Congenital Muscular Torticollis | Head Tilt | Sternocleidomastoid | Stretching vs Surgery
- Classic triad: Head tilt to AFFECTED side, chin rotation to OPPOSITE side, palpable SCM mass (pseudotumor)
- Screen for DDH: real association is most likely under 10% (older reports quoted up to 20%) - always perform a clinical hip examination
- Early stretching is key: Greater than 90% resolve with physiotherapy started before 1 year
- Plagiocephaly: Positional head flattening from persistent tilt - contributes to cosmetic concerns
- Surgical release: Consider if no improvement by 12-18 months, releases SCM at clavicular origin
- “Tilt is toward the TIGHT SCM (affected side), chin points AWAY
- “Pseudotumor (SCM mass) present in first weeks, usually resolves by 4-6 months
- “Facial asymmetry and plagiocephaly develop if untreated
- “Differential: congenital cervical spine anomaly, ocular torticollis, Sandifer syndrome
Head tilts TOWARD tight SCM, chin rotates AWAY. If right SCM is tight: head tilts RIGHT, chin points LEFT. Palpable "pseudotumor" (fibromatosis colli) in the SCM in early infancy, usually gone by 4-6 months. Passive rotation limited to opposite side.
Examine the hips in EVERY torticollis patient. Older reports quoted a 20% DDH association, but verified series put it nearer 8% (Walsh) and around 4.5% requiring treatment (Minihane), with a literature range of 2-29%. A normal clinical hip examination makes significant DDH unlikely; image selectively on abnormal exam or risk factors. Also check for plagiocephaly (flattening of ipsilateral occiput), facial asymmetry, and cervical spine anomalies. If atypical features, consider C-spine X-ray or MRI.
Passive stretching is first-line treatment. Stretch SCM by tilting head OPPOSITE to tight side and rotating chin TOWARD tight side. Do during every diaper change. Also positioning: encourage looking toward affected side. Greater than 90% success if started early properly.
Consider surgery if: No improvement by 12-18 months, significant residual rotation deficit (greater than 15-20 degrees), significant residual tilt, cosmetic/functional concerns. Open or endoscopic SCM release at clavicular origin. Post-op stretching and bracing crucial.
- Congenital Muscular Torticollis
- Birth or shortly after
- Cervical Spine Anomaly
- Birth
- Ocular Torticollis
- Often noted later, intermittent
- Congenital Muscular Torticollis
- Present early (pseudotumor)
- Cervical Spine Anomaly
- Absent
- Ocular Torticollis
- Absent
- Congenital Muscular Torticollis
- Limited passive rotation away from tilt
- Cervical Spine Anomaly
- Variable, may be fixed
- Ocular Torticollis
- Full passive ROM
- Congenital Muscular Torticollis
- Normal
- Cervical Spine Anomaly
- Abnormal (Klippel-Feil, hemivertebra)
- Ocular Torticollis
- Normal
- Congenital Muscular Torticollis
- Stretching, surgery if fails
- Cervical Spine Anomaly
- Depends on anomaly
- Ocular Torticollis
- Ophthalmology referral
TILTTILT - Torticollis Features
Hook:The head TILTs toward the tight SCM - same side as the problem.
DDHDDH - Screen in Torticollis
Hook:Examine the hips in every CMT patient - the association is real even if smaller than the classic 20% quote.
Overview and Epidemiology
Congenital Muscular Torticollis (CMT) is the most common cause of torticollis in infants and young children. It is characterized by unilateral shortening or fibrosis of the sternocleidomastoid muscle (SCM), leading to a head tilt toward the affected side with chin rotation to the opposite side.
Epidemiology:
- Incidence 0.4-2% of live births
- Third most common congenital musculoskeletal condition (after DDH and clubfoot)
- Right side more commonly affected (75%)
- Male slightly more often than female
- Associated with difficult delivery, breech presentation, first-born
CMT accounts for 80% of pediatric torticollis. The remaining 20% includes osseous abnormalities (Klippel-Feil, atlantoaxial rotatory subluxation), tumors (posterior fossa, spinal cord), ocular causes, and Sandifer syndrome (GERD). Consider imaging if no palpable SCM mass, atypical presentation, or failure to improve with stretching.
Etiology Theories:
- Intrauterine compartment syndrome of SCM (most accepted)
- Birth trauma and ischemia to muscle
- Venous occlusion and edema leading to fibrosis
- Associated with breech, oligohydramnios, multiple pregnancy
Pathophysiology and Mechanisms

Sternocleidomastoid Muscle
- Details
- Sternal head: manubrium. Clavicular head: medial clavicle
- Clinical Relevance
- Surgical release usually at clavicular end
- Details
- Mastoid process and lateral superior nuchal line
- Clinical Relevance
- Rarely released proximally
- Details
- Spinal accessory nerve (CN XI)
- Clinical Relevance
- At risk in surgery
- Details
- Ipsilateral tilt, contralateral rotation
- Clinical Relevance
- Explains clinical pattern in CMT
Biomechanics of Torticollis
- Unilateral SCM shortening pulls head into tilt
- Head tilts toward affected (tight) side
- Chin rotates away from affected side
- Limited passive rotation toward affected side
- Over time: facial asymmetry, plagiocephaly
- Plagiocephaly: Flattening of ipsilateral occiput (lies on that side)
- Facial asymmetry: Ipsilateral face appears smaller
- Frontal bossing: Contralateral forehead more prominent
- These changes drive urgency for early treatment
Positional plagiocephaly develops within months if torticollis is untreated. While mild cases improve with treatment, severe plagiocephaly may require helmet therapy. This underscores the importance of early stretching to prevent secondary skull deformity.
The plagiocephaly that accompanies CMT is positional (deformational) and must be distinguished from true unilateral lambdoid synostosis, which is rare but needs surgery. Look at the skull from above (vertex view): positional plagiocephaly produces a parallelogram — the flattened occiput pushes the ipsilateral ear forward with ipsilateral frontal bossing, so the ear and forehead shift toward the flat side. Lambdoid synostosis produces a trapezoid — the ear is displaced posteriorly and inferiorly on the fused side, with an ipsilateral mastoid bulge and contralateral frontal bossing, giving a tilted, windswept skull base. Positional plagiocephaly responds to repositioning and physiotherapy (helmet if severe); suspected synostosis warrants CT with 3D reconstruction and craniofacial referral.
Classification Systems
CMT Subtypes (by SCM characteristics)
- Clinical Finding
- Palpable mass in SCM
- Characteristics
- Most common, present in first weeks, resolves by 4-6 months
- Prognosis
- Excellent with stretching
- Clinical Finding
- Tight SCM without mass
- Characteristics
- No palpable mass, just tight muscle
- Prognosis
- Good with stretching
- Clinical Finding
- Positional preference, no tightness
- Characteristics
- Mildest form, normal ROM
- Prognosis
- Resolves with positioning
All three subtypes generally respond well to conservative treatment if started early.
Clinical Assessment
Systematic Examination
- Birth history: Breech, prolonged labor, forceps/vacuum
- Onset: When noticed head tilt
- Progression: Worsening, stable, improving
- Prior treatment: Any stretching program, PT
- Feeding: Any difficulty (may relate to Sandifer)
- Vision: Any concerns (ocular torticollis)
- Head position: Tilt direction, chin position
- SCM palpation: Mass (pseudotumor), tightness
- Plagiocephaly: Flattening of occiput
- Facial asymmetry: Ipsilateral face smaller
- Neck webbing: May indicate Klippel-Feil
- Passive rotation: Should be symmetric, check deficit
- Passive lateral flexion: Head tilt to each side
- Active ROM: Observe when child looks around
- Compare sides - asymmetry is diagnostic
- Hip examination: Barlow/Ortolani, asymmetry (DDH association, verified nearer 8% - document a clinical hip exam in every case)
- Foot examination: Metatarsus adductus, clubfoot
- Spine examination: Scoliosis, congenital anomalies
- General exam: Dysmorphic features if atypical
Developmental dysplasia of the hip co-exists with CMT in a clinically important minority - verified series report around 8% (Walsh) and about 4.5% requiring treatment (Minihane), below the classic 20% quote. Both conditions share the etiology of intrauterine crowding and malpositioning. A documented clinical hip examination is mandatory in every CMT patient; targeted ultrasound or radiograph follows an abnormal exam or DDH risk factors.
Investigations
X-ray cervical spine if: atypical features, no palpable SCM mass, failure to respond to stretching, restricted ROM in multiple planes, or concern for bony anomaly. Most routine CMT with classic features does not require imaging.
- When Used
- Atypical presentation, no improvement, bony abnormality suspected
- What to Look For
- Klippel-Feil, hemivertebra, atlantoaxial anomaly
- When Used
- Early, if diagnosis uncertain
- What to Look For
- Muscle thickening, echogenicity changes
- When Used
- CMT infant under 6 months with abnormal hip exam or DDH risk factors
- What to Look For
- DDH screening
- When Used
- Neurological signs, severe or atypical
- What to Look For
- Cord abnormality, tumor
- When Used
- Suspected atlantoaxial rotatory fixation
- What to Look For
- AARF diagnosis
When to Consider Non-CMT Causes:
- No palpable SCM mass or tightness
- Multiple planes of restriction
- Onset after first few months of life
- Neurological signs
- Failure to improve with proper stretching
Differential Diagnosis
The single most important exam skill is separating benign CMT from sinister or non-muscular causes. Atypical features (no SCM mass, onset after the first weeks, multi-plane restriction, neurological signs, or failure to respond to stretching) mandate further work-up.
- Distinguishing features
- Present at/near birth, SCM mass or tight band, isolated rotation deficit
- Key investigation
- Clinical; SCM ultrasound if unsure
- Implication
- Conservative stretching first-line
- Distinguishing features
- Short neck, low posterior hairline, limited multi-plane ROM, no SCM mass
- Key investigation
- Cervical radiograph (fused vertebrae)
- Implication
- Screen hearing, renal, cardiac, Sprengel; stretching ineffective
- Distinguishing features
- Acute onset, often after URTI (Grisel) or trauma, cock-robin posture, painful
- Key investigation
- Dynamic CT C-spine
- Implication
- Reduction; avoid forceful manipulation
- Distinguishing features
- Later onset, intermittent, full passive ROM, resolves when eyes covered
- Key investigation
- Ophthalmology (cranial nerve IV palsy, strabismus)
- Implication
- Treat the eye, not the neck
- Distinguishing features
- Paroxysmal posturing with feeds/reflux (GERD), normal between episodes
- Key investigation
- Clinical; pH study/upper GI if needed
- Implication
- Treat reflux
- Distinguishing features
- Progressive, neurological signs, head tilt to relieve pressure, vomiting
- Key investigation
- MRI brain and whole spine
- Implication
- Urgent neurosurgical referral
A head tilt that is new, progressive, painful, accompanied by neurological signs, or unresponsive to stretching is NOT congenital muscular torticollis until imaging proves otherwise. The dangerous misses are a posterior fossa tumour and atlantoaxial rotatory fixation.
A torticollis that is episodic and recurrent rather than fixed points away from CMT toward benign paroxysmal torticollis of infancy (BPTI). Recurrent, self-limiting attacks of head tilt (lasting hours to days) begin in the first year, often with pallor, irritability, vomiting or ataxia, and the child is entirely normal between episodes with full passive range of motion and no SCM mass. It is regarded as a migraine-variant / channelopathy (associated with CACNA1A, the gene of familial hemiplegic migraine and episodic ataxia type 2), usually with a family history of migraine. It is a clinical diagnosis of exclusion that resolves spontaneously by age 2-3 years; the priority is to exclude posterior fossa pathology and atlantoaxial rotatory fixation before reassuring.
Management Algorithm
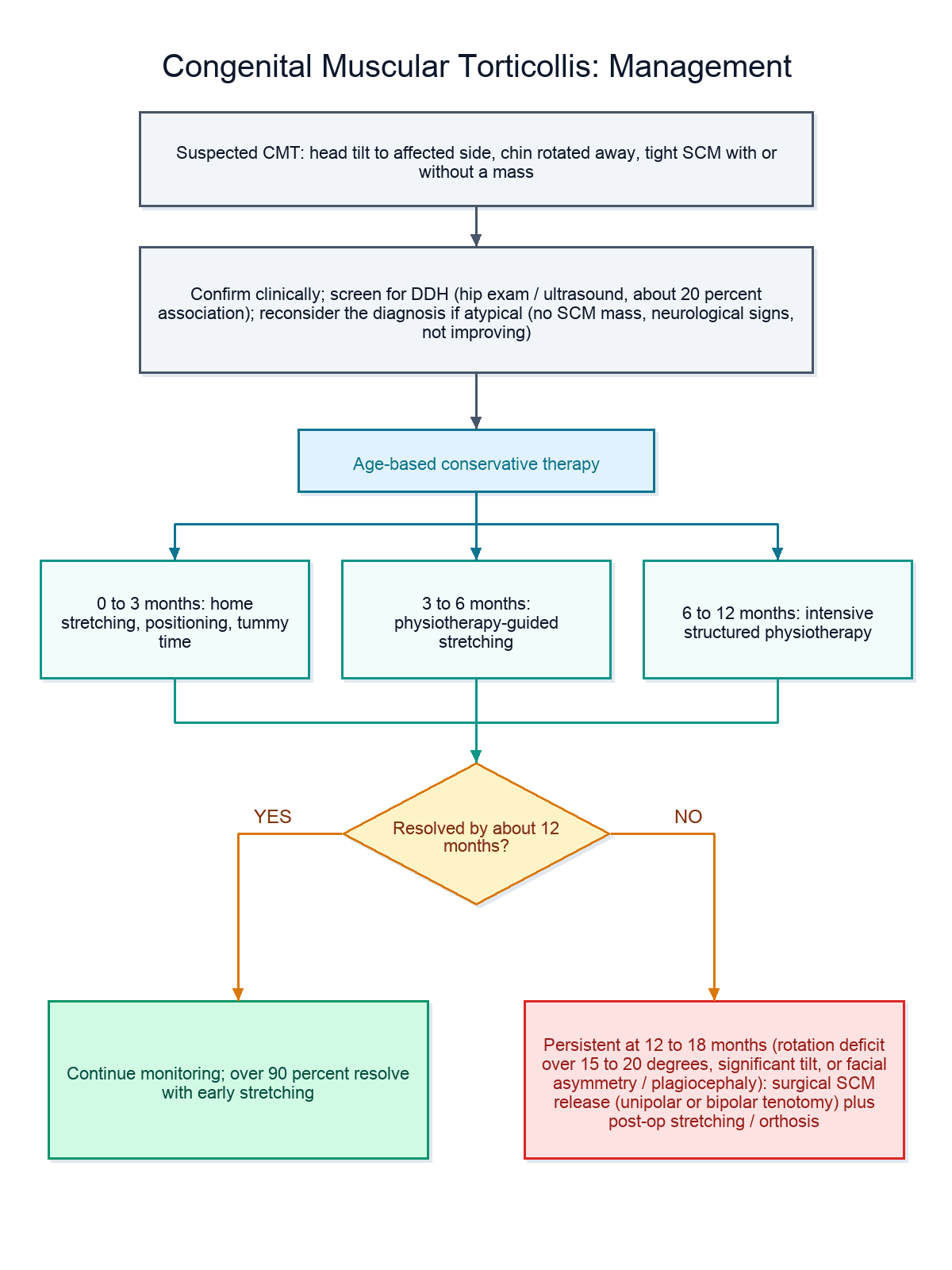
Physiotherapy-Based Management
- Approach
- Home program
- Key Elements
- Parent stretching, positioning, tummy time
- Expected Outcome
- Most resolve
- Approach
- PT-guided
- Key Elements
- Formal physiotherapy if not resolving
- Expected Outcome
- High success
- Approach
- Intensive PT
- Key Elements
- More structured program, monitor progress
- Expected Outcome
- Most still resolve
- Approach
- Re-evaluate
- Key Elements
- Consider surgery if significant residual deficit
- Expected Outcome
- Some need surgery
- Hold baby's shoulder down on affected side
- Tilt head TOWARD opposite side (stretches tight SCM)
- Rotate chin TOWARD affected side
- Hold 10-30 seconds, repeat 10-15 times
- Do at every diaper change (easily 4-6 times daily)
- Encourage looking toward affected side
- Toys, lights, parent position on affected side
- Tummy time supervised when awake
- Avoid prolonged time on back same position
Early, consistent stretching leads to greater than 90% success rate.
STRETCHSTRETCH - Treatment Principles
Hook:STRETCH the SCM by tilting opposite and rotating toward - start early for best results.
Surgical Technique
Open Unipolar SCM Release (Clavicular)
Standard procedure for CMT not responding to conservative treatment.
Surgical Steps
- Supine with shoulder roll
- Head turned toward affected side (exposes clavicular SCM)
- General anesthesia
- Transverse incision 1-2cm above clavicle
- In skin crease for cosmesis
- Approximately 2-3cm length
- Divide platysma
- Identify SCM sternal and clavicular heads
- Protect external jugular vein laterally
- Identify and protect spinal accessory nerve
- Divide SCM at its clavicular and sternal insertions
- Can divide any tight bands felt
- Passively move head to test release
- Should achieve full correction on table
- Hemostasis
- Close platysma, subcuticular skin closure
- Dressing, may use soft collar for comfort
Technical Points:
- Small incision in skin crease gives excellent cosmesis
- Ensure full correction achieved intraoperatively
- Be aware of spinal accessory nerve crossing SCM
Post-operative physiotherapy is essential for maintaining correction.
Complications
- Incidence
- 5-10% (usually minor)
- Prevention/Management
- Compliance with post-op PT, stretching
- Incidence
- Rare (less than 1%)
- Prevention/Management
- Careful dissection, know anatomy
- Incidence
- Minimal with skin crease incision
- Prevention/Management
- Transverse incision placement
- Incidence
- Rare
- Prevention/Management
- Avoid excessive release, PT guided
- Incidence
- Variable
- Prevention/Management
- May need helmet if severe, usually improves with time
- Incidence
- Improves but may not fully correct
- Prevention/Management
- Earlier treatment = better outcome
Facial asymmetry and plagiocephaly may improve but not fully resolve even with successful treatment. Earlier intervention leads to better remodeling potential. Families should be counseled that some residual asymmetry may remain.
Postoperative Care and Rehabilitation
Post-Surgery Protocol
- Wound check, remove dressing
- Soft collar for comfort (optional)
- Gentle ROM encouraged
- Discharge day 1 usually
- Begin formal stretching exercises
- PT referral
- Wound care
- Maintain correction with positioning
- Active physiotherapy program
- Stretching continued by parents at home
- Gentle strengthening as tolerated
- May use headband/brace overnight if needed
- Ongoing stretching maintenance
- Monitor for recurrence
- Assess facial/skull symmetry
- Discharge from active PT when stable
Conservative Treatment Rehabilitation:
- Continue stretching until full symmetric ROM achieved
- Gradual weaning of frequency once normalized
- Positioning strategies ongoing in infancy
- Monitor for recurrence
Outcomes
- Greater than 90% success if started before 1 year
- Best outcomes with early diagnosis and treatment
- Pseudotumor resolves by 4-6 months
- ROM normalizes within months in most cases
- High rates of good to excellent results across series
- Full or near-full ROM typically achieved
- Facial asymmetry and plagiocephaly improve but may not fully resolve - earlier correction gives greater remodeling potential
- Note the nuance: Shim (JBJS Br 2008) found movement, scar and head-tilt scores were as good or better in children operated at 5-16 years than at 1-4 years, and recommended deferring surgery until the child can comply with post-operative bracing and exercises. Surgery is therefore effective across the age range; the case for early intervention rests mainly on facial/skull remodeling rather than on ROM outcome
Guidelines, Registries & Global Practice
Global epidemiology:
- Reported birth incidence ranges from about 0.4% to as high as 16% depending on definition and screening intensity; a commonly cited clinical figure is 1-2% of newborns
- Third most common congenital musculoskeletal condition after DDH and clubfoot
- Right-sided predominance (roughly 75%); modest male predominance in several series
- Risk factors converge on intrauterine crowding/positioning: breech presentation, primiparity, oligohydramnios, multiple gestation and difficult/instrumented delivery
- The CMT-DDH association is real but smaller than the textbook 20%: verified series report around 8% (Walsh) and about 4.5% requiring treatment (Minihane), within a literature range of 2-29%
Side-by-side guidance (where emphasis differs):
- Region
- US/International
- Key emphasis
- Refer to physiotherapy as soon as asymmetry is found; severity classification; first-line passive and active ROM plus positioning; defined escalation criteria
- Region
- US
- Key emphasis
- Supine sleeping for SIDS prevention drove a rise in positional plagiocephaly and torticollis - counsel supervised tummy time and repositioning
- Region
- UK
- Key emphasis
- Plagiocephaly and CMT largely managed conservatively; helmet (cranial orthosis) therapy not routinely recommended on NHS for positional plagiocephaly given limited evidence and cost
- Region
- Global
- Key emphasis
- Conservative stretching before age 1; surgical release reserved for failure of an adequate stretching programme with persistent deficit/tight band
- CMT is not tracked in arthroplasty/implant registries; the evidence base is cohort and case-series level, anchored by the Cheng 821-patient prospective cohort
- Cranial orthosis (helmet) policy diverges internationally: more readily used in parts of North America, more restricted in several European public systems where high-quality comparative evidence is felt to be lacking
- High-resource settings: early physiotherapy referral, ultrasound for SCM/hip when indicated, access to cranial orthoses and craniofacial multidisciplinary teams
- Limited-resource settings: diagnosis is clinical; parent-delivered stretching is the mainstay; later presentation is more common, increasing the proportion needing surgical release and the burden of established facial asymmetry; emphasis falls on caregiver education and low-cost positioning strategies
Controversies and Areas of Uncertainty
Textbooks quote 20%, but the best primary series (Walsh approximately 8%; Minihane 4.5% requiring treatment) suggest the figure is considerably lower and that a normal clinical hip examination reliably excludes significant DDH. Whether universal hip ultrasound is justified in every CMT infant, or only those with an abnormal exam/risk factors, remains debated.
Conventional teaching favours release by 12-18 months, yet Shim found older children (5-16 years) had movement and scar outcomes at least as good as younger ones. The strongest argument for early surgery is facial/skull remodeling, not ROM. There is no high-level trial defining the ideal age.
Evidence on whether orthoses outperform repositioning for positional plagiocephaly is mixed; Lam reported greater measured head-shape correction with orthoses, but a randomised trial (Dutch HEADS study, not cited here) found no clinically meaningful difference for mild-to-moderate cases. Practice varies widely by region and payer.
Endoscopic/arthroscopic release (Wang) and open unipolar/bipolar techniques all report good outcomes, but no adequately powered head-to-head trial establishes superiority. Choice remains surgeon- and resource-dependent.
MCQ Practice Points
Q: In CMT affecting the right SCM, which direction does the head tilt? A: The head tilts to the RIGHT (toward the tight muscle). The chin rotates to the LEFT (away from the tight side).
Q: What musculoskeletal condition should you screen for in all CMT patients? A: Developmental dysplasia of the hip (DDH). The classic teaching is a 20% association, but verified series show nearer 8% (and about 4.5% requiring treatment) - so the imperative is a documented clinical hip examination in every CMT infant, with imaging reserved for abnormal findings or risk factors.
Q: How do you stretch a tight right SCM? A: Tilt the head to the LEFT (opposite to tight side) and rotate the chin to the RIGHT (toward the tight side).
Q: When should surgery be considered for CMT? A: After 12-18 months if no improvement with proper physiotherapy, or if significant rotation deficit (greater than 15-20°) persists.
Medicolegal Considerations
- Document head position, SCM mass, ROM measurements
- Record hip examination findings
- Document stretching instructions given to parents
- Note compliance with stretching at follow-up
- Record imaging results if obtained
- Scarring (usually minimal in skin crease)
- Recurrence risk (5-10%)
- Spinal accessory nerve injury (rare)
- Need for post-operative physiotherapy
- Residual facial asymmetry possible
Failure to examine the hips in CMT is a medicolegal risk. Even at the verified association rate (around 8%, with roughly 4.5% needing treatment), a documented clinical hip examination - and targeted imaging when the exam is abnormal or risk factors are present - should be recorded in all CMT patients.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 6-week-old infant is brought in with a persistent head tilt to the right. The mother noticed it shortly after birth and is concerned about the position.”
“A 14-month-old child with CMT has been receiving physiotherapy since 4 months of age. Despite reported compliance, there remains 25 degrees of rotation deficit and significant facial asymmetry.”
“A 3-month-old presents with a head tilt but you cannot feel an SCM mass. The passive ROM seems restricted in multiple planes. The parents report the tilt was not present at birth but appeared at around 6 weeks of age.”
Clinical Pattern
- Head tilts TOWARD tight SCM
- Chin rotates AWAY from tight side
- Limited rotation TO affected side
- Pseudotumor in first weeks (resolves by 4-6 months)
Associated Conditions
- DDH co-exists (around 8%, under 10%) - examine hips in every case
- Plagiocephaly - develops with persistent tilt
- Facial asymmetry - ipsilateral face smaller
- Metatarsus adductus (packaging)
Conservative Treatment
- Tilt head OPPOSITE to tight side
- Rotate chin TOWARD tight side
- Do at every diaper change
- Positioning: toys on affected side
Surgical Indications
- No improvement by 12-18 months
- Rotation deficit greater than 15-20 degrees
- Significant residual tilt/asymmetry
- Unipolar clavicular release standard
Differentials
- Klippel-Feil (fused vertebrae)
- AARF (atlantoaxial rotatory fixation)
- Ocular torticollis
- Sandifer syndrome (GERD)
Evidence Base
Landmark prospective cohort: manual stretching and surgery threshold
- Prospective study of 821 consecutive infants seen under 1 year, standardised manual stretching, mean follow-up 4.5 years
- Three clinical groups: sternomastoid tumour 55% (452), muscular torticollis 34% (276), postural torticollis 11% (93)
- Subsequent surgery required in 8% of the tumour group, 3% of the muscular group, 0% of the postural group
- Outcome predicted by clinical group, initial passive rotation deficit, and age at presentation
Operative timing: outcomes by age at surgery
- 47 children undergoing operative release, mean follow-up 74 months
- Group 1 aged 1-4 years versus Group 2 aged 5-16 years
- Craniofacial asymmetry and overall scores were similar between groups
- Older children (Group 2) had SUPERIOR movement, scar and head-tilt outcomes
CMT-DDH association: lower than the quoted 20%
- Retrospective review of 70 children with congenital muscular torticollis
- 6 had hip subluxation or dislocation, all detectable at presentation
- Calculated hip-disease rate of approximately 8%, lower than the 20% often quoted
- Reported literature range for the association spans 2-29%
Hip imaging strategy in CMT
- 292 infants with CMT reviewed; 16 had developmental dysplasia of the hip
- Every infant with DDH had an ABNORMAL clinical hip examination
- Coexistence rate for CMT and DDH requiring treatment was 4.5%
- Routine hip imaging not required when the clinical hip examination is normal
Minimally invasive (arthroscopic/endoscopic) release
- 69 teenagers (mean age 16.1 years) with arthroscopic radiofrequency release under local anaesthesia
- Mean rotation deficit improved from 22.5 to 4.1 degrees; lateral-bend deficit 14.6 to 3.3 degrees
- Good or excellent result (Cheng score) in 65 of 69 patients (94.2%)
- No intra-operative or post-operative complications reported
Positional plagiocephaly: factors influencing correction
- 991 infants under 1 year evaluated for positional skull deformity; 552 followed to completion
- Cranial orthosis produced the largest correction in oblique diagonal difference; repositioning/PT the least
- Earlier age at presentation correlated with greater head-shape correction
- Torticollis history was NOT significantly associated with magnitude of correction on multivariate analysis
APTA Evidence-Based Clinical Practice Guideline (CMT)
- 17 action statements linking graded evidence to practice, updating the 2013 guideline
- Infants with CMT should be referred to physical therapy as soon as asymmetry is identified
- Structured severity classification and referral flow sheets for monitoring, treating and onward referral
- First-choice intervention is neck passive range of motion, active range of motion and positioning/environmental adaptation