulsion = 5th MT base fracture.
- Anatomical Detail
- Origin: Proximal 2/3 lateral fibula. Insertion: Plantar 1st MT base + medial cuneiform. Position: POSTERIOR at groove.
- Clinical Significance
- Less commonly torn (protected position). Runs under cuboid tunnel (can develop os peroneum pathology).
- Anatomical Detail
- Fibular sulcus behind lateral malleolus. Depth varies (shallow groove = subluxation risk).
- Clinical Significance
- Highest stress point for PB. Shallow groove variant predisposes to subluxation and SPR tears.
- Anatomical Detail
- Fibrous band from lateral malleolus to calcaneus. Holds peroneal tendons in retromalleolar groove.
- Clinical Significance
- Tear = peroneal subluxation (tendons pop anteriorly with eversion). Must repair if torn.
- Anatomical Detail
- From calcaneus to inferior extensor retinaculum. Stabilizes tendons at lateral calcaneus.
- Clinical Significance
- Rarely torn. Secondary stabilizer after SPR.
- Anatomical Detail
- Anatomical variant: PB muscle extends into retromalleolar groove (normally only tendon present).
- Clinical Significance
- Increased compression = higher tear risk. Seen in 20-30% of population.
- Hindfoot eversion: PB primary everter (PL secondary)
- Lateral ankle stability: Resist inversion during stance
- Foot plantarflexion: PL contributes (inserts plantar 1st MT)
- First ray depression: PL depresses 1st ray (locks transverse tarsal joint)
- Stance phase: Peroneal eccentric contraction resists inversion
- Swing phase: Eversion prepares foot for heel strike
- Chronic ankle instability increases peroneal load (compensate for insufficient ligaments)
- PB compressed between fibula and PL
- Excursion during inversion-eversion creates friction
- Chronic microtrauma → tendon degeneration
- Longitudinal split develops (parallel to fibers)
- Split propagates with continued stress
- Degenerative process (not acute rupture)
- Friction creates intrasubstance damage
- Split follows fiber direction
The Peroneus Quartus Accessory Muscle
Several of this topic's source studies list peroneus quartus as a predisposing variant, but the muscle itself is never described. The peroneus quartus is an accessory muscle present in roughly 10-22% of the population. It usually arises from the peroneus brevis (or the distal fibula) and most often inserts onto the retrotrochlear eminence of the calcaneus (when it does so it is termed peroneocalcaneus externus).
Why it matters for tears:
- It is an extra structure crowding the retromalleolar groove, increasing the volume the superior peroneal retinaculum must contain.
- The crowding raises compression on the peroneus brevis and can stretch or render the SPR incompetent, predisposing to PB splits and to peroneal subluxation (the same final common pathway as a low-lying PB muscle belly).
- On MRI it appears as an additional muscle and tendon posteromedial to the peroneal tendons - recognising it pre-operatively explains the crowding and may prompt excision of the accessory muscle belly at surgery to decompress the groove.
Three anatomical variants crowd the retromalleolar groove and predispose to peroneus brevis tears and subluxation: a low-lying PB muscle belly, a peroneus quartus accessory muscle, and a shallow (convex) fibular groove. All act by the same mechanism - increased compression and a stretched, incompetent superior peroneal retinaculum. At surgery, excising an accessory or low-lying muscle belly helps decompress the groove.
Classification Systems
Sobel / Krause-Brodsky Grading - For Longitudinal Split Tears
The most commonly used surgical grading for peroneal tendon tears. Sobel et al (Foot & Ankle, 1992) first described the mechanism and longitudinal-split pattern of peroneus brevis tears (the eponymous "Sobel" lesion). Krause and Brodsky (Foot Ankle Int, 1998) then defined the clinically applied surgical grade based on the percentage of cross-sectional area involved, which drives the debride-versus-reconstruct decision.
- Tear Description
- Longitudinal split involving under 50% of tendon width
- Tendon Integrity
- Over 50% healthy tendon remaining - adequate function
- Treatment
- Debridement of diseased tissue OR tubularization (side-to-side repair)
- Tear Description
- Longitudinal split involving over 50% of tendon width
- Tendon Integrity
- Under 50% healthy tendon - inadequate to maintain function
- Treatment
- Tubularization if enough tissue OR allograft reconstruction/tenodesis to PL
- Tear Description
- Complete tendon rupture with retraction
- Tendon Integrity
- No continuity - direct repair impossible
- Treatment
- Allograft interpositional reconstruction OR tenodesis PB to PL (sacrifice brevis)
The 50% width cutoff is the key surgical decision point:
- Under 50% tear: Enough healthy tendon remains (over 50% intact) → Debridement alone preserves function. Simple excision of diseased portion.
- Over 50% tear: Too little healthy tendon (under 50% intact) → Debridement would leave inadequate bulk → Reconstruction required (tubularization, allograft, or tenodesis).
This threshold is based on biomechanical studies showing that removing over 50% of tendon width significantly impairs eversion strength. Preservation of function requires maintaining over 50% tendon bulk.
This classification guides surgical decision-making effectively.
The Os Peroneum and Painful Os Peroneum Syndrome (Peroneus Longus Pathology)
This topic is dominated by peroneus brevis tears, but the peroneus longus has its own characteristic lesion that the differential and radiograph sections rely on without developing it. The os peroneum is a sesamoid within the PL tendon where the tendon turns under the cuboid at the cuboid tunnel; it is ossified in roughly 5-30% of people and is frequently bipartite or multipartite.
Painful os peroneum syndrome (POPS) is the spectrum of PL pathology around this sesamoid:
- Acute os peroneum fracture or diastasis of a multipartite os peroneum (sudden plantar-lateral midfoot pain).
- PL tendinosis or a partial/complete tear at or distal to the os peroneum, often from attrition against the cuboid or a hypertrophied peroneal tubercle.
- Chronic plantar-lateral foot pain along the PL course with tenderness over the os peroneum.
On radiographs, proximal migration of the os peroneum (sitting more proximal than expected, away from the cuboid) indicates a complete distal peroneus longus rupture - the sesamoid is pulled proximally because the distal tendon no longer anchors it. Conversely, distal migration or diastasis of a bipartite os peroneum suggests a tear proximal to the sesamoid. A smooth, well-corticated bipartite os peroneum is a normal variant, whereas irregular fragments with surrounding oedema suggest an acute fracture. POPS is the peroneus longus counterpart to the peroneus brevis split tear, and explains why a normal-looking brevis does not exclude peroneal pathology.
SPLITSobel Classification of Longitudinal Tears
Hook:Peroneal tears SPLIT the tendon longitudinally - remember the Sobel grades!
Clinical Assessment
- Pain location: Lateral ankle, posterior to lateral malleolus
- Chronicity: Usually chronic (months to years), often misdiagnosed as sprain
- Mechanism: Recurrent inversion ankle sprains (80% have lateral instability)
- Functional limitation: Weakness with eversion, difficulty on uneven ground
- Popping/snapping: If SPR torn = peroneal subluxation over fibula
- Prior treatment: Often multiple ankle sprains treated conservatively
- Inspection: Swelling posterior to lateral malleolus, ecchymosis if acute
- Palpation: Tenderness along peroneal tendons, thickening at retromalleolar groove
- Resisted eversion: Weakness and pain (compare to contralateral)
- Painful arc sign: Pain at lateral malleolus during active eversion through range
- Subluxation test: Eversion with dorsiflexion - tendons pop anteriorly if SPR torn
- Lateral ankle stability: Anterior drawer, talar tilt (assess ATFL/CFL)
80% of peroneal tendon tears occur with lateral ankle instability (ATFL/CFL insufficiency). Always perform anterior drawer and talar tilt tests. Positive tests indicate ligamentous injury requiring concomitant repair. Missing lateral instability leads to:
- Persistent symptoms despite peroneal tendon surgery
- Recurrent peroneal tears (increased compensatory load)
- Poor patient outcomes You must address both pathologies surgically - peroneal tendon reconstruction PLUS lateral ligament reconstruction.
- Technique
- Patient actively everts foot against examiner resistance
- Positive Finding
- Weakness and pain posterior to lateral malleolus
- Significance
- Indicates peroneal tendon pathology (tear or tenosynovitis)
- Technique
- Patient actively everts foot through full range of motion
- Positive Finding
- Pain specifically at fibula tip during mid-range eversion
- Significance
- Highly specific for peroneal tendon pathology at retromalleolar groove
- Technique
- Ankle in dorsiflexion and eversion, palpate tendons at fibula
- Positive Finding
- Palpable pop or snap as tendons sublux anteriorly over fibula
- Significance
- SPR tear - requires SPR reconstruction ± fibular groove deepening
- Technique
- Knee flexed 90°, pull talus anteriorly with ankle in neutral
- Positive Finding
- Excessive anterior translation compared to contralateral (over 3mm)
- Significance
- ATFL insufficiency - must repair concomitantly with peroneal surgery
- Technique
- Ankle in neutral, invert hindfoot and assess for excessive tilt
- Positive Finding
- Talar tilt over 10° more than contralateral
- Significance
- CFL insufficiency - consider anatomical ligament reconstruction
- Distinguishing Features
- Chronic retromalleolar pain and swelling, weak/painful resisted eversion, positive painful arc, history of recurrent inversion sprains
- Key Investigation
- MRI (specific, moderately sensitive) ± dynamic ultrasound; surgical confirmation
- Distinguishing Features
- Audible/palpable snapping of tendons anteriorly over the fibula with dorsiflexion-eversion; acute injury often a forced dorsiflexion
- Key Investigation
- Dynamic ultrasound (real-time subluxation); MRI for SPR/fleck sign
- Distinguishing Features
- Recurrent giving-way and inversion sprains, positive anterior drawer/talar tilt - coexists with peroneal tears in a high proportion
- Key Investigation
- Clinical instability tests; stress radiographs; MRI
- Distinguishing Features
- Pain along the plantar-lateral cuboid (PL course); os peroneum tenderness; may follow PL tear
- Key Investigation
- Radiographs (os peroneum, proximal migration); MRI/CT
- Distinguishing Features
- Acute traumatic onset, point tenderness just below/anterior to lateral malleolus, often missed on plain films
- Key Investigation
- CT (radiographs frequently negative)
- Distinguishing Features
- Pain over the sinus tarsi anterolateral to the lateral malleolus, hindfoot instability sensation
- Key Investigation
- Diagnostic injection; MRI
- Distinguishing Features
- Burning/neuropathic pain and altered sensation over the lateral foot, positive Tinel, no eversion weakness
- Key Investigation
- Clinical examination; diagnostic nerve block; nerve studies
- Distinguishing Features
- Stiffness, deep aching, mechanical symptoms, often post-traumatic; tenderness over joint line not tendon
- Key Investigation
- Weight-bearing radiographs; CT for impingement
Investigations
Imaging Protocol for Peroneal Tendon Tears
- Ankle AP, lateral, mortise
- Foot AP, lateral, oblique
- 5th MT base avulsion fracture (PB insertion tear)
- Os peroneum (sesamoid in PL tendon - can be fractured or displaced)
- Calcaneofibular distance (SPR avulsion may show fleck sign)
- Cavovarus alignment (predisposes to peroneal overload)
Not diagnostic for tendon tears but rules out bony pathology.
Diagnostic accuracy: MRI is highly specific but its sensitivity for peroneus brevis tears is limited. Park 2010 reported sensitivity 83.9% and specificity 74.5% for peroneal tendinopathy overall, but Park 2012 (MRI vs surgical reference) found only 44% sensitivity (99% specificity) for PB interstitial tears. A positive scan is reliable; a normal scan does not exclude a tear.
Findings:
- Longitudinal split: Linear high signal T2 within tendon, parallel to fibers
- Complete rupture: Tendon discontinuity, gap, retracted ends
- Tenosynovitis: Fluid surrounding tendon, tendon may be thickened
- SPR tear: Discontinuity of retinaculum, fluid in peroneal sheath
- Associated findings: Lateral ligament tears (ATFL/CFL), bone marrow edema
Protocol: Axial, sagittal, and coronal sequences. Axial images at retromalleolar groove are critical.
- Dynamic assessment (can visualize subluxation in real-time during eversion)
- Less expensive than MRI
- No contraindications (MRI compatible implants)
- Operator-dependent
- Less sensitive than MRI for intrasubstance tears
- Cannot assess bone marrow edema or deep structures
Use: Consider if MRI unavailable or contraindicated, or to assess dynamic subluxation.
MRI is the investigation of choice for suspected peroneal tendon tears, but candidates must know its real performance characteristics. According to PubMed-indexed diagnostic-accuracy studies (Park 2010; Park 2012), MRI is highly specific (~99%) but only moderately sensitive (~44-84%) for peroneus brevis tears - a positive scan is reliable, but a normal scan does not exclude a tear. MRI is still valuable for:
- Characterising tear morphology (split vs complete vs tenosynovitis)
- Assessing associated pathology (lateral ligaments, SPR, bone oedema)
- Preoperative planning
Plain radiographs rule out bony pathology (5th MT fracture, os peroneum fracture) but cannot diagnose tendon tears. In a clinically suspicious ankle with a negative MRI, dynamic ultrasound or surgical exploration may still be warranted. Do not rely on X-rays alone.
Management Algorithm
- Conservative Options
- Immobilization 4-6 weeks, PT, NSAIDs, activity modification
- Surgical Indications
- Failure of 6 months conservative treatment
- Surgical Procedure
- Tenosynovectomy (debulk thickened synovium), assess for underlying tear
- Conservative Options
- Conservative rarely successful if true tear present
- Surgical Indications
- Persistent pain, functional limitation despite 3-6 months conservative
- Surgical Procedure
- Debridement of diseased portion OR tubularization (side-to-side repair)
- Conservative Options
- Conservative ineffective (inadequate tendon bulk)
- Surgical Indications
- Diagnosis confirmed on MRI
- Surgical Procedure
- Tubularization if sufficient tissue OR allograft reconstruction OR tenodesis to PL
- Conservative Options
- Conservative ineffective
- Surgical Indications
- Diagnosis confirmed clinically and on MRI
- Surgical Procedure
- Allograft interpositional graft OR tenodesis PB to PL (sacrifice brevis function)
- Conservative Options
- Conservative fails to address ligamentous pathology
- Surgical Indications
- ATFL/CFL insufficiency (anterior drawer, talar tilt positive)
- Surgical Procedure
- Peroneal surgery + anatomical lateral ligament reconstruction (Brostrom or augmented)
Conservative Management Protocol
Indications: Mild tears (Grade I under 25% width), tenosynovitis without structural tear, or patient unfit for surgery.
Conservative Treatment Steps
- Immobilization: CAM boot or short leg cast
- Weight-bearing: As tolerated in boot
- Ice: 15-20 minutes QID for first 2 weeks
- NSAIDs: If no contraindications
- Elevation: Reduce swelling
- Transition to ankle brace: Lateral support brace
- PT: Range of motion exercises (dorsi/plantarflexion, inversion/eversion)
- Strengthening: Resistance band eversion exercises (start week 8-10)
- Proprioception: Balance board exercises
- Progress strengthening: Increase resistance
- Sport-specific training: Gradual return to activity
- Ankle brace: Continue use during sports
- Activity modification: Avoid repetitive eversion stress
- Ankle brace: Use during high-risk activities
- Maintenance PT: Strengthening and proprioception exercises
- Shoe modifications: Lateral heel wedge if cavovarus alignment
- Surveillance: Return if symptoms recur
Conservative management success rate for peroneal tendon tears is poor compared to other tendinopathies:
- Tenosynovitis (no structural tear): 60-70% success with immobilization + PT
- Grade I tears (under 50%): 30-40% success with conservative management
- Grade II-III tears: Conservative ineffective (under 20% success)
This is because peroneal tears are degenerative splits within high-friction zones - continued use perpetuates the tear. Most Grade I-III tears ultimately require surgical debridement or reconstruction.
Conservative is worth trying but surgery is often needed.
Surgical Technique - Detailed Steps
Patient Positioning
Setup Checklist
Supine or lateral decubitus (lateral preferred by some surgeons for easier access to lateral ankle).
- Bump under ipsilateral hip (internal rotation improves lateral access)
- Sandbag or bolster under operative ankle
- Operative side up
- Beanbag or lateral positioner
- Axillary roll
- All bony prominences padded
- If lateral: axilla (axillary roll), down hip, fibular head (common peroneal nerve)
- If supine: sacrum, contralateral heel
- Thigh tourniquet, inflate to 300mmHg
- Exsanguinate with elevation or Esmarch
- Typical tourniquet time: 60-90 minutes
- Foot and ankle free draped
- Allows manipulation to assess peroneal excursion and lateral stability
- C-arm available if needed (usually not required)
Proper positioning enables optimal surgical exposure.
RECONSurgical Decision-Making
Hook:RECON = RECONstruction is the approach for severe tears and associated pathology!
Complications
- Incidence
- 10-15% at 5 years
- Risk Factors
- Inadequate debridement, uncorrected lateral instability, excessive activity too early
- Management
- If symptomatic: Revision surgery with allograft reconstruction + lateral ligament repair
- Incidence
- 5-10%
- Risk Factors
- SPR not repaired or repair failure, shallow fibular groove
- Management
- Revision SPR reconstruction ± fibular groove deepening
- Incidence
- 2-5% temporary, 1% permanent
- Risk Factors
- Direct injury during dissection, nerve branches variable
- Management
- Prevention: Identify and protect. Treatment: Observation (most recover), neurolysis if persistent
- Incidence
- 5-8%
- Risk Factors
- Thin skin over lateral ankle, tension, smoking
- Management
- Superficial: Local care. Deep: Debridement, VAC, possible flap
- Incidence
- 10-15%
- Risk Factors
- Excessive debridement (over 50% removed), inadequate reconstruction, allograft failure
- Management
- PT for strengthening. If severe: Revision with allograft reconstruction or tenodesis
- Incidence
- 2-5%
- Risk Factors
- More common after foot/ankle surgery
- Management
- Early PT, desensitization, gabapentin, stellate ganglion block
- Incidence
- 10-20%
- Risk Factors
- Prolonged immobilization, adhesions within peroneal sheath
- Management
- Aggressive PT, rarely require sheath release
The most common cause of recurrent peroneal tears is uncorrected lateral ankle instability. To prevent:
- Always assess for instability (anterior drawer, talar tilt tests)
- Repair lateral ligaments if instability present (Brostrom or augmented)
- Repair SPR if torn (prevents subluxation)
- Adequate debridement of all diseased tissue (incomplete debridement = recurrent pathology)
- Appropriate immobilization postop (4-6 weeks NWB, protect repairs)
- Address cavovarus alignment if present (lateral heel wedge or calcaneal osteotomy)
Postoperative Care and Rehabilitation
Rehabilitation Timeline (Debridement or Tubularization)
- Short leg splint, keep dry
- NWB with crutches or walker
- Elevation, ice, DVT prophylaxis
- Follow-up week 2: Remove splint, check wound, transition to boot
- Transition to CAM boot (removable for hygiene)
- Continue NWB for full 6 weeks total
- Rationale: Protect tendon repair/tubularization healing
- Start partial weight-bearing in boot (25-50% body weight)
- PT: Gentle ankle ROM (dorsi/plantarflexion)
- Avoid forced eversion until week 10
- Progress to full weight-bearing in boot
- PT: Strengthening (resistance band eversion), proprioception
- Wean from boot to supportive shoe + ankle brace
- Shoe + ankle brace for activities
- Continue PT: Progressive strengthening, sport-specific training
- Return to full activity: 4-6 months
- Long-term: Ankle brace for high-risk sports
6-week NWB protects tendon healing:
- Tubularization sutures achieve biological strength at 6-8 weeks
- Early weight-bearing risks re-tearing at repair site
- SPR repair (if performed) also requires 6 weeks to heal
Patients who bear weight early have higher recurrent tear rates (20-30% vs under 10% with compliant NWB).
Strict adherence to protocol optimizes outcomes.
Outcomes and Prognosis
- Success Rate
- 80-90% good outcomes
- Patient Satisfaction
- 85-90% satisfied
- Return to Activity
- 4-6 months
- Notes
- Best outcomes if under 25% tear, lateral instability addressed
- Success Rate
- 75-85% good outcomes
- Patient Satisfaction
- 80-85% satisfied
- Return to Activity
- 4-6 months
- Notes
- Effective if adequate tissue for side-to-side repair
- Success Rate
- 75-85% good outcomes
- Patient Satisfaction
- 75-85% satisfied
- Return to Activity
- 6-8 months
- Notes
- Longer recovery than debridement, graft incorporation time
- Success Rate
- 70-80% pain relief
- Patient Satisfaction
- 70-80% satisfied
- Return to Activity
- 6-8 months
- Notes
- Sacrifice of PB function, lower eversion strength, acceptable for low-demand patients
- Success Rate
- 80-85% good outcomes
- Patient Satisfaction
- 85-90% satisfied
- Return to Activity
- 6-8 months
- Notes
- Combined procedure has better outcomes than peroneal surgery alone if instability present
Risk factors for poor outcomes after peroneal tendon surgery:
- Lateral ankle instability not addressed: 50% recurrence if instability not repaired
- SPR not repaired: Recurrent subluxation, progression of pathology
- Worker's compensation: Lower satisfaction, prolonged recovery
- Smoking: Impaired wound and tendon healing
- Advanced degenerative tears: Grade III complete ruptures have lower success than Grade I-II
- Delayed diagnosis: Chronic tears (over 6 months) have more degeneration, worse tissue quality
Patients with multiple risk factors may benefit from earlier surgical intervention and realistic expectation counseling.
- 75-80% maintain good outcomes at 5 years
- 10-15% develop recurrent tears or progression
- 5-10% require revision surgery
- 70-80% maintain good outcomes at 5 years
- 15-20% have graft-related issues (failure, persistent weakness)
- 10-15% require revision
- 70-80% return to same level of sport
- 15-20% return to lower level
- 5-10% unable to return to sport
- 60-70% return to elite competition
- Longer recovery (6-8 months minimum)
- Higher recurrence risk if return too early
Long-term brace use recommended for pivoting sports (basketball, soccer, tennis)
Guidelines, Registries & Global Practice
Peroneal tendon pathology is a worldwide and frequently missed cause of chronic lateral ankle pain. There is no high-level (Level I) randomised evidence and no formal national-society guideline dedicated to peroneal tendon tears in any health system - management is built on Level III-IV cohorts, expert consensus and the principle of treating the tear and its cause (instability, subluxation, hindfoot varus).
Global Epidemiology (PubMed-backed)
- Figure
- Peroneal pathology found in a high proportion at surgery (e.g. 31/82 ankles, ~38%, on MRI-surgical correlation)
- Source / Population
- Park 2010, chronic-instability cohort (Korea)
- Figure
- Peroneus brevis far exceeds peroneus longus; concomitant PL+PB tears are recognised but uncommon
- Source / Population
- Sobel 1992; Krause & Brodsky 1998; Redfern & Myerson 2004
- Figure
- Active adults, commonly mid-30s (mean 36-39 years across surgical series)
- Source / Population
- Redfern & Myerson 2004; Park 2012
- Figure
- Chronic lateral ligament instability, SPR incompetence/subluxation, hindfoot/cavovarus alignment, low-lying PB belly, peroneus quartus
- Source / Population
- Sobel 1992; Park 2010; Redfern & Myerson 2004
Guidance and Consensus Across Regions
- Position
- No condition-specific clinical practice guideline; covered within general foot & ankle / tendon-disorder education. Practice driven by expert series.
- Evidence Level
- Expert/consensus (no CPG)
- Position
- No dedicated NICE guidance or BOAST for peroneal tendon tears; managed under general soft-tissue ankle injury and chronic lateral ankle pain pathways with MRI and physiotherapy-first principles.
- Evidence Level
- Expert/consensus (no CPG)
- Position
- Provides surgical technique and approach guidance (retromalleolar exposure, SPR repair, groove deepening) rather than a treatment guideline.
- Evidence Level
- Technique reference
- Position
- Echoes the international consensus on lateral ankle instability (e.g. ESSKA-AFAS): inspect and address peroneal pathology when operating on the unstable lateral ankle.
- Evidence Level
- Consensus (Level V)
- Position
- Trial of conservative care first (immobilisation, physiotherapy); surgery for refractory symptoms; grade by cross-sectional area (under vs over 50%); always correct instability/subluxation/varus.
- Evidence Level
- Level III-IV cohorts
Unlike arthroplasty or fracture fixation, peroneal tendon surgery is not captured by national joint or implant registries (NJR, AJRR, AOANJRR, SHAR, NZJR). The evidence base is therefore institutional case series and systematic reviews rather than registry data - candidates should be explicit that the recommendations rest on lower-level evidence, which is itself an examinable point.
Global Practice Variation
- Routine MRI ± dynamic ultrasound before surgery
- Allograft and tendon-transfer reconstruction freely available for Grade II-III tears
- Combined peroneal + anatomical lateral-ligament reconstruction performed in a single sitting
- Tendoscopic/minimally invasive techniques increasingly used
- Greater reliance on clinical diagnosis and ultrasound where MRI access is limited
- Autograft (e.g. hamstring/FHL transfer) preferred where allograft is unavailable or unaffordable
- Tenodesis to peroneus longus favoured as a simple, graft-free salvage
- Longer conservative trials due to access/waiting-time constraints
Whatever the health system, the standard of care is the same:
- Always assess for and correct lateral ankle instability - uncorrected instability is the leading driver of recurrent tears.
- Trial appropriate conservative care first (immobilisation, physiotherapy, activity modification) for tears amenable to it.
- Grade by cross-sectional area - under 50% debride/tubularise, over 50% reconstruct or tenodese.
- Repair the SPR / address subluxation and any hindfoot varus to remove the causative mechanical load.
- Counsel realistic recovery - protected weight-bearing for several weeks and 4-6 months to sport, with return-to-work planning for manual workers.
- Protect the sural nerve during the retromalleolar approach (~2-5% transient injury).
MCQ Practice Points
Q: At the retromalleolar groove behind the lateral malleolus, which peroneal tendon runs anterior and which runs posterior? A: Peroneus brevis (PB) runs anterior, peroneus longus (PL) runs posterior. This anatomy is critical because PB is compressed between the fibula (anteriorly) and PL (posteriorly), creating a high-friction zone. This is why PB tears are far more common than PL tears - PB subjected to higher stress from compression and friction.
Q: What is the critical threshold in Sobel classification that determines whether debridement alone is sufficient or reconstruction is required? A: 50% of tendon width. Sobel Grade I (under 50% width tear) can be treated with debridement alone because over 50% healthy tendon remains, which is adequate to maintain eversion function. Sobel Grade II (over 50% width tear) requires reconstruction (tubularization, allograft, or tenodesis) because under 50% healthy tendon remains after debridement, which is inadequate for function. This 50% threshold is based on biomechanical studies showing significant impairment when over 50% of tendon is removed.
Q: What percentage of peroneal tendon tears are associated with lateral ankle instability, and why is this clinically important? A: 80% of peroneal tendon tears occur with lateral ankle instability (ATFL/CFL insufficiency). This is clinically critical because: (1) Surgeons must assess for lateral instability in all peroneal tear patients (anterior drawer, talar tilt tests); (2) Failure to address lateral instability leads to 50% recurrent tear rate because the peroneals remain overloaded (compensating for insufficient ligaments); (3) Combined peroneal reconstruction + lateral ligament repair achieves 80-85% good outcomes vs only 50-60% for peroneal surgery alone if instability present.
Q: What is the diagnostic accuracy of MRI for peroneal tendon tears, and what is the characteristic MRI appearance of a longitudinal split tear? A: MRI is the imaging investigation of choice but candidates should know it is highly specific yet only moderately sensitive for peroneus brevis tears - Park 2010 reported sensitivity 83.9% / specificity 74.5% for tendinopathy overall, while Park 2012 (surgical reference standard) found only 44% sensitivity but 99% specificity for PB interstitial tears. A positive scan is reliable; a normal scan does not exclude a tear. Characteristic appearance of a longitudinal split tear: linear high T2 signal within the tendon substance, oriented parallel to the long axis of the tendon. This is distinct from complete rupture (gap with discontinuity) and tenosynovitis (fluid surrounding an intact tendon without intrasubstance signal). Axial images at the level of the retromalleolar groove are most useful.
Q: A patient has a Sobel Grade II peroneal brevis tear (65% width involved) and positive anterior drawer test. What is the appropriate surgical treatment? A: Allograft reconstruction of peroneus brevis + lateral ligament reconstruction (Brostrom). Rationale: (1) Grade II tear (over 50% width) requires reconstruction - debridement would leave inadequate tendon bulk; (2) Allograft reconstruction (Pulvertaft weave) restores tendon continuity and bulk; (3) Positive anterior drawer indicates ATFL insufficiency - MUST repair lateral ligaments concomitantly (Brostrom or augmented Brostrom-Gould) to prevent recurrent tears; (4) Failure to address instability leads to 50% recurrence rate.
Q: What is the most common cause of recurrent peroneal tendon tears after surgical treatment? A: Uncorrected lateral ankle instability. Peroneal tears have 80% association with lateral ankle instability (ATFL/CFL insufficiency). If the lateral ligaments are not repaired at the time of peroneal surgery, the tendons remain overloaded (compensating for the insufficient ligaments), leading to recurrent tears in up to 50% of cases. Other causes include inadequate debridement of diseased tissue, superior peroneal retinaculum not repaired (subluxation causes recurrent trauma), and excessive early activity. Prevention requires assessment for instability (anterior drawer, talar tilt) and concomitant lateral ligament reconstruction if present.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old recreational basketball player presents with chronic lateral ankle pain for 8 months. He has a history of multiple ankle sprains. Pain is posterior to the lateral malleolus, worse with activity. On examination, he has tenderness along the peroneal tendons, weakness with resisted eversion, and positive anterior drawer test. How would you assess and manage this patient?”
“You are performing peroneal tendon surgery via retromalleolar approach. After opening the peroneal sheath, you identify a longitudinal split tear of the peroneus brevis. How do you assess the severity intraoperatively, and what are your surgical options based on different tear grades?”
“A patient returns 18 months after peroneal tendon debridement surgery with recurrent lateral ankle pain and weakness. Examination reveals tenderness over peroneals and positive anterior drawer test. MRI shows recurrent longitudinal tear of PB, now involving 60% of tendon width. How do you manage this complication?”
Key Anatomy
- PB runs ANTERIOR to PL at retromalleolar groove - PB compressed between fibula and PL = high friction
- PB insertion = 5th MT styloid (avulsion = Jones fracture). PL insertion = plantar 1st MT base + medial cuneiform
- Superior peroneal retinaculum (SPR) = holds tendons in retromalleolar groove, tear = subluxation
- Low-lying PB muscle belly = anatomical variant (20-30%), muscle extends into groove = increased compression = tear risk
- Sural nerve = posterior to retromalleolar incision, variable branches at ankle = injury risk 2-5%
Classification - Sobel Grading
- Grade I = under 50% width tear = debridement or tubularization
- Grade II = over 50% width tear = reconstruction (allograft or tenodesis to PL)
- Grade III = complete rupture with retraction = allograft reconstruction or tenodesis
- CRITICAL THRESHOLD: 50% width - under 50% debride, over 50% reconstruct
- Longitudinal split pattern = degenerative tears parallel to fibers (not traumatic transverse ruptures)
Surgical Algorithm
- 80% association with lateral ankle instability - MUST assess (anterior drawer, talar tilt) and repair ATFL/CFL if present
- Grade I under 25%: Debridement alone. Grade I 25-50%: Tubularization (side-to-side repair)
- Grade II-III: Allograft reconstruction (Pulvertaft weave) or tenodesis PB to PL (low-demand)
- SPR torn: Repair with suture anchors to fibula (prevents subluxation)
- Combined surgery (peroneal + lateral ligament) = 80-85% success vs 50-60% peroneal alone if instability present
Surgical Pearls
- Retromalleolar approach: Protect sural nerve (posterior to incision), open peroneal sheath longitudinally
- Assess severity intraoperatively: Grade by % width, debride diseased tissue first then assess remaining healthy tissue
- Tubularization: Side-to-side with 2-0 or 3-0 absorbable suture, creates single tubular tendon
- Allograft: Pulvertaft weave 3-4 passes, tension in PF/eversion, non-absorbable suture, NWB 6 weeks for incorporation
- SPR repair mandatory if torn: Suture anchors to fibula or periosteal flap augmentation
Complications
- Recurrent tear: 10-15% - most common cause is uncorrected lateral instability (50% recurrence if not repaired)
- Sural nerve injury: 2-5% temporary, 1% permanent - protect during retromalleolar exposure
- Persistent subluxation: 5-10% - SPR not repaired or repair failure, requires revision SPR reconstruction
- Persistent weakness: 10-15% - excessive debridement (over 50%), inadequate reconstruction, allograft failure
- Wound complications: 5-8% - thin skin over lateral ankle, smoking risk factor
Evidence Base and Key Trials
Sobel: Dynamics of Peroneus Brevis Splits - Mechanism and Classification
- Anatomic and histologic study proposing the mechanism and classification of peroneus brevis longitudinal splits
- Splits develop from chronic mechanical attrition at the fibular groove - PB is splayed against the sharp posterior fibular edge by peroneus longus compression
- Superior peroneal retinaculum laxity allowing subluxation is central to the pathomechanism
- Predisposing anatomic factors: shallow (convex) fibular groove, low-lying PB muscle belly, peroneus quartus
- This paper is the origin of the eponymous Sobel description of PB split tears
Krause & Brodsky: Peroneus Brevis Tears - Grading and Surgical Reconstruction
- Clinical series of 20 patients - largest of its kind at the time - defining the widely used surgical grading
- Grade 1: under 50% of cross-sectional area damaged - debridement and tubularisation repair
- Grade 2: over 50% of cross-sectional area destroyed - excision of damaged segment and tenodesis to peroneus longus
- Both groups must additionally be augmented by stabilising the causative subluxation (SPR)
- Mean postoperative AOFAS score 85; good-to-excellent results in the majority but prolonged recovery
Redfern & Myerson: Management of Concomitant Peroneus Longus and Brevis Tears
- 28 patients (29 feet) with combined PL and PB tears, mean follow-up 4.6 years
- Surgical algorithm based on whether a functioning tendon remains, mobility of the muscle, ankle stability and heel position
- 9/28 had hindfoot varus or cavovarus; 8/28 had mechanical ankle instability
- Mean postoperative AOFAS 82; 91% achieved normal or moderate peroneal strength
- Conclusion: address the primary or contributing cause (instability, subluxation, hindfoot varus) at the time of tendon repair
Demetracopoulos: Long-Term Results of Debridement and Primary Repair
- 34 patients with PB and/or PL tears treated by debridement and primary repair (single surgeon, 1994-2008)
- 18 followed for a mean of 6.5 years (range 2-14 years)
- Mean VAS pain improved from 39 to 10; LEFS improved from 45 to 71 (both p under 0.001)
- 17 of 18 returned to full sporting activity without limitation
- No reoperations or operative failures over the study interval
Park: Reliability of MRI for Peroneal Tendinopathy in Chronic Lateral Ankle Instability
- 82 ankles with chronic lateral ankle instability had preoperative MRI compared with operative findings
- Sensitivity 83.9%, specificity 74.5% for peroneal tendinopathy overall
- Positive predictive value 66.7%, negative predictive value 88.4%, accuracy 78.0%
- Low-lying muscle belly and peroneus quartus frequently identified as associated variants
- Conclusion: MRI is useful but often equivocal - thorough clinical examination remains essential
Park: Accuracy of MRI vs Surgery for Characterising Peroneal Tendon Disorders
- 97 patients with chronic lateral ankle instability had MRI followed by surgery (reference standard), two blinded readers
- For PB interstitial tears: sensitivity 44%, specificity 99%
- For PB swelling: sensitivity 50%, specificity 99%
- MRI of chronic peroneal pathology is diagnostically specific but NOT sensitive
- Tempers the common teaching that MRI is highly sensitive for peroneal tears
Oden: Classification of Peroneal Tendon Dislocation
- Describes tendon injuries about the ankle resulting from skiing, including peroneal tendon dislocation
- Presents four types of peroneal tendon dislocation and related problems
- The four-grade scheme modifies the earlier Eckert and Davies classification of SPR injury
- Forms the basis of the still-cited Oden grading of peroneal subluxation/dislocation
- Mechanism is forced dorsiflexion with reflex peroneal contraction