Juvenile Kyphosis | Thoracic Greater Than 45 Degrees | Vertebral Wedging | Bracing vs Surgery
- Diagnostic criteria: Thoracic kyphosis greater than 45°, 3+ consecutive vertebrae with greater than 5° anterior wedging each
- Rigid kyphosis: Does NOT correct on hyperextension (unlike postural kyphosis which corrects)
- Peak incidence: 12-17 years during growth spurt, male predominance
- Bracing effective in immature patients: Greater than 1 year growth remaining, kyphosis 50-75°
- Surgical threshold: Greater than 75° kyphosis, progressive despite bracing, neurological symptoms
- “Adams forward bend test shows angular kyphosis (not smooth curve like postural)
- “Tight hamstrings and hip flexors common - always assess flexibility
- “Check for associated scoliosis (30% have combined deformity)
- “MRI if neurological symptoms - rare thoracic disc herniation can occur
Classic criteria: Thoracic kyphosis greater than 45° (Cobb angle), with 3 or more consecutive vertebrae each having greater than 5° anterior wedging. Additional findings include Schmorl nodes, endplate irregularities, and disc space narrowing. Apex typically T7-T9.
Key differentiation on exam: Have patient hyperextend spine. Postural kyphosis CORRECTS with hyperextension (flexible). Scheuermann kyphosis does NOT correct (rigid, structural). Also, postural kyphosis is a smooth, round curve; Scheuermann has angular apex.
Brace if: Kyphosis 50-75°, skeletally immature (Risser 0-3, greater than 1 year growth remaining), compliant patient. Milwaukee brace or TLSO worn 16-23 hours/day until skeletal maturity. Bracing can prevent progression but rarely corrects established deformity.
Surgery if: Kyphosis greater than 75°, progressive despite bracing, intractable pain not responding to conservative treatment, neurological deficit (rare). Posterior-only fusion now most common. Anterior release rarely needed with modern posterior techniques.
- Scheuermann Kyphosis
- Rigid, angular apex
- Postural Kyphosis
- Flexible, smooth curve
- Scheuermann Kyphosis
- Does NOT correct
- Postural Kyphosis
- Corrects fully
- Scheuermann Kyphosis
- Vertebral wedging, Schmorl nodes, endplate changes
- Postural Kyphosis
- Normal vertebrae, no structural changes
- Scheuermann Kyphosis
- Often present, activity-related
- Postural Kyphosis
- Usually painless
- Scheuermann Kyphosis
- Bracing if immature, surgery if severe
- Postural Kyphosis
- Posture training, exercises only
BRACEBRACE - Bracing Criteria
Hook:To BRACE, patient must meet all criteria - immature, kyphosis 50-75°, compliant.
Overview and Epidemiology
Scheuermann Disease (Scheuermann Kyphosis) is the most common cause of structural kyphosis in adolescents. It is characterized by vertebral wedging leading to an exaggerated thoracic kyphosis that is rigid and does not correct with hyperextension.
Epidemiology:
- Prevalence 1-8% of adolescents (varies by diagnostic criteria used)
- Male predominance 2:1 (historical), may be equalizing
- Peak presentation during adolescent growth spurt (12-17 years)
- Often diagnosed when parents notice "round back" or stooped posture
- Associated with heavy manual labor historically (juvenile disc disorder)
Classic (thoracic): Apex T7-T9, more common, better tolerated. Atypical (thoracolumbar/lumbar): Apex T10-L2, more painful, higher risk of degenerative changes. Lumbar Scheuermann may present primarily as low back pain rather than visible kyphosis.
Etiology (Multifactorial):
- Genetic component (autosomal dominant with variable penetrance)
- Mechanical overload during growth (anterior vertebral compression)
- Possible cartilage endplate abnormality
- Associated with growth plate disorders
The atypical (lumbar or thoracolumbar) Scheuermann is a distinct, exam-favoured entity - and the one most often seen in adolescent athletes and manual workers (gymnasts, rowers, fast bowlers, weightlifters). Repetitive flexion plus axial loading injures the immature vertebral endplate and ring apophysis, producing Schmorl nodes, endplate irregularity and disc-space narrowing at the thoracolumbar junction (T10-L2) - often with little or no visible kyphotic deformity. The hallmark is therefore activity-related low back pain as the dominant symptom, not a cosmetic round back (contrast with classic thoracic Scheuermann). Management is correspondingly different: it is load-based and symptom-driven - relative rest from the offending sport, activity modification, core and hamstring rehabilitation, and analgesia - with bracing reserved for refractory pain rather than for cosmesis, and surgery almost never required. Most settle with skeletal maturity, although the segment carries a higher long-term degenerative/disc risk. Recognise it as a cause of "mechanical" adolescent back pain rather than dismissing it as a sprain.
Pathophysiology and Mechanisms
Normal vs Scheuermann Kyphosis
- Normal Range
- 20-45°
- Scheuermann Threshold
- Greater than 45° (with vertebral wedging)
- Surgical Threshold
- Greater than 75°
- Normal Range
- 40-60°
- Scheuermann Threshold
- May be increased (compensatory)
- Surgical Threshold
- Consider in surgical planning
- Normal Range
- 20-40°
- Scheuermann Threshold
- May be increased (compensatory)
- Surgical Threshold
- Assess for chin-on-chest risk
Vertebral Wedging Mechanism
- Anterior growth plate injury: Repetitive loading damages vertebral endplates
- Asymmetric growth: Posterior vertebral body grows faster than anterior
- Vertebral wedging: Each affected vertebra contributes greater than 5° wedging
- Schmorl nodes: Disc material herniates into weakened endplates
- Disc space narrowing: Secondary degenerative changes
- Increased thoracic kyphosis: Cumulative effect of wedged vertebrae
- Compensatory hyperlordosis: Lumbar and cervical regions compensate
- Tight posterior chain: Hamstrings, hip flexors tighten
- Anterior chest wall tightness: Pectorals shortened
- Altered center of gravity: Forward shift
30% of Scheuermann patients have associated scoliosis. Always check for coronal plane deformity as well. Combined kyphoscoliosis may affect surgical planning.
Classification Systems
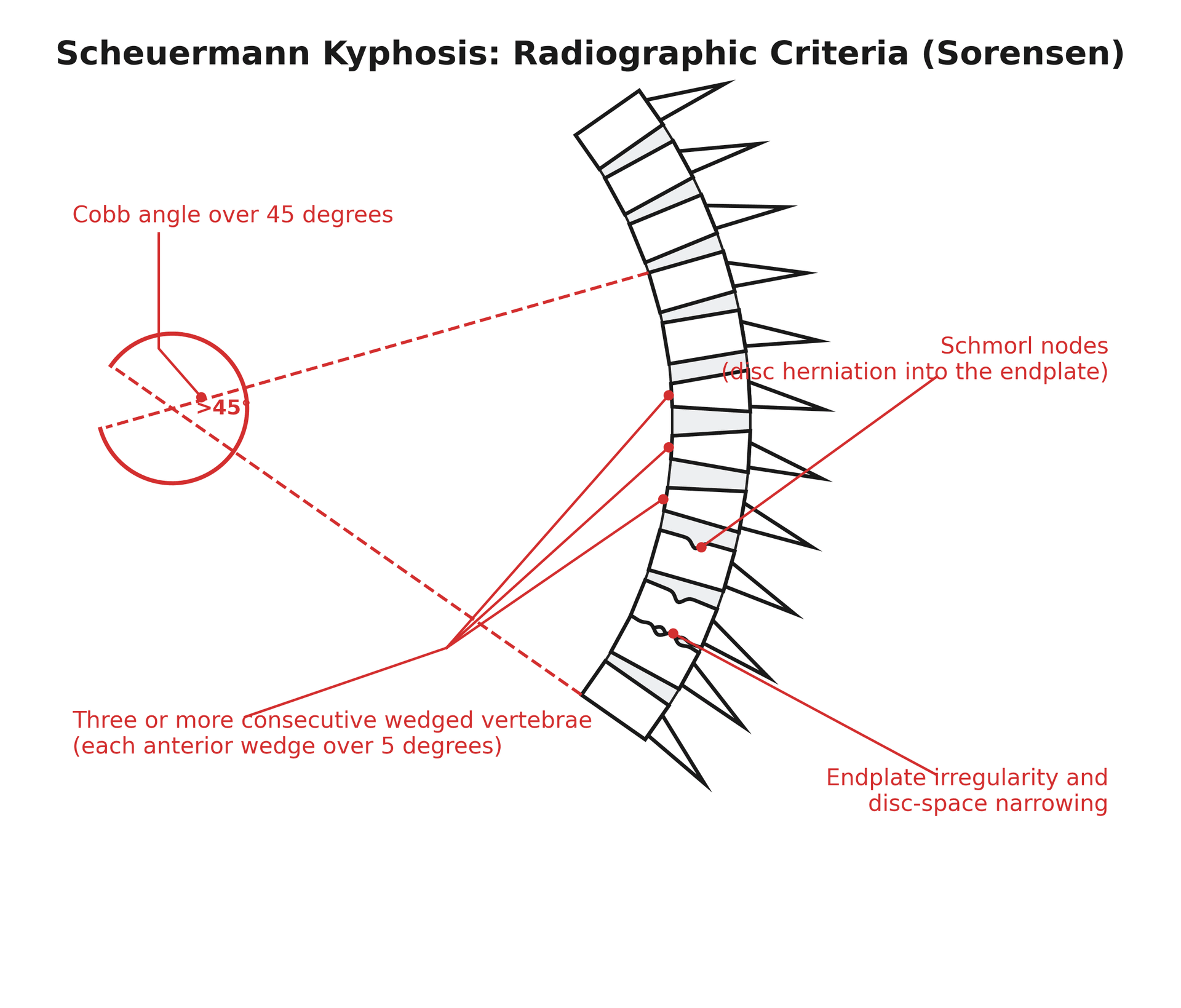
Classic Diagnostic Criteria (Sorensen 1964)
- Thoracic kyphosis greater than 45° (Cobb angle on standing lateral X-ray)
- Three or more consecutive vertebrae with greater than 5° anterior wedging each
- Vertebral endplate irregularities
- Schmorl nodes (disc herniation into vertebral body)
- Disc space narrowing
- Increased AP diameter of apical vertebrae
- Apex typically T7-T9
Standard criteria for diagnosis. Some authors use greater than 40° as threshold.
Clinical Assessment
Systematic Examination
- Onset: Gradual, noticed during growth spurt
- Pain: Present in 50%, usually activity-related, localized to apex
- Cosmesis: Parents/patient notice "round back" or stooped posture
- Activity level: Impact on sports, sitting tolerance
- Family history: May be positive
- Neurological symptoms: RARE - but ask about weakness, numbness
- Standing: Exaggerated thoracic kyphosis, forward head posture
- Adams forward bend: Angular apex (not smooth curve)
- Compensatory lordosis: Increased lumbar curve, extended cervical spine
- Shoulder position: Often protracted
- Associated scoliosis: Check for rib hump, asymmetry
- Hyperextension test: Scheuermann does NOT correct (rigid)
- Postural kyphosis DOES correct - key differentiation
- Hamstring tightness: Very common, assess straight leg raise
- Hip flexor tightness: Thomas test often positive
- Pectoralis tightness: Assess shoulder flexibility
- Full neurological examination if any symptoms
- Cord compression rare but possible with severe kyphosis
- Thoracic disc herniation can occur into spinal canal
- Check reflexes, strength, sensation in lower limbs
Have patient lie prone and hyperextend the spine (or extend over examiner's arm). Scheuermann kyphosis remains fixed (rigid, structural). Postural kyphosis corrects completely (flexible, non-structural). This single test distinguishes the two conditions.
Investigations
Standing lateral spine X-ray with arms forward (on a support) is the standard view for measuring kyphosis. Cobb angle measured from superior endplate of first tilted vertebra to inferior endplate of last tilted vertebra (usually T4-T12). Also obtain AP view to assess scoliosis.
- Description
- Cobb angle T4-T12 or affected levels
- Clinical Significance
- Diagnostic criterion
- Description
- Anterior height loss, 3+ consecutive vertebrae
- Clinical Significance
- Diagnostic criterion
- Description
- Disc herniation into vertebral endplates
- Clinical Significance
- Supportive finding
- Description
- Wavy, irregular vertebral endplates
- Clinical Significance
- Supportive finding
- Description
- Secondary degenerative change
- Clinical Significance
- Supportive finding
Other Imaging:
- MRI: Only if neurological symptoms, to assess cord/disc
- CT: Rarely needed, for surgical planning in complex cases
- Bone scan: Not routinely indicated
Advanced Imaging Examples
Skeletal Maturity Assessment:
- Risser sign on iliac crest
- Hand X-ray for bone age if needed
- Critical for determining bracing candidacy

SCHEUERMANNSCHEUERMANN - Diagnostic Features
Hook:SCHEUERMANN criteria are specific - remember each letter corresponds to a diagnostic or management point.
Differential Diagnosis
The structural, rigid kyphosis of Scheuermann disease must be distinguished from other causes of an increased thoracic or thoracolumbar curve in a young person. Getting this wrong risks bracing a flexible postural curve, or missing infection, tumour or a syndromic/neuromuscular cause.
- Key Discriminating Features
- Rigid, angular apex; 3+ wedged vertebrae over 5°; Schmorl nodes; positive family history
- Confirmatory Test
- Standing lateral radiograph (Cobb, wedging, endplate change)
- Key Discriminating Features
- Smooth round curve, fully corrects on hyperextension, no vertebral wedging
- Confirmatory Test
- Hyperextension test + normal radiograph
- Key Discriminating Features
- Present from infancy/early childhood, often sharp angular gibbus; failure of formation/segmentation
- Confirmatory Test
- Radiograph ± CT showing hemivertebra/bar; high cord risk
- Key Discriminating Features
- Constitutional symptoms, night pain, sharp gibbus, vertebral destruction
- Confirmatory Test
- MRI (paraspinal abscess, disc/endplate destruction), inflammatory markers
- Key Discriminating Features
- Long C-shaped curve, hypotonia or spasticity, known syndrome (e.g. Marfan, neurofibromatosis)
- Confirmatory Test
- Underlying disease workup; MRI for dystrophic change/dural ectasia
- Key Discriminating Features
- Acute pain, trauma or steroid history, single-level wedge
- Confirmatory Test
- Radiograph/MRI marrow oedema; bone density assessment
A sharp angular gibbus, constitutional symptoms or rapid progression should prompt MRI to exclude infection (TB) or tumour before attributing a kyphosis to Scheuermann disease. Scheuermann produces a broad rounded structural curve over several segments, not a single-segment sharp angulation.
Management Algorithm
Non-Operative Management
- Skeletal Maturity
- Any
- Treatment
- Observation, physiotherapy, posture training
- Expected Outcome
- Stable, rarely progresses
- Skeletal Maturity
- Immature (Risser 0-3)
- Treatment
- Milwaukee brace or TLSO 16-23 hrs/day
- Expected Outcome
- Prevents progression, some correction
- Skeletal Maturity
- Mature (Risser 4-5)
- Treatment
- Physiotherapy, activity modification
- Expected Outcome
- Bracing ineffective after maturity
- Skeletal Maturity
- Any
- Treatment
- Surgical consultation
- Expected Outcome
- Likely needs operative treatment
- Core strengthening (especially extensors)
- Hamstring and hip flexor stretching
- Pectoralis stretching
- Postural awareness training
- Activity modification (avoid heavy lifting)
- Milwaukee brace (extends to chin) or TLSO
- Wear 16-23 hours/day until skeletal maturity
- Weaning protocol over 6-12 months after maturity
- Exercises continued during bracing
Compliance is the key determinant of bracing success.
Surgical Technique
Posterior Spinal Fusion with Instrumentation
Standard approach for Scheuermann kyphosis.
Surgical Steps
- Prone position on appropriate frame
- Arms forward, knees slightly flexed
- Neuromonitoring (SSEPs, MEPs) throughout
- Midline incision over affected levels
- Subperiosteal exposure of posterior elements
- Usually T2/T3 to L1/L2 depending on curve
- Ponte osteotomies at multiple levels to increase flexibility
- Remove ligamentum flavum and facet joints
- Allows posterior column shortening and correction
- Pedicle screws at all levels (or hybrid with hooks)
- Dual rods (usually cobalt chrome or titanium)
- Sequential compression to correct kyphosis
- Use of set screws to lock correction
- Decorticate transverse processes and facets
- Apply bone graft (local autograft ± allograft)
- Close in layers over drain
Key Principles:
- Preserve lower lumbar lordosis (avoid flat-back)
- Stop fusion at stable vertebra
- Achieve correction with compression, not distraction
These principles are essential for durable correction and avoiding junctional complications.
Junctional kyphosis is the dominant complication of Scheuermann surgery, and level selection is the main way to prevent it. Proximally, include the proximal end vertebra (the most cephalad vertebra of the measured kyphotic Cobb) - stopping short of it leaves an uninstrumented kyphotic segment that becomes proximal junctional kyphosis (PJK). Distally, extend the construct to the sagittal stable vertebra (SSV) - the most proximal vertebra touched by the posterior sacral vertical line (a vertical line from the posterosuperior corner of S1) - and at least to the first lordotic disc; stopping above the SSV (in particular at or above the first lordotic vertebra alone) leaves the lower curve unbalanced and predisposes to distal junctional kyphosis (DJK). Combine this with avoiding over-correction (aim toward a physiological kyphosis of about 50 degrees, matched to pelvic incidence, rather than a straight spine) and gentle proximal fixation. So the examinable trio is: instrument the proximal end vertebra, reach the sagittal stable vertebra distally, and do not over-correct.
SURGERYSURGERY - Surgical Indications
Hook:SURGERY threshold is greater than 75° or failed conservative treatment.
Complications
- Incidence
- 10-20%
- Prevention/Management
- Appropriate fusion levels, avoid flat-back
- Incidence
- Less than 1%
- Prevention/Management
- Neuromonitoring, careful correction
- Incidence
- 5-10%
- Prevention/Management
- Adequate bone graft, avoid smoking
- Incidence
- 1-3%
- Prevention/Management
- Prophylactic antibiotics, meticulous technique
- Incidence
- Variable
- Prevention/Management
- Adequate fixation, patient compliance
- Incidence
- Common
- Prevention/Management
- Padding, skin checks, brace adjustments
PJK is the most common complication after kyphosis surgery. Occurs at the level above the instrumentation. Risk factors: osteoporosis, stopping fusion at kyphotic segment, excessive correction. Prevention includes ending fusion at lordotic vertebra, avoiding overcorrection, and hooks/wires at proximal level.
Postoperative Care and Rehabilitation
Post-Surgery Protocol
- Mobilize day 1-2 with physiotherapy
- Wean pain control, oral medications
- Drain removal when output minimal
- Wound check before discharge
- Limited activity, no bending/twisting/lifting
- Walking encouraged, increase distances
- Wound care, monitor for infection
- May use brace if surgeon preference
- Gradual increase in activity
- May return to school/desk work
- No sports or heavy activity
- X-rays to assess alignment
- Progressive return to activities
- Sports typically 6-12 months
- Physical therapy for core strength
- Final X-rays at 1-2 years
Conservative Treatment Rehabilitation:
- Physiotherapy ongoing during bracing
- Exercises continued after brace weaning
- Postural awareness lifelong
- Activity modification if symptomatic
Outcomes
- Bracing effective in preventing progression if criteria met
- Rarely achieves significant correction of established deformity
- Good long-term function for curves less than 75°
- Back pain may persist, usually manageable
- High satisfaction rates (greater than 90%)
- Correction from average 75° to 45-50°
- Pain improvement in most patients
- Return to full activities 6-12 months
- Long-term fusion outcomes generally good
Guidelines, Registries & Global Practice
Global Epidemiology:
- Reported prevalence 1-8% of adolescents, varying with the diagnostic threshold (greater than 40° vs greater than 45°) and the population screened
- Danish twin data estimate heritability at 0.74 with an underlying population prevalence near 1.9% and an approximately 2:1 male predominance
- Peak presentation in the pubertal growth spurt (roughly 12-17 years), reflecting the period of maximal anterior vertebral growth
- Diagnostic & Conservative Stance
- Greater than 45° with structural wedging; bracing for flexible curves 55-80° in the immature
- Operative Stance
- Surgery generally reserved for curves over 70-75°, progression or refractory pain
- Diagnostic & Conservative Stance
- Observation and physiotherapy for mild curves; bracing offered selectively in the immature
- Operative Stance
- Deformity surgery centralised to specialist units; posterior-only with osteotomies favoured
- Diagnostic & Conservative Stance
- Emphasis on standing sagittal Cobb and global sagittal balance; brace for progressive immature curves
- Operative Stance
- Posterior column osteotomies + segmental pedicle screws; anterior release for very rigid curves only
- Diagnostic & Conservative Stance
- Structured bracing and physiotherapeutic scoliosis-specific exercises in the immature
- Operative Stance
- Refers for surgery when bracing fails or curve is severe
There is no single international consensus number: thresholds differ because evidence is largely retrospective and outcome measures vary. The common thread is structural confirmation plus skeletal maturity to decide between bracing and surgery.
- Unlike arthroplasty, Scheuermann kyphosis has no dedicated worldwide implant registry; deformity outcomes are reported through SRS morbidity-and-mortality databases and multicentre study groups
- Spinal deformity registries (e.g. national paediatric spine collaboratives) track instrumentation complications such as PJK, infection and reoperation across centres
- Well-resourced settings: standing long-cassette/EOS imaging, custom TLSO/CAD bracing with compliance sensors, neuromonitoring (SSEP/MEP/triggered EMG) and cell salvage for surgery
- Limited-resource settings: reliance on plain radiographs, generic off-the-shelf bracing, later presentation with larger rigid curves, and fewer centres offering safe deformity surgery with neuromonitoring - shifting the balance toward conservative management or referral
Controversies & Areas of Uncertainty
Sorensen's greater than 5° wedging of 3+ contiguous vertebrae is classic, but some authors diagnose with a single wedged vertebra plus typical endplate change, and use greater than 40° rather than greater than 45° as the kyphosis cut-off. There is no universally agreed numeric definition.
Brace efficacy is supported only by retrospective data. The curve magnitude at which to start, target wear time, and whether physiotherapeutic scoliosis-specific exercises add benefit all vary between centres and societies.
Over-correction is linked to proximal junctional kyphosis. Many surgeons now deliberately under-correct toward physiological kyphosis (around 50°) and match correction to pelvic incidence rather than aiming for a "straight" spine.
Selecting the lowest instrumented vertebra (first lordotic vertebra vs sagittal stable vertebra) to minimise distal junctional kyphosis remains debated, with different rules proposed and no randomised comparison.
Anterior release has largely fallen out of routine use because posterior column osteotomies achieve comparable correction (see Evidence Base), but its precise residual role in the most rigid curves is still individualised rather than protocol-driven.
MCQ Practice Points
Q: What are the Sorensen criteria for Scheuermann kyphosis? A: Thoracic kyphosis greater than 45° with 3 or more consecutive vertebrae each having greater than 5° anterior wedging. Supportive findings include Schmorl nodes, endplate irregularities, and disc space narrowing.
Q: How do you differentiate Scheuermann from postural kyphosis clinically? A: Hyperextension test - Scheuermann does NOT correct (rigid, structural). Postural kyphosis corrects fully (flexible, non-structural).
Q: When is bracing indicated for Scheuermann kyphosis? A: Kyphosis 50-75° in skeletally immature patients (Risser 0-3) with greater than 1 year growth remaining. Bracing is ineffective after skeletal maturity.
Q: What is the surgical threshold for Scheuermann kyphosis? A: Greater than 75° kyphosis, or progressive curve despite bracing, or intractable pain, or neurological symptoms.
Medicolegal Considerations
- Document hyperextension test result (rigid vs flexible)
- Record Cobb angle and vertebral wedging measurements
- Document skeletal maturity assessment (Risser sign)
- Record neurological examination findings
- Document bracing compliance discussions
- Proximal junctional kyphosis risk (10-20%)
- Neurological injury risk (less than 1%)
- Pseudarthrosis, infection, hardware failure
- Blood loss and transfusion possibility
- Long fusion and loss of motion
Although rare, thoracic cord compression can occur with severe Scheuermann kyphosis. Document neurological examination at each visit. Missing progressive weakness could lead to delayed treatment and worse outcomes.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 14-year-old boy presents with progressive round back posture noticed by his parents over the past year. He complains of mild mid-back pain after prolonged sitting. How would you differentiate Scheuermann kyphosis from postural kyphosis?”
“A 16-year-old girl with known Scheuermann kyphosis returns after completing 2 years of bracing. Her curve has progressed from 55° to 70° despite reported compliant brace wear. She now has daily back pain. Why might the kyphosis have progressed despite bracing?”
“A 15-year-old with severe Scheuermann kyphosis (85°) presents with new onset lower limb weakness over 2 weeks. He has difficulty walking and describes numbness in both legs. What is your immediate concern and management?”
Diagnosis
- Kyphosis greater than 45° (Cobb angle)
- 3+ consecutive vertebrae with greater than 5° wedging each
- Schmorl nodes, endplate irregularities
- Hyperextension test: does NOT correct (rigid)
Bracing
- Kyphosis 50-75°
- Risser 0-3 (immature)
- Greater than 1 year growth remaining
- 16-23 hours/day until maturity
Surgery
- Kyphosis greater than 75°
- Progressive despite bracing
- Intractable pain
- Neurological symptoms
Surgical Approach
- Posterior fusion with pedicle screws
- Ponte osteotomies for correction
- Anterior release rarely needed
- Goal: 45-50° final kyphosis
Complications
- PJK 10-20% (most common)
- Neurological less than 1%
- Pseudarthrosis 5-10%
- End fusion at lordotic vertebra
Evidence Base
The evidence below is drawn from PubMed-indexed primary literature. Landmark natural-history, genetic-epidemiology, bracing, and operative studies are summarised with the actual sample sizes and conclusions of each paper.
Natural History at 32-Year Follow-up (Iowa cohort)
- 67 patients (mean kyphosis 71°) reviewed at mean 32 years vs 34 matched controls
- More intense back pain, reduced trunk extension range and strength than controls
- No difference in education, days off work, ADL interference, self-esteem or social limitation
- Restrictive lung disease only when kyphosis exceeded 100° with apex T1-T8
Genetic Epidemiology - Danish Twin Study
- 11,436 complete twin pairs analysed by classical twin modelling
- Heritability estimate 0.74 (95% CI 0.65-0.81); environment 0.26
- Estimated female prevalence 1.9%; male threshold lower (about 2:1 male predominance)
- Prevalence stable across a 50-year age span