Tillaux (SH-III) | Triplane (SH-IV) | Adolescent Ankle | CT Essential
- Occur during physeal closure - Central, Medial, then Lateral (CML)
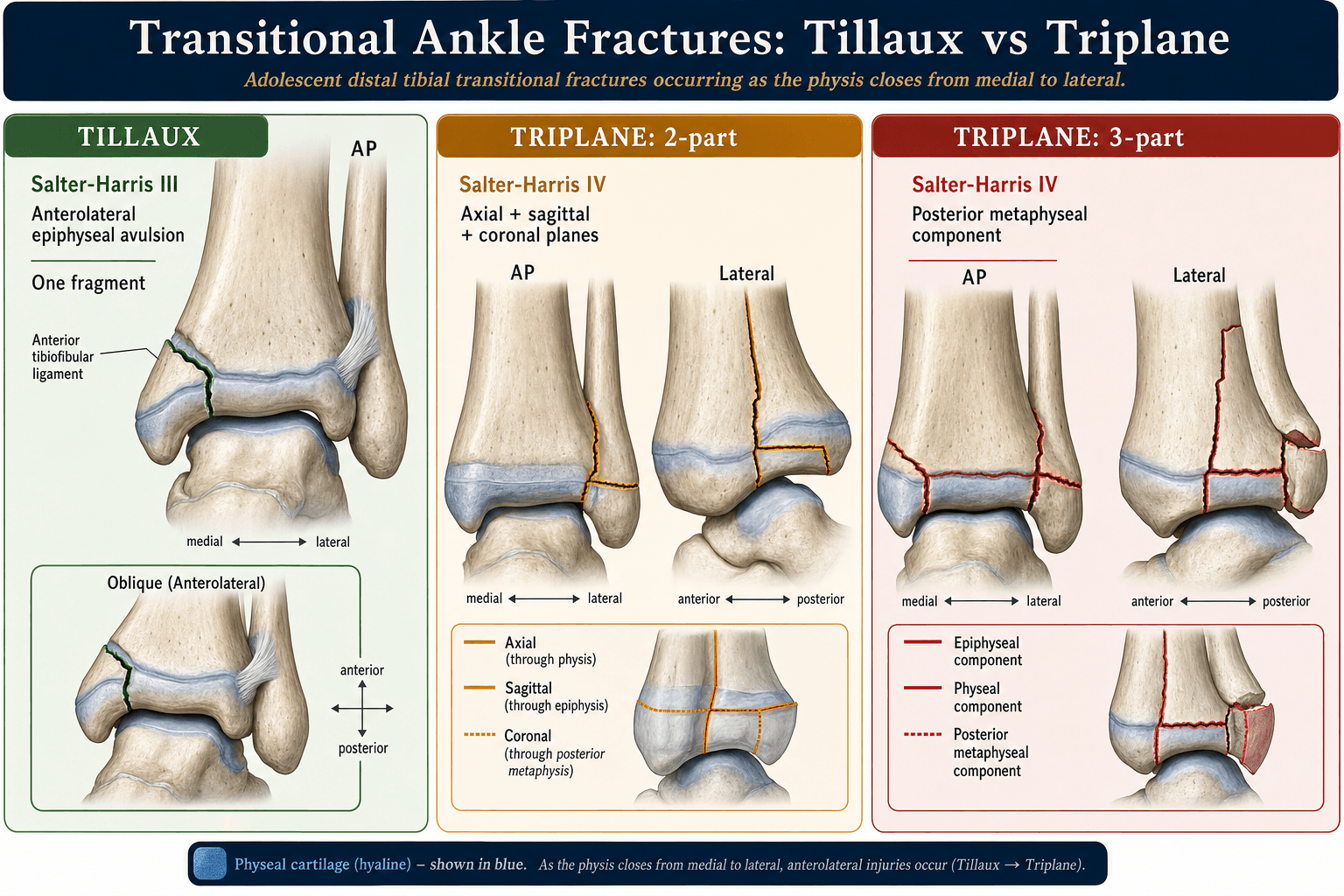
- Tillaux = SH-III - anterolateral epiphysis only
- Triplane = SH-IV - epiphysis + metaphysis (2 or 3 part)
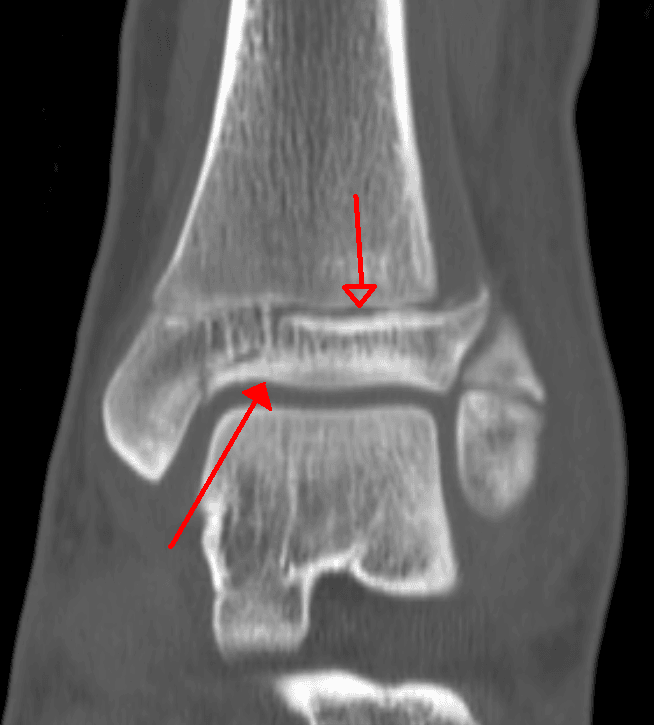
- CT is essential to determine fracture configuration and step-off
- Greater than 2mm articular step-off requires ORIF
- “Tillaux and Triplane are NOT adult ankle fractures
- “CT defines 2-part vs 3-part triplane pattern
- “Anterolateral fragment in Tillaux is attached to AITFL
- “Near skeletal maturity means low growth arrest risk
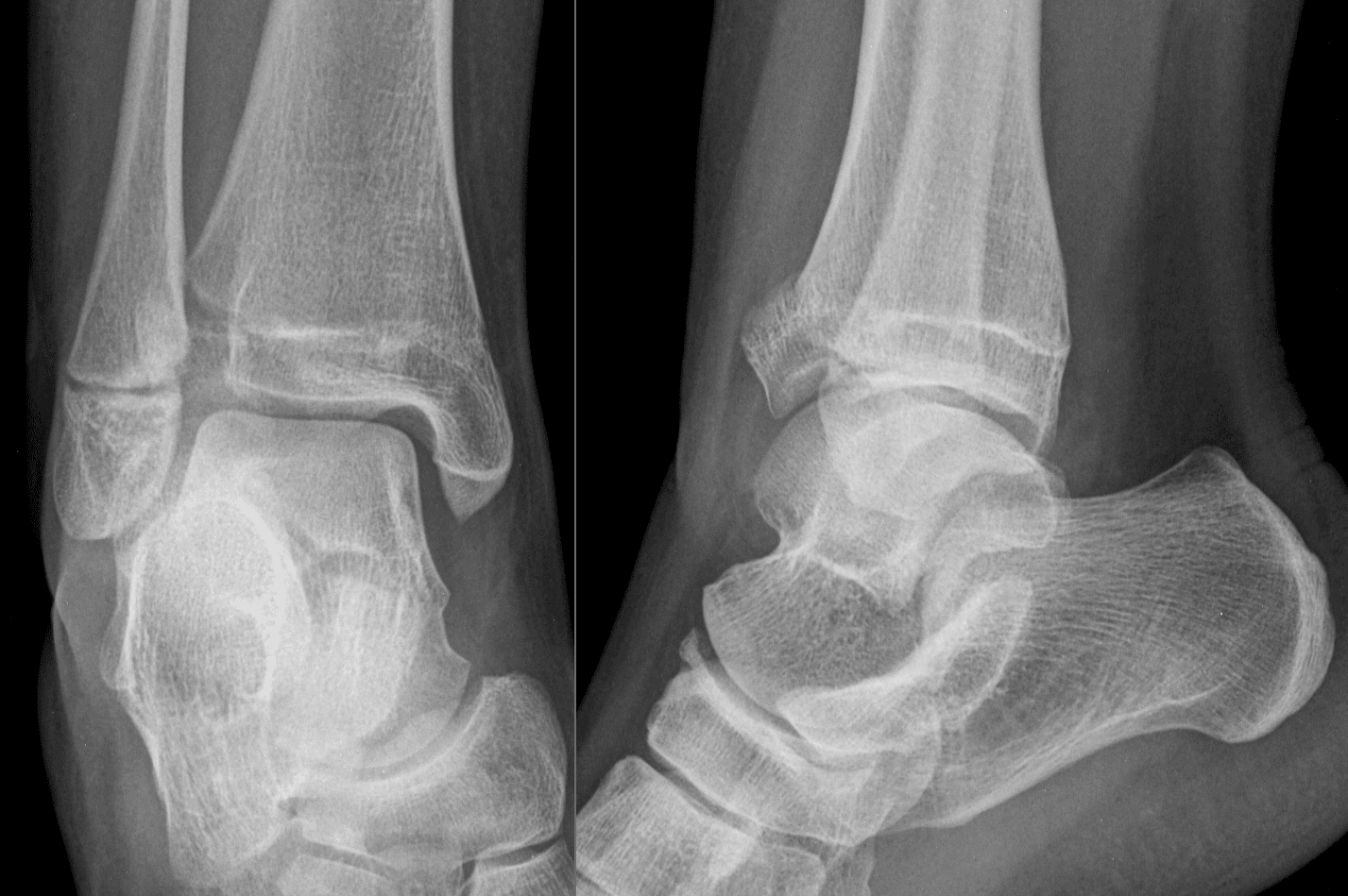
X-rays underestimate displacement. CT scan is essential to determine 2-part vs 3-part triplane, measure articular step-off, and plan surgical approach.
The distal tibial physis closes Central, Medial, Lateral (CML) over 18 months. Transitional fractures occur when lateral physis is still open.
Greater than 2mm articular step-off is the threshold for operative treatment. Measure on CT axial and sagittal reformats.
These occur near skeletal maturity, so growth arrest is rarely clinically significant. Focus on articular reduction.
- Fracture Type
- Tillaux or Triplane
- Treatment
- Long leg cast 4-6 weeks
- Key Pearl
- Weekly X-rays to check displacement
- Fracture Type
- Tillaux
- Treatment
- ORIF via anterolateral approach
- Key Pearl
- Single epiphyseal screw
- Fracture Type
- 2-Part Triplane
- Treatment
- ORIF - one approach may suffice
- Key Pearl
- Lateral approach, epiphyseal + metaphyseal screws
- Fracture Type
- 3-Part Triplane
- Treatment
- ORIF - may need medial approach
- Key Pearl
- Fix medial epiphyseal fragment separately
CMLPhyseal Closure Pattern
Hook:CML - Closes in the Middle, then Later Lateral leaves the anterolateral fragment vulnerable!
TILTTillaux Key Features
Hook:The Tillaux TILTs when AITFL pulls the anterolateral fragment!
Overview/Epidemiology
Transitional fractures are unique pediatric ankle injuries occurring during the 18-month period of asymmetric distal tibial physeal closure.
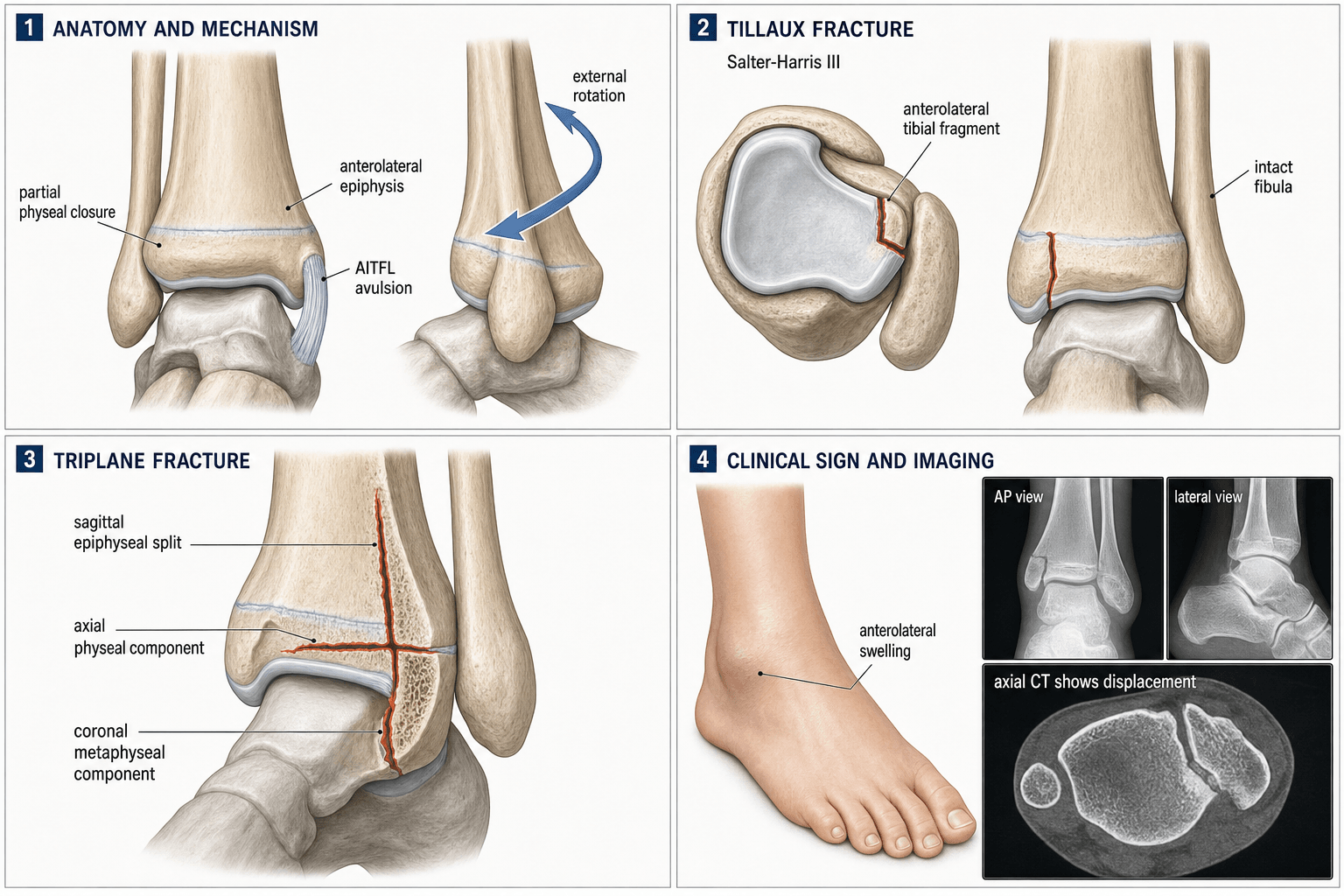
- External rotation of the foot on a fixed leg (similar to adult ankle fracture mechanism).
- The anterolateral fragment is avulsed via the anterior inferior tibiofibular ligament (AITFL).
- The pattern depends on which portions of the physis remain open.
- These are intra-articular injuries requiring anatomic reduction.
- Growth arrest is rarely clinically significant due to near-skeletal maturity.
- Focus is on articular congruity, not physeal preservation.
Anatomy and Pathomechanics
Physeal Closure Pattern (CML):
- The distal tibial physis closes asymmetrically over approximately 18 months.
- Central portion closes first (age 12-13).
- Medial portion closes next (age 14-15).
- Lateral (anterolateral) portion closes last (age 15-16).
When the medial physis has fused but the lateral remains open, external rotation forces cause the AITFL to avulse the anterolateral epiphyseal fragment - creating a Tillaux fracture. If the force propagates into the metaphysis, a Triplane results.
- AITFL (Anterior Inferior Tibiofibular Ligament): Attaches to the anterolateral tibia (Tillaux fragment).
- Lateral malleolus: Usually intact (not fractured in pure transitional fractures).
- Fibular physis: Closes earlier than tibial physis.
- Sagittal through the epiphysis (separating anterior from posterior).
- Transverse/Axial through the physis.
- Coronal through the metaphysis.
Hence the name "triplane" - three planes of fracture.
Classification Systems
Tillaux Fracture (Juvenile Tillaux)
Salter-Harris Type III
- Involves physis and epiphysis only.
- Anterolateral epiphyseal fragment.
- Occurs when only the lateral physis remains open.
- Tillaux
- 12-15 years
- Adult Chaput Tubercle
- Adult
- Tillaux
- Partially open
- Adult Chaput Tubercle
- Closed
- Tillaux
- Intact
- Adult Chaput Tubercle
- May be involved
Treatment: ORIF if more than 2mm articular step-off.
This represents the final stage of the transitional fracture spectrum.
Medial and Intramalleolar Triplane Variants
Most triplane fractures are lateral - the epiphyseal fragment is anterolateral, as described above - but two less common variants are examinable because they behave differently and are easy to miss if you assume every triplane exits laterally.
- Where the fracture exits
- Anterolateral epiphysis (AITFL-bearing), as in Tillaux
- Why it matters
- Commonest pattern; intra-articular at the lateral plafond
- Management note
- ORIF if step over 2 mm; lateral approach
- Where the fracture exits
- Through the medial malleolus / medial plafond
- Why it matters
- Tends to occur in slightly younger children with more open physis; can be intra-articular medially and carries a relatively higher growth-disturbance risk
- Management note
- CT to map fragments; anatomic reduction of the medial plafond; watch the physis
- Where the fracture exits
- Vertical epiphyseal limb running within the medial malleolus
- Why it matters
- Rare; the key question is whether the articular exit lies within the WEIGHT-BEARING plafond
- Management note
- Intra-articular weight-bearing variant needs anatomic ORIF; a purely extra-articular exit behaves benignly
The unifying principle is unchanged: define the fragments and the articular exit on CT, and reduce any step within the weight-bearing plafond to under 2 mm. The reason to recognise the medial variant specifically is that it appears in a slightly younger patient with more growth remaining, so the standard reassurance about growth arrest is less absolute than for the classic late-adolescent lateral Tillaux/triplane.
If the epiphyseal fragment exits medially rather than anterolaterally, think medial / intramalleolar triplane (Cummings classified the intramalleolar variant by whether the articular exit lies in the weight-bearing plafond). These occur in younger patients with more growth remaining, so growth-arrest risk is genuinely higher and articular reduction of the medial plafond matters - map it on CT exactly as you would a lateral triplane.
STEPTriplane Decision Making
Hook:STEP through the CT to plan your surgery - don't skip the scan!
Clinical Assessment
- Mechanism: Rotational injury (external rotation of foot).
- Age: 12-15 years (crucial - physis must be closing).
- Pain location: Anterolateral ankle.
- Weight-bearing: Usually unable.
- Inspection: Swelling, ecchymosis anterolaterally.
- Palpation: Point tenderness over anterolateral physis.
- Movement: Painful ROM, especially external rotation.
- Neurovascular: Document (usually intact).
Differentiation from Adult Ankle Fractures:
- Age is the key factor.
- In adolescents, the physis is weaker than the ligaments.
- Similar mechanisms cause physeal fractures, not ligament sprains.
Investigations
Imaging Protocol
AP, Lateral, Mortise views. Look for physeal widening laterally, epiphyseal fragment on mortise view. X-rays often underestimate displacement.
Mandatory for all transitional fractures. Determines 2-part vs 3-part pattern, measures articular step-off accurately, and guides surgical approach.
Rarely needed. May help if diagnosis unclear or to assess soft tissue/ligament injury.
Plain radiographs consistently underestimate displacement. A fracture that appears 1-2mm on X-ray may be more than 2mm on CT. Always get a CT before deciding on non-operative treatment.
Differential Diagnosis
The anterolateral painful adolescent ankle after a twisting injury has a tight differential. The pivotal discriminator is patient age and physeal status - the same external-rotation force produces a ligament sprain in an adult but a physeal fracture in an adolescent because the open physis is weaker than the AITFL.
- Typical Age
- 12-15 (lateral physis open)
- Salter-Harris / Pattern
- SH-III
- Key Discriminator
- Isolated anterolateral epiphyseal fragment, metaphysis intact
- Imaging Clue
- Mortise view + axial CT: single epiphyseal fragment
- Typical Age
- 10-14 (more physis open than Tillaux)
- Salter-Harris / Pattern
- SH-IV (multiplanar)
- Key Discriminator
- Epiphyseal + metaphyseal involvement, 2 or 3 fragments
- Imaging Clue
- Lateral X-ray looks SH-II, AP looks SH-III; CT resolves
- Typical Age
- Skeletally mature
- Salter-Harris / Pattern
- Intra-articular avulsion
- Key Discriminator
- Physis closed, often with syndesmotic injury
- Imaging Clue
- No physeal lucency; assess syndesmosis
- Typical Age
- Adult
- Salter-Harris / Pattern
- Fibular fracture +/- medial
- Key Discriminator
- Fibula fractured; physes closed
- Imaging Clue
- Talar shift, fibular fracture line
- Typical Age
- Under 12 (whole physis open)
- Salter-Harris / Pattern
- SH-I / SH-II
- Key Discriminator
- Whole physis open, metaphyseal Thurston-Holland fragment
- Imaging Clue
- No isolated anterolateral fragment
- Typical Age
- Any (but rare to be pure in adolescent)
- Salter-Harris / Pattern
- Soft-tissue
- Key Discriminator
- No bony tenderness over physis, normal films
- Imaging Clue
- Normal radiographs; MRI shows ligament only
A 13-year-old who has "just sprained an ankle" with point tenderness over the anterolateral distal tibia has a Tillaux fracture until proven otherwise. In the adolescent the physis fails before the ligament, so dedicated radiographs (and CT if a fragment is seen) are mandatory before labelling it a sprain.
Management Algorithm
Non-Displaced or Minimally Displaced (Less than 2mm on CT)
- Articular step-off less than 2mm on CT.
- Acceptable alignment on X-ray.
- Long leg cast or CAM boot for 4-6 weeks.
- Non-weight bearing initially, then progressive WB.
- Weekly X-rays for 2-3 weeks to ensure no displacement.
Early displacement is possible. If step-off increases beyond 2mm on follow-up X-ray, convert to operative treatment.
Surgical Techniques
Patient Positioning
Position: Supine on radiolucent table. Padding: Bump under ipsilateral hip (slight internal rotation of leg). Draping: Free drape the lower extremity for manipulation. C-arm: From contralateral side for AP, mortise, and lateral views.
A small bump under the hip internally rotates the leg, making the anterolateral approach more accessible.
Intraoperative Tips:
- Use fluoroscopy liberally to confirm reduction.
- The articular surface should be anatomic (less than 1-2mm step).
- Avoid screw penetration into the joint.
Complications
- Incidence
- Variable
- Risk Factors
- Non-anatomic reduction
- Management
- Accept less than 2mm, revise if more
- Incidence
- Rare short-term
- Risk Factors
- Articular incongruity
- Management
- Anatomic reduction prevents
- Incidence
- Rare clinically
- Risk Factors
- Near maturity
- Management
- Usually not significant
- Incidence
- Uncommon
- Risk Factors
- Prolonged immobilization
- Management
- Early mobilization
- Incidence
- Rare
- Risk Factors
- Lateral approach
- Management
- Careful dissection
Unlike more proximal physeal injuries, growth arrest in transitional fractures is rarely clinically significant because these patients are near skeletal maturity. Focus on articular reduction rather than physeal preservation.
Detecting and Managing Growth Disturbance
Although growth arrest is usually inconsequential in the late-adolescent Tillaux or lateral triplane, the risk is not zero - and in younger patients (and the medial variants above) a partial physeal bar can produce angular deformity or leg-length discrepancy. Examiners expect you to know how you would detect and manage it, not simply assert that it "rarely matters."
Detection
- Surveillance to skeletal maturity in the younger or higher-risk patient, with comparison radiographs of the contralateral limb.
- Harris (growth-arrest) lines: a transverse sclerotic line laid down after the injury. A line that stays parallel to the physis indicates symmetric resumed growth; a line that is asymmetric or converges toward the physis points to a tethering bar at the point of convergence.
- Cross-sectional bar mapping: CT or MRI to locate and size a suspected physeal bar, expressed as a percentage of the physeal area, which guides treatment.
Management
- Option
- Bar resection with interposition (e.g. fat graft or bone wax / PMMA)
- Rationale
- Can restore growth if enough healthy physis remains
- Option
- Complete the arrest, plus contralateral epiphysiodesis if leg-length discrepancy is projected
- Rationale
- Prevents progressive angular deformity and balances limb length
- Option
- Corrective osteotomy and/or limb-length equalisation
- Rationale
- Addresses the established deformity rather than the physis itself
The practical rule: the closer to skeletal maturity, the less you need to do - the classic late-adolescent Tillaux essentially needs nothing - but a younger patient deserves follow-up because a partial bar is treatable if it is caught early.
"Rarely significant" is the right headline, but be ready for the examiner's follow-up: detect a bar with Harris lines and CT/MRI mapping, then manage it by bar resection (small bar, growth remaining), completion of the arrest with contralateral epiphysiodesis (large bar or near maturity), or osteotomy for established deformity.
Postoperative Care
Rehabilitation Protocol
Backslab initially, convert to short leg cast. Non-weight bearing. Elevation, ice.
Short leg cast or CAM boot. Non-weight bearing continues. Check X-rays at 2-4 weeks.
If healing confirmed, transition to weight-bearing as tolerated in boot. Begin gentle ankle ROM.
Wean from boot. Physiotherapy for ROM and strength. Return to sport at 3 months if healed and strong.
Hardware:
- Screws are usually left in situ unless symptomatic.
- No routine removal needed.
Outcomes/Prognosis
- Articular reduction quality is the main determinant of outcome.
- Greater than 2mm step is associated with increased arthritis risk.
- Growth arrest, if it occurs, is usually not clinically significant.
- Most return to full sport by 3-4 months.
- Outcomes are generally excellent with appropriate treatment.
Guidelines, Registries & Global Practice
Global epidemiology:
- Triplane fractures account for approximately 5-10% of paediatric intra-articular ankle injuries (Schnetzler & Hoernschemeyer 2007); juvenile Tillaux is rarer.
- Peak age 12-15 years, with triplane tending to occur slightly younger than Tillaux because more of the physis remains open.
- Slight male predominance; mechanism is external rotation across a narrow window of asymmetric physeal closure, so true incidence is similar worldwide where physeal maturation is comparable.
Side-by-side guidance (no formal RCT-based guideline exists - recommendations are consensus/textbook-derived):
- Imaging stance
- CT for displaced or intra-articular patterns
- Operative threshold
- ORIF if step over 2 mm
- Emphasis
- Anterolateral or anteromedial approach, screw fixation
- Imaging stance
- Cross-sectional imaging when surgery contemplated; senior decision-maker
- Operative threshold
- Restore articular congruity
- Emphasis
- Definitive care in unit with paediatric expertise
- Imaging stance
- CT for fragment mapping and pre-op planning
- Operative threshold
- Anatomic joint reduction; lag screw fixation
- Emphasis
- Respect closing physis; avoid hardware across open lateral physis
- Imaging stance
- CT to define 2- vs 3-part configuration
- Operative threshold
- Reduce to under 2 mm; closed/percutaneous if achievable
- Emphasis
- Minimise soft-tissue insult, early mobilisation
- Paediatric physeal ankle fractures are not implant-survival registry topics (these are not arthroplasty), so NJR/AOANJRR/AJRR data do not apply.
- Evidence is therefore single-centre Level III-IV series and reviews, not registry datasets - candidates should know the evidence base is comparatively thin.
- High-resource: routine CT, image-intensifier-guided or arthroscopic-assisted percutaneous screws, day-case ORIF.
- Limited-resource: reliance on good mortise radiographs and closed reduction; CT reserved for clearly displaced cases; cast immobilisation more often accepted when CT is unavailable.
Counselling points (globally applicable):
- Explain that growth arrest is unlikely to be clinically significant because the patient is near skeletal maturity.
- Emphasise that the goal is articular congruity, and that displacement may be greater on CT than on plain films.
- Consent should cover the small risks of stiffness, superficial peroneal nerve irritation, and the possibility of converting a closed plan to open reduction.
Controversies and Areas of Uncertainty
The 2 mm step-off rule derives from small Level IV series (Ertl 1988, Rapariz 1996). Some authors argue the location of the gap matters more than the absolute number - a step outside the principal weight-bearing zone may tolerate more displacement, whereas central plafond incongruity warrants reduction even near 2 mm. No randomised data exist to define a precise cut-off.
CT undeniably changes management (Eismann 2015), but it adds radiation and cost. A reasonable compromise is selective CT for any fracture that looks displaced, intra-articular, or triplane on plain films, while truly non-displaced extra-articular patterns may be followed radiographically. Practice varies by centre.
Several series report success with closed or percutaneous fixation under fluoroscopic and even arthroscopic control, avoiding open arthrotomy. Critics counter that the articular surface cannot be verified to within 2 mm without direct or CT-confirmed visualisation. The decision hinges on surgeon experience and intra-operative imaging quality.
MRI avoids radiation and shows the physeal cartilage and ligaments, and some paediatric centres prefer it. However CT remains faster, more available, and better for bony step-off measurement and screw planning. The radiation-versus-availability trade-off is unsettled, particularly in younger patients.
State the mainstream position (CT for displaced/intra-articular patterns, ORIF for over 2 mm step), then acknowledge the nuance: the threshold is evidence-light, fragment location matters, and percutaneous techniques are a legitimate alternative in experienced hands. Examiners reward candidates who know where the evidence is soft.
MCQ Practice Points
Q: In what order does the distal tibial physis close? A: Central, Medial, Lateral (CML) - this asymmetric closure creates transitional fractures.
Q: A Tillaux fracture is which Salter-Harris type? A: Type III - involves the physis and epiphysis only.
Q: A Triplane fracture is which Salter-Harris type? A: Type IV - involves metaphysis, physis, and epiphysis.
Q: What imaging modality is essential for transitional fractures? A: CT scan - determines 2-part vs 3-part pattern and measures articular step-off.
Q: What is the threshold for operative treatment in transitional fractures? A: Greater than 2mm of articular step-off on CT.
Q: Why is growth arrest less concerning in transitional fractures? A: They occur near skeletal maturity - any growth arrest is rarely clinically significant.
Self-Assessment Quiz
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“14-year-old girl twisted her ankle playing netball. X-ray shows an anterolateral epiphyseal fragment at the distal tibia. What is your assessment and management?”
“Same patient - CT shows an anterolateral epiphyseal fragment, a posterolateral metaphyseal spike, and the medial epiphysis is attached to the metaphysis. What is this pattern and how would you treat it?”
“CT shows an anterolateral epiphyseal fragment, a SEPARATE medial epiphyseal fragment, and a posterolateral metaphyseal fragment. How does this change your approach?”
KEY FACTS
- CML physeal closure pattern
- Tillaux = SH-III
- Triplane = SH-IV
- Age 12-15 years
IMAGING
- CT is mandatory
- X-rays underestimate displacement
- Determine 2-part vs 3-part
- Measure articular step-off
TREATMENT THRESHOLD
- Greater than 2mm step = surgery
- Less than 2mm = cast with monitoring
- Weekly X-rays for first 2-3 weeks
- CT measurement is the gold standard
SURGICAL APPROACH
- Tillaux: anterolateral
- 2-part triplane: lateral
- 3-part triplane: may need medial too
- Epiphyseal screws parallel to joint
PROGNOSIS
- Excellent with anatomic reduction
- Growth arrest rarely significant
- Low arthritis risk if reduced
- Return to sport 3-4 months
KEY EVIDENCE
- 2mm threshold (Ertl 1988)
- CT changes management in 27% (Eismann 2015)
- Triplane described by Cooperman/Spiegel 1978
- Focus on articular reduction
Evidence Base
- 15 children (mean age 13 years); triplane represented 6% of 237 consecutive physeal ankle fractures
- Tomography redefined the anatomy - a medial epiphyseal/malleolar fragment plus a lateral fragment carrying posterior metaphysis
- 13 of 15 treated closed; 3 of 14 showed premature symmetrical physeal closure with under 0.5 cm shortening and no angular deformity
- 23 patients reviewed; 11 of 15 anatomically confirmed cases were 3-fragment patterns
- Plain radiographs alone did not accurately demonstrate fracture configuration
- Residual displacement of 2 mm or more after reduction was associated with a less than optimum result unless the fragment lay outside the weight-bearing zone
- 35 patients reviewed; CT required because plain films did not accurately show configuration
- Closed reduction attempted first; failure to obtain or maintain reduction was the indication for surgery
- Degenerative change at over 5 years was seen only when reduction left more than 2 mm of displacement
- 5 raters assessed 25 triplane fractures with radiographs alone then with CT
- Adding CT moved displacement across the 2 mm threshold in 39% of ratings and changed the treatment decision (non-operative to operative) in 27%
- Rapariz classification reliability improved from poor (kappa 0.17) to moderate (kappa 0.41) with CT
- Narrative review: triplane fractures are 5-10% of paediatric intra-articular ankle injuries, typically age 12-15, slightly more common in boys
- Result of asymmetric distal tibial physeal closure over ~18 months
- Non-displaced fractures cast; displaced fractures need ORIF to within 2 mm via anterolateral or anteromedial approach
- Retrospective series identifying 10 atypical triplane patterns, including an extra-articular variant with an anteromedial epiphyseal sleeve fragment
- Closed reduction and percutaneous screw fixation gave no long-term complications
- Average return to sport 5.2 months; full range of motion regained by ~13 weeks