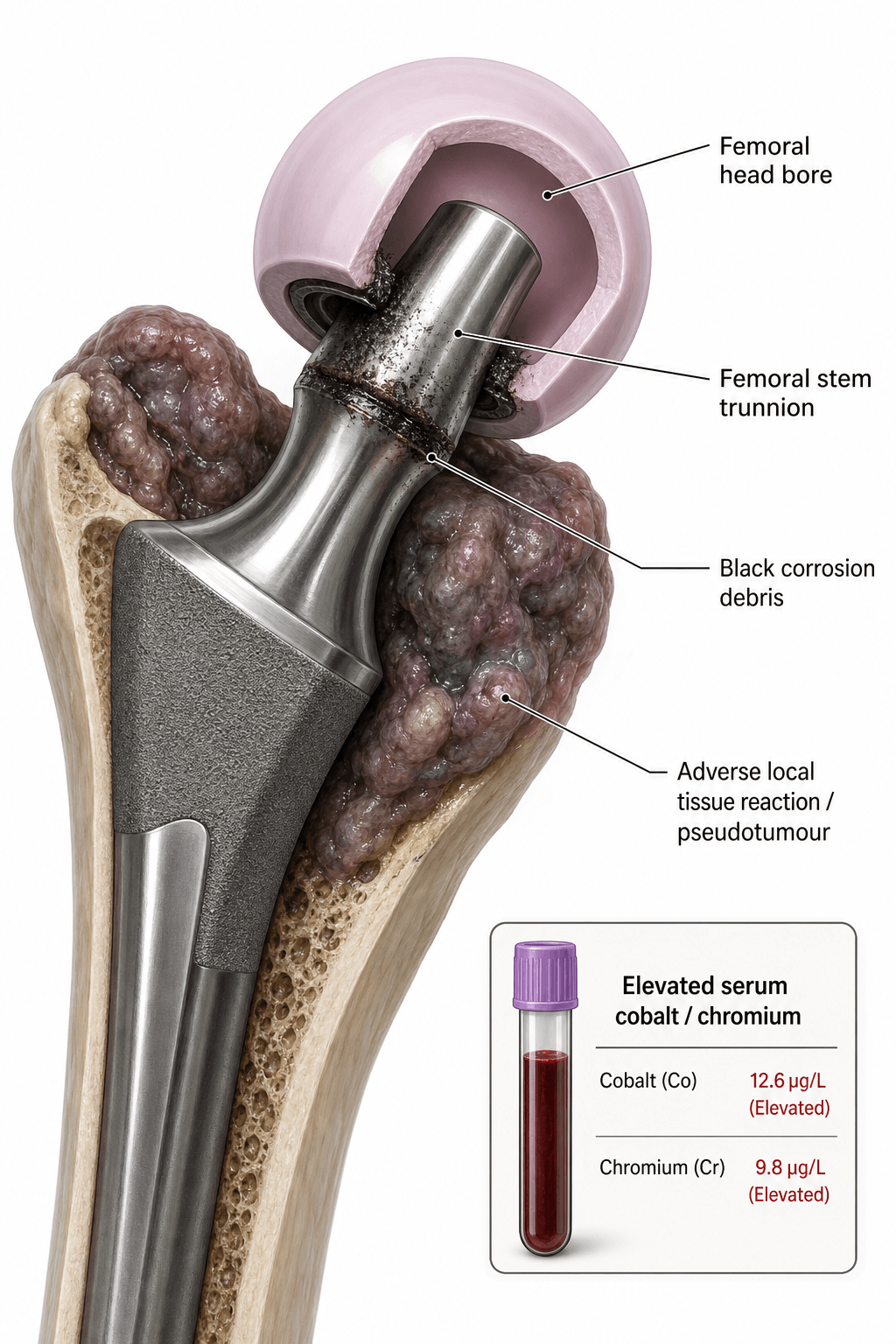
Mechanically-Assisted Crevice Corrosion at Head-Neck Junction
- Trunnionosis = mechanically-assisted crevice corrosion (MACC) at head-neck taper
- Risk factors: large heads (36mm+), high offset, long necks, Ti stems, mixed metals
- Cobalt more systemically toxic than chromium (cardiotoxicity, neurotoxicity)
- MARS MRI is investigation of choice - detects soft tissue destruction
- Revision must address soft tissue debridement AND component considerations
- “Cobalt greater than 7 ppb and Cr greater than 5 ppb are concerning thresholds
- “MoP with large CoCr head on Ti stem = highest risk combination
- “ALTR = Adverse Local Tissue Reaction (umbrella term)
- “ARMD = Adverse Reaction to Metal Debris (same entity, different name)
Understand the tribology. Fretting (micromotion) + crevice corrosion (oxygen-depleted environment) = mechanically-assisted crevice corrosion. This is the pathomechanism.
Head size is the key modifiable risk factor. Heads 36mm and larger generate greater taper moments and micromotion. Combined with Ti stems, risk is multiplicative.
Cobalt and chromium levels guide management. Co greater than 7 ppb is threshold for concern. BUT imaging (MARS MRI) determines tissue damage and surgical decision-making.
ALTR causes extensive tissue necrosis. Pseudotumors, abductor destruction, bone loss. Revision is complex - must debride all necrotic tissue for success.
- Risk Level
- Low
- Recommended Action
- Standard surveillance
- Key Point
- Small head, matched metals = low risk
- Risk Level
- High
- Recommended Action
- Annual metal ions + clinical review
- Key Point
- Large head on Ti = high risk combination
- Risk Level
- Moderate
- Recommended Action
- Annual metal ions, clinical review
- Key Point
- Bearing surface wear, not taper
- Risk Level
- Critical
- Recommended Action
- Urgent MARS MRI + revision planning
- Key Point
- High ions with symptoms = tissue damage likely
PUNCHSystemic Effects of Cobalt
Hook:Cobalt can really PUNCH you - systemic toxicity is serious!
Overview and Epidemiology
Trunnionosis refers to mechanically-assisted crevice corrosion (MACC) occurring at the modular head-neck taper junction of total hip arthroplasty, leading to metal debris release and adverse local tissue reactions (ALTR). It is distinct from bearing surface wear in metal-on-metal articulations.
- Reported in 2-4% of modular THA overall
- Higher rates with specific designs (up to 10%)
- Male patients may be at higher risk (greater activity)
- Recognition increased dramatically post-2010
- Joint registry data show elevated revision rates for certain stem-head combinations
- Modularity introduced 1980s for surgical flexibility
- Initial focus on MoM bearing surface failures
- Taper corrosion recognized as distinct entity ~2010
- MHRA alerts and recalls highlighted problem
- Now affects MoP and CoP combinations too
Risk Factors
Implant-Related Risk Factors
- Low Risk
- 28-32mm
- High Risk
- 36mm+
- Mechanism
- Larger head = greater taper moment
- Low Risk
- CoCr stem
- High Risk
- Titanium stem
- Mechanism
- Ti has inferior taper performance
- Low Risk
- Matched metals
- High Risk
- CoCr head on Ti stem
- Mechanism
- Galvanic couple accelerates corrosion
- Low Risk
- Standard
- High Risk
- Long (+5, +10)
- Mechanism
- Increased lever arm at taper
- Low Risk
- Standard
- High Risk
- High offset
- Mechanism
- Greater bending moment at taper
- Low Risk
- Manufacturer matched
- High Risk
- Mismatch or poor design
- Mechanism
- Taper angle/roughness mismatch
The worst combination: Large CoCr head (36mm+) on a high-offset titanium stem with extended neck.
Titanium stem + Large CoCr head + High offset = Maximum risk. National joint registry data (AOANJRR, NJR, AJRR) confirm these combinations have the highest revision rates for ALTR. Avoid this combination or implement surveillance protocols.
THOLTRisk Factors for Taper Corrosion
Hook:A THOLT of caution with large heads on titanium - the taper takes the toll!
Pathophysiology
Fretting disrupts the protective oxide layer → Crevice environment prevents repassivation → Metal ions released → Local tissue toxicity (ALTR) → Possible systemic toxicity. Understanding this cascade is essential.
Morse Taper Fundamentals
- Morse taper creates interference fit via cold welding
- Taper angle varies between manufacturers (5°44' common)
- Taper length affects contact area and stability
- Impaction force critical for initial fixation
- Axial loads from body weight
- Torsional loads from gait (internal/external rotation)
- Bending moments from offset/neck length
- Larger heads amplify moment arm at taper
Moment = Force × Distance. Larger heads increase the lever arm from hip center to taper junction. This amplifies bending moments and torsional stresses at the taper, increasing fretting micromotion. A 36mm head generates approximately 30% more moment than a 28mm head.
Clinical Presentation
- Groin pain (may be insidious onset)
- Hip pain with activity
- Clicking, squeaking, or grinding
- Swelling (pseudotumor)
- Progressive weakness (abductor destruction)
- Sense of instability
- Recurrent dislocation
- Fatigue and malaise
- Cognitive changes (memory, concentration)
- Peripheral neuropathy
- Visual or hearing changes
- Palpitations or dyspnea (cardiomyopathy)
- Hypothyroidism symptoms
- Depression
Clinical Stages
Progression of Trunnionosis
Metal ion release begins. Patient asymptomatic. May only be detected on surveillance bloods. Tissue changes minimal.
Groin or hip pain develops. May be mistaken for other causes. Early soft tissue changes on MRI. Metal ions typically elevated.
Pseudotumor formation. Abductor destruction. Bone loss possible. Significant functional impairment. High metal ions.
Cobaltism develops. Cardiac, neurological, thyroid manifestations. May be irreversible. Urgent revision required.
Systemic cobalt toxicity requires urgent action. Signs include: unexplained cardiomyopathy, peripheral neuropathy, visual/hearing loss, cognitive decline, hypothyroidism. Cobalt levels often greater than 20 ppb. Can be fatal if not addressed. Echo and cardiology referral essential.
Investigations
Serum Metal Ion Testing
- Normal
- Less than 1 ppb
- Concerning
- Greater than 4 ppb
- Action Threshold
- Greater than 7 ppb = imaging required
- Normal
- Less than 1 ppb
- Concerning
- Greater than 4 ppb
- Action Threshold
- Greater than 5 ppb = imaging required
- Normal
- Approximately 1:1
- Concerning
- Greater than 2:1
- Action Threshold
- High ratio suggests taper source
- Co:Cr ratio greater than 2:1 suggests taper corrosion (rather than bearing wear)
- Levels can fluctuate - trend is important
- Some patients develop ALTR with low ion levels (hypersensitivity)
- Whole blood samples required (not serum alone)
- Co or Cr greater than 7 ppb = concern, requires imaging
- Annual surveillance for at-risk implants
1. Serum metal ions (Co and Cr) → 2. Plain radiographs → 3. MARS MRI if ions elevated or symptoms persist → 4. Aspiration to rule out infection before surgery. Do not skip the aspiration - occult infection can coexist.
Differential Diagnosis
- Key Features
- Elevated metal ions, pseudotumor on MRI
- Distinguishing Investigation
- Metal ions + MARS MRI
- Key Features
- Fever, elevated CRP/ESR, positive cultures
- Distinguishing Investigation
- Aspiration, WBC count, culture
- Key Features
- Start-up pain, progressive, radiolucent lines
- Distinguishing Investigation
- Serial X-rays, bone scan
- Key Features
- Recurrent dislocation, sense of giving way
- Distinguishing Investigation
- Clinical exam, X-ray, CT for version
- Key Features
- Acute pain after trauma, may be subtle
- Distinguishing Investigation
- X-ray, CT if needed
- Key Features
- Back pain, radicular symptoms
- Distinguishing Investigation
- Spine imaging, selective injection
- Key Features
- Anterior groin pain, worse with flexion
- Distinguishing Investigation
- CT (cup position), lidocaine injection
Must distinguish ALTR from infection before revision. Both can present with pain and elevated inflammatory markers. Aspiration is MANDATORY. ALTR fluid is typically dark/metallic but sterile. Infection requires completely different management.
Management
Non-Operative Surveillance
- Asymptomatic patient with at-risk implant
- Low-grade metal ion elevation (Co less than 7 ppb)
- No significant ALTR on MARS MRI
- Well-fixed, well-positioned components
- Annual clinical review
- Annual metal ions (Co and Cr)
- MARS MRI every 1-2 years if ions elevated
- Patient education on warning symptoms
- Symptomatic progression
- Rising metal ion trend
- ALTR progression on MRI
- Systemic symptoms develop
The single most important factor for revision success is complete debridement of necrotic tissue. Retained necrotic/reactive tissue leads to persistent inflammation, poor healing, and high complication rates. Be aggressive with debridement.
Surgical Technique Considerations
Surgical Approach
- Posterior approach with extended capsulotomy
- May need trochanteric osteotomy for access
- Must visualize extent of pseudotumor
- Direct lateral may limit access posteriorly
- Identify and protect sciatic nerve (often displaced by pseudotumor)
- Evacuate pseudotumor contents carefully
- Complete capsulectomy and synovectomy
- Debride all necrotic tissue back to bleeding margins
Ti sleeve/adapter devices allow retention of a well-fixed stem with damaged trunnion. The sleeve covers the corroded taper and provides a new surface for head impaction. This avoids stem revision morbidity in selected cases. Check manufacturer compatibility.
Complications
Complications of ALTR and Revision Surgery
- Rate
- 10-25%
- Risk Factors
- Abductor loss, revision surgery
- Management
- Constrained liner, bracing, re-revision
- Rate
- 5-10%
- Risk Factors
- Necrotic tissue, prolonged surgery
- Management
- Debridement, antibiotics, staged revision
- Rate
- 2-5%
- Risk Factors
- Scarring, pseudotumor displacement
- Management
- Careful dissection, may recover
- Rate
- 15-30%
- Risk Factors
- Incomplete debridement, tissue damage
- Management
- May need re-revision
- Rate
- 20-40%
- Risk Factors
- Pre-existing damage from ALTR
- Management
- Gait aids, reconstruction options limited
- Rate
- 2-5%
- Risk Factors
- Bone loss, osteolysis
- Management
- May need additional fixation
Revision for ALTR has higher complication rates than routine revision THA. Dislocation rates of 10-25% reflect abductor deficiency. Counsel patients appropriately. May require constrained components, brace, or assistive devices long-term.
Outcomes and Prognosis
Prognostic Factors
- Early diagnosis before extensive tissue damage
- Intact or recoverable abductors
- Good bone stock
- Low metal ion levels
- Complete surgical debridement achieved
- Delayed diagnosis with extensive destruction
- Abductor loss/atrophy
- Significant bone loss
- Very high metal ion levels (cobaltism)
- Systemic toxicity (cardiac, neurological)
- Multiple prior revisions
Re-revision is common after ALTR revision - registry data (NJR) show 13.5% re-revision at a mean of 1.2 years and only ~84% implant survival at 4 years, worse than for many other revision indications. Dislocation and infection are the leading reasons for re-revision. Early diagnosis and meticulous, complete revision optimise outcomes.
Guidelines, Registries & Global Practice
Global Epidemiology
- Trunnionosis-related ALTR is reported across all major modular THA designs and bearing couples, including conventional metal-on-polyethylene, not only MoM
- True incidence is uncertain because many cases are subclinical; symptomatic revision for ALTR remains a small but rising proportion of all revisions
- Large-head MoM THA (36mm and over) and large-diameter resurfacings concentrated the early failures that drew attention to the modular junction
- Recognition surged after 2010 following retrieval studies and regulatory alerts; conventional MoP taper corrosion is now an established differential for the painful THA worldwide
Side-by-Side Guidance
- Region
- UK
- Key Recommendation
- Whole-blood Co/Cr; 7 micrograms/L (≈7 ppb) trigger for cross-sectional imaging; lifelong follow-up for large-head MoM
- Region
- USA
- Key Recommendation
- Symptom-led metal-ion testing and MARS MRI for symptomatic MoM hips; no single mandated ion threshold
- Region
- USA
- Key Recommendation
- Differential cobalt-over-chromium elevation points to taper source; ceramic-head exchange at revision
- Region
- Europe
- Key Recommendation
- Risk-stratified surveillance using implant type, symptoms, ion trend and imaging
The widely quoted 7 micrograms/L (≈7 ppb) trigger derives from UK MHRA guidance and large-head MoM retrieval data. US regulators favour a symptom-led approach without a single fixed cut-off. The unifying principle globally is the same: ion levels SCREEN, imaging (MARS MRI) and symptoms DECIDE. A differential cobalt-greater-than-chromium pattern specifically localises the problem to the taper rather than the bearing.
Registry Evidence
- MoM bearings carry the highest revision rate of any bearing couple across the AOANJRR (Australia), NJR (UK) and AJRR (US)
- Large-head MoM THA performs worse than resurfacing, and ceramic-on-polyethylene / ceramic-on-ceramic show the lowest revision rates
- Registries flagged specific titanium-stem plus large-CoCr-head combinations for surveillance and informed device withdrawals
- Registry data underpins the global shift toward smaller ceramic heads on polyethylene at primary and revision surgery
High- vs Limited-Resource Practice
- Surveillance / Diagnosis
- Routine whole-blood Co/Cr, MARS MRI, registry-linked recall
- Practical Reality
- Structured surveillance programmes; ceramic heads readily available
- Surveillance / Diagnosis
- Clinical review and plain radiographs; ion assays and MARS MRI may be unavailable
- Practical Reality
- Reliance on symptoms and effusion/mass on ultrasound; ceramic/sleeve supply may be constrained
Patients with recalled or high-risk implants (large-head MoM THA and certain conventional THA stem-head combinations) should be identified, notified and enrolled in surveillance. Maintaining an accurate implant register for every patient is the foundation of safe long-term follow-up, whatever the healthcare setting.
Controversies & Areas of Uncertainty
The 7 micrograms/L trigger is pragmatic, not absolute. Some patients develop florid ALTR at near-normal ions (hypersensitivity), while others tolerate very high levels. The trend and the Co:Cr ratio matter more than any single number.
When to revise an asymptomatic patient with a rising ion level or enlarging pseudotumour is unresolved. Prophylactic revision must be balanced against the high complication rate of ALTR revision surgery.
Retaining a well-fixed stem with a ceramic head and titanium sleeve avoids morbidity but leaves the original (damaged) trunnion in situ. Long-term durability of the sleeve construct versus full stem revision remains debated.
Evidence for chelation therapy in arthroprosthetic cobaltism is weak and largely anecdotal. Source control by revision to cobalt-free implants is the mainstay; reversibility of cardiac and neurological injury is variable.
Be ready to argue both sides: "Would you revise an asymptomatic patient with cobalt of 12 ppb?" There is no single right answer. Demonstrate a structured, individualised approach integrating symptoms, ion trend, imaging (lesion type), abductor status, patient factors and the morbidity of revision.
The Neck-Body (Dual-Taper) Junction: A Second Modular Corrosion Site
The management section notes that revision may require a "modular neck exchange if available" - a reminder that some femoral stems carry a second modular interface. In a dual-taper (modular-neck) stem, the surgeon can adjust version, offset and length independently of stem fixation by selecting a separate modular neck; this adds a neck-body (neck-stem) junction distinct from the head-neck taper. That extra junction sits closer to the fixed stem, carries large cantilever bending moments and is a corrosion site in its own right - the mechanism behind the withdrawal of several dual-taper designs (for example the Rejuvenate and ABG II modular-neck stems).
- Classic pairing is a cobalt-chromium modular neck on a titanium-alloy stem body - a mixed-alloy (galvanic) couple
- Long lever arm and cyclic bending drive fretting that disrupts passivation, then crevice corrosion in the oxygen-depleted junction (the same MACC process as the head-neck taper)
- Because it is proximal and load-bearing, failure can occur early (within the first post-operative year)
- Rarely the modular neck can fatigue-fracture, not just corrode
- Presentation mirrors head-neck trunnionosis: new groin/thigh pain, effusion, pseudotumour, ALTR on MARS MRI
- Metal-ion pattern is again cobalt-dominant, but serum titanium may also rise from the Ti stem side of the couple
- A simple ceramic-head-plus-sleeve swap does NOT treat this junction - source control usually means exchanging the modular neck and often revising the stem
- Always ask which taper is the culprit before planning: head-neck versus neck-body changes the whole operation
Cooper - ALTR from Corrosion at the Modular Neck-Body Junction (Dual-Taper Stems)
- 12 hips (11 patients) with ALTR from corrosion at the modular neck-body junction of a dual-taper stem
- All had a titanium-alloy stem with a cobalt-chromium modular neck; new-onset pain at a mean of 7.9 months
- Serum cobalt (mean 6.0 ng/mL) was elevated more than chromium (0.6) or titanium (3.4)
- MARS MRI showed adverse reactions; SEM confirmed fretting and crevice corrosion at the neck-body interface
When the examiner hands you a modular-neck stem, remember there are two modular junctions. A cobalt-over-chromium elevation still localises the problem to a taper, but you must ask which one. Neck-body junction corrosion is not salvaged by a ceramic head on a titanium sleeve - it typically needs exchange of the modular neck and frequently full stem revision. A concurrent rise in serum titanium is a clue that the neck-body (Ti-side) junction, not just the head-neck taper, is involved.
FCGCorrosion Mechanisms
Hook:FCG - Fretting, Crevice, Galvanic - the triple threat of taper destruction!
Grading Taper Damage: the Goldberg Retrieval Score
The intraoperative decision that runs through this topic - "moderate corrosion, keep the stem and use a titanium sleeve" versus "severe corrosion, revise the stem" - rests on an objective way to grade the taper. The reference tool is the Goldberg semiquantitative fretting-and-corrosion score, a four-point visual scale applied to each taper surface (the femoral head bore and the stem trunnion), read by quadrant:
- Appearance
- Bright machined surface, no fretting scars or corrosion
- Revision Implication
- Trunnion salvageable; ceramic head on titanium sleeve acceptable
- Appearance
- Isolated fretting scars or single small patch of discolouration
- Revision Implication
- Usually salvageable with a clean sleeve construct
- Appearance
- Fretting/corrosion over up to roughly a third of the surface, visible pits or black debris
- Revision Implication
- Higher-risk taper; weigh sleeve against stem revision
- Appearance
- Extensive pitting, etched/matte surface, heavy black corrosion product
- Revision Implication
- Damaged beyond reliable reuse; favour stem revision
The landmark retrieval study defined this scoring system and produced the mechanistic evidence behind the risk factors in this topic: mixed-alloy couples corrode more than matched couples, heads tend to corrode more than necks, and neck flexural rigidity and implantation time predict damage - the mechanical basis for the head-size, offset and titanium-stem warnings elsewhere on this page.
Goldberg - Multicentre Retrieval Study Defining Taper Corrosion Scoring
- 231 retrieved modular hip implants scored for fretting and corrosion by taper quadrant (the 4-point Goldberg scale)
- Moderate-to-severe head corrosion in 42% of mixed-alloy versus 28% of similar-alloy couples
- Heads corroded more than necks; implantation time and neck flexural rigidity predicted damage
- Findings attributed in-vivo taper damage to mechanically-assisted crevice corrosion (MACC)
Grade the trunnion before you commit. A Goldberg grade 1-2 (bright or minimally scarred) trunnion on a well-fixed stem can accept a new ceramic head on a titanium adapter sleeve. A grade 3-4 trunnion - pitted, etched, coated in black corrosion product - or any loose stem should push you toward stem revision, because a ceramic head impacted onto a damaged taper risks poor seating and ceramic fracture. The score also explains prevention: avoid mixed CoCr-on-titanium couples and very slim necks.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old man is 5 years post primary THA with a 36mm cobalt-chrome head on a titanium uncemented stem. He is currently asymptomatic but was referred for surveillance due to implant concerns. How would you assess and counsel this patient?”
“A 62-year-old woman presents with progressive right hip pain and weakness 7 years after THA. She has a 38mm metal-on-polyethylene bearing on a titanium stem. Her cobalt is 18 ppb and chromium is 6 ppb. MARS MRI shows a large posterolateral pseudotumor with abductor muscle atrophy. How would you manage this patient?”
“A 55-year-old man presents with fatigue, hearing loss, and peripheral neuropathy. He had bilateral THA 6 years ago (large head MoM). His cobalt level is 85 ppb. MARS MRI shows bilateral pseudotumors. His cardiologist has diagnosed new cardiomyopathy. How would you approach this complex case?”
Definition
- Mechanically-assisted crevice corrosion (MACC) at head-neck taper
- ALTR = Adverse Local Tissue Reaction (umbrella term)
- ARMD = Adverse Reaction to Metal Debris (same entity)
- ALVAL = histological pattern of metal hypersensitivity
Risk Factors (THOLT)
- Titanium stem (Ti has worse taper performance)
- Head size large (36mm+ increases taper moment)
- Offset increased / Long neck
- Lateral offset designs
- Taper mismatch / Mixed metals (CoCr on Ti)
Corrosion Mechanisms
- Fretting: micromotion disrupts oxide layer
- Crevice: oxygen-depleted environment accelerates corrosion
- Galvanic: dissimilar metals create electrochemical gradient
- All three combine in MACC
Metal Ion Thresholds
- Cobalt greater than 7 ppb = concern, imaging required
- Chromium greater than 5 ppb = concern
- Co:Cr ratio greater than 2:1 suggests taper source
- Very high levels (greater than 20 ppb) = check for systemic toxicity
MARS MRI Findings
- Pseudotumor (cystic or solid)
- Muscle atrophy (abductors)
- Fluid collections
- Bone involvement/osteolysis
Revision Principles
- Complete debridement of necrotic tissue (most important)
- Ceramic head to eliminate metal ions
- Smaller head size (32mm)
- Ti adapter sleeve if stem well-fixed but taper damaged
- Consider constrained liner if abductors deficient
Systemic Cobalt Toxicity (PUNCH)
- Peripheral neuropathy
- Unexplained fatigue
- Neuro-ocular toxicity (vision/hearing)
- Cardiomyopathy (can be fatal)
- Hypothyroidism
Evidence Base and Key Studies
Cooper / Della Valle - Head-Neck Taper Corrosion Causing ALTR in MoP THA (Landmark)
- 10 metal-on-polyethylene THAs revised for corrosion at the modular head-neck taper
- All presented with pain/swelling; 2 with recurrent instability from abductor destruction
- Serum cobalt characteristically elevated more than chromium (differential Co greater than Cr)
- Treated with debridement plus ceramic head and titanium sleeve; cobalt fell to mean 1.61 ng/mL
Langton - Trunnion-Taper Failure in Large-Diameter MoM THR
- ASR total hip replacement failed at 48.8% at 6 years (vs 25% for the resurfacing)
- 26.1% of patients had serum cobalt greater than 7 micrograms/L
- Some THRs had low articular wear but marked damage at the trunnion-taper interface
- Wear at the modular junction is an important driver of adverse tissue reactions
Langton - Taper Junction Mechanics: Lever Arm Drives Failure
- Coordinate-measured taper material loss in 126 failed large-diameter MoM prostheses
- Primary driver of taper failure is the increased lever arm at the junction
- Varus stems, laterally engaging taper systems and larger head diameters all contributed
- Quantified the mechanical basis for the head-size and offset risk relationship
Plummer / Della Valle - Diagnosis and Management of MoP Taper ALTR
- 27 MoP hips revised for head-neck corrosion ALTR; mean cobalt 11.2 ppb, chromium 2.2 ppb
- Cobalt elevated above chromium and cobalt greater than 1 ppb supports the diagnosis
- Ceramic head plus titanium sleeve used in 23/27; ALTR recurred in 1 of 4 NOT given a ceramic head
- Retaining a well-fixed stem with modular ceramic exchange resolved symptoms and lowered metal levels
Hart - Pseudotumour Prevalence on MARS MRI
- Case-control study of MARS MRI in painful vs well-functioning MoM hips
- Pseudotumours present in 59% overall and were common even in well-functioning hips
- Prevalence in painful (57%) vs control (61%) hips was NOT significantly different
- Cystic pseudotumour alone does not mandate revision; correlate with symptoms and ions
Matharu - Outcomes of Revision for ARMD (NJR England and Wales)
- 185 non-MoM hips revised for ARMD from the National Joint Registry
- Re-revision in 13.5% at mean 1.2 years; 4-year implant survival 83.8%
- Commonest re-revision indications: infection, dislocation/subluxation, aseptic loosening
- Selective component revision and multiple revision indications predicted re-revision
Bridges / Tower - Systemic Arthroprosthetic Cobaltism (Neurotoxicity)
- FDG-PET in screened arthroprosthetic patients showed regional cerebral hypometabolism
- MoM and MoP joints produced similar patterns of toxicity
- 8 of 15 patients showed improved brain metabolism after revision to cobalt-free implants
- Neurotoxicity occurred at relatively low blood cobalt levels in some patients
AOANJRR / NJR / AJRR - Registry Evidence on MoM and Modular THA
- Metal-on-metal bearings carry the highest revision rate of all bearing couples
- Large-head MoM THA performs worse than hip resurfacing
- Ceramic-on-polyethylene and ceramic-on-ceramic show the lowest revision rates
- Specific titanium-stem / large-CoCr-head combinations flagged for surveillance