Benign Proliferative Synovial Disorder | Locally Aggressive | High Recurrence Risk
- PVNS is now classified as tenosynovial giant cell tumor (TGCT) - same pathological entity
- Benign but locally aggressive - causes cartilage and bone erosion through mechanical and enzymatic destruction
- Diffuse form has 30-50% recurrence despite complete synovectomy
- MRI characteristic: hemosiderin deposition causes blooming artifact on gradient echo sequences
- Treatment: Complete synovectomy + consider adjuvant (radiation, imatinib for CSF1R mutation)
- “PVNS and giant cell tumor of tendon sheath are the SAME disease - intra-articular vs extra-articular
- “Gold standard MRI finding: Low signal on T1 and T2 due to hemosiderin (blooming on GRE)
- “CSF1-COL6A3 fusion drives pathogenesis - CSF1R inhibitors (imatinib) for recurrent disease
- “Arthroscopic synovectomy alone has higher recurrence than open - consider adjuvant radiation
PVNS equals TGCT (tenosynovial giant cell tumor). Driven by CSF1-COL6A3 fusion causing CSF1 overexpression. This recruits inflammatory cells and creates the proliferative synovial mass.
Hemosiderin blooming on MRI. Low signal on T1 and T2 weighted sequences. Blooming artifact on gradient echo (GRE) sequences is pathognomonic for hemosiderin deposition.
Complete synovectomy is key. Diffuse disease requires open or combined arthroscopic-open approach. Consider adjuvant radiation (20 Gy) or imatinib for recurrence prevention.
Localized form recurs in under 10%. Diffuse form recurs in 30-50% despite complete excision. Recurrence peaks at 2-3 years post-op - long surveillance needed.
- Classification
- Localized (nodular) PVNS
- Treatment
- Arthroscopic local excision
- Key Pearl
- Low recurrence (under 10%) if complete excision
- Classification
- Diffuse PVNS (villonodular)
- Treatment
- Open synovectomy + consider adjuvant
- Key Pearl
- High recurrence (30-50%) - counsel about surveillance
- Classification
- Recurrent diffuse PVNS
- Treatment
- Re-synovectomy + adjuvant (radiation or imatinib)
- Key Pearl
- Consider CSF1R inhibitor (imatinib) for multiple recurrences
Overview and Epidemiology
PVNS (pigmented villonodular synovitis) is a rare benign proliferative disorder of the synovium that is locally aggressive and causes significant joint destruction if untreated. It is now recognized as part of the tenosynovial giant cell tumor (TGCT) spectrum - the same pathological process occurring intra-articularly (PVNS) versus extra-articularly (giant cell tumor of tendon sheath). Despite being benign, diffuse PVNS has high recurrence rates (30-50%) and can lead to premature arthritis requiring joint replacement in young adults.
- Age: Peak incidence 20-40 years (young adults)
- Gender: Slight female predominance (1.5-2:1)
- Laterality: Usually monoarticular (95%)
- Race: No racial predilection
- Joint destruction: Progressive cartilage and bone erosion
- Recurrence: 30-50% for diffuse form despite synovectomy
- Disability: Chronic pain, swelling, mechanical symptoms
- Arthroplasty: May require joint replacement in young patients
The disease shows no hereditary pattern and no clear environmental or genetic risk factors have been identified. The hallmark is chronic monoarticular synovitis with recurrent hemarthrosis.
Pathophysiology and Molecular Biology
Despite the name "synovitis", PVNS is NOT an inflammatory arthritis. It is a clonal neoplastic proliferation driven by CSF1-COL6A3 fusion causing CSF1 (colony stimulating factor 1) overexpression. CSF1 recruits inflammatory cells (macrophages, giant cells) that create the mass and cause joint destruction.
- Mechanism
- Chromosomal translocation t(1;2) drives CSF1 overexpression
- Clinical Consequence
- Neoplastic cells recruit inflammatory infiltrate
- Mechanism
- CSF1R on macrophages binds CSF1, recruiting inflammatory cells
- Clinical Consequence
- Mass effect from macrophage and giant cell infiltration
- Mechanism
- Friable vascular tissue bleeds into joint
- Clinical Consequence
- Hemosiderin deposition (iron) causes MRI blooming artifact
- Mechanism
- Macrophages release metalloproteases (MMPs)
- Clinical Consequence
- Cartilage degradation and bone erosion
- Multinucleated giant cells: Hallmark (but reactive, not neoplastic)
- Hemosiderin-laden macrophages: From recurrent hemorrhage
- Mononuclear stromal cells: The neoplastic component (CSF1 expressing)
- Foam cells: Lipid-laden macrophages
- Villous or nodular architecture: Synovial proliferation pattern
- CSF1R inhibitors (imatinib, pexidartinib) block macrophage recruitment
- Effective for recurrent disease
- Reduces tumor burden and symptoms
- FDA-approved pexidartinib for TGCT (2019)
The key pathological distinction is localized versus diffuse forms, which have different prognosis and recurrence risk.
HEMOSIDERINPVNS Pathological Features
Hook:HEMOSIDERIN - the pathological pigment that defines PVNS on imaging and histology!
Classification and Clinical Forms
Localized (Nodular) PVNS
- Discrete nodular mass, often pedunculated
- Focal mechanical symptoms (locking, catching)
- Less hemarthrosis than diffuse form
- Better prognosis with local excision
- Well-defined lobulated mass
- Blooming artifact on GRE MRI
- Less extensive bone and cartilage erosion
- Arthroscopic local excision
- Lower recurrence (under 10%)
- No adjuvant therapy usually needed
Localized PVNS behaves more like a benign tumor amenable to complete excision.
The critical exam point: Localized PVNS behaves like a benign tumor (low recurrence with complete excision), while diffuse PVNS behaves like a locally aggressive malignancy (high recurrence despite aggressive synovectomy). This distinction guides treatment intensity and patient counseling.
Clinical Presentation and Assessment
- Symptoms: Chronic joint swelling (months to years)
- Hemarthrosis: Recurrent bloody effusions (not traumatic)
- Pain: Dull aching pain, worse with activity
- Mechanical symptoms: Locking, catching (localized form)
- Stiffness: Progressive loss of range of motion
- Effusion: Chronic joint swelling, often tense
- Range of motion: Reduced, especially terminal flexion
- Palpable mass: May feel discrete nodule (localized)
- Synovial thickening: Diffuse boggy synovium (diffuse form)
- Instability: Usually absent (vs inflammatory arthritis)
Young adult with chronic monoarticular swelling and recurrent hemarthrosis - differential includes rheumatoid arthritis (RA), hemophilic arthropathy, tuberculous arthritis, and pigmented villonodular synovitis. The key distinguishing features: PVNS has hemosiderin blooming on MRI, lacks systemic inflammatory markers, and shows characteristic gross pathology (rust-brown synovium).
Joint Distribution:
- Knee (80% of cases) - most common site
- Hip (10-15%) - more challenging diagnosis and treatment
- Ankle, shoulder, elbow (rare, each under 5%)
- Temporomandibular joint (case reports)
The key clinical clue is monoarticular chronic synovitis with recurrent hemarthrosis in a young adult.
Imaging and Diagnosis
Diagnostic Imaging Protocol
Initial assessment: May show soft tissue swelling, joint effusion, bone erosions (late finding). Often normal in early disease.
Key findings:
- Soft tissue mass (if large)
- Bone erosions on both sides of joint (subchondral cysts)
- Preserved joint space (until late)
- No calcification (unlike synovial chondromatosis)
Diagnostic MRI features: Low signal on T1 and T2 weighted sequences due to hemosiderin. Blooming artifact on gradient echo (GRE) or susceptibility-weighted imaging (SWI) is pathognomonic.
Sensitivity/Specificity: Over 90% for PVNS diagnosis when blooming artifact present.
Additional findings:
- Synovial thickening (nodular or diffuse)
- Joint effusion (often bloody)
- Bone erosions with sclerotic margins
- Extent of disease (critical for surgical planning)
Appearance: Bloody or serosanguinous (not clear)
Cytology: Hemosiderin-laden macrophages, multinucleated giant cells, mononuclear cells
Role: Exclude infection, crystal arthropathy, inflammatory arthritis
Indications: Atypical imaging, need to exclude malignancy
Approach: Arthroscopic synovial biopsy (safe, diagnostic)
Histology confirms: Hemosiderin, giant cells, mononuclear stromal cells

Q: What is the characteristic MRI finding in PVNS? A: Blooming artifact on gradient echo (GRE) sequences - caused by hemosiderin (iron) deposition from recurrent hemorrhage. This produces susceptibility artifact with signal dropout (blooming) that is much larger than the actual lesion size on GRE images. Low signal on T1 and T2 is also characteristic.
Differential Diagnosis
- Key Distinguishing Features
- Extra-articular location (tendon sheath), same histology as PVNS
- Imaging Differences
- No intra-articular involvement, no blooming (usually)
- Key Distinguishing Features
- Calcified loose bodies, no hemosiderin, younger age
- Imaging Differences
- Calcifications on XR, high signal on T2, no blooming
- Key Distinguishing Features
- Known hemophilia, recurrent hemarthrosis, factor deficiency
- Imaging Differences
- Similar MRI findings, but systemic disease and clotting history
- Key Distinguishing Features
- Polyarticular, positive RF/anti-CCP, systemic inflammation
- Imaging Differences
- Synovial enhancement, erosions, no blooming artifact
- Key Distinguishing Features
- MALIGNANT, aggressive bone destruction, rapid growth
- Imaging Differences
- Heterogeneous enhancement, invasion, calcification (30%)
- Key Distinguishing Features
- Chronic monoarthritis, systemic TB symptoms, positive cultures
- Imaging Differences
- Synovial enhancement, erosions, rice bodies, no blooming
The critical distinction is benign (PVNS, chondromatosis) versus malignant (synovial sarcoma) - biopsy if any doubt.
GIANTPVNS Differential Diagnosis
Hook:GIANT cells are the histological hallmark - but remember the differentials!
Management Algorithm
Localized PVNS Management
Goal: Complete excision of nodule with preservation of joint function.
Treatment Steps
Approach: Arthroscopic local excision of nodule (with margin)
Technique:
- Visualize entire nodule and stalk
- Excise with 2-3mm margin of normal synovium
- Remove in toto if possible (avoid fragmentation)
- Hemostasis critical (prevent recurrent bleeding)
Success rate: Over 90% cure with complete excision
Indications: Large nodule, difficult location (posterior knee, hip)
Approach: Mini-arthrotomy or formal arthrotomy
Advantage: Better visualization and complete excision
Protocol: Clinical and MRI surveillance every 6-12 months for 3 years
Recurrence: Under 10% for localized form
Management of recurrence: Re-excision, consider adjuvant
Localized PVNS has excellent prognosis with complete excision and low recurrence.
The paradox of diffuse PVNS: Complete synovectomy is the goal and reduces recurrence, but even with "complete" excision, recurrence rates are 30-50%. This is because microscopic disease is often left behind, and the CSF1-driven proliferation can restart. Patients must be counseled about high recurrence risk and need for long-term surveillance.
Malignant Tenosynovial Giant Cell Tumour (Malignant PVNS)
The differential table and the Murphey evidence card both allude to "malignant PVNS", and the SafetyAlert warns to "exclude malignancy", but the topic never develops this rare, important entity - a genuine exam curveball for an otherwise "benign" disease.
- It exists, and it is rare. Malignant TGCT (malignant PVNS) is a sarcomatous transformation of, or a malignant tumour arising alongside, a diffuse-type giant cell tumour. It is very rare (well under 5% of TGCT) but carries a metastatic potential and mortality quite unlike benign PVNS - so a "benign" label must never be applied without adequate sampling.
- When to suspect it. Red flags are older age at onset, a large or rapidly enlarging mass, recurrent disease that becomes more aggressive, and destructive/atypical imaging (aggressive bone destruction and soft-tissue extension beyond the usual PVNS pattern). Most malignant cases arise in recurrent, previously-benign diffuse disease rather than at first presentation.
- How it is diagnosed. By histology: alongside the typical mononuclear/hemosiderin/giant-cell background there are overtly malignant features - marked cytological atypia, high mitotic activity, atypical mitoses, spindling into a sarcomatous pattern, necrosis, and enlarged mononuclear cells. This is why an atypical, aggressive or unexpectedly recurrent lesion warrants generous biopsy and expert sarcoma pathology, not just a diagnosis of "recurrent PVNS".
- Management is that of a sarcoma. Wide surgical resection (rather than simple synovectomy), with adjuvant radiotherapy/chemotherapy and staging for metastases (lungs, nodes) via a sarcoma MDT. Prognosis is markedly worse than benign disease, with a real risk of metastasis and death.
Q: A patient with recurrent diffuse PVNS has a rapidly enlarging, destructive mass - what must you exclude? A: Malignant tenosynovial giant cell tumour (malignant PVNS) - a rare sarcomatous transformation, usually arising in recurrent diffuse disease, suggested by older age, a large/rapidly growing mass, aggressive bone destruction and increasingly aggressive recurrence. It is diagnosed on histology (cytological atypia, high/atypical mitoses, sarcomatous spindling, necrosis) - so biopsy generously with expert sarcoma pathology. It is managed like a sarcoma (wide resection + adjuvant therapy + metastatic staging via MDT) and can metastasise and kill - never call an atypical, aggressive lesion "benign PVNS" without adequate sampling.
Radiosynovectomy (Radioactive Synoviorthesis)
The topic covers external-beam radiotherapy and the Verspoor series explicitly lists "radiosynovectomy" among treatments received, but the intra-articular radioisotope option is never explained - a distinct, exam-relevant adjunct different from external-beam radiation.
- What it is. Radiosynovectomy (radiosynoviorthesis) is the intra-articular injection of a beta-emitting radionuclide that is taken up by the synovium and ablates residual diseased synovial lining from within - a "medical synovectomy". It targets microscopic residual disease that surgery leaves behind, which is the very reason diffuse PVNS recurs.
- Which isotope for which joint. The agent is matched to joint size by the radionuclide's tissue penetration: Yttrium-90 (⁹⁰Y) for the knee (large joint, deeper penetration), Rhenium-186 (¹⁸⁶Re) for medium joints (hip, shoulder, ankle, wrist, elbow), and Erbium-169 (¹⁶⁹Er) for small (finger/toe) joints. Colloid/particulate carriers keep the isotope in the joint.
- Where it fits. It is used mainly as an adjunct after surgical synovectomy in diffuse disease (to treat residual synovium and reduce recurrence), or for inaccessible/multiply-recurrent disease where repeat open surgery is unattractive - conceptually similar to adjuvant external-beam radiotherapy but delivered from inside the joint with less exposure to surrounding tissues. It is also long-established for haemophilic and inflammatory synovitis.
- Cautions. The joint must be sealed (no leak/fistula) to avoid radionuclide escape and lymphatic/systemic spread; post-injection rest/immobilisation limits leakage; and it is generally avoided in the very young (theoretical radiation risk). Availability is limited to centres with nuclear-medicine support.
Q: What is radiosynovectomy in PVNS and which isotope for which joint? A: Intra-articular injection of a beta-emitting radionuclide that ablates residual synovium from within ("medical synovectomy"), used mainly as an adjunct after synovectomy in diffuse disease or for inaccessible/recurrent disease. Match isotope to joint size: Yttrium-90 for the knee (large), Rhenium-186 for medium joints (hip/shoulder/ankle/wrist/elbow), Erbium-169 for small finger/toe joints. The joint must be sealed (no leak) and it is avoided in the very young.
Complications of PVNS and Treatment
- Incidence/Risk Factors
- 30-50% for diffuse PVNS, under 10% for localized
- Prevention/Management
- Complete synovectomy, adjuvant radiation, long surveillance
- Incidence/Risk Factors
- Untreated or recurrent disease causes cartilage and bone erosion
- Prevention/Management
- Early diagnosis and complete excision critical
- Incidence/Risk Factors
- PVNS tissue is vascular, risk of bleeding after synovectomy
- Prevention/Management
- Meticulous hemostasis, drain placement, monitor drain output
- Incidence/Risk Factors
- After extensive synovectomy or radiation
- Prevention/Management
- Early range of motion, physiotherapy
- Incidence/Risk Factors
- CSF1R inhibitor can cause liver injury
- Prevention/Management
- Liver function test monitoring, dose adjustment or discontinuation
- Incidence/Risk Factors
- Recurrent disease or delayed diagnosis
- Prevention/Management
- Total joint arthroplasty as salvage (young age is challenging)
Key monitoring requirement: Pexidartinib (CSF1R inhibitor) carries FDA black box warning for hepatotoxicity. Liver function tests (LFTs) must be monitored before, during, and after treatment. Severe or progressive liver enzyme elevation requires dose reduction or discontinuation. This limits use to recurrent or unresectable PVNS where benefit outweighs risk.
The major complication of PVNS is recurrence, which drives need for surveillance and adjuvant therapy strategies.
Surgical Technique - Open Total Synovectomy (Knee)
Patient Positioning and Setup
Setup Checklist
Supine on standard operating table.
- Tourniquet on proximal thigh
- Leg free-draped from tourniquet distally
- Lateral post at foot of table for valgus stress
- Contralateral leg secured and padded
- Heel free of bed (prevent pressure injury)
- Tourniquet padding adequate
- No fluoroscopy needed for synovectomy
- Pre-operative MRI reviewed in OR for extent of disease
Standard positioning for knee arthrotomy.
Postoperative Care and Rehabilitation
Immediate Postoperative Management (Days 0-7)
Early Recovery Protocol
- Pain control: Multimodal analgesia (opioids, NSAIDs, ice)
- Drain management: Monitor output (remove at 24-48h when decreasing)
- DVT prophylaxis: Aspirin or LMWH per protocol
- Mobilization: Bed to chair, weight-bearing as tolerated
- Wound care: Monitor for bleeding, infection
- Range of motion: Start gentle passive ROM to prevent stiffness
- Mobilization: Crutches for comfort, full weight-bearing
- Discharge planning: Home with physiotherapy referral
Early range of motion is critical to prevent stiffness after extensive synovectomy.
- Localized PVNS: MRI every 6-12 months for 3 years
- Diffuse PVNS: MRI every 6 months for 5 years
- Clinical exam: At each imaging visit (assess ROM, swelling, function)
- Baseline: Post-op MRI at 6 months (compare future scans to this)
- Recurrent swelling: New or worsening joint effusion
- Mechanical symptoms: Locking, catching (new nodule)
- Pain: Progressive pain not explained by arthritis
- MRI: Synovial thickening, blooming artifact reappears
Long-term surveillance is essential given high recurrence risk in diffuse PVNS.
Outcomes and Prognosis
- Treatment
- Local excision
- Recurrence Rate
- Under 10%
- Long-Term Outcome
- Excellent - over 90% retain full function
- Treatment
- Open total synovectomy
- Recurrence Rate
- 30-50%
- Long-Term Outcome
- Good if no recurrence, but recurrence common
- Treatment
- Synovectomy + 20 Gy XRT
- Recurrence Rate
- 15-20%
- Long-Term Outcome
- Better than synovectomy alone, some stiffness risk
- Treatment
- Pexidartinib or imatinib
- Recurrence Rate
- Disease stabilization/shrinkage
- Long-Term Outcome
- Palliative - not curative, requires ongoing therapy
Poor prognostic factors (higher recurrence risk):
- Diffuse form (vs localized)
- Hip location (vs knee)
- Incomplete synovectomy (residual disease)
- Arthroscopic approach for diffuse disease (vs open)
- Young age (longer follow-up allows recurrence detection)
Good prognostic factors:
- Localized nodular form
- Complete excision with margins
- Open synovectomy (vs arthroscopic for diffuse)
- Adjuvant radiation (reduces recurrence by 50%)
The key message: PVNS is a chronic disease requiring long-term surveillance, but outcomes are generally good if recurrence is detected and treated early.
Recurrence and Surveillance
- Localized PVNS
- Under 10%
- Diffuse PVNS
- 30-50%
- Localized PVNS
- 1-2 years (median)
- Diffuse PVNS
- 2-3 years (median)
- Localized PVNS
- Incomplete excision, fragmentation
- Diffuse PVNS
- Diffuse involvement, posterior disease, hip location
- Localized PVNS
- MRI every 6-12 months for 3 years
- Diffuse PVNS
- MRI every 6 months for 5 years
Key counseling point: Even with complete synovectomy, diffuse PVNS recurs in 30-50% of cases. Recurrence typically occurs at 2-3 years post-op. Patients need long-term MRI surveillance (every 6 months for 5 years). Early recurrence detection allows re-synovectomy before extensive joint destruction occurs.
Management of Recurrent PVNS:
- First recurrence: Re-synovectomy + adjuvant radiation (20 Gy)
- Multiple recurrences: Consider CSF1R inhibitor (pexidartinib, imatinib)
- Unresectable disease: CSF1R inhibitor or arthroplasty
The goal is to balance aggressive treatment with preservation of joint function.
RECURRecurrence Risk Factors for PVNS
Hook:PVNS will RECUR unless you address these risk factors with complete excision and adjuvant therapy!
Guidelines, Registries & Global Practice
- Incidence: Diffuse PVNS roughly 2 per million per year; localized/tendon-sheath form more common
- Age: Peak in young/middle-aged adults (third to fifth decades)
- Distribution: Knee dominant (~80%), then hip; tendon-sheath form (GCTTS) outnumbers intra-articular PVNS ~3:1
- Data sources: No dedicated arthroplasty registry captures PVNS; epidemiology comes from sarcoma networks and single-centre series
- WHO Classification of Soft Tissue Tumours: groups PVNS as diffuse-type tenosynovial giant cell tumour (TGCT)
- Sarcoma networks (ESMO, NCCN soft-tissue, BSG/sarcoma MDTs): rare-tumour pathways favour specialist-centre referral
- No society publishes a stand-alone PVNS surgical guideline; management is consensus and evidence-led
- Systemic CSF1R-targeted therapy is reserved for advanced/unresectable disease via sarcoma MDT
- High-Resource Setting
- MRI with gradient-echo/SWI (blooming) and specialist musculoskeletal pathology
- Limited-Resource Setting
- Plain radiographs and clinical pattern; MRI often limited or delayed
- High-Resource Setting
- Open or combined open-arthroscopic total synovectomy; posterior approach when needed
- Limited-Resource Setting
- Open synovectomy where arthroscopic expertise/equipment is unavailable
- High-Resource Setting
- External-beam radiotherapy and CSF1R inhibitors (pexidartinib/imatinib) via MDT
- Limited-Resource Setting
- Radiotherapy access variable; targeted agents frequently unavailable or unaffordable
- High-Resource Setting
- Serial MRI for years (longer for diffuse disease)
- Limited-Resource Setting
- Clinical follow-up with selective imaging
Key counselling and documentation points for PVNS surgery:
- Recurrence risk: Counsel diffuse PVNS patients about high recurrence (30-50%) despite complete excision
- Completeness of excision: Document intra-operative assessment and pre-operative MRI extent
- Adjuvant options: Discuss radiotherapy and, for advanced disease, CSF1R-inhibitor referral
- Surveillance plan: Define follow-up imaging schedule and duration
- Joint preservation: Counsel young patients about possible future arthroplasty if disease recurs and destroys the joint
- Orthopaedic oncology / tumour surgery: Diagnosis and synovectomy
- Musculoskeletal radiology: MRI diagnosis and surveillance
- Pathology: Histological confirmation and exclusion of malignant TGCT
- Radiation oncology: Adjuvant radiotherapy planning for high-risk diffuse disease
- Medical oncology / sarcoma MDT: CSF1R inhibitor therapy for advanced or recurrent disease
- Patient communication: Emphasise the benign (non-cancerous) nature while explaining its locally aggressive, recurring behaviour
PVNS is a rare locally aggressive disease best managed through specialist multidisciplinary pathways worldwide; the principal global variation is access to advanced imaging, radiotherapy and CSF1R-targeted agents rather than differences in underlying clinical principles.
MCQ Practice Points
Q: What is the molecular driver of PVNS/TGCT? A: CSF1-COL6A3 fusion causing CSF1 overexpression. The chromosomal translocation t(1;2) drives colony stimulating factor 1 (CSF1) overexpression, which recruits inflammatory cells (macrophages, giant cells) via CSF1R. This is the rationale for CSF1R inhibitor therapy.
Q: What is the pathognomonic MRI finding in PVNS? A: Blooming artifact on gradient echo (GRE) sequences - caused by hemosiderin (iron) deposition from recurrent hemorrhage. Also low signal on T1 and T2 weighted images. This finding has over 90% sensitivity and specificity for PVNS.
Q: What is the difference between localized and diffuse PVNS in terms of recurrence? A: Localized PVNS recurs in under 10% after complete excision (behaves like benign tumor). Diffuse PVNS recurs in 30-50% despite complete synovectomy (behaves like locally aggressive lesion). This distinction is critical for counseling and treatment planning.
Q: What is the role of adjuvant radiation in diffuse PVNS? A: Adjuvant external beam radiation (20 Gy) reduces recurrence from 50% to approximately 20% in diffuse PVNS. Indicated for high recurrence risk (diffuse disease, incomplete excision, recurrent disease). Complications include stiffness and wound healing issues.
Q: What is pexidartinib and its indication? A: Pexidartinib is a CSF1R inhibitor FDA-approved for TGCT (PVNS) in 2019. Indicated for recurrent or unresectable disease. Mechanism: blocks CSF1R, preventing macrophage recruitment. Efficacy: 50-60% tumor shrinkage in recurrent disease. Key complication: hepatotoxicity (black box warning) - requires liver function monitoring.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old female presents with 18 months of progressive left knee swelling and recurrent episodes of joint effusion. She describes the fluid as 'bloody' when aspirated previously. MRI shows diffuse synovial thickening with low signal on T1 and T2, and blooming artifact on gradient echo sequences. What is your diagnosis and management?”
“You have decided to proceed with open total synovectomy for diffuse PVNS of the knee. Walk me through your surgical approach and key steps.”
“A 35-year-old male had open total synovectomy for diffuse PVNS of the knee 2 years ago. He now presents with recurrent swelling and MRI shows synovial thickening in the suprapatellar pouch and medial gutter consistent with recurrent disease. How do you manage this?”
Key Pathology
- PVNS equals TGCT (tenosynovial giant cell tumor) - same disease, different location
- CSF1-COL6A3 fusion drives CSF1 overexpression = macrophage recruitment
- Histology: Hemosiderin-laden macrophages, multinucleated giant cells, mononuclear stromal cells
- Gross: Orange-brown synovium (from hemosiderin = recurrent hemorrhage)
Classification
- Localized (nodular) = discrete mass = excision = under 10% recurrence
- Diffuse (villonodular) = entire synovium = synovectomy = 30-50% recurrence
- Knee 80%, hip 10-15%, other joints rare
Imaging
- MRI blooming artifact on GRE = pathognomonic (hemosiderin)
- Low signal T1 and T2 = hemosiderin deposition
- Bone erosions with sclerotic margins (late finding)
- Synovial thickening (nodular or diffuse)
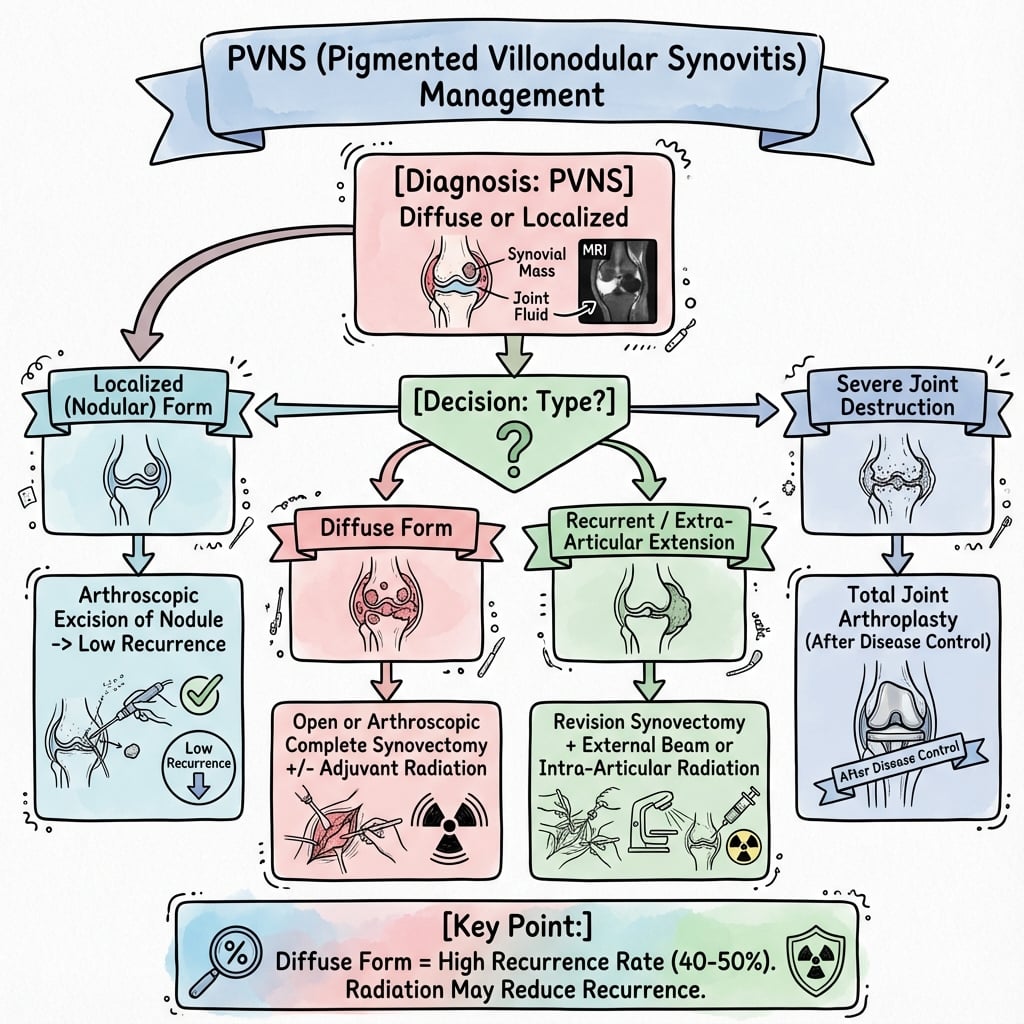
Treatment Algorithm
- Localized: Arthroscopic local excision (under 10% recurrence)
- Diffuse: Open total synovectomy (30-50% recurrence despite complete excision)
- Adjuvant radiation: 20 Gy reduces recurrence from 50% to 20%
- Recurrent/unresectable: CSF1R inhibitor (pexidartinib, imatinib)
Surgical Pearls
- Complete synovectomy: Suprapatellar pouch, gutters, intercondylar notch, posterior capsule
- Posterior approach if extensive posterior disease on MRI
- Meticulous hemostasis (vascular tissue) - large bore drain
- Danger: Popliteal vessels posterior, cruciate ligaments in notch
Evidence Base and Key Studies
Surgery and Radiotherapy for PVNS Recurrence: Individual-Patient Meta-Analysis
- Individual-patient meta-analysis, 630 patients across 35 observational studies (knee PVNS)
- Overall recurrence after synovectomy: 137 of 630 (21.8%)
- Diffuse PVNS: open synovectomy reduced recurrence vs arthroscopic (OR 0.47)
- Diffuse PVNS: combined open + arthroscopic reduced recurrence further (OR 0.19)
- Peri-operative radiotherapy reduced diffuse recurrence (OR 0.31); approach did not affect localized recurrence
CSF1 Translocation and the Landscape Effect in TGCT/PVNS
- Translocations involving chromosome 1p13 are present in the majority of TGCT and PVNS cases
- CSF1 is the gene at the 1p13 breakpoint; in some cases fused to COL6A3 (2q35)
- The translocation is present in only a MINORITY of intratumoral cells (the neoplastic clone)
- These cells overexpress CSF1, recruiting non-neoplastic CSF1R-positive macrophages - a tumor-landscaping effect
Pexidartinib for Advanced TGCT: Phase 3 ENLIVEN Trial
- Randomized, double-blind phase 3 trial: pexidartinib vs placebo in 120 patients with advanced TGCT not amenable to surgery
- Overall response at week 25 (RECIST 1.1): 39% (24 of 61) vs 0% (placebo); p less than 0.0001
- Enrolment stopped early after mixed/cholestatic hepatotoxicity emerged
- First systemic therapy to show robust tumour response in TGCT; FDA-approved 2019
- Carries a hepatotoxicity risk requiring monitoring (boxed warning)
Long-Term Outcome of Primary and Recurrent PVNS
- Single-institution consecutive series of 107 PVNS patients (29 localized, 75 diffuse); knee in 88%
- Diffuse PVNS recurrence-free survival: 69% at 1 year, falling to 32% at 5 years
- Recurrence rates increase over time - diffuse PVNS is a continually recurring problem
- Quality of life (SF-36 general health) lower than population norms in both subtypes
PVNS: Radiologic-Pathologic Correlation
- AFIP radiologic-pathologic review covering intra-articular PVNS, bursal and tendon-sheath (GCTTS) forms
- Low T2 signal plus gradient-echo blooming artifact from hemosiderin is described as nearly pathognomonic
- Tendon-sheath form (GCTTS) is most common, outnumbering intra-articular PVNS roughly 3:1
- Bone erosion on both sides of the joint is most frequent in hip involvement (over 90%)
- MRI best defines lesion extent - essential to guide complete surgical resection
Imatinib for Locally Advanced / Metastatic TGCT-PVNS
- Multi-institutional retrospective study, 29 patients (Europe, Australia, USA) with locally advanced/metastatic PVNS-TGCT
- RECIST overall response 19% (1 complete, 4 partial of 27 evaluable); stable disease in 74%
- Symptomatic improvement in 16 of 22 assessable patients (73%)
- Provided proof of concept for CSF1R targeting; 6 patients discontinued for toxicity