Pediatric Spine | Pars Defect | Stress Fracture | Extension Pain
- Definition: A defect (stress fracture) in the pars interarticularis.
- Mechanism: Repetitive hyperextension (Gymnasts, Fast Bowlers, Linebackers).
- Presentation: Extension-based low back pain. Tight hamstrings.
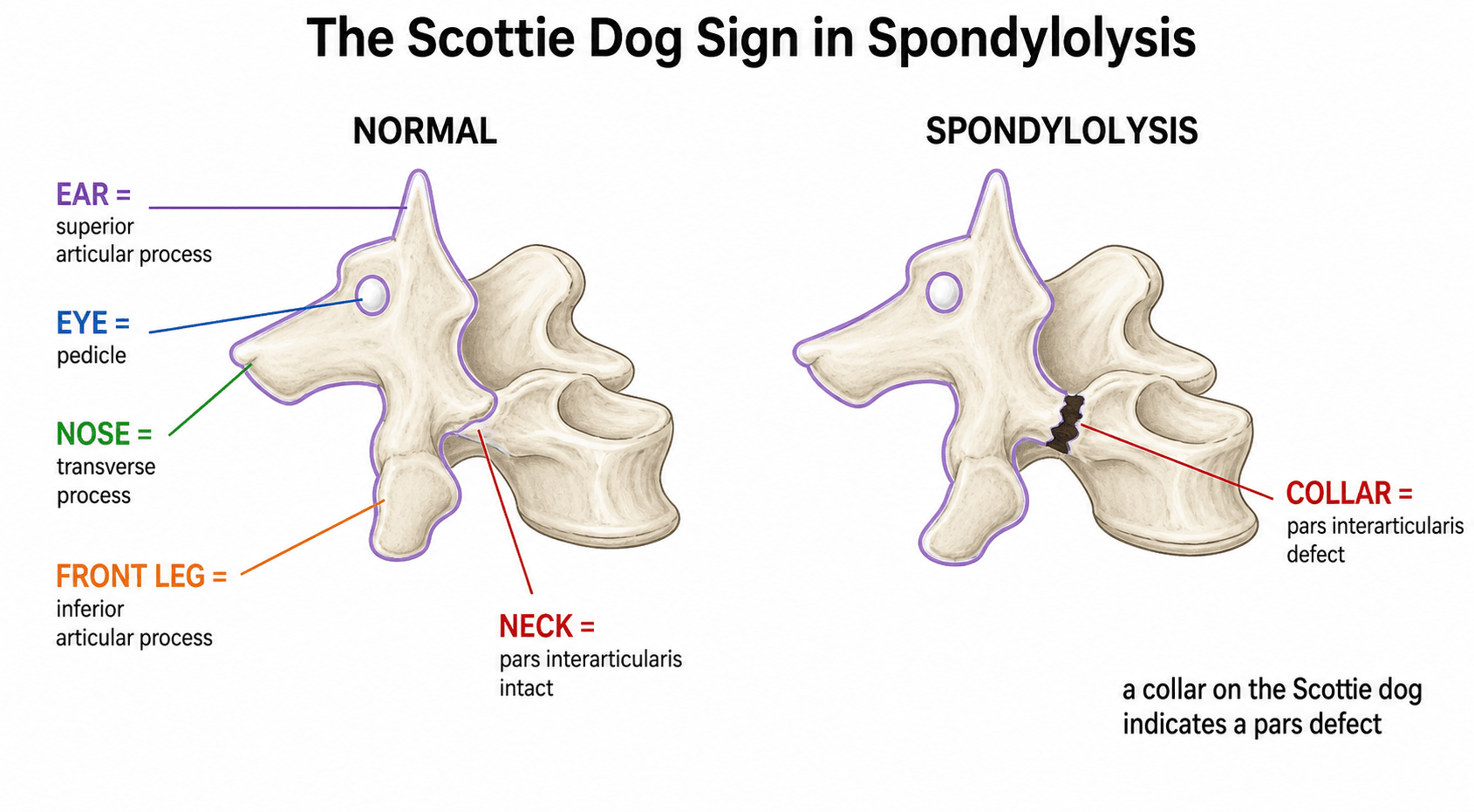
- Scottie Dog: Visible on Oblique X-rays (Collared dog = fracture).
- Imaging: MRI is now gold standard (STIR edema = acute). SPECT is sensitive but high radiation.
- “The 'Scottie Dog' sign is classic but oblique views are high radiation and often skipped for MRI.
- “Hamstring tightness is a cardinal sign (Phalen-Dickson sign is for Spondylolisthesis, but tightness present in lysis too).
- “Unilateral lysis often results in sclerosis of the CONTRALATERAL pedicle (Wilkinson syndrome).
- “Direct Repair (Buck's) is preferred over Fusion for isolated L5 lysis.
High Dose. A SPECT/CT carries significant radiation (equivalent to ~500 CXRs). Use MRI (STIR sequence) as first line for diagnosis in children to spare gonads.
Avoid Routinely. Oblique lumbar views increase radiation dose significantly and have low sensitivity compared to MRI/SPECT.
- Pros
- Cheap, fast, shows grade of slip
- Cons
- Low sensitivity for lysis
- Role
- Screening
- Pros
- No radiation, shows acute edema
- Cons
- Can miss chronic non-union
- Role
- Gold Standard Diagnosis
- Pros
- Best for bony detail (healing)
- Cons
- Radiation
- Role
- Assessment of healing
- Pros
- Highest sensitivity for turnover
- Cons
- High radiation
- Role
- Problem solving only
SPORTRisk Factors
Hook:SPORTs that extend the spine break the pars.
SPECTImaging Strategy
Hook:SPECT is sensitive but Radiation is high. MRI First!
Overview and Epidemiology
Pediatric Spondylolysis is a stress fracture of the pars interarticularis (isthmus). It represents a fatigue failure of the bone from repetitive extension and rotation.
Key Associations:
- Inuit Population: Extremely high prevalence (~50%).
- Spina Bifida Occulta: Associated with S1 occulta.
- Scheuermann's: Increased incidence of lysis.
Definitions
Depending on the pathology, the terminology changes:
- Spondylolysis: A defect in the pars interarticularis. No slip.
- Spondylolisthesis: Translation of one vertebra on another.
- Isthmic Spondylolisthesis: A slip CAUSED by a lysis (pars defect). The L5 body slips forward, leaving the posterior elements behind.
- Dysplastic Spondylolisthesis: A slip caused by congenital facet insufficiency. The pars is often intact.
- Spondyloptosis: Complete (greater than 100%) dislocation of L5 in front of the sacrum.
In children, we are mostly dealing with Isthmic or Dysplastic types. Degenerative slips are for adults.
Pathophysiology and Mechanisms
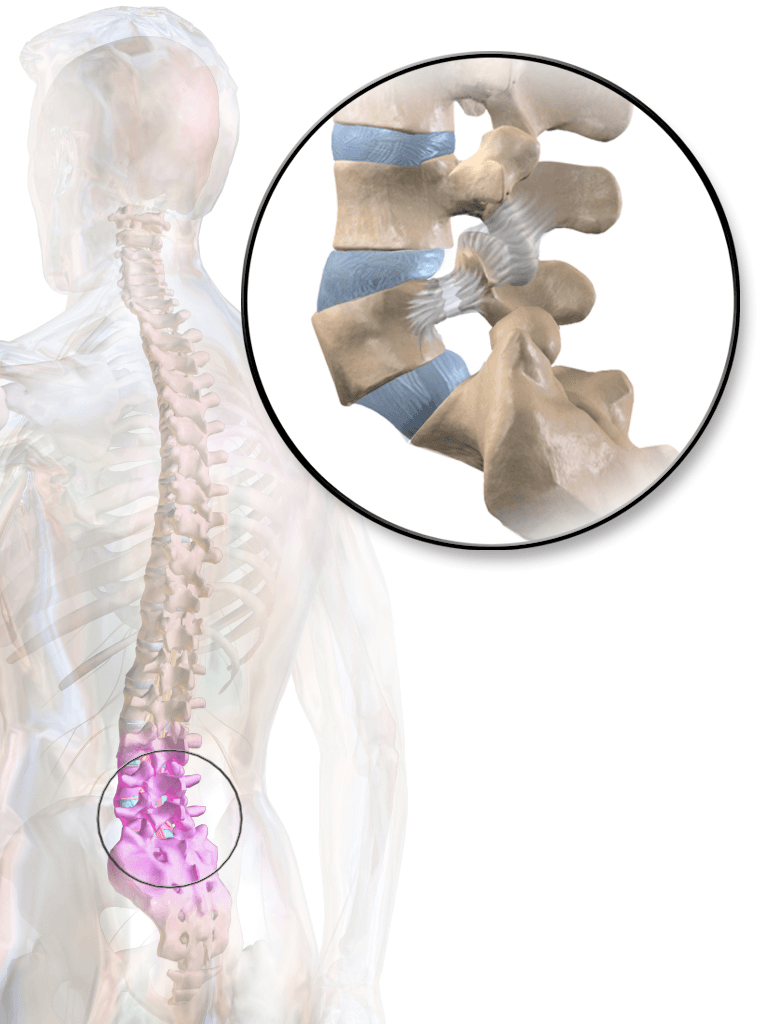
The Pars Interarticularis:
- The bridge of bone between the superior and inferior articular facets.
- It is the "weak link" in the neural arch.
- Biomechanics: In extension, the inferior facet of the cephalad vertebra impacts the pars of the caudal vertebra (Nutcracker mechanism).
- L5 Vulnerability: The L5 pars is susceptible due to the high shear forces at the lumbosacral junction and the transition from mobile spine to fixed pelvis.
Spino-Pelvic Parameters
The geometry of the pelvis plays a crucial role in the etiology and progression of lysis/listhesis.
-
Pelvic Incidence (PI):
- An anatomical constant (Morphology).
- Angle between the line perpendicular to the sacral plate and the line connecting the sacral midpoint to the femoral head axis.
- High PI (greater than 60 deg): Predisposes to Spondylolisthesis. The sacrum is more vertical, creating higher shear forces at L5-S1.
- Low PI: Protective against slip, but may cause impingement.
-
Sacral Slope (SS):
- The angle of the sacral plate to the horizontal.
- High PI usually results in High SS (greater than 50 deg).
- A steep sacral slope increases the anterior shear component of gravity (The "Ski Slope" effect).
-
Pelvic Tilt (PT):
- A compensatory mechanism.
- As the body tries to maintain balance with a high slip, the pelvis retroverts (High PT).
- This leads to the characteristic "crouched gait" and flattened lumbar lordosis above the slip.
Understanding PI is essential for surgical planning, especially if fusion is considered.
Classification
Wiltse Classification of Spondylolysis/Listhesis
-
Dysplastic (Type I):
- Congenital deficiency of the S1 dome or L5 arch.
- The facets are often oriented axially/sagittally, allowing slip.
- Highly associated with Spina Bifida Occulta.
- High risk of progression to high-grade slip.
-
Isthmic (Type II):
- The classic stress fracture lesion in the pars.
- IIA: Lytic stress fracture. The bone fails under tension/shear. This is the common form in athletes.
- IIB: Elongated pars. The bone "heals" with fibrous tissue that lengthens over time, allowing the body to slip forward. The pars is intact but attenuated.
- IIC: Acute fracture. A traumatic event triggers the break (Rare).
-
Degenerative (Type III):
- Adult instability.
- L4/5 is most common level (vs L5/S1 for isthmic).
- Due to facet joint and disc degeneration.
- Rare in pediatric population.
-
Traumatic (Type IV):
- High energy fracture (MVA, Fall).
- Often associated with other spinal fractures.
-
Pathologic (Type V):
- Tumor (Osteoid Osteoma? Metastasis?).
- Infection (Osteomyelitis).
-
Iatrogenic (Type VI):
- Post-surgical destabilization.
- Removal of too much pars/facet during laminectomy.
Wiltse classification is the standard.
Clinical Assessment
Clinical Features
- Pain: Low back pain, worse with extension (Stork test).
- Radiation: Usually localized to belt-line, occasionally to buttocks/thighs.
- Radiculopathy: Rare in lysis (unless high grade slip).
- Hyperlordosis: Posture.
- Palpation: Step-off (if slip present). Tenderness at L5/S1.
- Hamstrings: TIGHTness is universal. Popliteal angle measurement.
- Stork Test: One-legged hyperextension test. Pain implies lysis on the standing side.
Red Flag Symptoms:
- Saddle anesthesia (perineal numbness).
- Bladder retention or incontinence (overflow).
- Bowel incontinence.
- Bilateral significant lower limb weakness.
Mechanism:
- In high grade slips (Dysplastic), the lumbosacral kyphosis creates a "pincer" effect on the cauda equina between the L5 body and S1 posterior elements.
- Action: Immediate MRI and Surgical Decompression.
The High-Grade Slip Phenotype and the Phalen-Dickson Sign
While isolated lysis often looks normal on inspection, a high-grade isthmic or dysplastic slip produces a characteristic, examinable phenotype that the pearls above allude to.
- Phalen-Dickson sign: a crouched, flexed-hip and flexed-knee gait, with the knees held flexed through stance and gait. It results from hamstring tightness/spasm and the lumbosacral kyphosis of a high-grade slip, and signals significant listhesis (not isolated lysis).
- Hamstring spasm/tightness is near-universal and limits the popliteal angle; it is protective splinting rather than true neural tension.
- Heart-shaped ("flat") buttocks and a palpable step-off at the lumbosacral junction: as L5 translates forward the posterior sacral prominence becomes visible and the L5 spinous process is felt as a step.
- Trunk shortening with a low rib-to-pelvis distance and a transverse abdominal crease, plus a compensatory hyperlordosis above the slip and pelvic retroversion (high pelvic tilt) to keep the trunk balanced.
- Gait may be frankly waddling in severe slips.
The Phalen-Dickson sign is the crouched, knee-flexed gait of a high-grade slip (driven by hamstring spasm and lumbosacral kyphosis). Together with heart-shaped buttocks, a palpable step-off and trunk shortening, it marks spondylolisthesis, not isolated spondylolysis — and should prompt assessment of slip grade and spinopelvic balance.
Investigations
- Finding
- Scottie Dog with collar
- Indication
- Historical standard. Often low yield.
- Finding
- High signal in Pars (Edema)
- Indication
- First line for active pain. Detects stress reaction before fracture.
- Finding
- Increased uptake (Hot spot)
- Indication
- Problem solving if MRI normal but suspicion high.
- Finding
- Fracture line (Sharp/Sclerotic)
- Indication
- To assess HEALING. Rounded sclerotic margins = non-union.


PARSDiagnosis
Hook:PARS defect causes the pain.
Differential Diagnosis
Adolescent low back pain has a different differential to the adult. Mechanical/discogenic pain is far less common; an organic cause is found more often, so red flags must be actively excluded.
- Distinguishing Features
- Extension pain, single-leg stork test positive, tight hamstrings, athlete
- Key Investigation
- MRI STIR (pars/pedicle oedema); CT for healing
- Distinguishing Features
- Night pain, dramatically relieved by NSAIDs, painful scoliosis
- Key Investigation
- CT shows nidus with sclerotic rim; do not confuse with reactive pedicle sclerosis
- Distinguishing Features
- Younger child, refusal to walk, fever, raised CRP/ESR
- Key Investigation
- MRI with contrast; blood cultures
- Distinguishing Features
- Rigid thoracic/thoracolumbar kyphosis, anterior wedging
- Key Investigation
- Lateral radiograph (over 5 degrees wedging at 3 adjacent levels)
- Distinguishing Features
- Flexion-pattern pain, positive straight-leg raise, true radiculopathy
- Key Investigation
- MRI lumbar spine
- Distinguishing Features
- Adolescent, acute axial load, radicular pain mimicking disc
- Key Investigation
- CT shows bony fragment off the vertebral rim
- Distinguishing Features
- Constant non-mechanical pain, weight loss, neurology, night pain
- Key Investigation
- MRI whole spine; bloods; refer urgently
Management Algorithm

The Mainstay of Treatment
Success Rate: greater than 90%.
- Rest: Cessation of sport (the "offending agent") for 3-6 months.
- Analgesia: NSAIDs.
- Bracing:
- Boston Overlap Brace (Antilordotic).
- Role: Symptom control and immobilization?
- Protocol: Full time for 3-6 months vs Symptomatic wear.
- Controversy: Does bracing actually heal the defect or just stop pain?
- Physical Therapy:
- Hamstring stretching (Crucial).
- Core strengthening (Abdominals).
- Pelvic tilt exercises.
- Williams Flexion Exercises:
- Pelvic Tilt.
- Single Knee to Chest.
- Double Knee to Chest.
- Partial Sit-ups.
- Hamstring stretch.
- Hip Flexor stretch.
- Squat.
- Avoid hyperextension exercises (McKenzie) initially. Use flexion bias to open the neural foramen and unload the pars.
Return to sport: When pain-free and full ROM.
Fibrous union is an acceptable outcome.
Surgical Technique
Pars Repair (Buck's / Scott's)
Idea: Reconnect the broken bone without fusing the joint. Preserves motion. Indication: L1-L4 lysis (L5 is hard due to depth), No slip (Grade 0), Healthy disc (MRI).
Techniques:
- Buck's Repair: Screw directly across the defect (Lag screw).
- Scott's Wiring: Wire around transverse process to spinous process.
- Pedicle Screw-Hook: Screw in pedicle, rod/hook on lamina. Compression.
Buck's Technique
- Midline incision. Expose lamina/pars.
- Debride the fibrous tissue in the defect (pseudarthrosis).
- Drill to bleeding bone.
- Bone graft (local/iliac) into defect.
- Graft Choice:
- Iliac Crest Bone Graft (ICBG) is Gold Standard.
- Local bone from lamina is often insufficient.
- BMP is generally Contraindicated in direct repair (risk of stenosis/overgrowth in canal).
- Insert screw from inferior lamina, across the pars, into the pedicle/body.
- Compress the defect.
High-Grade Slip Surgery: Reduction, In-Situ Fusion and the Gaines Procedure
For high-grade slips the central, examinable surgical debate is whether to reduce the slip or fuse it in situ, and the dominant hazard is to the L5 nerve root.
- In-situ posterolateral fusion (often L4-S1) is the traditional, lower-neurological-risk option; it accepts the deformity but reliably arrests progression and relieves pain in most patients.
- Reduction with instrumented fusion improves the sagittal profile by correcting the lumbosacral kyphosis and restoring balance, but carries a substantially higher risk of L5 nerve-root injury.
- The key safety principle: L5 root injury occurs predominantly during the final part of the reduction, when correcting the slip and kyphosis stretches the L5 root over the sacral dome. Many surgeons therefore perform a deliberate partial reduction, prioritise correcting the slip angle (lumbosacral kyphosis) over the translation, and use intra-operative neuromonitoring.
- For spondyloptosis (Meyerding grade V), where L5 has translated completely in front of the sacrum, one described salvage is the Gaines procedure: a staged L5 vertebrectomy (anterior excision of the L5 body, then posterior removal of the L5 posterior elements) with reduction of L4 directly onto S1.
- It is technically demanding with a high neurological-complication rate and is reserved for severe, fixed deformity.
In high-grade slip surgery, L5 nerve-root injury is the major risk of reduction and is worst during the final phase (the root is stretched over the sacral dome). Favour correcting the slip angle / lumbosacral kyphosis over full translational reduction, use neuromonitoring, and reserve the Gaines L5 vertebrectomy for spondyloptosis. In-situ fusion remains the safe default.
Complications
- Specifics
- Failure of defects to heal
- Prevention
- Adequate debridement, compression, bone graft.
- Specifics
- Screw breakage/pullout
- Prevention
- Don't oversize screws. Avoid excessive torque.
- Specifics
- L5 root at risk
- Prevention
- Careful dissection.
Postoperative Care and Rehabilitation
Recovery Pathway
- Goal: Allow bone/fibrous healing. Symptom control.
- Brace: TLSO with thigh extension (Antilordotic). Worn 23hrs/day? (Controversial).
- Activity: Walking allowed. No sports. No PE.
- Restrictions: No BLT (Bending, Lifting, Twisting).
- Goal: Restore core strength and flexibility.
- Wean Brace: Over 2 weeks.
- PT:
- Hamstring stretching (Gentle).
- Transversus abdominis activation.
- Dead bugs / Bird-dog exercises (Neutral spine).
- Imaging: CT scan at 12 weeks to assess union? (Only if contemplating return to contact sport or if pain persists).
- Goal: Sport specific reconditioning.
- Progression:
- Jogging to Running to Sprinting.
- Sport specific drills (Non-contact).
- E.g. Cricket: Batting to Bowling (reduced run-up).
- Return to Contact:
- Pain free.
- Full ROM.
- Normal strength.
- Radiographic Union? (Debated. Asymptomatic non-union allows play in many leagues, but risk of refracture/progression exists).
Outcomes
Prognosis:
- Excellent for most adolescents.
- Cessation of sport is the hardest part.
- Unilateral defects have virtually 100% healing rate.
- Bilateral defects have lower healing rates but high asymptomatic rates.
Guidelines, Registries & Global Practice
Global epidemiology
- Overall prevalence of the pars defect is approximately 6% of the adult population (Fredrickson), with a strong hereditary component and a marked association with spina bifida occulta.
- Highest prevalence is reported in some Inuit/circumpolar populations (historically up to ~40-50%), suggesting a genetic predisposition layered on activity.
- It is the single most common identifiable cause of low back pain in the young athlete worldwide; hyperextension/rotation sports (gymnastics, diving, cricket fast bowling, pole vault, dance, throwing, American football line play) carry the greatest risk.
Side-by-side guidance
- Emphasis
- Treat persistent adolescent back pain as organic until excluded; MRI without ionising radiation favoured first line in children
- Emphasis
- Activity modification and physiotherapy are first-line; bracing optional; surgery reserved for failed prolonged conservative care
- Emphasis
- Low back pain over 2-3 weeks in an adolescent athlete is spondylolysis until proven otherwise; load management and technique correction central to prevention and rehabilitation
- Emphasis
- Spinopelvic parameters (pelvic incidence) guide decisions in higher-grade slips; in-situ vs reduction remains case-dependent
Registry and surveillance notes
- There is no dedicated spondylolysis implant registry; outcomes derive from sport-injury surveillance cohorts (e.g. junior cricket fast-bowler programmes) and observational meta-analyses rather than arthroplasty-style registries.
- Sport-governing-body workload surveillance (limits on bowling/throwing frequency, mandatory rest, screening of skeletally immature athletes) is the main population-level prevention lever and is broadly convergent across cricketing nations.
High- vs limited-resource practice variation
- Well-resourced settings: MRI STIR as first-line, low-dose/limited CT for healing assessment, and access to motion-preserving repair where indicated.
- Limited-resource settings: diagnosis often rests on plain radiographs and clinical findings (extension pain, tight hamstrings, stork test); management is overwhelmingly activity modification and physiotherapy, which is appropriate given the benign natural history and the high rate of good clinical outcomes without union.
- Persistent athletic back pain beyond 2-3 weeks warrants imaging and specialist input in any setting; early recognition reduces progression to a terminal non-union.
Areas of Uncertainty and Controversy
Klein's meta-analysis found bracing did NOT change clinical outcome versus activity restriction alone. Many centres now reserve a brace for symptom control in the child who cannot otherwise rest, rather than as a healing device.
MRI is preferred to spare radiation, but it can miss the earliest stress reaction that SPECT/CT detects (Masci). Practice varies: some use limited low-dose CT after a positive SPECT for problem-solving and to grade healing.
A stable fibrous (terminal) defect is an accepted endpoint. Most patients become asymptomatic without union, so return-to-sport decisions are increasingly driven by symptoms and function rather than CT healing.
For isolated L5 lysis with a healthy disc, motion-preserving repair is attractive but technically demanding; many surgeons still choose L5-S1 fusion for reliability. There is no high-level randomised evidence to settle this.
MCQ Practice Points
Q: Which level is most commonly affected in pediatric spondylolysis? A: L5 (90% of cases).
Q: What structure corresponds to the 'neck' of the Scottie Dog? A: The Pars Interarticularis. (Eye = Pedicle, Nose = Transverse Process, Ear = Superior Facet, Leg = Inferior Facet).
Q: Why is SPECT/CT falling out of favor? A: High radiation dose. MRI STIR sequences can detect early stress reactions without radiation.
Q: What position does the Boston brace for spondylolysis hold the spine in? A: Antilordotic (Flexion). This unloads the posterior elements (pars).
Q: What congenital anomaly is associated with spondylolysis? A: Spina Bifida Occulta (at S1).
Q: Unilateral pedicle sclerosis with contralateral lysis is called: A: Wilkinson Syndrome. (Often misdiagnosed as Osteoid Osteoma).
Q: Which pelvic parameter is a constant risk factor for slip progression? A: Pelvic Incidence (PI). High PI (greater than 60 deg) correlates with isthmic spondylolisthesis.
Q: Which modality is best to distinguish a visible fracture line as acute vs chronic/non-union? A: CT Scan. Rounded sclerotic margins indicate chronic non-union. Sharp irregular margins indicate acute fracture.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 14-year-old male gymnast presents with low back pain worsening with back handsprings. He has tight hamstrings.”
“X-rays show a unilateral L5 lysis. MRI shows sclerosis of the contralateral pedicle.”
“A 16-year-old cricket fast bowler has persistent pain after 9 months of rest and bracing. CT shows a bilateral L5 lysis with sclerotic margins and no slip.”
Diagnostic Triad
- Extension Pain (Stork Test)
- Tight Hamstrings
- Pars Edema (MRI STIR)
Wiltse Classification
- I: Dysplastic
- II: Isthmic (Lytic)
- III: Degenerative
- IV: Traumatic
- V: Pathologic
Management Rules
- Acute: Rest + Brace (3-6m)
- Chronic: Rehab to Surgery
- Surgery: Repair if L1-L4, Fusion if L5?
- Return to sport: Pain free (Union not mandatory)
- Wilkinson Syndrome: Do NOT Biopsy
Evidence Base
Each card has been checked against the primary PubMed record. Note the Masci finding in particular: it is frequently mis-quoted. The original data actually favour scintigraphy/SPECT plus limited CT over MRI for detecting the earliest bone stress, even though MRI is preferred clinically to spare radiation. Know the difference between "best test" and "best first test".
MRI vs Bone Scintigraphy (SPECT) for Active Lysis
- Prospective cohort of 71 young athletes with low back pain; 55% had active lysis on bone scintigraphy with SPECT
- MRI detected bone stress in only 40 of 50 pars shown active on SPECT (LOWER sensitivity for early stress, p=0.001)
- MRI matched CT for visualising established fractures (18 of 19, p=0.345)
- The one-legged hyperextension (stork) test was neither sensitive nor specific
Natural History of Lysis and Listhesis
- Prospective radiographic study of 500 unselected first-grade children followed into adulthood
- Incidence of spondylolysis 4.4% at age 6, rising to 6% in adulthood
- Slip progression was unusual and was rare after adolescence
- Strong association with spina bifida occulta; no slip became symptomatic in the studied cohort
Nonoperative Treatment Meta-Analysis
- Meta-analysis of 15 observational studies (665 patients) for clinical outcome and 10 studies (847) for radiographic union
- Pooled clinical success 83.9%; bracing did NOT change clinical outcome versus no brace (p=0.75)
- Overall bony union only 28%, yet good clinical outcomes occurred without union
- Unilateral defects healed 71% vs bilateral 18.1% (p<0.0001); acute defects healed 68% while terminal defects healed in NONE
Direct Pars Repair (Original Description)
- Original description of direct screw repair of the pars defect
- Lag screw placed across the defect with bone grafting after debridement of fibrous tissue
- Restores the neural arch and preserves the motion segment, avoiding fusion in young patients
MRI Marrow Oedema Precedes Symptomatic Injury (Fast Bowlers)
- 65 junior elite cricket fast bowlers prospectively scanned through one 8-month season
- 15 (23%) developed a lumbar bone stress injury; ALL 15 had preceding bone marrow oedema on MRI
- Marrow oedema 2 weeks before a high-load tournament carried a very high risk of progression (RR 18.9)
- Higher proportion of bowling days and shorter in-season breaks predicted injury more than ball counts
Progression of Slip in Children (Long-Term)
- 272 children and adolescents followed radiographically for a mean of 14.8 years
- About 90% of the eventual slip was already present at first presentation
- The percentage of primary slip was the only radiographic variable predicting progression
- In-situ posterior/posterolateral fusion had no statistically significant effect on slip progression
Spondylolysis Risk in a High-Risk Sport (Pole Vault)
- Prospective cohort of 135 collegiate pole vaulters over one season
- Low back was the single most common injury site (16.7%); 83% of back injuries occurred at the plant/takeoff (forced hyperextension)
- One-third of lumbar injuries were spondylolysis, and 75% of those were season-ending
- Prior injury raised the odds of new injury 2.7-fold