Inferior Pole Patellar Apophysitis | Adolescent Athletes | Activity Modification | Self-Limiting
- Traction apophysitis: Repetitive stress on inferior pole of patella from patellar tendon during growth spurt
- Self-limiting condition: Resolves when apophysis closes (typically 1-2 years), may leave painless calcification
- Clinical diagnosis: Point tenderness over inferior pole of patella, worsened by resisted knee extension
- Treatment is conservative: Activity modification, ice, stretching - rarely any surgery needed
- Less common than OSD: Similar mechanism but affects proximal end of patellar tendon
- “Less common than Osgood-Schlatter but same mechanism and treatment
- “Bilateral in 20-30% but usually asymmetric
- “Often coexists with Osgood-Schlatter disease
- “Persistent calcification at inferior pole after resolution is normal
Traction apophysitis at inferior pole of patella. Repetitive contraction of quadriceps pulls on inferior pole via patellar tendon origin. Peak age 10-14 years (slightly younger than OSD). More common in jumping/running sports (basketball, soccer, gymnastics, volleyball).
Point tenderness over inferior pole of patella is pathognomonic. Pain worsened by running, jumping, kneeling, squatting, stairs. Reproduced by resisted knee extension and passive flexion. May have palpable calcification. No effusion, no instability.
X-rays NOT required for diagnosis - clinical diagnosis. If obtained, may show soft tissue swelling, fragmentation, or irregular ossification at inferior pole. Reserve X-rays for: atypical presentation, ruling out tumor/infection, failed treatment, suspected avulsion fracture.
Most cases managed in primary care. Refer if: symptoms persist beyond skeletal maturity, complete avulsion fracture suspected, concern for other diagnoses (tumor, infection), severe symptoms not responding to conservative care after 6 months.
- Key Features
- 10-14y athletes, activity-related pain
- Tenderness Location
- Inferior pole of patella
- Management
- Activity modification, stretching, ice
- Key Features
- 10-15y athletes, activity-related pain, bump
- Tenderness Location
- Tibial tubercle (anterior, distal to patella)
- Management
- Same conservative treatment as SLJ
- Key Features
- Anterior knee pain, worse sitting/stairs
- Tenderness Location
- Diffuse peripatellar, retropatellar
- Management
- VMO strengthening, patellar taping
- Key Features
- Older athletes (16+), jumping sports
- Tenderness Location
- Inferior pole patella to tendon insertion
- Management
- Eccentric exercises, load management
- Key Features
- Acute traumatic event, swelling, unable to extend
- Tenderness Location
- Inferior pole with deformity
- Management
- URGENT - surgical fixation usually needed
INFERIORINFERIOR - Location and Features
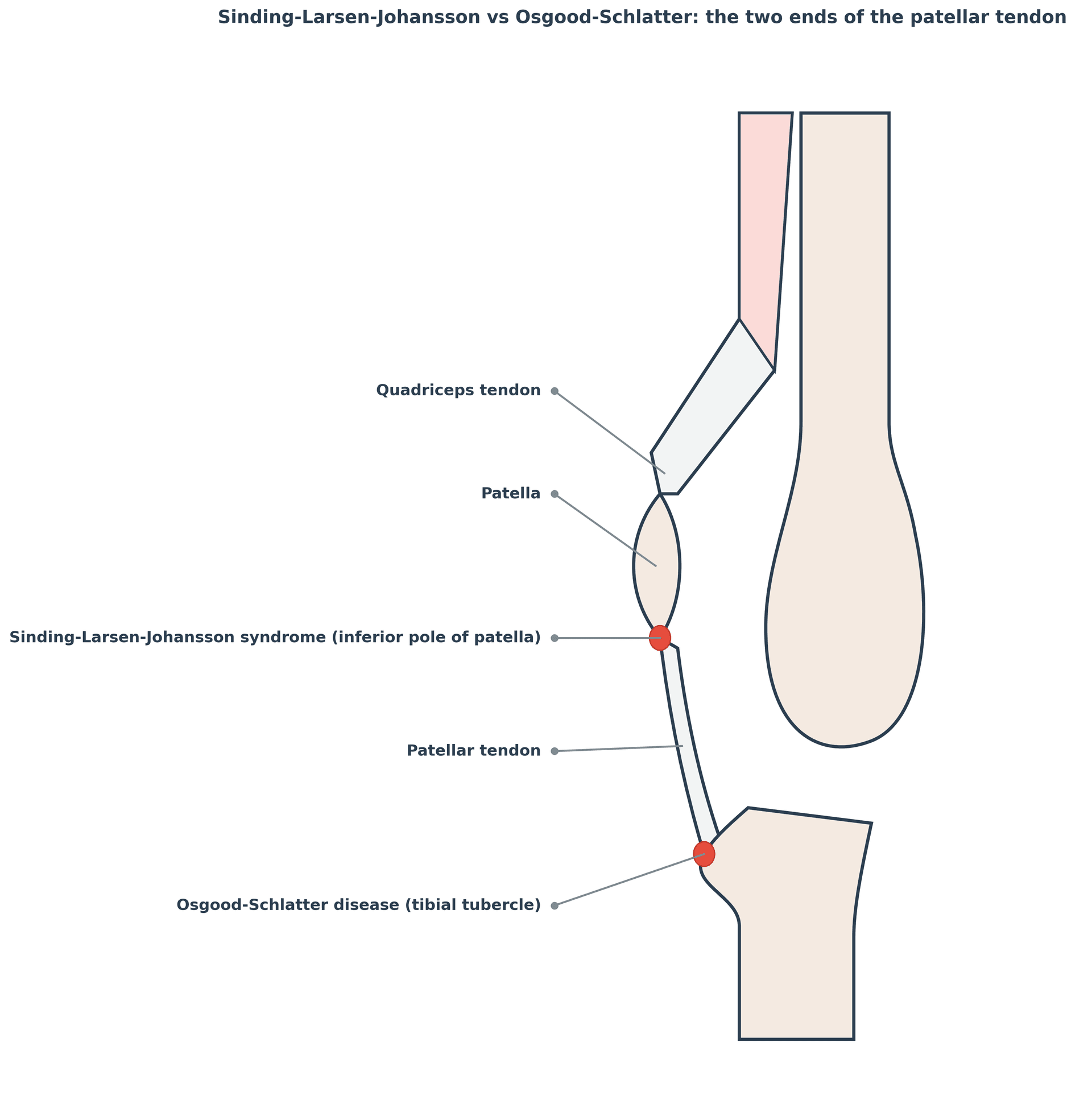
Hook:INFERIOR pole is where the patellar tendon originates - this is the proximal end of the extensor mechanism, opposite to OSD at the distal end.
Overview and Epidemiology
Sinding-Larsen-Johansson (SLJ) Syndrome is a traction apophysitis affecting the inferior pole of the patella in active adolescents. It is characterized by localized pain, swelling, and tenderness at the origin of the patellar tendon on the inferior pole of the patella.
Epidemiology:
- Less common than Osgood-Schlatter disease but same mechanism
- Peak incidence: males 11-14 years, females 10-13 years
- Male to female ratio approximately 2:1
- 20-30% bilateral (often asymmetric in severity)
- Most common in running, jumping, kicking sports (soccer, basketball, gymnastics, volleyball)
- Often coexists with Osgood-Schlatter disease (both ends of patellar tendon affected)
The inferior pole of the patella has a secondary ossification center (apophysis) that is biomechanically weaker than mature bone or the patellar tendon. During the adolescent growth spurt, rapid bone growth increases muscle-tendon tension while the apophysis has not yet fused. Repetitive traction from the powerful quadriceps causes microtrauma, inflammation, and sometimes fragmentation of the apophysis at the patellar tendon origin.
Etiology and Risk Factors:
- Age: Skeletal immaturity with open patellar apophysis
- Sex: Male more common (puberty timing, sports participation)
- Rapid growth: Growth spurt increases tension
- Quadriceps tightness: Tight quads increase traction force
- Hamstring tightness: Adds load to extensor mechanism
- High-impact sports: Running, jumping, kicking
- Training volume: Intense practice schedules during growth
- Poor conditioning: Sudden increase in activity level
- Hard playing surfaces: Increase impact loading
- Inadequate rest periods: No recovery time between training
Natural History:
- Most cases resolve spontaneously when the patellar apophysis fuses (typically 1-2 years)
- Residual calcification at inferior pole may persist - this is NORMAL, not a complication
- 5-10% have persistent symptoms into adulthood
- Rare complications: inferior pole avulsion fracture, persistent symptomatic calcification
Pathophysiology and Mechanisms
Inferior Pole Patella Anatomy
The inferior pole of the patella is where the patellar tendon originates. The patella has a secondary ossification center at its inferior pole that appears during childhood and fuses during adolescence.
- Age (years)
- 0-8
- Description
- Entirely cartilage, no ossification
- Clinical Relevance
- Rarely symptomatic at this age
- Age (years)
- 8-12
- Description
- Secondary ossification center appears at inferior pole
- Clinical Relevance
- Beginning of vulnerability period
- Age (years)
- 10-14
- Description
- Ossification extends, peak vulnerability
- Clinical Relevance
- Peak SLJ incidence
- Age (years)
- 14-18
- Description
- Apophysis fuses to patella
- Clinical Relevance
- SLJ symptoms resolve with fusion
The cartilaginous apophysis is the weak link. During the epiphyseal stage, the inferior pole may avulse with acute trauma (jumping sports, landing). Unlike SLJ, avulsion is an ACUTE injury with sudden pain, inability to extend knee, and visible/palpable deformity. Treat as a fracture - usually requires surgical fixation.
Extensor Mechanism Biomechanics
Quadriceps muscle generates force that is transmitted through:
- Quadriceps tendon → inserts on superior pole of patella
- Patella → acts as sesamoid/pulley
- Patellar tendon → originates from inferior pole, inserts on tibial tubercle
In growing adolescents, the inferior pole apophysis experiences HIGH tensile stress at the tendon-bone junction.
- Tendon origin: Patellar tendon originates from inferior pole
- Peak stress at origin: Tendon-bone junction concentrates force
- Weak link: Cartilaginous apophysis weaker than tendon or bone
- Growth-related tension: Rapid femoral growth increases quad tightness
SLJ and OSD affect opposite ends of the patellar tendon. SLJ affects the origin (inferior pole of patella) while OSD affects the insertion (tibial tubercle). Both are traction apophysitides with the same mechanism, age group, and treatment. Patients may have both conditions simultaneously, representing stress at both ends of the extensor mechanism.
Classification Systems
Clinical Severity Grading
- Symptoms
- Pain only after activity, no swelling at rest
- Impact on Activity
- Can complete training sessions
- Treatment Approach
- Ice after activity, stretching, continue sports
- Symptoms
- Pain during AND after activity, mild swelling
- Impact on Activity
- Performance affected, some activity limitation
- Treatment Approach
- Modify activity level, patellar strap, formal physio
- Symptoms
- Pain at rest, limits daily activities, walking painful
- Impact on Activity
- Unable to participate in sport
- Treatment Approach
- Rest from sport, possible short immobilization, physio
Mild SLJ may improve in 6-8 weeks with basic activity modification. Moderate SLJ typically requires 3-6 months of modified activity. Severe SLJ may need 6-12 months, possibly with periods of complete rest. All grades typically resolve when the physis closes, but symptom duration is proportional to severity.
Clinical Assessment
History:
- Age and sex: Peak 10-14 years, more common in males
- Sports participation: Type, frequency, intensity
- Training changes: Recent increase in volume or intensity?
- Pain characteristics: Location, timing, aggravating factors
- Bilateral symptoms: 20-30% bilateral
- Previous injury: Rule out acute trauma
- Coexisting OSD: Check for tibial tubercle symptoms
- Night pain or rest pain: Consider tumor, infection
- Acute traumatic onset: Avulsion fracture
- Knee effusion: Unusual for SLJ - suggests other pathology
- Systemic symptoms: Fever, weight loss - infection, malignancy
- Very young child: Under age 8 - SLJ rare, investigate
- Hip symptoms: SCFE, Perthes - examine hip in all knee pain
Physical Examination:
Systematic Examination
- Visible swelling over inferior pole of patella (less common than OSD bump)
- Compare bilateral - may be asymmetric if bilateral SLJ
- Look for effusion (unusual for SLJ - suggests other diagnosis)
- Assess overall limb alignment, muscle bulk
- Point tenderness over inferior pole of patella - pathognomonic
- Palpate entire patellar tendon (rule out tendinopathy)
- Palpate tibial tubercle (check for coexisting OSD)
- Palpate medial and lateral joint lines (meniscal pathology)
- Palpate patella and peripatellar tissues
- Knee ROM: Usually full, may have slight flexion discomfort
- Passive flexion: May be painful at end range (compresses inferior pole)
- Quadriceps and hamstring flexibility: Often reduced
- Hip ROM: Must examine hip to rule out referred pain (SCFE)
- Resisted knee extension: Reproduces pain over inferior pole
- Active knee extension: May be painful against resistance
- Patellar mobility: Normal in SLJ (unlike patellofemoral syndrome)
- Ligament stability: Should be normal
- Meniscal tests: Should be negative
SCFE and Perthes disease commonly present as knee pain in children due to referred pain along the obturator nerve. In ANY child presenting with knee pain, especially if obesity or limited hip ROM is present, you MUST examine the hip. Missing SCFE can lead to avascular necrosis and hip destruction.
SLJSLJ - Clinical Features
Hook:SLJ affects the Superior-Lower Junction of the patellar tendon - where it originates from the inferior pole of the patella.
Investigations
Sinding-Larsen-Johansson is a CLINICAL diagnosis. Imaging is NOT required in typical cases. Key clinical features (point tenderness over inferior pole of patella in athletic adolescent during growth spurt) are sufficient for diagnosis. Reserve imaging for atypical presentations or to exclude other pathology.
When to Order Imaging:
- Acute traumatic event (rule out avulsion fracture)
- Atypical age (too young or too old for SLJ)
- Night pain or rest pain (rule out tumor)
- Effusion (unusual for SLJ)
- Failure to improve with 3-6 months conservative treatment
- Suspected loose ossicle in symptomatic adult
- Soft tissue swelling anterior to inferior pole
- Fragmentation of inferior pole ossification center
- Irregular ossification of apophysis
- Separate ossicle at inferior pole (may persist)
- Calcification at inferior pole post-fusion
Other Imaging:
- Indication
- First-line if imaging needed
- Findings
- Soft tissue swelling, fragmentation, ossicle
- Clinical Use
- Confirm diagnosis, rule out fracture
- Indication
- Assess patellar tendon, soft tissues
- Findings
- Tendon thickening, fragmentation, bursa
- Clinical Use
- Useful if tendinopathy suspected
- Indication
- Rule out tumor, stress fracture, infection
- Findings
- Edema at inferior pole, soft tissue changes
- Clinical Use
- Rarely needed - reserve for red flags
Management Algorithm
Non-Operative Management (First-Line for ALL Cases)
95%+ of SLJ resolves with conservative treatment alone.
Conservative Treatment Protocol
- Do NOT stop all activity - reduce intensity and volume
- Avoid painful activities (deep squats, jumping, kneeling)
- Continue sport at reduced level if tolerable
- Cross-train with low-impact activities (swimming, cycling)
- Ice after activity (15-20 minutes) for symptom relief
- Quadriceps stretching: Reduces traction force on inferior pole
- Hamstring stretching: Decreases quadriceps demand
- Hip flexor stretching: Improves mechanics
- Hold stretches 30 seconds, 3-4 times daily
- Dynamic warm-up before activity
- Eccentric quadriceps: Once acute pain settles
- Core stability: Reduce load on knee during activity
- Hip strengthening: Improve biomechanics
- Progress gradually as symptoms allow
- Patellar strap/brace: Reduces traction on inferior pole
- Knee pad: Protects inferior pole when kneeling
- NSAIDs: Short-term for acute flares (not long-term)
- Ice/heat: Symptom relief
Prolonged complete rest is NOT recommended. It weakens muscles, detrains the athlete, and delays return to sport. Modify activity to a tolerable level rather than stopping entirely. The exception is severe cases with rest pain, which may need a short period of immobilization.
TREATTREAT - Treatment Approach
Hook:TREAT SLJ with Tender care - this is self-limiting, don't over-treat.
Surgical Technique
Ossicle Excision (Adults Only)
Surgery for Sinding-Larsen-Johansson syndrome is extremely rare and reserved for symptomatic ossicle in adults (post-skeletal maturity) or persistent pain from calcification. Surgery is NOT indicated for active SLJ in adolescents.
- Skeletal maturity (closed patellar apophysis)
- Persistent focal pain over ossicle
- Failed conservative management (6+ months)
- Imaging confirms symptomatic ossicle at inferior pole
- Longitudinal or transverse incision over inferior pole
- Identify ossicle at patellar tendon origin
- Excise ossicle, debride tendon edges
- Repair tendon if needed
- Some surgeons also smooth prominent inferior pole
This is a straightforward procedure with excellent outcomes in appropriately selected patients.
Inferior-pole pain is age-determined at the same anatomical site. In the skeletally immature athlete with an open apophysis it is SLJ (traction apophysitis); once the apophysis has fused, identical proximal-patellar-tendon pain in a jumping athlete is patellar tendinopathy (jumper's knee) - an overload tendinopathy of the deep proximal tendon fibres rather than a bone-apophysis problem. The pivot matters because management changes with maturity: SLJ is self-limiting and treated with activity modification, stretching and reassurance, whereas jumper's knee is driven by a structured progressive loading programme - eccentric decline-squat or heavy-slow-resistance training - with imaging-guided injection or surgery reserved for refractory cases. So in the 16-18-year-old with the "same" history, confirm skeletal maturity and shift both the diagnosis and the rehabilitation accordingly rather than labelling it persistent SLJ.
Complications
- Incidence
- Common (30-50%)
- Risk Factors
- Part of natural history
- Management
- Reassurance - cosmetic only, does not affect function
- Incidence
- Rare (less than 1%)
- Risk Factors
- Acute trauma in severe SLJ
- Management
- Surgical ORIF if displaced, cast if non-displaced
- Incidence
- 5-10%
- Risk Factors
- Large initial ossicle, non-compliance
- Management
- Ossicle excision if failed conservative treatment
- Incidence
- Uncommon
- Risk Factors
- Return to sport too early, ongoing overuse
- Management
- Eccentric loading program, activity modification
- Incidence
- 10-20%
- Risk Factors
- Calcification persists
- Management
- Knee pads, reassurance, rarely surgical reduction
Inferior pole avulsion fracture is DIFFERENT from SLJ. Avulsion is acute, traumatic, with sudden pain and inability to extend knee. It requires urgent orthopaedic referral. SLJ is chronic, overuse, with gradual onset and preserved extension. Do not confuse these conditions.
The acute injury that mimics SLJ is the patellar sleeve fracture, a paediatric avulsion (peak 8-12 years) in which a sleeve of cartilage and periosteum is stripped off the pole of the patella, taking only a tiny fleck of bone. The classic trap is that the plain radiograph grossly under-represents the injury - the visible osseous fragment is small while the avulsed cartilage sleeve is large - so the true extensor-mechanism disruption is easily missed. Look for patella alta on the lateral film (the patella rides high once the inferior tether is lost), a palpable gap below the patella, and inability to perform a straight-leg raise or actively extend the knee. Most occur at the inferior pole (superior-pole and medial/lateral variants are described). Because the cartilage is radiolucent, MRI or ultrasound defines the true extent. Unlike SLJ this is a surgical injury: a displaced sleeve fracture needs open reduction and fixation (suture/anchor or tension-band) to restore the extensor mechanism, with the physis respected. This is the entity the viva is probing when it asks you to classify an "inferior pole avulsion."
Postoperative Care and Rehabilitation
Rehabilitation for Ossicle Excision (Adults)
Post-Ossicle Excision Protocol
- Weight-bearing as tolerated
- ROM exercises as comfort allows
- Ice, elevation for swelling
- Gentle quadriceps sets
- Full ROM expected by 6 weeks
- Progressive strengthening
- Bike, swimming for cardio
- Avoid deep squats, jumping
- Sport-specific training
- Plyometrics progression
- Jogging, running progression
- Full return based on strength testing
- Typically 3-4 months for full competition
- Ongoing maintenance stretching
Rehabilitation for Conservative SLJ (Adolescents)
This is the main patient population - structured rehab program while continuing modified activity:
- Daily stretching: Quadriceps, hamstrings, hip flexors (30 sec × 3)
- Eccentric strengthening: When acute pain settles
- Core stability exercises
- Sport modification: Continue at reduced level
- Ice after activity
- Gradual progression as symptoms allow
Outcomes
- Excellent prognosis - most cases resolve completely with skeletal maturity
- Symptoms typically improve within 1-2 years (when patellar apophysis fuses)
- Persistent calcification at inferior pole is common but NOT a functional problem
- Most athletes return to full sport without long-term issues
- 5-10% have some adult symptoms, usually mild or related to ossicle
- Severe initial presentation
- Delay in activity modification
- Ongoing intense sports participation without modification
- Bilateral involvement
- Coexisting Osgood-Schlatter disease
Parents often worry about the residual calcification at the inferior pole. Reassure them this is part of the normal healing process - the calcification represents bone that formed during the inflammatory phase and is now incorporated into the mature patella. It is cosmetic only and does not affect function or sports performance.
Guidelines, Registries & Global Practice
Global epidemiology. Sinding-Larsen-Johansson syndrome is a worldwide condition of the skeletally immature, jumping/running athlete and is consistently reported as less common than its sister apophysitis, Osgood-Schlatter disease. As girls' participation in jumping and running sports has grown internationally, female incidence is rising and the historical male predominance is narrowing. In an unselected population-based Dutch adolescent cohort (3800 knees, ages 12-15), MRI features of SLJ were present in 0.8% versus 2.3% for OSD, according to PubMed (DOI). Accessory-ossicle prevalence rises markedly in high-load youth sport: elite male soccer players show roughly 3-fold higher apophyseal ossicle rates than controls (DOI). There is no dedicated SLJ registry; surveillance comes from sports-medicine cohorts and imaging-prevalence studies rather than arthroplasty-style national registries.
Guideline landscape. No major society publishes an SLJ-specific guideline; recommendations are extrapolated from paediatric overuse-injury and apophysitis guidance, which is strikingly consistent across systems:
- Position
- Activity modification, relative rest, quadriceps/hamstring flexibility; reassurance about self-limiting course
- Imaging Stance
- Clinical diagnosis; radiograph only for atypical features or to exclude other pathology
- Evidence Basis
- Expert consensus / Level 5 (no high-level RCTs)
- Position
- Primary-care conservative management, load modification, physiotherapy; orthopaedic referral reserved for red flags
- Imaging Stance
- Imaging not routine; reserved for diagnostic uncertainty or trauma
- Evidence Basis
- CKS-type narrative guidance, consensus-based
- Position
- Conservative, family education; avoid overinvestigation of incidental ossicles
- Imaging Stance
- Selective imaging only
- Evidence Basis
- Consensus / practice standards
- Position
- Load management and graded return; flag prolonged courses for follow-up
- Imaging Stance
- Ultrasound or MRI selectively for atypical or refractory cases
- Evidence Basis
- Cohort evidence (Level 3-4)
- Position
- Training-load monitoring during growth spurts, gradual return-to-sport progression
- Imaging Stance
- Clinical diagnosis emphasised
- Evidence Basis
- Consensus / sports guidance
The main international variation is in imaging threshold and follow-up intensity, not in treatment: management is uniformly conservative worldwide. Higher-resource and elite-sport settings use ultrasound/MRI more liberally and monitor load formally, while primary-care systems (e.g. NHS) keep the diagnosis clinical. Emerging cohort data (apophysitis pain persisting in roughly one-third at 2 years, DOI) is shifting guidance toward longer, structured follow-up rather than one-off reassurance.
Medicolegal Considerations:
Key documentation points:
- Clear history of gradual onset and activity-related symptoms
- Documentation of point tenderness specifically over inferior pole of patella
- Hip examination performed (to exclude SCFE/Perthes)
- Discussion of self-limiting nature and expected timeline (counsel that a minority take 1-2+ years)
- Activity modification advice given (not complete rest)
Don't Miss SCFE: SCFE commonly presents as knee pain in obese adolescent males. Missing SCFE diagnosis causes significant morbidity from AVN. Document hip examination in ALL adolescents presenting with knee pain. This is a frequent source of litigation in paediatric orthopaedics.
Prevention Strategies:
- Training-load management during growth spurts (volume progression before intensity)
- School and club programmes increasingly aware of growth-spurt overuse risk
- Pre-season flexibility screening may identify at-risk athletes (tight quadriceps/hamstrings)
MCQ Practice Points
Q: An adolescent presents with knee pain after jumping. How do you distinguish SLJ from avulsion fracture? A: SLJ has GRADUAL onset, pain during/after activity, ability to extend knee, and no visible deformity. Avulsion has ACUTE onset after trauma, inability to extend knee, visible/palpable deformity, and severe pain. X-ray shows displaced fragment in avulsion vs fragmentation in SLJ.
Q: Which of the following is an indication for X-ray in suspected SLJ? A: Night pain (rule out tumor), acute traumatic onset (rule out avulsion), failure to improve after 6 months conservative treatment, atypical age (less than 8 or after skeletal maturity). Routine SLJ does NOT require imaging.
Q: What is the recommended activity level for adolescent with SLJ? A: Activity MODIFICATION, not complete rest. Continue sport at reduced level if tolerable. Avoid painful activities (deep squats, kneeling, jumping). Cross-train with low-impact activities. Complete rest weakens muscles and delays return.
Q: What happens to the calcification after SLJ resolves? A: The inferior pole calcification typically persists as a painless, cosmetic finding in 30-50% of patients. This represents ossification that occurred during the healing process and is now incorporated into the mature patella. It is NOT a complication and does not affect function.
Q: A 12-year-old with knee pain has point tenderness at the INFERIOR POLE of patella. What is the diagnosis? A: Sinding-Larsen-Johansson syndrome - traction apophysitis at the inferior pole of patella (where patellar tendon originates). Same mechanism as Osgood-Schlatter but at the proximal end of the patellar tendon. Treatment is identical - activity modification, stretching, ice.
Q: How does SLJ differ from Osgood-Schlatter disease? A: SLJ affects the inferior pole of the patella (patellar tendon origin) while OSD affects the tibial tubercle (patellar tendon insertion). Both are traction apophysitides with the same mechanism, age group, and treatment. Patients may have both conditions simultaneously.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 12-year-old boy who plays basketball presents with 2 months of anterior knee pain. The pain is worse after training and he has point tenderness at the front of his knee.”
“A 13-year-old female gymnast presents with bilateral anterior knee pain. On examination, she has tenderness at both the inferior pole of the patella and the tibial tubercle bilaterally.”
“A 14-year-old basketball player jumps for a rebound and lands with sudden severe knee pain. He cannot extend his knee and you notice tenderness and swelling over the inferior pole of the patella.”
Key Anatomy
- Inferior pole of patella = patellar tendon origin
- Secondary ossification center at inferior pole
- Apophysis fuses during adolescence (14-18 years)
- Opposite end of patellar tendon from Osgood-Schlatter
Diagnosis
- Clinical diagnosis - imaging not required
- Point tenderness over inferior pole of patella
- Pain with resisted knee extension
- 10-14 years, athletic, growth spurt
Treatment
- Activity MODIFICATION not complete rest
- Stretching: quads, hamstrings, hip flexors
- Ice after activity (15-20 min)
- Patellar strap during sport
- NSAIDs short-term for flares only
Imaging Indications
- Acute traumatic onset (avulsion)
- Night pain (tumor)
- Failure after 6 months conservative
- Atypical age or presentation
Red Flags
- Acute trauma with inability to extend = AVULSION
- Night/rest pain = tumor, infection
- Knee effusion = not typical for SLJ
- Hip symptoms = SCFE, Perthes
Prognosis
- 90%+ resolve with skeletal maturity
- Duration 1-2 years (until physis closes)
- Calcification persists but is painless
- 5-10% adult symptoms (usually ossicle)
Evidence Base
SLJ has a small dedicated literature, so much of the practice base is shared with Osgood-Schlatter disease (OSD) and patellar tendinopathy, which sit at the opposite ends of the same extensor mechanism. Each card below is verified against PubMed; where direct SLJ data are sparse, high-quality apophysitis evidence is used and labelled as such.
Defining Natural-History Study (Original Prospective Series)
- Prospective study of 8 patients (10 knees) with clinical and radiographic SLJ
- Aetiology described as traction tendinitis with de novo calcification at the patellar tendon proximal attachment, which had partially avulsed
- Course was self-limited and benign, paralleling Osgood-Schlatter disease
- Residual calcification at the inferior pole was common and asymptomatic
Population Prevalence on Adolescent Knee MRI
- Population-based cohort of 1910 adolescents (3800 knees) imaged at age 12-15 years
- Sinding-Larsen-Johansson characteristics seen in 16 participants (0.8%); Osgood-Schlatter in 43 (2.3%)
- At least one abnormality or normal variant present in 19.4% of unselected adolescents
- Bone marrow oedema and Osgood-Schlatter were more common in boys
Mechanical Loading and Ossicle Formation in Elite Athletes
- Cross-sectional comparison of 334 knees of male professional soccer players versus 223 control knees
- Players had significantly higher tuberosity height ratio, steeper posterior tibial slope, and more Osgood-Schlatter ossicles (10.8% vs 3.1%)
- Dominant-side tuberosity prominence and slope were greater than non-dominant
- Findings attributed to repetitive mechanical loading during skeletal growth
Acute Presentation Mimicking Patellar Sleeve Fracture
- 10-year-old boy with sudden anterior knee pain after a non-contact soccer injury
- Radiographs showed a minimally displaced distal patellar ossicle suggestive of SLJ
- MRI excluded a cartilaginous sleeve injury and confirmed SLJ
- Brief immobilisation gave complete radiographic healing by 4 weeks
Apophysitis Prognosis Is Not Always Benign (OSD Analogue)
- Prospective cohort of 51 adolescents (10-14 y) with Osgood-Schlatter, 90% followed to 24 months
- 37% still had apophysitis-related knee pain at 2 years; over 1 in 5 had stopped sport
- Persistent pain was associated with worse KOOS Sport/Recreation and quality of life
- An ununited ossicle was present in 32% of those rescanned at follow-up
Eponym and Historical Context
- Biographical review of Christian Magnus Falsen Sinding-Larsen (1866-1930), Norwegian physician
- Documents the origin of the SLJ eponym in the musculoskeletal radiology literature
- Describes the original radiographic descriptions of inferior-pole change
- Places SLJ within the family of described osteochondroses