Degenerative Process | Conservative First | 90% Resolve at 1 Year | Surgery Only After 6-12 Months
- Plantar fasciitis is a degenerative process, not inflammatory - prefer term plantar fasciosis or plantar heel pain
- 90% resolve with conservative management within 12 months - surgery is rarely needed
- Risk factors: obesity, pes planus, limited ankle dorsiflexion, prolonged standing
- Diagnosis is clinical - tenderness at medial calcaneal tubercle, pain with first steps
- Conservative trial 6-12 months mandatory before considering surgery
- Steroid injection provides short-term relief but risk of fascia rupture - use sparingly
- Surgical release: partial (medial 50%) vs complete - never release more than 50% to avoid lateral column overload
- “Plantar fascia is windlass mechanism - passive toe extension tightens fascia and raises arch
- “Heel spur present in 50% but is incidental finding, not cause of pain
- “Fascia rupture causes sudden relief of pain but lateral column pain and arch collapse
- “Nerve entrapment (Baxter nerve) is important differential - burning pain, night pain
Histology shows myxoid degeneration and collagen necrosis, not inflammation. Use term plantar fasciosis or plantar heel pain. This explains why NSAIDs and steroid injections have limited long-term benefit.
90% resolve within 12 months with conservative care. Mandatory trial of 6-12 months before surgery. Include stretching (gastrocnemius and plantar fascia), orthoses, activity modification, and PT.
Never release more than 50% of the plantar fascia width. Complete release causes lateral column overload, arch collapse, and worse outcomes. Release medial half only from medial calcaneal tubercle.
Baxter nerve entrapment mimics plantar fasciitis - first branch of lateral plantar nerve compressed between abductor hallucis and quadratus plantae. Look for burning pain, night pain, and positive Tinel sign.
Overview and Epidemiology
Plantar fasciitis (also termed plantar fasciosis or plantar heel pain syndrome) is the most common cause of inferior heel pain in adults, accounting for approximately 1 million patient visits annually in the United States. Despite the suffix "itis" suggesting inflammation, histological studies demonstrate a degenerative process characterized by myxoid degeneration, collagen necrosis, and angiofibroblastic hyperplasia rather than acute inflammation.
Epidemiology:
- Incidence: Affects approximately 10% of the population at some point in their lifetime
- Peak age: 40-60 years, though can occur at any age
- Gender: Slight female predominance (2:1 ratio)
- Bilateral: Occurs in 30% of cases
- Athletes: Higher incidence in runners (up to 22% prevalence) and dancers
The term plantar fasciitis is entrenched in clinical practice, but plantar fasciosis or plantar heel pain more accurately reflects the pathology. In exams, acknowledge that histology shows degeneration, not inflammation, which explains the limited benefit of anti-inflammatory treatments.
Natural history:
- Self-limiting condition: 80-90% resolve within 12 months with conservative treatment
- Spontaneous resolution: Even without treatment, many cases improve over 1-2 years
- Recurrence: Approximately 25% experience recurrent symptoms
- Chronic cases: 10% develop chronic, refractory symptoms requiring advanced interventions
The excellent prognosis with conservative care is the foundation of treatment algorithms, with surgery reserved only for the small minority who fail comprehensive non-operative management.
Risk Factors and Prevention
- Modifiable
- Tight gastrocnemius, poor footwear, training errors, abnormal gait
- Non-Modifiable
- Pes planus, pes cavus, leg length discrepancy, age 40-60
- Modifiable
- Obesity (BMI over 30), weight management
- Non-Modifiable
- Female gender, genetic predisposition to flat feet
- Modifiable
- Occupational standing, running volume, surface hardness
- Non-Modifiable
- None
- Modifiable
- Diabetes control, inflammatory arthritis management
- Non-Modifiable
- Seronegative spondyloarthropathy, diabetes mellitus
- Obesity: Strongest modifiable risk factor - BMI over 30 increases risk 5-fold
- Tight gastrocnemius-soleus complex: Limited ankle dorsiflexion (under 10 degrees) increases plantar fascia strain
- Inappropriate footwear: Worn-out shoes, lack of arch support, high heels, flip-flops
- Training errors: Sudden increase in running distance or intensity (over 10% per week increase)
- Occupational: Prolonged standing or walking on hard surfaces (over 8 hours daily)
- Poor biomechanics: Overpronation, supination, or other gait abnormalities
- Weight management: Maintain healthy BMI
- Stretching program: Daily gastrocnemius and plantar fascia stretching
- Appropriate footwear: Well-cushioned shoes with arch support, replace running shoes every 400-500 miles
- Activity progression: Gradual increase in activity level (10% rule)
- Cross-training: Vary exercise to reduce repetitive stress
- Early intervention: Address tight calf muscles and biomechanical issues promptly
Pathophysiology
Plantar Fascia Anatomy
- Origin: Medial calcaneal tubercle on the medial process of the calcaneal tuberosity
- Insertion: Divides into five bands inserting onto the proximal phalanges and flexor tendon sheaths
- Composition: Dense fibrous connective tissue arranged in three bands (medial, central, lateral)
- Central band: Thickest and strongest, most commonly affected in plantar fasciitis
- Thickness: Normal fascia is 2-4mm thick; in plantar fasciitis often exceeds 4mm
- Blood supply: Relatively avascular, which contributes to slow healing
- Windlass mechanism: Passive toe extension during push-off tightens the plantar fascia and raises the medial longitudinal arch
- Arch support: Provides static support to the longitudinal arch of the foot
- Shock absorption: Absorbs impact forces during heel strike (up to 2-3 times body weight)
- Spring ligament: Works in concert with spring ligament and posterior tibial tendon for arch stability
The windlass test reproduces pain by passively dorsiflexing the hallux, which tightens the plantar fascia and stresses the inflamed origin. This test has good sensitivity (32-100%) but variable specificity, and helps confirm the diagnosis clinically.
Pathophysiology
Degenerative process (not inflammatory):
Histological studies of chronic plantar fasciitis demonstrate:
- Myxoid degeneration: Disorganization of collagen fibers
- Collagen necrosis: Breakdown of normal fascial architecture
- Angiofibroblastic hyperplasia: Proliferation of fibroblasts and small blood vessels
- Absence of inflammatory cells: Minimal or no lymphocytes, macrophages, or neutrophils
This pathology is similar to other tendinopathies (Achilles tendinosis, lateral epicondylosis) and explains why anti-inflammatory treatments have limited long-term efficacy.
Mechanical overload theory:
The most accepted theory involves repetitive microtrauma to the plantar fascia origin:
- Repetitive stress: Excessive or repetitive loading exceeds the fascia's capacity for repair
- Microtears: Develop at the fascial origin from the medial calcaneal tubercle
- Failed healing response: Instead of inflammation and repair, degeneration occurs
- Cycle continues: Ongoing stress prevents healing, perpetuating the degenerative process
- Tight gastrocnemius: Limited ankle dorsiflexion increases strain on plantar fascia by up to 15%
- Obesity: Increased BMI directly increases load on the fascia
- Abnormal foot mechanics: Both pes planus (overpronation) and pes cavus (poor shock absorption) increase stress
- Occupational standing: Prolonged standing or walking on hard surfaces
- Training errors: Sudden increase in activity in runners or athletes
- Prevalence: Calcaneal spurs present in 50% of patients with plantar fasciitis
- Asymptomatic spurs: Also present in 15-25% of asymptomatic individuals
- Formation: Develops from traction at the origin of flexor digitorum brevis, not the plantar fascia
- Clinical significance: Spur is an incidental finding, not the cause of pain
- Surgical implication: Spur excision is unnecessary during plantar fascia release
Classification
Classification by Severity
- Description
- Early/acute
- Symptoms
- Morning pain resolving within 10-15 minutes
- Impact on Activity
- Minimal activity modification
- Description
- Subacute
- Symptoms
- Persistent pain affecting daily activities
- Impact on Activity
- Modified exercise program
- Description
- Chronic
- Symptoms
- Constant pain with rest pain
- Impact on Activity
- Unable to perform usual activities
- Description
- Treatment-resistant
- Symptoms
- Failed 6+ months conservative care
- Impact on Activity
- Consider procedural intervention
Clinical Presentation and Diagnosis
History
Classic presentation:
- First-step pain: Severe pain with first steps in the morning or after prolonged sitting (95% of cases)
- Pain location: Inferior heel at the medial calcaneal tubercle
- Gradual onset: Usually develops over weeks to months, not acute
- Pain pattern: Improves with initial activity as fascia "warms up," then worsens with prolonged activity
- Impact of rest: Pain decreases with rest, recurs with weight-bearing
- Night pain: Typically absent - if present, consider other diagnoses
Red flags requiring further investigation:
- Severe night pain (possible infection, tumor, inflammatory arthritis)
- Fever, systemic symptoms (septic arthritis, osteomyelitis)
- History of trauma (calcaneal fracture)
- Progressive neurological symptoms (tarsal tunnel, nerve compression)
- Lack of response to conservative treatment (reconsider diagnosis)
- Walking barefoot on hard surfaces
- Climbing stairs
- Prolonged standing or walking
- Running or jumping activities
- First steps after rest
- Rest
- Sitting with feet elevated
- Supportive footwear
- Activity modification
Physical Examination
- Gait: May demonstrate antalgic gait with shortened stance phase on affected side
- Foot alignment: Assess for pes planus, pes cavus, or neutral arch
- Muscle atrophy: Chronic cases may show calf atrophy
- Swelling: Typically absent - if present, consider alternative diagnosis
- Point tenderness: Exquisite tenderness at medial calcaneal tubercle (95% sensitive)
- Location: Typically 4cm or less from the insertion point
- Diffuse vs focal: Plantar fasciitis causes focal tenderness; diffuse pain suggests alternative diagnosis
- Lateral tenderness: Absence of lateral heel tenderness helps distinguish from other conditions
- Ankle dorsiflexion: Assess with knee extended (gastrocnemius) and flexed (soleus)
- Limited dorsiflexion: Less than 10 degrees with knee extended is significant risk factor
- Hallux dorsiflexion: Normal but may reproduce pain (windlass test)
- Technique
- Passively dorsiflex hallux
- Positive Finding
- Reproduction of heel pain
- Clinical Significance
- Confirms plantar fascia as pain source
- Technique
- Tap over tarsal tunnel or Baxter nerve
- Positive Finding
- Radiating burning pain
- Clinical Significance
- Suggests nerve entrapment
- Technique
- Dorsiflex ankle and evert foot
- Positive Finding
- Pain medial heel
- Clinical Significance
- Suggests posterior tibial tendon pathology
- Technique
- Deep palpation between abductor hallucis and quadratus plantae
- Positive Finding
- Burning pain, radiation
- Clinical Significance
- Baxter nerve entrapment
With the patient standing or sitting, passively dorsiflex the hallux (great toe) while palpating the plantar fascia. This tightens the fascia through the windlass mechanism. Pain at the medial calcaneal origin is a positive test. Sensitivity varies (32-100%) but specificity is good when combined with history.
Differential Diagnosis
Important alternative diagnoses:
-
Baxter nerve entrapment (first branch of lateral plantar nerve):
- Burning pain, often with radiation to medial heel
- Night pain more common than plantar fasciitis
- Positive Tinel sign between abductor hallucis and quadratus plantae
- May coexist with plantar fasciitis
-
Tarsal tunnel syndrome:
- Pain and paresthesias in plantar foot
- Positive Tinel sign posterior to medial malleolus
- Night pain and numbness common
-
Calcaneal stress fracture:
- History of increased activity or trauma
- Pain with medial-lateral calcaneal squeeze test
- Tenderness over calcaneal body, not just plantar aspect
-
Fat pad atrophy or contusion:
- Diffuse heel pain, not focal at medial tubercle
- History of repetitive impact or prior steroid injections
- Pain worse with direct pressure to heel pad
-
Inflammatory arthritis (seronegative spondyloarthropathy):
- Bilateral symptoms common
- Morning stiffness lasting over 30 minutes
- Associated symptoms (back pain, uveitis, psoriasis)
- Positive HLA-B27 in many cases
-
Calcaneal apophysitis (Sever disease) in children:
- Age 8-15 years
- Tenderness at calcaneal insertion of Achilles tendon
- Pain with squeeze test of calcaneus
-
Tumor or infection (rare):
- Night pain, systemic symptoms
- Progressive pain unrelieved by rest
- Requires imaging to rule out
- Key distinguishing features
- First-step pain, focal medial calcaneal tubercle tenderness, no night pain, positive windlass test
- Best confirmatory test
- Clinical; ultrasound fascia over 4mm
- Key distinguishing features
- Burning pain, night pain, radiation to lateral heel, Tinel sign between abductor hallucis and quadratus plantae
- Best confirmatory test
- MRI / nerve studies; diagnostic block
- Key distinguishing features
- Plantar paraesthesiae, Tinel sign posterior to medial malleolus, numbness
- Best confirmatory test
- MRI; nerve conduction studies
- Key distinguishing features
- Activity-related, positive medial-lateral squeeze test, calcaneal body tenderness
- Best confirmatory test
- MRI (marrow oedema) / bone scan
- Key distinguishing features
- Diffuse central heel pain, prior steroid injections or impact, thin heel pad
- Best confirmatory test
- Clinical; ultrasound pad thickness
- Key distinguishing features
- Bilateral, morning stiffness over 30 min, enthesitis, uveitis/psoriasis, HLA-B27
- Best confirmatory test
- HLA-B27, inflammatory markers, MRI
- Key distinguishing features
- Child 8-15 years, posterior calcaneal pain, positive squeeze test
- Best confirmatory test
- Clinical (radiographs to exclude other)
The Heel Fat Pad and Heel Fat Pad Syndrome
The heel fat pad recurs through this topic — as a differential (above), as the structure thinned by misplaced steroid, and as the "normal 2cm" landmark on ultrasound — but it is worth understanding in its own right because it is the most commonly confused alternative cause of plantar heel pain.
Specialised anatomy: The plantar heel pad is not ordinary subcutaneous fat. It is a purpose-built shock absorber made of fat-filled chambers tethered by tough fibrous (collagen and elastin) septa that anchor the skin to the calcaneus. These are arranged as larger deep macrochambers and smaller superficial microchambers, giving a hydraulic, self-recoiling cushion that dissipates the high impulsive loads of heel strike and protects the calcaneus and plantar nerves.
Why it fails: The septa stiffen and the chambers lose elasticity and height with age, with repetitive high-impact loading, in high body weight, and after corticosteroid injection (the same atrophy listed among this topic's complications). The result is heel fat pad atrophy, which reduces cushioning and exposes the calcaneal tuberosity.
Heel fat pad syndrome — distinguishing it from plantar fasciitis:
- Pain is deep and central under the weight-bearing calcaneus, rather than at the medial calcaneal tubercle of plantar fasciitis.
- It is worse walking barefoot on hard surfaces and after prolonged standing, but lacks the classic severe first-step (post-static) pain of plantar fasciitis.
- The pad feels thin and the bone readily palpable; the windlass test is negative.
- Management is cushioning (heel cups, cushioned orthoses, supportive footwear), activity and weight modification — and specifically avoiding corticosteroid, which accelerates atrophy. It does not respond to plantar fascia release.
A patient with central heel pain that is worst barefoot on hard floors, a thin palpable heel pad, and a negative windlass test has heel fat pad syndrome, not plantar fasciitis — the pain is under the body of the calcaneus, not at the medial tubercle. Treat with cushioning and load management and avoid steroid (it worsens fat pad atrophy); fascia-directed treatments, including release, will not help.
Investigations and Imaging
Diagnosis is Clinical
Plantar fasciitis is primarily a clinical diagnosis based on history and physical examination. Imaging is reserved for atypical presentations, failed conservative treatment, or when alternative diagnoses are suspected.
Normal Plantar Fascia Anatomy

Plain Radiographs
- Atypical presentation
- History of trauma
- Failed conservative treatment over 3 months
- Need to rule out fracture, tumor, or other bony pathology
- Heel spur: Present in 50% of plantar fasciitis cases but also in 15-25% of asymptomatic individuals
- Incidental finding: Spur location is at flexor digitorum brevis origin, not plantar fascia
- Not diagnostic: Presence or absence does not confirm or exclude diagnosis
- Other findings: May reveal stress fracture, tumor, or arthritic changes
- Lateral view: Best view for assessing heel spur and soft tissue thickness
- Weight-bearing: Preferred for assessing foot alignment and arch height
- Bilateral comparison: May be helpful in assessing arch differences
Ultrasound
- Non-invasive, no radiation
- Dynamic assessment: Can assess fascia with foot in different positions
- Cost-effective: Less expensive than MRI
- Readily available: Can be performed in clinic
- Guided injections: Allows real-time visualization for injection therapy
- Fascial thickening: Normal fascia less than 4mm; plantar fasciitis typically over 4mm (often 5-7mm)
- Hypoechoic appearance: Loss of normal fibrillar pattern, indicating degeneration
- Perifascial edema: Fluid around the fascia
- Power Doppler: Increased vascularity suggests active process (though less common given degenerative nature)
Plantar fascia thickness over 4mm on ultrasound has sensitivity of 80-95% and specificity of 80-85% for plantar fasciitis. Measurement should be taken at the fascial origin from the medial calcaneal tubercle in sagittal plane.
Differential findings on ultrasound:
- Fascia rupture: Discontinuity of fascia, often with hematoma
- Heel pad atrophy: Thinning of the normal 2cm heel fat pad
- Nerve compression: Hypoechoic mass or swelling along nerve course
- Plantar fibroma: Hypoechoic nodule within the plantar fascia (more distal)
Magnetic Resonance Imaging (MRI)
- Atypical presentation with concern for alternative diagnosis
- Failed conservative treatment over 6 months
- Preoperative planning in rare surgical candidates
- Suspected stress fracture, tumor, or infection
- Nerve entrapment evaluation
- Fascial thickening: Greater than 4mm, often 5-8mm
- Increased T2 signal: Indicates edema and degeneration within the fascia
- Perifascial edema: High signal around fascia on fluid-sensitive sequences
- Calcaneal bone marrow edema: Seen in severe cases at the fascial attachment site
- Fascial discontinuity: Indicates partial or complete rupture (complication)
- Baxter nerve entrapment: Edema or mass between abductor hallucis and quadratus plantae
- Tarsal tunnel syndrome: Nerve enlargement or mass in tarsal tunnel
- Calcaneal stress fracture: Bone marrow edema in calcaneal body
- Tumor: Mass lesion with characteristic signal patterns
- Infection: Bone marrow edema with cortical destruction and soft tissue involvement
Multimodal Imaging Comparison


Laboratory Tests
Generally not required for typical plantar fasciitis.
- Bilateral symptoms with systemic features (inflammatory arthropathy)
- Concern for seronegative spondyloarthropathy
- Atypical presentation
- HLA-B27: If suspecting ankylosing spondylitis or reactive arthritis
- Inflammatory markers: ESR, CRP if concerned about inflammatory or infectious process
- Rheumatoid factor, anti-CCP: If rheumatoid arthritis suspected
- Uric acid: If gout is in differential (though rarely causes isolated heel pain)
Management
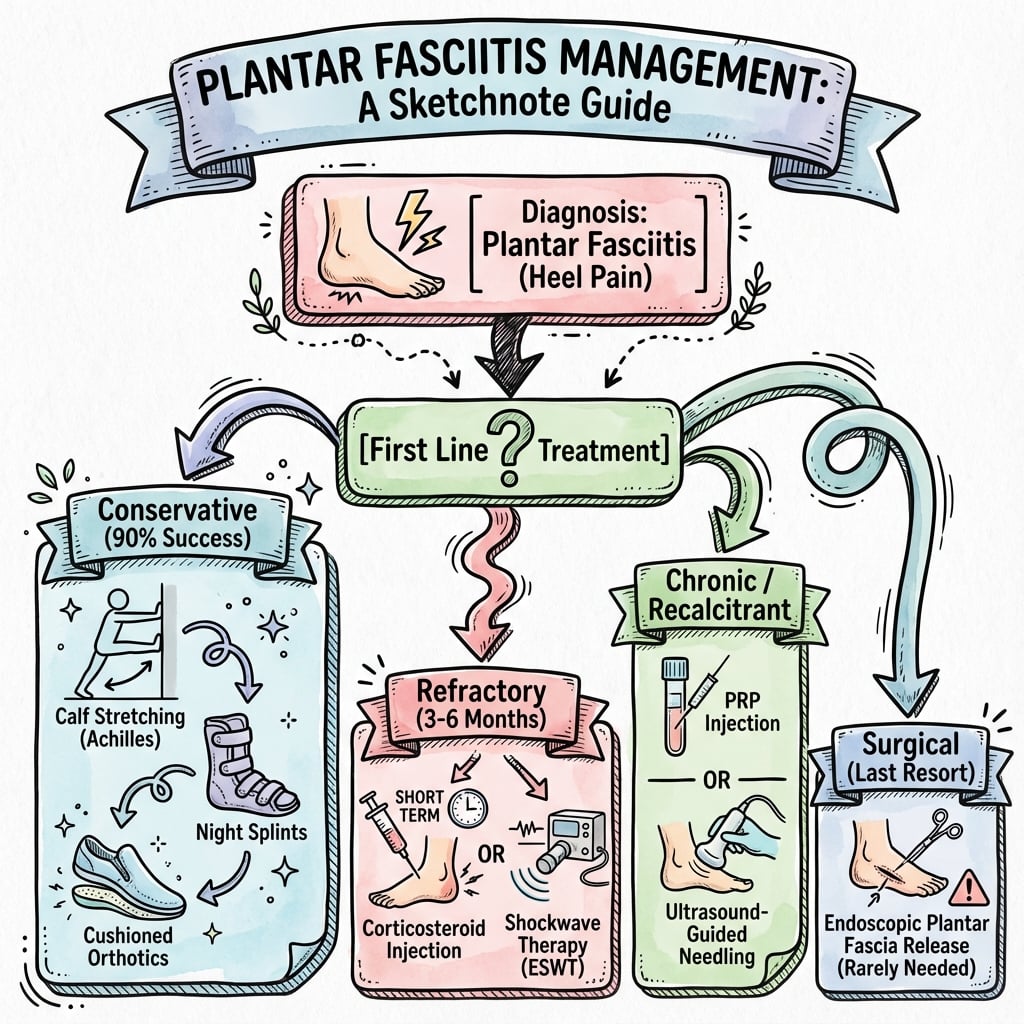
Treatment Philosophy
90% of patients improve with conservative management within 12 months. The goal is to address biomechanical factors, reduce load on the fascia, and allow the degenerative process to resolve. A structured, stepwise approach is recommended with patience and realistic expectations.
Initial treatment:
- Activity modification (reduce standing, running)
- Ice massage (15 minutes, 3-4 times daily)
- NSAIDs (2-week course for pain relief, not long-term)
- Stretching exercises (calf and plantar fascia)
- Supportive footwear with cushioned heels
- Avoid barefoot walking
Expected outcome: 20% significant improvement by 6 weeks.
Escalate conservative treatment:
- Formal physical therapy referral
- Night splints (maintain dorsiflexion overnight)
- Custom orthoses or prefabricated arch supports
- Low-dye taping technique
- Continue stretching program (3 times daily)
- Consider extracorporeal shockwave therapy (ESWT)
Expected outcome: Additional 30-40% improvement by 3 months (total 60% improved).
Advanced conservative therapies:
- ESWT if not already tried (2000-4000 shocks)
- Consider corticosteroid injection (use sparingly)
- Platelet-rich plasma (PRP) injection (emerging evidence)
- Intensive PT with iontophoresis
- Assess footwear and biomechanics
- Weight loss if BMI over 30
Expected outcome: Additional 20-25% improvement by 6 months (total 80-85% improved).
Final conservative measures:
- Repeat injection therapy if single prior injection
- Trial of different orthoses or footwear
- Consider walking boot for 4-6 weeks (rarely needed)
- Rule out alternative diagnoses with imaging
- Reassess compliance with stretching and PT
Expected outcome: Additional 5-10% improvement by 12 months (total 90% improved).
Criteria for surgery:
- Failed ALL conservative measures above
- Symptoms significantly impair quality of life
- Minimum 6-12 months of treatment
- Imaging confirms no alternative diagnosis
- Patient motivated and understands risks
Surgical success: 70-90% improvement with plantar fascia release.
Specific Conservative Interventions
1. Stretching Exercises (First-Line, Essential)
- Technique: Stand facing wall, affected leg behind, knee straight, lean forward until stretch felt in calf
- Duration: Hold 30 seconds, repeat 3 times
- Frequency: 3 times daily (morning, midday, evening)
- Soleus variation: Repeat with knee bent to isolate soleus
- Evidence: High-quality evidence supporting stretching as cornerstone of treatment
- Technique: Seated, cross affected foot over opposite knee, pull toes back toward shin while massaging arch
- Duration: Hold 10 seconds, repeat 10 times
- Frequency: Before first steps in morning and before standing after prolonged sitting
- Evidence: Specific fascia stretching may be superior to calf stretching alone
A landmark RCT by DiGiovanni et al. demonstrated that plantar fascia-specific stretching was superior to standard Achilles stretching for pain relief and functional improvement at 8 weeks. This has become the foundation of conservative treatment protocols.
2. Orthoses and Footwear Modifications
- Silicon heel cups: Reduce impact forces on heel
- Gel inserts: Provide cushioning
- Taping: Low-dye taping supports arch and reduces fascia strain
- Over-the-counter arch supports: Readily available, inexpensive
- Cushioned insoles: Reduce heel impact
- Evidence: Moderate evidence for short-term benefit (3-6 months)
- Semi-rigid orthoses: Provide arch support and control pronation
- Indications: Significant pes planus or cavus, failed prefabricated orthoses
- Cost: More expensive but may be worth trial in refractory cases
- Evidence: Limited evidence that custom is superior to prefabricated
- Avoid: High heels, flip-flops, worn-out shoes, flat unsupportive shoes
- Prefer: Well-cushioned athletic shoes, shoes with arch support and heel counter
- Running shoes: Replace every 400-500 miles
3. Night Splints
Mechanism: Maintain ankle in neutral or slight dorsiflexion overnight, preventing fascia from contracting and reducing "first-step" pain in morning.
- Posterior leaf spring: L-shaped splint maintaining dorsiflexion
- Sock-type splints: More comfortable, lower profile
- Adjustable: Allow gradual increase in dorsiflexion stretch
- Wear: Nightly for 1-3 months
- Compliance: Key challenge - 50% discontinue due to discomfort
- Evidence: Moderate evidence for effectiveness when tolerated
4. Extracorporeal Shockwave Therapy (ESWT)
Mechanism: High-energy acoustic waves induce microtrauma, stimulating neovascularization and healing response in degenerative tissue.
- Energy level: 0.1-0.2 mJ/mm² (low to medium energy)
- Shocks per session: 2000-4000 shocks
- Sessions: Typically 3 sessions, 1-2 weeks apart
- Anesthesia: Usually performed without anesthesia (mild discomfort)
- Meta-analyses: Show moderate benefit over placebo for pain reduction
- Success rate: 60-80% improvement in refractory cases
- Timing: Best used after 3-6 months of failed conservative care
- Cochrane review: Moderate evidence for effectiveness
- Infection at treatment site
- Malignancy
- Pregnancy
- Coagulopathy or anticoagulation
- Open growth plates in children
- Multicentre, double-blind, placebo-controlled FDA trial of 250 subjects with recalcitrant plantar fasciitis
- Three sessions of 2000 focused impulses (0.25 mJ/mm²) reduced the composite VAS heel-pain score by 69.2% versus 34.5% with placebo (p=0.0027)
- Roles and Maudsley score also significantly favoured ESWT (p=0.0006); success rates 50-65%
- Only temporary pain and swelling were observed as device-related adverse events
Focused versus Radial Shockwave — and How Energy Is Classified
ESWT is not a single modality, and the distinction is examinable because the level-I evidence above applies to one specific type:
- Focused ESWT (true shockwave): An electrohydraulic, electromagnetic or piezoelectric source generates a genuine shockwave that is geometrically converged so that peak energy is delivered at a chosen focal depth in the deep tissue. It reaches higher energy flux density and is the modality used in the Gollwitzer level-I trial (0.25 mJ/mm²). Higher-energy focused protocols can be uncomfortable and some centres add local anaesthesia, although the Gollwitzer trial notably demonstrated efficacy without it (and there is a theoretical concern that anaesthesia may blunt the analgesic effect).
- Radial pressure-wave therapy (rESWT): A pneumatically driven projectile produces a radially dispersing pressure wave whose energy is maximal at the skin surface and falls off with depth. It is lower energy, delivered without anaesthesia, cheaper and more widely available, but its evidence base is more mixed than that for focused ESWT.
Energy flux density (EFD, mJ/mm²) is how dose is described and conventionally banded into low (roughly below 0.1), medium (roughly 0.1 to 0.3) and high (roughly above 0.3) energy — the local low-to-medium figures quoted above sit in the radial/low-energy range, whereas the recalcitrant-disease RCT evidence used a higher focused dose.
Mechanism (mechanotransduction): Acoustic energy is converted into a biological signal that produces controlled microtrauma, upregulates angiogenic and growth factors (including VEGF and endothelial nitric oxide synthase) to drive neovascularisation of degenerate fascia, and provides analgesia by hyperstimulation of nociceptors and modulation of substance P — fitting the degenerative (fasciosis) rather than inflammatory model of the disease.
When asked about shockwave therapy, separate focused from radial: the strongest (level-I) evidence for recalcitrant plantar fasciitis is for focused, higher-energy ESWT (Gollwitzer 2015, 0.25 mJ/mm², success 50-65%), and dose is reported as energy flux density in mJ/mm². Radial pressure-wave therapy is lower energy, needs no anaesthesia and is more accessible, but has a weaker evidence base — do not quote the focused-ESWT trial results as if they apply to a radial device.
5. Activity Modification
- Limit standing: Take regular sitting breaks if occupation requires prolonged standing
- Modify exercise: Replace running with swimming, cycling, or elliptical
- Avoid barefoot walking: Always wear supportive footwear, even at home
- Weight management: Target BMI under 30 if overweight
- 10% rule: Increase activity by no more than 10% per week
- Cross-training: Vary activities to reduce repetitive stress
- Appropriate surfaces: Avoid hard surfaces; prefer grass or synthetic tracks
This completes the conservative management overview.
Surgical Management
Indications for Surgery
Strict criteria must be met before considering surgical intervention:
- Failed comprehensive conservative treatment for minimum 6-12 months
- All non-operative measures attempted: stretching, PT, orthoses, night splints, ESWT, and at least one injection
- Imaging confirmation: No alternative diagnosis (MRI if needed)
- Significant functional impairment: Pain limiting activities of daily living
- Patient motivated and compliant: Understanding of postoperative rehabilitation
- Realistic expectations: Surgery is not guaranteed success
- Active infection
- Peripheral neuropathy (diabetic neuropathy increases risk of complications)
- Venous insufficiency or PAD (poor healing)
- Inflammatory arthropathy (may have systemic component)
- Worker's compensation or litigation (poorer outcomes)
- Non-compliance with prior treatment
Only 10% of plantar fasciitis patients are surgical candidates after appropriate conservative management. Surgery should be considered a last resort for chronic, refractory cases only.
Surgical Options
Open Plantar Fascia Release
- Failed conservative treatment over 6-12 months
- Surgeon preference or lack of endoscopic equipment
- Need for nerve decompression (Baxter nerve)
- Concern for atypical anatomy or pathology
- Supine with bump under ipsilateral hip
- Tourniquet on thigh
- Foot and ankle prepped and draped
- Medial longitudinal incision: 3-4 cm incision centered over medial calcaneal tubercle
- Start just distal to tubercle, extend distally along medial arch
- Avoid plantar surface to prevent painful scar
- Incise skin and subcutaneous tissue
- Identify abductor hallucis muscle along medial border
- Retract abductor hallucis plantarly to expose plantar fascia origin
- Identify thick, glistening white fascia inserting onto medial tubercle
- Partial release only: Release medial 50% of fascia width
- Transect fascia sharply 1-2 cm from calcaneal origin
- Preserve lateral 50%: Essential to prevent lateral column overload and arch collapse
- Palpate release with finger to confirm adequate release but lateral half intact
- Identify first branch of lateral plantar nerve (Baxter nerve) deep between abductor hallucis and quadratus plantae
- Release fascia compressing nerve if entrapment suspected
- Decompress nerve distally to medial calcaneal tuberosity
- Do NOT routinely excise - spur is incidental finding
- If large and prominent, may remove with rongeur
- Not necessary for symptom relief
- Irrigate wound
- Close subcutaneous layer with absorbable suture
- Skin closure with non-absorbable suture or staples
- Apply soft dressing and posterior splint in neutral
- Weight-bearing: Non-weight-bearing or toe-touch for 2 weeks, then progressive weight-bearing in boot
- Immobilization: Posterior splint or boot for 2-4 weeks
- Range of motion: Gentle ankle ROM exercises starting at 2 weeks
- Physical therapy: Formal PT at 4-6 weeks for strengthening
- Return to sport: 3-6 months depending on activity level
This completes the open release technique description.
Surgical Outcomes
- Overall: 70-90% of patients report good to excellent outcomes after plantar fascia release
- Pain relief: 80-85% achieve significant pain reduction
- Return to activity: Most return to normal activities by 3-6 months
- Endoscopic vs open: Similar outcomes in experienced hands; endoscopic may have faster return
- Appropriate patient selection (failed all conservative measures)
- Correct diagnosis (no alternative pathology)
- Partial (not complete) fascia release
- Compliance with postoperative rehabilitation
- Non-worker's compensation cases
- Incomplete conservative trial
- Worker's compensation or litigation
- Secondary gain issues
- Peripheral neuropathy or systemic disease
- Complete fascia release (causes new problems)
- Plantar fasciopathy affects roughly one in ten people in their lifetime, and around 90% resolve within 12 months with conservative care
- Eccentric calf stretching combined with fascia-specific stretching is the non-operative treatment of choice for chronic disease
- Medial open release of approximately the medial third of the fascia plus release of the first branch of the lateral plantar nerve is the most accepted surgical option
- Isolated proximal medial gastrocnemius release achieves excellent results for refractory cases without the complications of plantar fasciotomy
Complications
Conservative Treatment Complications
- Plantar fascia rupture (5-10%): Sudden relief of pain, followed by arch collapse, lateral column pain, and worse function
- Fat pad atrophy: Permanent thinning of heel fat pad if injection misplaced
- Skin depigmentation: More common in darker-skinned patients
- Infection: Rare with sterile technique
- Hyperglycemia: Transient in diabetic patients
- Pain during treatment: Usually mild and tolerable
- Bruising: Temporary, resolves in 1-2 weeks
- Rare: Nerve injury, skin burns (very rare)
- Poor compliance: 50% discontinue due to discomfort
- Skin irritation: Friction at points of contact
- Calf cramping: From prolonged dorsiflexion stretch
Surgical Complications
- Nerve injury: Baxter nerve (lateral plantar nerve) injury causing lateral heel numbness or burning pain
- Incomplete release: Under-release fails to relieve symptoms
- Excessive release: Over-release (more than 50%) causes lateral column overload
- Vascular injury: Rare; medial plantar artery at risk
- Wound infection: 1-2% incidence
- Hematoma: Usually resolves spontaneously
- Wound dehiscence: More common in diabetics, smokers, or with excessive early activity
- Deep vein thrombosis: Rare; consider prophylaxis in high-risk patients
- Lateral column pain and overload (10-15%): From excessive release (more than 50%), causes lateral foot pain and stress fractures
- Arch collapse: Loss of medial longitudinal arch from complete release
- Continued heel pain (10-30%): Incomplete release, scar tissue, or incorrect diagnosis
- Calcaneal stress fracture: Rare; from altered biomechanics post-release
- Tarsal tunnel syndrome: From scarring around posterior tibial nerve
- Neuromas: Entrapment of small sensory nerves in scar tissue
- Painful scar: Especially if incision placed on plantar surface
Lateral column overload syndrome is the most serious complication of plantar fascia release. It results from releasing more than 50% of the fascia width, causing loss of arch support, lateral foot pain, cuboid stress fractures, and peroneal tendinitis. This complication can be more disabling than the original plantar fasciitis. Prevention is essential - never release more than 50% of fascia.
Plantar Fascia Rupture (Non-Surgical)
- Corticosteroid injection (most common)
- Acute trauma in chronically degenerated fascia
- Spontaneous in severe plantar fasciitis
- Sudden "pop" or tearing sensation in arch
- Immediate relief of heel pain (diagnostic clue)
- Acute arch collapse: Foot flattens
- Bruising and swelling: Develops over 24-48 hours along medial arch
- New lateral column pain: From altered biomechanics
- Clinical: History of pop, sudden relief of plantar heel pain, new arch collapse
- Ultrasound: Discontinuity of fascia, hematoma
- MRI: Fascial disruption with surrounding edema

- Conservative: Most ruptures are treated non-operatively
- Boot immobilization: 4-6 weeks in walking boot
- Arch support: Custom orthoses to support collapsed arch
- Activity modification: Avoid high-impact activities for 3-6 months
- Physical therapy: Strengthen intrinsic foot muscles, peroneal tendons
- Surgical repair: Rarely needed; consider if complete rupture with severe symptoms
- Variable outcomes: Some patients do well, others develop chronic lateral column pain
- Arch may not fully recover
- Return to sport often delayed 6-12 months
Postoperative Rehabilitation
Immediate Postoperative Period (0-2 Weeks)
- Weight-bearing: Non-weight-bearing or toe-touch weight-bearing in boot or splint
- Immobilization: Posterior splint or walking boot
- Elevation: Keep foot elevated above heart level to reduce swelling
- Ice: Apply ice 15-20 minutes every 2-3 hours
- Wound care: Keep dressing clean and dry until suture removal at 10-14 days
- Pain management: Oral analgesics as needed
- Weight-bearing: Protected weight-bearing as tolerated in surgical shoe or boot
- Earlier mobilization: Small incisions allow faster recovery
- Suture removal: 7-10 days
Rehabilitation Phase (2-6 Weeks)
- Week 2-4: Gradual increase to full weight-bearing in boot
- Week 4-6: Transition from boot to supportive athletic shoe
- Gentle ankle ROM: Begin at 2 weeks (dorsiflexion, plantarflexion, circumduction)
- Avoid forced dorsiflexion: To protect healing fascia
- Start formal PT at 2-4 weeks
- Goals: Restore ROM, begin gentle strengthening, normalize gait
Strengthening Phase (6-12 Weeks)
- Intrinsic foot muscles: Towel curls, marble pickups
- Calf strengthening: Heel raises (bilateral progressing to unilateral)
- Peroneal strengthening: Resistance band eversion exercises
- Balance training: Single-leg stance, wobble board
- Low-impact activities: Walking, swimming, cycling at 6-8 weeks
- Gradual progression: 10% increase in activity per week
Return to Sport Phase (3-6 Months)
- Running: Begin interval training at 3 months if pain-free with walking
- Jumping and cutting: Delay until 4-6 months
- Gradual return: Use 10% rule for increasing activity
- Stretching: Continue gastrocnemius and plantar fascia stretching indefinitely
- Footwear: Supportive shoes with arch support
- Orthoses: May need continued use of arch supports
- Open release: 4-6 months for return to full unrestricted activity
- Endoscopic release: 3-4 months for return to full activity
Outcomes
Natural History and Conservative Outcomes
- Self-limiting: 80-90% resolve within 12-18 months with conservative treatment
- 6-month outcomes: 70% improved with structured conservative protocol
- 12-month outcomes: 85-90% satisfied with conservative management alone
Treatment-Specific Outcomes
- Success Rate
- 70-80%
- Time to Effect
- 6-8 weeks
- Duration of Benefit
- Long-term if maintained
- Success Rate
- 60-70%
- Time to Effect
- 4-8 weeks
- Duration of Benefit
- Variable
- Success Rate
- 70-85%
- Time to Effect
- 1-2 weeks
- Duration of Benefit
- 3-6 months
- Success Rate
- 60-75%
- Time to Effect
- 6-12 weeks
- Duration of Benefit
- 12+ months
- Success Rate
- 70-80%
- Time to Effect
- 8-12 weeks
- Duration of Benefit
- 12+ months
- Success Rate
- 75-90%
- Time to Effect
- 6-12 weeks
- Duration of Benefit
- Long-term
- Success Rate
- 80-90%
- Time to Effect
- 3-6 months
- Duration of Benefit
- Long-term
Surgical Outcomes
- Success rate: 75-90%
- Patient satisfaction: 80-85%
- Complications: 10-15% (nerve injury, lateral column overload)
- Return to full activity: 3-6 months
- Success rate: 80-90%
- Faster recovery: 4-8 weeks to regular footwear
- Lower complication rate: 5-10%
Prognostic Factors
- Duration less than 6 months
- BMI less than 30
- No systemic inflammatory disease
- Good compliance with stretching
- Bilateral symptoms
- Workers' compensation claims
- Obesity (BMI greater than 35)
- Inflammatory arthropathy
- Previous failed surgery
Guidelines, Registries & Global Practice
Global Epidemiology
Plantar fasciopathy is one of the most common causes of inferior heel pain worldwide, affecting approximately one in ten people during their lifetime, with around 90% resolving within 12 months of conservative care (Monteagudo, EFORT Open Rev 2018, DOI). Peak incidence is in the 40-60 year age group. The dominant, modifiable risk factors are consistent across populations: a matched case-control study found reduced ankle dorsiflexion the strongest factor (odds ratio 23.3 for ≤0° versus over 10°), with obesity (BMI over 30: OR 5.6) and prolonged occupational weight-bearing (OR 3.6) also independently associated (Riddle, JBJS Am 2003, DOI).
Major Guidelines — Side by Side
- Diagnosis & imaging
- Clinical; imaging reserved for atypical or refractory cases
- First-line
- Stretching (fascia-specific + calf), orthoses, activity modification
- Adjuncts / second-line
- Night splints, ESWT, short-term corticosteroid (limit number due to rupture risk)
- Surgery threshold
- After failure of comprehensive conservative care (≥6 months)
- Diagnosis & imaging
- Clinical diagnosis; imaging only if diagnosis in doubt
- First-line
- Reassurance (self-limiting), footwear advice, stretching, weight loss
- Adjuncts / second-line
- Orthoses, physiotherapy; ESWT considered for persistent pain
- Surgery threshold
- Refer to specialist only after sustained failure of conservative care
- Diagnosis & imaging
- Clinical; ultrasound (fascia over 4mm) supports uncertain cases
- First-line
- Eccentric calf + fascia-specific stretching (treatment of choice)
- Adjuncts / second-line
- ESWT for chronic disease; injections used cautiously
- Surgery threshold
- Medial open release of medial third + Baxter nerve release; gastrocnemius recession for selected refractory cases
There is broad international agreement on three points: the diagnosis is clinical, conservative care is first-line for at least 6-12 months, and surgery is a last resort for a small refractory minority. The main areas of genuine variation are the role and energy protocol of ESWT (more entrenched in European and US specialist practice), enthusiasm for PRP versus corticosteroid, and whether isolated gastrocnemius recession is offered as a fascia-sparing alternative to fasciotomy.
Evidence Base for Key Recommendations
- Strength
- Level I RCT
- Source
- DiGiovanni 2006, DOI
- Strength
- Level I RCT
- Source
- Gollwitzer 2015, DOI
- Strength
- Level I Cochrane
- Source
- David 2017, DOI
- Strength
- Level I Cochrane
- Source
- Hawke 2008, DOI
- Strength
- Expert consensus
- Source
- Monteagudo 2018, DOI
Registry & Surveillance Note
Plantar fasciopathy is a soft-tissue, predominantly non-operative condition, so it is not tracked by the arthroplasty/implant registries (NJR, AJRR, AOANJRR). Population-level burden is instead captured through primary-care and insurance datasets; in the USA it accounts for roughly one million patient visits annually, underscoring its public-health importance despite its benign natural history.
Global Practice Variation
In high-resource settings, refractory patients can readily access podiatry, formal physiotherapy, ESWT and image-guided injections before surgery is contemplated. In limited-resource settings, management relies more heavily on low-cost, high-value interventions — patient education, calf and fascia stretching, weight management, footwear modification and prefabricated insoles — which address the same modifiable risk factors and resolve the large majority of cases without specialist referral. Work-relatedness (prolonged standing on hard surfaces) is recognised across jurisdictions, with return-to-work and workplace-modification programmes a common feature of occupational management.
MCQ Practice Points
Q: What is the windlass mechanism and how does it relate to plantar fasciitis?
A: Passive toe dorsiflexion tightens the plantar fascia, raising the medial longitudinal arch and converting the foot to a rigid lever for push-off. This mechanism creates repetitive tension at the calcaneal origin, predisposing to degeneration. Dorsiflexion of the great toe reproduces pain (windlass test).
Q: What percentage of plantar fasciitis cases resolve with conservative management and what is the recommended duration before considering surgery?
A: 90% resolve with conservative management within 12 months. A minimum of 6-12 months of conservative treatment is mandatory before considering surgical intervention. Conservative measures include stretching, orthoses, night splints, and activity modification.
Q: What is the clinical significance of a calcaneal heel spur in a patient with plantar heel pain?
A: Heel spurs are an incidental finding present in 50% of asymptomatic individuals. They are NOT the cause of pain and do not correlate with symptom severity. The spur originates from the flexor digitorum brevis, not the plantar fascia. Spur excision is NOT routinely performed with plantar fascia release.
Q: In plantar fascia release surgery, what percentage of the fascia should be released and why?
A: Release the medial 50% ONLY. Complete release causes lateral column overload with lateral foot pain and arch collapse. The windlass mechanism is eliminated, causing push-off weakness. Partial release preserves some mechanical function while decompressing the medial insertion.
At a Glance
Plantar fasciitis is a degenerative process (not inflammatory—prefer "plantar fasciosis") causing plantar heel pain at the medial calcaneal tubercle, classically worst with first steps after rest. Histology shows myxoid degeneration and collagen necrosis, explaining limited long-term benefit from anti-inflammatory treatments. 90% resolve with conservative management within 12 months—stretching (gastrocnemius and plantar fascia), orthoses, and activity modification are first-line. A 6-12 month conservative trial is mandatory before surgery. Surgical release should preserve the lateral 50% of fascia (release medial half only) to prevent lateral column overload and arch collapse. Baxter nerve entrapment is an important differential with burning pain and night symptoms.
PLANTARPLANTAR - Risk Factors
Hook:PLANTAR reminds you of all key risk factors and the classic first-step pain pattern
STRETCHSTRETCH - Conservative Management Algorithm
Hook:STRETCH emphasizes the conservative approach and the importance of stretching exercises
RELEASERELEASE - Surgical Considerations
Hook:RELEASE guides surgical decision-making and emphasizes partial release only
504-4-50 Rule - Diagnostic Criteria
Hook:4-4-50 helps remember key diagnostic measurements and the incidental nature of heel spurs
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 48-year-old female school teacher presents with 3 months of left heel pain. She describes severe pain with the first steps in the morning that improves after walking for 10 minutes but returns after prolonged standing at work. She is otherwise healthy with BMI of 32. Examination reveals exquisite tenderness at the medial calcaneal tubercle. Ankle dorsiflexion is 5 degrees with knee extended. How would you manage this patient?”
“A 52-year-old recreational runner presents with 18 months of right heel pain despite comprehensive conservative treatment including PT, custom orthoses, night splints, two cortisone injections, and ESWT. Pain significantly limits his running and daily activities. MRI shows plantar fascia thickening to 7mm with no other pathology. He is motivated and understands recovery time. Would you offer surgery, and if so, what procedure?”
“A 45-year-old male presents with 6 months of medial heel pain that is worse at night and described as burning. Pain radiates to the lateral heel. He has undergone 3 months of PT and stretching without improvement. Examination reveals tenderness at the medial heel but also a positive Tinel sign deep between the abductor hallucis and quadratus plantae. How does this change your management?”
Key Definitions
- **Plantar fasciitis**: Degenerative condition of plantar fascia origin causing inferior heel pain - prefer term plantar fasciosis or plantar heel pain
- **Windlass mechanism**: Passive toe extension tightens fascia and raises arch - basis for windlass test
- **Baxter nerve**: First branch of lateral plantar nerve between abductor hallucis and quadratus plantae - can mimic plantar fasciitis
- **Partial release**: Surgical release of medial 50% of fascia only - complete release causes lateral column overload
Epidemiology Numbers
- **10%** lifetime incidence in population
- **40-60 years** peak age of onset
- **90%** resolve with conservative management within 12 months
- **4mm** normal plantar fascia thickness on ultrasound (over 4mm in plantar fasciitis)
- **50%** have heel spur but it is incidental finding, not cause of pain
- **70-90%** success rate with surgical release in properly selected patients
Risk Factors (PLANTAR)
- **P** - Prolonged standing/walking occupations
- **L** - Limited ankle dorsiflexion (less than 10 degrees)
- **A** - Age 40-60 years
- **N** - No arch support (pes planus or cavus)
- **T** - Training errors in runners
- **A** - Adiposity (BMI over 30)
- **R** - Reduced first step pain (classic symptom)
Clinical Diagnosis
- **First-step pain**: Severe pain with first steps in morning or after sitting (95% sensitive)
- **Point tenderness**: Medial calcaneal tubercle tenderness (most specific finding)
- **Windlass test**: Passive hallux dorsiflexion reproduces pain - positive test confirms fascia as source
- **Limited dorsiflexion**: Less than 10 degrees with knee extended is risk factor
- **Red flags**: Night pain, burning pain, radiation suggest alternative diagnosis (nerve entrapment)
Conservative Treatment Stages
- **0-6 weeks (Acute)**: Stretching (fascia-specific and gastrocnemius), ice, NSAIDs, activity modification, supportive footwear
- **6 weeks-3 months (Subacute)**: Add PT, night splints, orthoses, consider ESWT
- **3-6 months (Chronic)**: ESWT (2000-4000 shocks), consider steroid injection (max 2 due to rupture risk)
- **6-12 months (Refractory)**: Repeat injection or trial PRP, rule out alternative diagnoses with MRI
- **Over 12 months**: Consider surgery if failed ALL conservative measures
Injection Therapies
- **Steroid**: Short-term relief (1 month) but no long-term benefit; 5-10% rupture risk; max 2 injections; use medial approach to avoid fat pad
- **PRP**: Slower onset but better long-term outcomes vs steroid at 3-6 months; lower rupture risk; 2-3 mL under ultrasound guidance
- **Technique**: Medial approach under ultrasound guidance to visualize fascia and avoid fat pad injection
Surgical Indications (Strict)
- **Failed 6-12 months** of comprehensive conservative treatment
- **All measures tried**: Stretching, PT, orthoses, night splints, ESWT, at least one injection
- **Imaging confirmation**: MRI to rule out alternative diagnosis if needed
- **Significant impairment**: Pain limiting ADLs and quality of life
- **Motivated patient**: Understands recovery time and realistic expectations
Surgical Technique Principles
- **Partial release only**: Release medial 50% of fascia - NEVER complete release
- **Complete release complication**: Causes lateral column overload, arch collapse, worse pain than original problem
- **Open approach**: 3-4cm medial incision, visualize and release medial half, allows Baxter nerve decompression
- **Endoscopic**: Medial and lateral 1cm portals, faster recovery but cannot address nerve
- **Heel spur**: Do NOT routinely excise - incidental finding not requiring removal
- **Baxter nerve**: Decompress if burning pain, night pain, or positive Tinel sign suggesting entrapment
Surgical Outcomes
- **Success**: 70-90% good to excellent outcomes in properly selected patients
- **Recovery**: 3-4 months return to running (endoscopic) or 4-6 months (open)
- **Continued pain**: 10-30% have residual symptoms despite surgery
- **Complications**: Lateral column overload (10-15% if over-released), nerve injury, infection, continued pain
Differential Diagnosis
- **Baxter nerve entrapment**: Burning pain, night pain, radiation to lateral heel, Tinel sign deep between abductor hallucis and quadratus plantae
- **Tarsal tunnel**: Posterior tibial nerve compression, Tinel posterior to medial malleolus, plantar foot radiation
- **Calcaneal stress fracture**: Pain with medial-lateral squeeze, history of increased activity
- **Fat pad atrophy**: Diffuse heel pain, history of steroid injections, no focal tenderness
- **Inflammatory arthritis**: Bilateral symptoms, morning stiffness over 30 minutes, systemic features
Exam Viva Pearls
- **Plantar fasciosis not fasciitis**: Histology shows degeneration (myxoid, collagen necrosis) not inflammation
- **Heel spur is incidental**: Present in 50% of plantar fasciitis but also 15-25% of asymptomatic people - not the cause
- **Fascia rupture presentation**: Sudden pop, immediate relief of heel pain, arch collapse, bruising, new lateral column pain
- **50% rule**: Never release more than 50% of fascia width to prevent lateral column overload
- **Baxter nerve anatomy**: First branch of lateral plantar nerve between abductor hallucis and quadratus plantae - important differential
- **Conservative is key**: 90% resolve without surgery - set realistic 6-12 month timeline expectations
Evidence Base and Guidelines
- Eleven RCTs (1332 participants), of which five evaluated custom orthoses for plantar fasciitis
- Only 'silver level' evidence for custom orthoses in plantar fasciitis — it is unclear whether they outperform sham or prefabricated devices
- Custom orthoses were a safe intervention across all studies
- Supports custom orthoses as an adjunct rather than a stand-alone cure for plantar heel pain
- Two-year follow-up of an RCT in which the tissue-specific plantar fascia-stretching protocol was favoured over Achilles stretching at 8 weeks
- All patients adopted the fascia-specific stretch after 8 weeks; by 2 years there was no significant between-group difference, confirming durable benefit
- 92% of patients reported satisfaction and 94% reported a decrease in pain at 2 years
- Establishes tissue-specific plantar fascia stretching as the key, inexpensive component of conservative treatment
- Matched case-control study (50 cases, 100 controls) identifying independent risk factors for plantar fasciitis
- Reduced ankle dorsiflexion was the strongest factor — ≤0° gave an odds ratio of 23.3 (95% CI 4.3-124.4) versus over 10° of dorsiflexion
- BMI over 30 kg/m² conferred an odds ratio of 5.6 (95% CI 1.9-16.6)
- Spending most of the workday weight-bearing gave an odds ratio of 3.6 (95% CI 1.3-10.1)
- Histological review of 50 heel-spur surgery specimens for chronic plantar fasciitis
- Findings showed myxoid degeneration, fascial fragmentation and bone-marrow vascular ectasia — not inflammation
- Supports the term 'plantar fasciosis': a degenerative process rather than a true fasciitis
- Authors warn serial corticosteroid injection into degenerative fascia should be re-evaluated given the risk of rupture
- Case series of 20 patients (23 feet) undergoing endoscopic plantar fascia release with mean 47-month follow-up
- AOFAS hindfoot score improved from 66 to 88 and Maryland Foot Score from 62 to 83 (both p<0.05)
- Patients with symptoms longer than 2 years before surgery and workers'-compensation patients had inferior results
- Obesity had no negative effect on outcome; supports careful patient selection for endoscopic release
References
-
Hawke F, Burns J, Radford JA, du Toit V. Custom-made foot orthoses for the treatment of foot pain. Cochrane Database Syst Rev. 2008;(3):CD006801.
-
DiGiovanni BF, Nawoczenski DA, Malay DP, et al. Plantar fascia-specific stretching exercise improves outcomes in patients with chronic plantar fasciitis. A prospective clinical trial with two-year follow-up. J Bone Joint Surg Am. 2006;88(8):1775-1781.
-
Tong KB, Furia J. Economic burden of plantar fasciitis treatment in the United States. Am J Orthop. 2010;39(5):227-231.
-
Riddle DL, Pulisic M, Pidcoe P, Johnson RE. Risk factors for plantar fasciitis: a matched case-control study. J Bone Joint Surg Am. 2003;85(5):872-877.
-
Lemont H, Ammirati KM, Usen N. Plantar fasciitis: a degenerative process (fasciosis) without inflammation. J Am Podiatr Med Assoc. 2003;93(3):234-237.
-
McMillan AM, Landorf KB, Barrett JT, Menz HB, Bird AR. Diagnostic imaging for chronic plantar heel pain: a systematic review and meta-analysis. J Foot Ankle Res. 2009;2:32.
-
Gollwitzer H, Saxena A, DiDomenico LA, et al. Clinically relevant effectiveness of focused extracorporeal shock wave therapy in the treatment of chronic plantar fasciitis: a randomized, controlled multicenter study. J Bone Joint Surg Am. 2015;97(9):701-708.
-
Bazaz R, Ferkel RD. Results of endoscopic plantar fascia release. Foot Ankle Int. 2007;28(5):549-556.
-
David JA, Sankarapandian V, Christopher PR, Chatterjee A, Macaden AS. Injected corticosteroids for treating plantar heel pain in adults. Cochrane Database Syst Rev. 2017;(6):CD009348.
-
Monto RR. Platelet-rich plasma efficacy versus corticosteroid injection treatment for chronic severe plantar fasciitis. Foot Ankle Int. 2014;35(4):313-318.
-
Neufeld SK, Cerrato R. Plantar fasciitis: evaluation and treatment. J Am Acad Orthop Surg. 2008;16(6):338-346.
-
Monteagudo M, de Albornoz PM, Gutierrez B, Tabuenca J, Alvarez I. Plantar fasciopathy: A current concepts review. EFORT Open Rev. 2018;3(8):485-493.
-
Davies MS, Weiss GA, Saxby TS. Plantar fasciitis: how successful is surgical intervention? Foot Ankle Int. 1999;20(12):803-807.
-
Gollwitzer H, Saxena A, DiDomenico LA, et al. Clinically relevant effectiveness of focused extracorporeal shock wave therapy in the treatment of chronic plantar fasciitis: a randomized, controlled multicenter study. J Bone Joint Surg Am. 2015;97(9):701-708.
-
League AC. Current concepts review: plantar fasciitis. Foot Ankle Int. 2008;29(3):358-366.
-
Cole C, Seto C, Gazewood J. Plantar fasciitis: evidence-based review of diagnosis and therapy. Am Fam Physician. 2005;72(11):2237-2242.
-
Thomas JL, Christensen JC, Kravitz SR, et al. The diagnosis and treatment of heel pain: a clinical practice guideline-revision 2010. J Foot Ankle Surg. 2010;49(3 Suppl):S1-19.
-
Goff JD, Crawford R. Diagnosis and treatment of plantar fasciitis. Am Fam Physician. 2011;84(6):676-682.
-
Buchbinder R. Clinical practice. Plantar fasciitis. N Engl J Med. 2004;350(21):2159-2166.
-
Cornwall MW, McPoil TG. Plantar fasciitis: etiology and treatment. J Orthop Sports Phys Ther. 1999;29(12):756-760.