Post-Traumatic Lateral Hindfoot Pain | Sinus Tarsi Tenderness | Conservative First
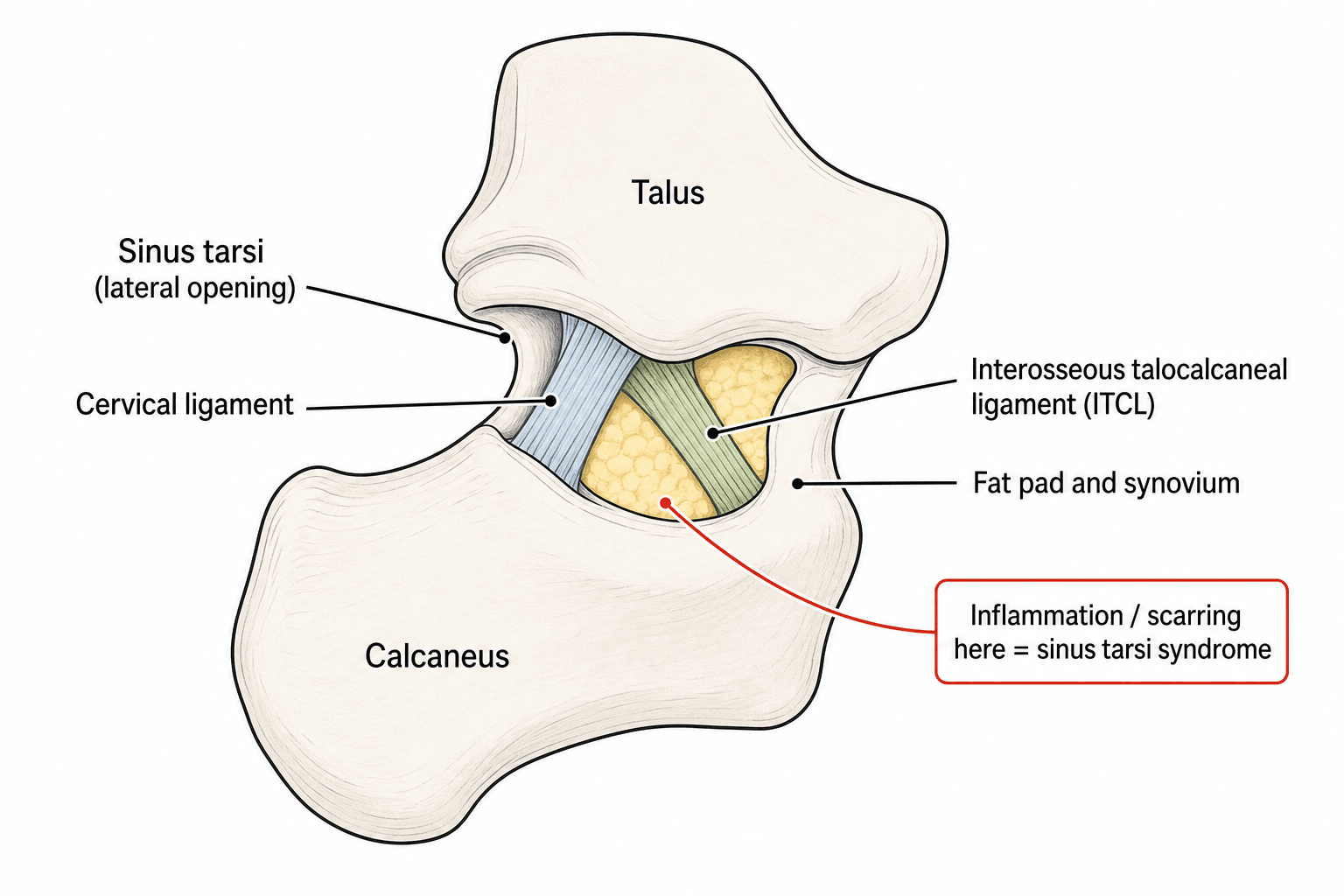
- Sinus Tarsi Anatomy: Conical tunnel between talus and calcaneus, contains interosseous talocalcaneal ligament, cervical ligament, fat, and mechanoreceptors
- Post-Traumatic Etiology: 90% follow ankle inversion injury - disrupts ligaments and fat pad
- Clinical Triad: Lateral hindfoot pain, sinus tarsi tenderness, sensation of hindfoot instability
- MRI Findings: High signal in sinus tarsi on T2, ligament disruption, fat pad edema
- Conservative First: 70-80% respond to physiotherapy, injections, and proprioceptive training
- “Sinus tarsi is anterior and lateral to lateral malleolus
- “Pain worse on uneven ground and lateral movements
- “Single-leg stance reveals hindfoot instability
- “Diagnostic injection provides immediate but temporary relief
Sinus tarsi is a cone-shaped tunnel located between the talus superiorly and calcaneus inferiorly, opening laterally anterior to the lateral malleolus. Contains the interosseous talocalcaneal ligament (ITCL), cervical ligament, inferior extensor retinaculum, fat pad, and rich mechanoreceptors. Injury disrupts proprioception.
90% follow ankle inversion injury. The mechanism is forceful inversion that crushes the lateral structures of the sinus tarsi, disrupting ligaments and fat pad. Chronic inflammation, synovitis, and adhesions develop. Often associated with lateral ankle instability.
Triad: Vague lateral hindfoot pain, point tenderness over sinus tarsi, and sensation of instability on uneven ground. Pain reproduced by forced inversion and eversion. Negative anterior drawer (unless coexisting ATFL injury). MRI confirms with high T2 signal in sinus tarsi.
70-80% respond to non-operative treatment. Physiotherapy with proprioceptive training is key. Diagnostic and therapeutic corticosteroid injection into sinus tarsi provides temporary relief and confirms diagnosis. Surgery reserved for refractory cases after 6 months.
- Clinical Features
- Recent inversion injury, lateral pain
- Management
- Rest, NSAIDs, physiotherapy, ankle brace
- Key Pearl
- Most resolve with conservative treatment
- Clinical Features
- Persistent pain, sinus tarsi tenderness
- Management
- Corticosteroid injection, proprioceptive training
- Key Pearl
- Injection confirms diagnosis if relief obtained
- Clinical Features
- Failed conservative, MRI shows synovitis
- Management
- Arthroscopic sinus tarsi debridement
- Key Pearl
- Exclude subtalar arthritis before surgery
LATERALDifferential Diagnosis
Hook:LATERAL foot pain has many causes - exclude these before diagnosing sinus tarsi syndrome!
Overview and Epidemiology
Sinus tarsi syndrome is an underdiagnosed cause of chronic lateral ankle pain following inversion injury. The syndrome was first described by O'Connor in 1958 as a clinical entity distinct from lateral ankle ligament injury. It represents chronic inflammation and scarring within the sinus tarsi following disruption of its contents. The vague nature of symptoms and lack of specific tests lead to delayed diagnosis averaging 6-12 months from injury.
- Antecedent injury: Lateral ankle sprain is the commonest precursor; ankle sprain incidence in the US general population is approximately 2.15 per 1000 person-years, peaking at 7.2 per 1000 at age 15-19 years (Waterman 2010)
- Post-sprain risk: In one cohort, 22.5% of patients developed sinus tarsi syndrome after lateral ankle sprain (Xu 2024)
- Age: Typically active adults; reported series average around 30-41 years
- Athletic: Half of ankle sprains occur during sport, most often basketball, football, and soccer (Waterman 2010)
- Bilateral: Usually unilateral
Young active individuals with a history of inadequately rehabilitated ankle sprains are typical. Note that "sinus tarsi syndrome" is increasingly regarded as a descriptive umbrella term rather than a single discrete pathology (Frey 1999, Willegger 2023).
Predisposing factors:
- Previous ankle inversion injury (90% of cases)
- Chronic lateral ankle instability
- Repetitive microtrauma (running, jumping)
- Hindfoot valgus alignment
- Generalized ligamentous laxity
- Inflammatory arthropathy (RA, seronegative)
Protective factors:
- Proper ankle rehabilitation after sprains
- Proprioceptive training
- Ankle bracing during sports
History of inadequately rehabilitated ankle sprain is almost universal.
The differential examiners most want distinguished from sinus tarsi syndrome after an inversion sprain is anterolateral ankle soft-tissue impingement - and the key is pain LOCATION.
- Pathology: after an inversion injury, hypertrophic synovium and scar form a "meniscoid" soft-tissue lesion in the anterolateral gutter (between the lateral talus, the fibula and the anteroinferior tibiofibular ligament); a thickened distal fascicle of the AITFL - Bassett's ligament - can also impinge on the anterolateral talar dome.
- Clinical: chronic anterolateral ankle pain over the joint line/gutter (more anterior and superior than the sinus tarsi), worse on dorsiflexion/eversion and push-off, with a positive anterolateral impingement test (pain/tenderness on dorsiflexion). Contrast with sinus tarsi pain, which is over the lateral hindfoot sinus tarsi opening and is worse on uneven ground.
- Diagnosis: largely clinical; MRI or MR-arthrography shows the anterolateral soft-tissue mass; diagnostic arthroscopy is confirmatory.
- Management: physiotherapy first, then arthroscopic debridement of the meniscoid lesion / Bassett's ligament for refractory cases (good results).
Exam point: post-sprain lateral pain that is anterolateral over the joint line and worse on dorsiflexion is anterolateral impingement (meniscoid lesion / Bassett's ligament), not sinus tarsi syndrome.
Anatomy and Pathophysiology
Sinus Tarsi Anatomy
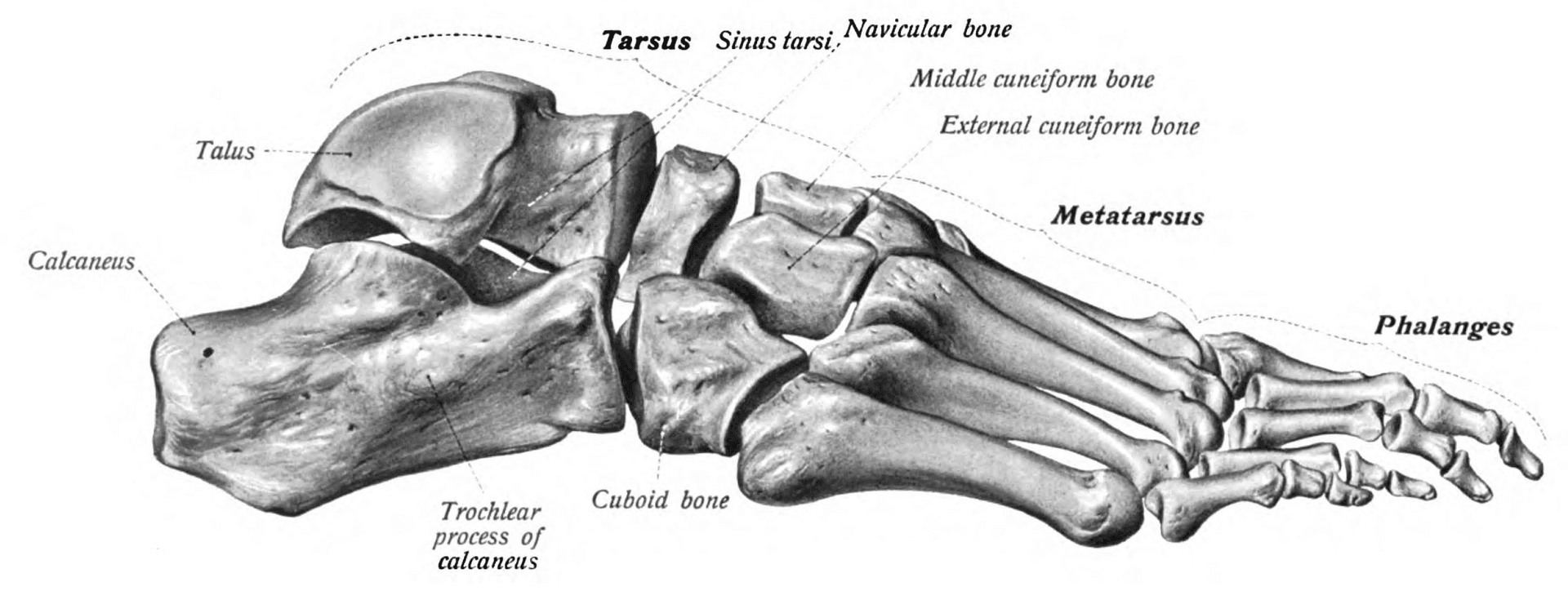
The sinus tarsi is a cone-shaped tunnel between the talus and calcaneus. The wide opening faces laterally (anterior and inferior to lateral malleolus). The narrow apex points medially and becomes the tarsal canal (containing posterior tibial neurovascular bundle). Boundaries: Superior - neck and body of talus. Inferior - superior surface of calcaneus. Medial - tarsal canal. Lateral - opens between anterior process of calcaneus and talar neck.
Sinus Tarsi Contents:
- Anatomy
- Strong ligament in tarsal canal, two bands
- Function
- Primary stabilizer of subtalar joint
- Injury Effect
- Disruption causes subtalar instability
- Anatomy
- Oblique ligament from talar neck to calcaneus
- Function
- Restricts inversion, secondary stabilizer
- Injury Effect
- Injury common in inversion sprains
- Anatomy
- Crosses lateral opening of sinus tarsi
- Function
- Restrains extensor tendons
- Injury Effect
- Thickening contributes to stenosis
- Anatomy
- Adipose tissue filling the sinus
- Function
- Shock absorption, gliding surface
- Injury Effect
- Inflammation, fibrosis after trauma
- Anatomy
- Dense proprioceptive nerve endings
- Function
- Proprioception for hindfoot position
- Injury Effect
- Loss causes instability sensation
- Anatomy
- Extension of subtalar joint synovium
- Function
- Joint lubrication
- Injury Effect
- Chronic synovitis, adhesions
Clinical Relevance:
- The sinus tarsi is palpable anterior to the lateral malleolus
- Depth: approximately 1-2 cm from skin surface
- Width at lateral opening: 1-2 cm diameter
- Rich vascular and nerve supply explains pain severity
Pathophysiology
Initial trauma (ankle inversion):
- Forced inversion crushes lateral sinus tarsi structures
- Disruption of cervical and interosseous ligaments
- Fat pad contusion and hemorrhage
- Synovial membrane inflammation
- Nerve ending trauma
This acute phase lasts 2-6 weeks.
Chronic inflammation develops:
- Persistent synovitis
- Fibrosis and adhesions
- Scar tissue formation
- Fat pad degeneration
- Loss of proprioceptive function
- Secondary subtalar instability
Chronic changes perpetuate symptoms beyond 3-6 months.
Proposed Mechanisms:
- Mechanical compression: Inversion crushes lateral sinus tarsi contents between talus and calcaneus
- Ligamentous disruption: Cervical and ITCL partial tears lead to microinstability
- Proprioceptive loss: Mechanoreceptor damage causes subjective instability and poor proprioception
- Inflammatory cascade: Chronic synovitis perpetuates pain
- Scar tissue stenosis: Adhesions narrow the sinus tarsi, causing impingement
Classification Systems
Classification by Duration
- Duration
- Under 3 months
- Pathology
- Acute inflammation, edema
- Treatment Approach
- Conservative - rest, NSAIDs, physio
- Duration
- 3-6 months
- Pathology
- Persistent synovitis, early fibrosis
- Treatment Approach
- Injection therapy, proprioceptive training
- Duration
- Over 6 months
- Pathology
- Fibrosis, adhesions, stenosis
- Treatment Approach
- Consider surgical debridement
Stage determines management approach and prognosis.
Clinical Assessment
Classic presentation:
- Pain location: Vague lateral hindfoot pain anterior to lateral malleolus
- Character: Deep, aching, poorly localized
- Onset: Gradual after ankle inversion injury (weeks to months)
- Aggravating factors: Uneven ground, stairs, slopes, lateral movements
- Associated symptoms: Sensation of instability, giving way
- Previous injury: 90% report ankle sprain 3-12 months prior
The triad of lateral pain, sinus tarsi tenderness, and instability sensation is pathognomonic.
Key findings:
- Inspection: Usually normal, may have mild lateral swelling
- Palpation: Exquisite point tenderness over sinus tarsi (anterior to lateral malleolus)
- Range of motion: Subtalar motion painful at extremes of inversion and eversion
- Forced inversion test: Reproduces pain in sinus tarsi
- Forced eversion test: Also reproduces pain
- Anterior drawer: Usually negative unless coexisting ATFL injury
- Single-leg stance: Reveals proprioceptive deficit, hindfoot instability
Sinus tarsi point tenderness is the most reliable clinical sign.
Special Tests
- Technique
- Press 1 cm anterior and inferior to lateral malleolus
- Positive Finding
- Exquisite point tenderness
- Sensitivity/Specificity
- High sensitivity (over 90%), moderate specificity
- Technique
- Passively invert hindfoot, apply axial pressure
- Positive Finding
- Pain reproduced in sinus tarsi
- Sensitivity/Specificity
- Moderate sensitivity and specificity
- Technique
- Passively evert hindfoot
- Positive Finding
- Pain in sinus tarsi (compression of lateral contents)
- Sensitivity/Specificity
- Lower sensitivity than inversion
- Technique
- Stand on affected leg 30 seconds
- Positive Finding
- Difficulty maintaining balance, subjective instability
- Sensitivity/Specificity
- Reflects proprioceptive deficit
- Technique
- Inject 2 mL lidocaine into sinus tarsi
- Positive Finding
- Immediate pain relief confirms diagnosis
- Sensitivity/Specificity
- High specificity (over 90%)
Must exclude:
- Lateral ankle instability: Positive anterior drawer, talar tilt. May coexist with sinus tarsi syndrome.
- Subtalar arthritis: Older age, crepitus, reduced subtalar motion. X-ray shows joint space narrowing.
- Peroneal tendinopathy: Tenderness posterior to lateral malleolus, pain with resisted eversion.
- Stress fracture: Calcaneus, talus. High index of suspicion in athletes. MRI shows bone marrow edema.
- Tarsal coalition: Rigid flat foot, usually younger age. CT diagnostic.
- L5-S1 radiculopathy: Back pain, dermatomal sensory loss, weakness.
Coexisting lateral ankle instability is found in 30-40% and should be addressed surgically if present.
A high-yield nuance: some cases labelled sinus tarsi syndrome are genuinely subtalar instability, which is debridement-resistant and needs ligament reconstruction.
- Anatomy: the interosseous talocalcaneal ligament (ITCL) and cervical ligament - both sinus tarsi contents - are the primary stabilisers of the subtalar joint; their disruption in an inversion injury produces subtalar instability, not merely inflammation. This is why debridement must preserve these ligaments.
- The diagnostic difficulty: subtalar instability is clinically very hard to separate from talocrural (ankle/ATFL) instability - both give a feeling of "giving way" on uneven ground with lateral hindfoot pain, and the anterior drawer/talar tilt test the ankle, not the subtalar joint.
- Imaging: Broden stress views and subtalar stress radiography have been used but are poorly standardised and unreliable; MRI/MR-arthrography and diagnostic arthroscopy help, and a bilateral comparison is essential.
- Management implication: where genuine subtalar (ITCL/cervical ligament) instability is present, debridement alone is inadequate - it requires anatomic ligament reconstruction, with any coexisting ATFL/CFL instability addressed (e.g. a Brostrom-type repair extended to the subtalar stabilisers).
Exam point: persistent post-sprain "giving way" with sinus tarsi pain should raise subtalar instability - it is hard to demonstrate clinically, and true instability needs ligament reconstruction, not just debridement.
TENDERClinical Features of Sinus Tarsi Syndrome
Hook:The sinus tarsi is TENDER to palpation - this is the pathognomonic clinical sign!
Investigations
Investigation Algorithm
Diagnosis is primarily clinical based on history (post-inversion lateral hindfoot pain) and examination (sinus tarsi point tenderness). No investigations required if typical presentation and good response to initial conservative treatment.
Weight-bearing AP, lateral, and mortise ankle views:
- Usually normal in sinus tarsi syndrome
- Exclude fractures, arthritis, tarsal coalition
- Assess hindfoot alignment (valgus, varus)
- Check for talar tilt (lateral instability)
Findings: Normal in isolated sinus tarsi syndrome. May show signs of chronic lateral instability.
Gold standard for diagnosis:
T2-weighted sequences show:
- High signal intensity in sinus tarsi (edema, inflammation)
- Fat pad signal changes
- Disruption of cervical ligament
- ITCL abnormalities
- Synovitis, fluid in subtalar joint
- Exclude subtalar arthritis
Sensitivity 80-90% for sinus tarsi pathology.
Ultrasound or fluoroscopy-guided injection:
- 2 mL 1% lidocaine into sinus tarsi
- Immediate pain relief confirms diagnosis
- Can combine with corticosteroid for therapeutic effect
Specificity over 90% - positive response confirms sinus tarsi syndrome as pain source.
Typical findings:
- High T2 signal in sinus tarsi (greater than 90%)
- Fat pad edema and inflammation
- Cervical ligament disruption or thickening
- ITCL signal abnormality
- Subtalar joint effusion
- Synovial thickening
Sensitivity: 80-90% for diagnosis
Dynamic assessment:
- Evaluate sinus tarsi soft tissues
- Assess cervical ligament integrity
- Identify fluid collections
- Guide injection placement
Advantages: Dynamic, real-time, cost-effective. Operator-dependent.
Management Algorithm

Conservative Management (First-Line)
Initial Management (Under 3 Months)
Goal: Reduce inflammation, restore proprioception, prevent chronicity
Conservative Protocol
- Reduce impact activities
- Avoid uneven surfaces
- Use lateral ankle brace or taping
- Continue non-impact exercise (swimming, cycling)
Relative rest allows acute inflammation to settle.
- NSAIDs: Regular dosing for 3-4 weeks
- Ice therapy: 15 minutes 3-4 times daily
- Compression: Ankle sleeve or wrap
Controls acute inflammatory response.
Key interventions:
- Range of motion: Subtalar joint mobility exercises
- Strengthening: Peroneal and tibialis posterior strengthening
- Proprioceptive training: Balance board, single-leg stance (critical)
- Manual therapy: Soft tissue mobilization
Proprioceptive retraining is the most important component.
- Lateral wedge: Reduces inversion stress
- Cushioned heel: Shock absorption
- Arch support: Controls excessive pronation
Biomechanical support reduces sinus tarsi loading.
Expected outcome: 50-60% improve with conservative treatment alone within 3 months.
Surgical Technique - Arthroscopic Sinus Tarsi Debridement
Indications for Surgery
All of the following must be met:
- Minimum 6 months failed conservative treatment
- Documented compliance with physiotherapy and proprioceptive training
- Failed injection therapy (at least one corticosteroid injection)
- MRI confirms sinus tarsi pathology (synovitis, adhesions)
- Pain significantly limiting activities
- Exclusion of subtalar arthritis (poor surgical outcomes)
Contraindications:
- Active infection
- Subtalar arthritis (consider arthrodesis instead)
- Inadequate conservative trial
- Inflammatory arthropathy (higher failure rate)
- Unrealistic expectations
Arthroscopic Sinus Tarsi Debridement
Advantages over open:
- Smaller incisions
- Less soft tissue disruption
- Faster recovery
- Better visualization
- Lower complication rate
Surgical Steps
- Lateral decubitus position with affected side up
- Beanbag or lateral positioning device
- Thigh tourniquet applied
- Ankle and foot prepped free
- C-arm available for portal placement
Anterolateral portal:
- Just anterior to tip of lateral malleolus
- At level of ankle joint
- For visualization
Sinus tarsi portal:
- 1-2 cm anterior and inferior to lateral malleolus
- Directly into sinus tarsi opening
- For instrumentation
Mark portals before inflation to identify landmarks.
- Insert 2.7 mm 30-degree arthroscope via anterolateral portal
- Navigate to sinus tarsi
- Inspect contents: Synovitis, adhesions, scar tissue
- Switch to sinus tarsi portal for direct access
- Debride inflamed synovium with shaver
- Remove scar tissue and adhesions
- Preserve cervical and ITCL ligaments (do not excise)
- Irrigate thoroughly
Goal is debridement of pathologic tissue while preserving ligamentous stability.
- View subtalar joint through sinus tarsi
- Assess for articular cartilage damage
- If significant arthritis, reconsider surgical plan
- May require arthrodesis instead
- Irrigate portals
- Close skin only with nylon suture
- Soft compressive dressing
- Non-weight bearing for first week in boot
Minimal closure required for arthroscopic technique.
Key technical points:
- Preserve ligaments - debride synovium and scar only
- Thorough debridement of all inflamed tissue
- Assess subtalar joint for arthritis
- Gentle technique to avoid iatrogenic damage
These steps ensure optimal outcomes while preserving stability.
SINUSSinus Tarsi Contents
Hook:The SINUS contains five key structures - disruption causes pain and instability!
Complications
- Incidence
- 20-30%
- Risk Factors
- Subtalar arthritis, inflammatory arthropathy, inadequate debridement
- Management
- Reassess for missed pathology, consider subtalar arthrodesis
- Incidence
- 5-10%
- Risk Factors
- Open technique, inadequate visualization
- Management
- Numbness dorsum of foot. Usually recovers 3-6 months. Desensitization if persistent
- Incidence
- 5%
- Risk Factors
- Open surgery, smoking, diabetes
- Management
- Wound care, antibiotics if infection. Delayed healing common with open technique
- Incidence
- 10-15%
- Risk Factors
- Aggressive debridement, prolonged immobilization
- Management
- Physiotherapy, mobilization. Rarely clinically significant
- Incidence
- 10-20%
- Risk Factors
- Incomplete debridement, untreated instability
- Management
- Revision debridement or consider arthrodesis
- Incidence
- Rare (under 5%)
- Risk Factors
- Excessive ligament excision
- Management
- Prevention: Preserve cervical and ITCL. Treatment: Lateral ligament reconstruction
Most common cause of surgical failure is unrecognized subtalar arthritis. Preoperative MRI must assess subtalar joint cartilage. If arthritis present, counsel patient that debridement alone has 40-60% failure rate, and subtalar arthrodesis may be necessary.
Other causes of persistent pain:
- Incomplete debridement of pathologic tissue
- Coexisting lateral ankle instability not addressed
- Inflammatory arthropathy (RA, seronegative)
- Wrong diagnosis (L5-S1 radiculopathy, peroneal pathology)
Postoperative Care and Rehabilitation
Rehabilitation After Arthroscopic Debridement
- Below-knee boot or CAM walker
- Non-weight bearing first week
- Partial weight-bearing week 2 (if minimal pain)
- Elevate, ice, analgesia
- Ankle pumps and toe exercises
- Sutures removed at 2 weeks
- Weight-bearing as tolerated in boot
- Begin gentle range of motion exercises
- Subtalar mobilization (plantarflexion-inversion, dorsiflexion-eversion)
- Proprioceptive training: Balance board, single-leg stance
- Continue ice and elevation
Proprioceptive retraining is critical to prevent recurrence.
- Wean from boot to supportive shoes
- Progressive strengthening: Peroneal, tibialis posterior
- Advance proprioception: Unstable surfaces, eyes closed
- Start low-impact activities (swimming, cycling)
- Gradual return to walking, then light jogging
Most patients return to full activity by 3 months.
- Sport-specific training from month 3
- Continue proprioceptive maintenance
- May require ankle brace initially for high-risk sports
- Full return to sport 4-6 months typically
Athletes return to competitive sport by 4-6 months in most cases.
Success rates:
- Arthroscopic debridement: 70-80% good to excellent
- Open debridement: 65-75% good to excellent
- Best outcomes: Post-traumatic, no arthritis
- Poorer outcomes: Inflammatory arthropathy, subtalar arthritis
Return to activity:
- Walking: 6-8 weeks
- Running: 3-4 months
- Full sports: 4-6 months
Contact surgeon if:
- Increasing pain after initial improvement
- Signs of infection (fever, drainage, erythema)
- No improvement by 3 months
- New instability or giving way
- Numbness or tingling (nerve injury)
- Unable to bear weight by 6 weeks
Early identification prevents complications.
Outcomes and Prognosis
Prognostic Factors
- Poor Prognosis
- Inflammatory arthropathy (RA, seronegative)
- Poor Prognosis
- Chronic symptoms (over 12 months)
- Poor Prognosis
- Subtalar arthritis on MRI
- Poor Prognosis
- No response to injection
- Poor Prognosis
- Poor compliance, inadequate rehab
- Poor Prognosis
- Older age (over 50)
Best outcomes:
- Post-traumatic sinus tarsi syndrome without arthritis
- Early treatment (within 6 months of symptom onset)
- Good compliance with proprioceptive training
- Positive response to diagnostic injection
Worst outcomes:
- Concomitant subtalar arthritis (consider arthrodesis instead)
- Inflammatory arthropathy as underlying cause
- Chronic symptoms over 12 months
- Failed multiple injection attempts
The presence of subtalar arthritis on MRI is the single strongest predictor of poor outcome with debridement alone.
Guidelines, Registries & Global Practice
Sinus tarsi syndrome (STS) is not covered by a dedicated society guideline (no AAOS, NICE, BOA, AO Foundation or EFORT clinical practice guideline addresses it specifically), and there is no joint/implant registry for it because no implant is used. Practice is therefore guided by lateral-ankle-sprain and chronic-ankle-instability evidence plus expert consensus. The evidence base is dominated by retrospective level IV series, and a recurring theme in the modern literature (Frey 1999; Willegger 2023) is that "STS" is a descriptive label for several distinct pathologies that should be named precisely whenever possible.
Global Epidemiology
- Figure
- 2.15 per 1000 person-years (peak 7.2 at 15-19 yrs)
- Source
- Waterman 2010 (PMID 20926721)
- Figure
- 49.3% (basketball, football, soccer)
- Source
- Waterman 2010
- Figure
- 22.5% in one cohort
- Source
- Xu 2024 (PMID 38664210)
- Figure
- Frequent; drives combined surgery
- Source
- Li 2017 (PMID 29189883)
Guidance & Evidence Synthesis Across Bodies
- Position relevant to STS
- No STS-specific guideline; lateral ankle sprain managed with functional rehabilitation and bracing, surgery for refractory instability
- Evidence level
- Consensus / level II for rehab
- Position relevant to STS
- No STS-specific guidance; chronic lateral ankle pain investigated with MRI and managed conservatively first, specialist foot & ankle referral if refractory
- Evidence level
- Consensus
- Position relevant to STS
- Address subtalar instability and arthroscopy within foot & ankle education; STS treated as part of the subtalar instability/impingement spectrum
- Evidence level
- Expert / level IV
- Position relevant to STS
- Recommend abandoning the umbrella term and using subtalar arthroscopy to reach a specific diagnosis
- Evidence level
- Narrative review
Practice Variation
- Conservative first: structured rehabilitation with proprioceptive training before any procedure
- Diagnostic injection: local anaesthetic into the sinus tarsi to confirm the pain source
- MRI before surgery: to characterise ligaments and exclude subtalar arthritis
- Preserve stabilising ligaments (cervical, ITCL) during debridement
- Terminology: "sinus tarsi syndrome" vs specific diagnoses (subtalar instability, impingement, ITCL tear)
- Image guidance for injection: ultrasound vs fluoroscopy vs landmark technique
- Adjuncts (PRP, prolotherapy): used in some centres, limited high-level evidence, variable funding
- Surgery: arthroscopic vs open debridement, and whether to combine with lateral ligament reconstruction
Differential Diagnosis
- Distinguishing Feature
- Recurrent giving way, lateral laxity
- Key Test
- Positive anterior drawer / talar tilt; stress views
- Discriminator vs STS
- Drawer positive (negative in isolated STS); may coexist
- Distinguishing Feature
- Older patient, stiffness, crepitus
- Key Test
- Weight-bearing X-ray / CT shows joint narrowing
- Discriminator vs STS
- Joint space loss; predicts poor debridement outcome
- Distinguishing Feature
- Pain posterior to lateral malleolus
- Key Test
- Resisted eversion pain; dynamic ultrasound
- Discriminator vs STS
- Tenderness behind, not anterior to, malleolus
- Distinguishing Feature
- Younger patient, rigid flatfoot
- Key Test
- CT / MRI (talocalcaneal or calcaneonavicular bar)
- Discriminator vs STS
- Bony/fibrous bar; restricted subtalar motion
- Distinguishing Feature
- Athlete, load-related pain
- Key Test
- MRI bone marrow oedema
- Discriminator vs STS
- Marrow oedema in bone, not just sinus fat pad
- Distinguishing Feature
- Anterolateral pain with dorsiflexion
- Key Test
- MRI / arthroscopy soft-tissue impingement
- Discriminator vs STS
- Pain at ankle joint line, not sinus tarsi opening
- Distinguishing Feature
- Back pain, dermatomal sensory change
- Key Test
- Neuro exam; lumbar MRI
- Discriminator vs STS
- Neurological signs; no focal sinus tarsi tenderness
High-risk areas for litigation:
-
Inadequate conservative trial: Document minimum 6 months comprehensive conservative treatment including physiotherapy with proprioceptive training, bracing, and injection therapy before recommending surgery.
-
Missed subtalar arthritis: Preoperative MRI must assess subtalar joint. Performing debridement in presence of arthritis leads to high failure rate. Document discussion of findings and potential need for arthrodesis.
-
Nerve injury: Superficial peroneal nerve at risk. Informed consent must include numbness risk (5-10%). Document protection of nerve during surgery.
-
Persistent pain: 20-30% have incomplete relief. Set realistic expectations preoperatively. Document that surgery is not guaranteed cure.
-
Wrong diagnosis: Exclude lateral ankle instability, peroneal pathology, subtalar arthritis, stress fracture before diagnosing sinus tarsi syndrome. Consider diagnostic injection to confirm.
Documentation requirements:
- Timeline of conservative treatment and compliance
- Injection response (diagnostic confirmation)
- MRI findings especially subtalar joint assessment
- Informed consent discussion including complications and incomplete relief risk
- Surgical findings (presence of arthritis, extent of debridement)
MCQ Practice Points
Q: What is the most important ligament within the sinus tarsi for subtalar joint stability?
A: The interosseous talocalcaneal ligament (ITCL) is the primary stabilizer of the subtalar joint. It is located in the medial aspect of the sinus tarsi (tarsal canal) and has two bands. The cervical ligament is located more laterally in the sinus tarsi and is a secondary stabilizer. During surgical debridement, both ligaments must be preserved to maintain subtalar stability. Excessive excision of these ligaments can lead to iatrogenic subtalar instability.
Q: What is the pathognomonic physical examination finding for sinus tarsi syndrome?
A: Exquisite point tenderness over the sinus tarsi (located anterior and inferior to the lateral malleolus) is the most reliable clinical sign. This is present in over 90% of cases. The sinus tarsi is palpable approximately 1-2 cm anterior to the lateral malleolus. Other findings include pain with forced inversion and eversion, and subjective instability, but sinus tarsi point tenderness is the hallmark finding that differentiates it from other causes of lateral ankle pain.
Q: A patient with suspected sinus tarsi syndrome undergoes MRI. What is the characteristic finding?
A: High T2 signal intensity within the sinus tarsi (fat pad edema and inflammation) is seen in 80-90% of cases. Additional findings may include disruption or signal changes in the cervical ligament, interosseous talocalcaneal ligament abnormalities, synovitis, and subtalar joint effusion. Plain radiographs are usually normal. The most important MRI assessment is to exclude subtalar arthritis, which is a poor prognostic indicator for surgical debridement and may require arthrodesis instead.
Q: What is the most important component of conservative treatment for sinus tarsi syndrome?
A: Proprioceptive training with balance exercises and single-leg stance work is the most critical component. The sinus tarsi contains dense mechanoreceptors that provide proprioceptive feedback for hindfoot position. Injury disrupts this proprioceptive function, leading to the sensation of instability. Rehabilitation must include balance board exercises, single-leg stance on unstable surfaces, and sport-specific proprioceptive drills. This is combined with activity modification, NSAIDs, ankle bracing, and orthotics. Approximately 70-80% of patients respond to conservative treatment over 3-6 months.
Q: During arthroscopic sinus tarsi debridement, what is the most important technical point?
A: Preserve the cervical ligament and interosseous talocalcaneal ligament while debriding synovium and scar tissue. The goal of surgery is to remove inflamed synovium, scar tissue, and adhesions that are causing pain and impingement. However, the ligaments provide essential subtalar joint stability and must be preserved. Complete excision of these ligaments can lead to iatrogenic subtalar instability. The surgical principle is debridement of pathologic soft tissue while maintaining ligamentous integrity.
Q: Which MRI finding predicts the poorest outcome with arthroscopic sinus tarsi debridement?
A: Subtalar arthritis (joint space narrowing, cartilage loss, subchondral changes) is the strongest predictor of poor outcome. Debridement alone in the presence of subtalar arthritis has only a 40-60% success rate compared to 70-80% without arthritis. If significant arthritis is present, the patient should be counseled that subtalar arthrodesis may be necessary for definitive pain relief. Preoperative MRI assessment of the subtalar joint is essential to identify arthritis and set realistic expectations.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old recreational soccer player presents with 4 months of lateral ankle pain following an inversion injury. He describes vague pain anterior to the lateral malleolus, worse on uneven ground. He feels his ankle gives way occasionally. On examination, you find exquisite point tenderness over the sinus tarsi. Anterior drawer is negative. How do you diagnose and initially manage this patient?”
“The same patient returns after 5 months of comprehensive conservative treatment including physiotherapy with proprioceptive training, bracing, and orthotics. He remains significantly symptomatic with persistent sinus tarsi pain limiting his soccer. MRI shows high T2 signal in sinus tarsi with cervical ligament disruption but no subtalar arthritis. What are your next steps?”
“You are planning arthroscopic sinus tarsi debridement for a patient who has failed 8 months of conservative treatment and two corticosteroid injections. Walk me through your surgical technique. What would you do if you encounter significant subtalar arthritis during the arthroscopy? What are the potential complications?”
Key Anatomy
- Sinus tarsi: Cone-shaped tunnel between talus (superior) and calcaneus (inferior)
- Location: Opens laterally anterior to lateral malleolus, palpable 1-2 cm anterior to tip
- Contents: Interosseous talocalcaneal ligament (ITCL - main stabilizer), cervical ligament, fat pad, mechanoreceptors
- Function: Subtalar stability, proprioception for hindfoot position
Clinical Features
- Triad: Lateral hindfoot pain, sinus tarsi point tenderness, instability sensation
- History: 90% follow ankle inversion injury, pain worse on uneven ground
- Examination: Exquisite sinus tarsi tenderness (pathognomonic), pain with forced inversion/eversion
- Negative anterior drawer unless coexisting lateral ankle instability (30-40%)
Investigations
- Clinical diagnosis: Based on history and examination
- X-rays: Usually normal, exclude fracture and arthritis
- MRI: High T2 signal in sinus tarsi (80-90% sensitivity), assess subtalar joint for arthritis
- Diagnostic injection: 2 mL lidocaine, immediate relief confirms diagnosis (over 90% specificity)
Conservative Management
- First-line: 70-80% respond to conservative treatment over 3-6 months
- Proprioceptive training: Most important component - balance exercises, single-leg stance
- Activity modification: Avoid uneven surfaces, lateral ankle brace
- Injection: Corticosteroid if failed 3 months conservative, 60-70% temporary relief
- Limit 2 corticosteroid injections maximum
Surgical Technique
- Indication: Over 6 months failed conservative including injection therapy
- Arthroscopic debridement: Lateral decubitus, anterolateral and sinus tarsi portals
- Key technical point: Debride synovium and scar, PRESERVE cervical and ITCL ligaments
- Assess subtalar joint: If arthritis present, may require arthrodesis instead
- Success: 70-80% good to excellent results without arthritis, 40-60% if arthritis present
Complications and Outcomes
- Persistent pain: 20-30% most common, often due to unrecognized arthritis
- Nerve injury: 5-10% superficial peroneal nerve, numbness dorsum of foot
- Recurrence: 10-20%, incomplete debridement or untreated instability
- Best prognosis: Post-traumatic, no arthritis, good injection response
- Worst prognosis: Subtalar arthritis (consider arthrodesis), inflammatory arthropathy
Evidence Base and Key Studies
Tarsal Sinus: MR Imaging and Pathologic Findings
- Combined cadaveric (10 specimens) and retrospective clinical study (37 patients with a clinical diagnosis of sinus tarsi syndrome)
- MR imaging and MR arthrography assessed the cervical ligament (CL) and interosseous talocalcaneal ligament (ITCL)
- In 18 patients the diagnosis was confirmed on MR: combined ITCL and CL tears in 11, isolated CL tears in 3, ganglia in 3, and pigmented villonodular synovitis in 1
- Reconstructed MR arthrograms aligned to the ligament axes improved evaluation of individual tarsal sinus structures
Arthroscopic Evaluation of the Subtalar Joint: Does Sinus Tarsi Syndrome Exist?
- Retrospective review of 49 subtalar arthroscopies (1989-1996); 94% good/excellent results overall for subtalar pathology
- Of 14 feet with a preoperative diagnosis of 'sinus tarsi syndrome', ALL diagnoses were changed at arthroscopy
- Revised diagnoses: 10 interosseous ligament tears, 2 arthrofibrosis, 2 degenerative joints
- Authors concluded 'sinus tarsi syndrome' is an inaccurate, non-specific term that should be replaced with a precise arthroscopic diagnosis
- Commonest complication was transient superficial peroneal nerve neuropraxia (low overall complication rate)
Arthroscopic Debridement with Ankle Stabilisation for STS in Chronic Ankle Instability
- Retrospective series of 57 patients with STS and chronic ankle instability; 40 followed (mean 30.7 months)
- All underwent thorough tarsal sinus debridement; 54 had lateral ligament repair and 3 reconstruction
- Modified AOFAS improved from median 62.5 to 93, Karlsson from 57 to 90, Tegner from 1 to 5
- Addressing coexisting lateral instability at the same setting gave satisfactory functional outcomes
Sinus Tarsi Corticosteroid Injection after Lateral Ankle Sprain
- Retrospective cohort: 391 lateral ankle sprains screened, 88 with STS treated by sinus tarsi corticosteroid injection (betamethasone + lidocaine)
- Incidence of STS after lateral ankle sprain was 22.5%
- VAS and AOFAS improved significantly at 1 month (VAS 1.2, AOFAS 88.7) versus baseline
- Benefit waned over time with a ~65% symptom recurrence rate within 12 months (AOFAS 79.1 at 1 year)
- Authors suggest ankle arthroscopy when conservative measures fail to give durable benefit
The Evolution of Sinus Tarsi Syndrome - What Is the Underlying Pathology? A Critical Review
- Critical narrative review of the pathoanatomy, biomechanics and aetiology of sinus tarsi pain
- Concludes STS is largely a 'catch-all' descriptor for several distinct pathologies (impingement, subtalar instability, ligament/ganglion lesions and others)
- Proposes a structured algorithm for clinical, radiological and arthroscopic evaluation
- Recommends replacing the umbrella term with the specific underlying diagnosis whenever possible
The Epidemiology of Ankle Sprains in the United States
- Prospective national surveillance (NEISS) of an estimated 3.14 million ED-presenting ankle sprains, 2002-2006
- Overall incidence 2.15 per 1000 person-years; peak 7.2 per 1000 at age 15-19 years
- Nearly half (49.3%) of sprains occurred during sport, most often basketball (41%), football (9%) and soccer (8%)
- Sex differences are age-dependent: higher in young males, higher in women over 30