
Cases, discussion & exam tips.
Read an image case and commit to your call, debate management, swap exam-day experiences, and share what worked when you studied — a friendly place to pressure-test your reasoning before the exam.
- Threads
- 63
- Comments
- 0
threads posted
replies shared
Discussions
Anatomy revision using both prosection and MRI correlation
For each joint or region I spend one session with a prosection and the next with the corresponding MRI slices of the same specimen. Labelling structures on both modalities in the same sitting improved my ability to interpret cross-sectional imaging in the clinical exam more than either method alone.
Peer teaching on controversial topics only
Instead of teaching standard topics, I prepare 10-minute micro-teaches on areas where evidence is conflicting (e.g., partial rotator cuff repair versus debridement). Teaching forces me to articulate both sides clearly and identify the exact point of equipoise, which directly translates to viva performance.

Periprosthetic distal femur fracture after TKR: fixation or revision?
I'm increasingly seeing periprosthetic distal femur fractures around well-fixed TKRs managed with locked plating (or retrograde nailing) rather than revision to a distal femoral replacement, especially in younger patients. Registry data suggest reoperation rates for fixation are non-trivial, but so are the complications of mega-prosthetic revision. How are people balancing these — is there an age, bone-stock or activity-level threshold where you reflexively choose one over the other?
Achilles tendinopathy: have we moved beyond eccentric loading?
Heavy slow resistance training and progressive tendon loading protocols have been gaining ground over the classic Alfredson eccentric programme, with several RCTs suggesting comparable or superior outcomes at mid-term follow-up. PRP injections continue to polarise opinions despite multiple trials. For a recreational runner with mid-substance tendinopathy of 4 months failing conservative management, what's your actual algorithm?
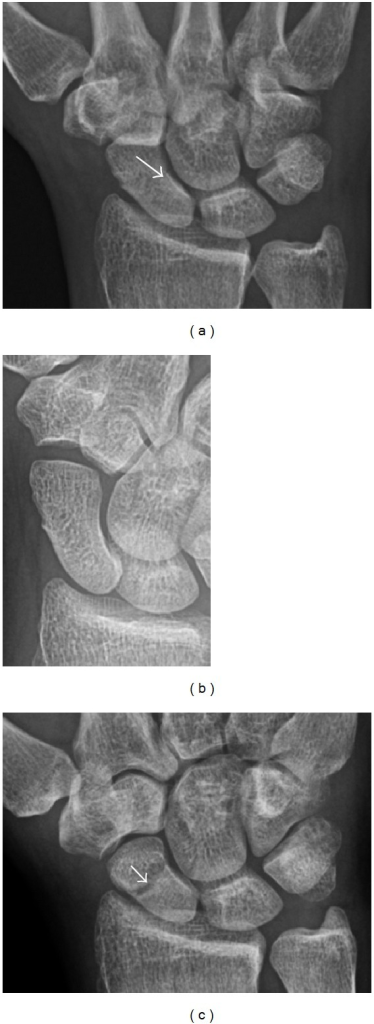
Undisplaced scaphoid waist fracture: cast or percutaneous screw?
The SWIFFT trial (Dias et al, Lancet 2020) shook up practice here, showing no clinically meaningful difference between cast immobilisation and early surgical fixation for minimally displaced scaphoid waist fractures at 12 months, with more complications in the surgical arm. Yet many surgeons still offer early fixation, arguing return-to-work time and grip-strength recovery favour surgery. How has your practice actually changed post-SWIFFT?
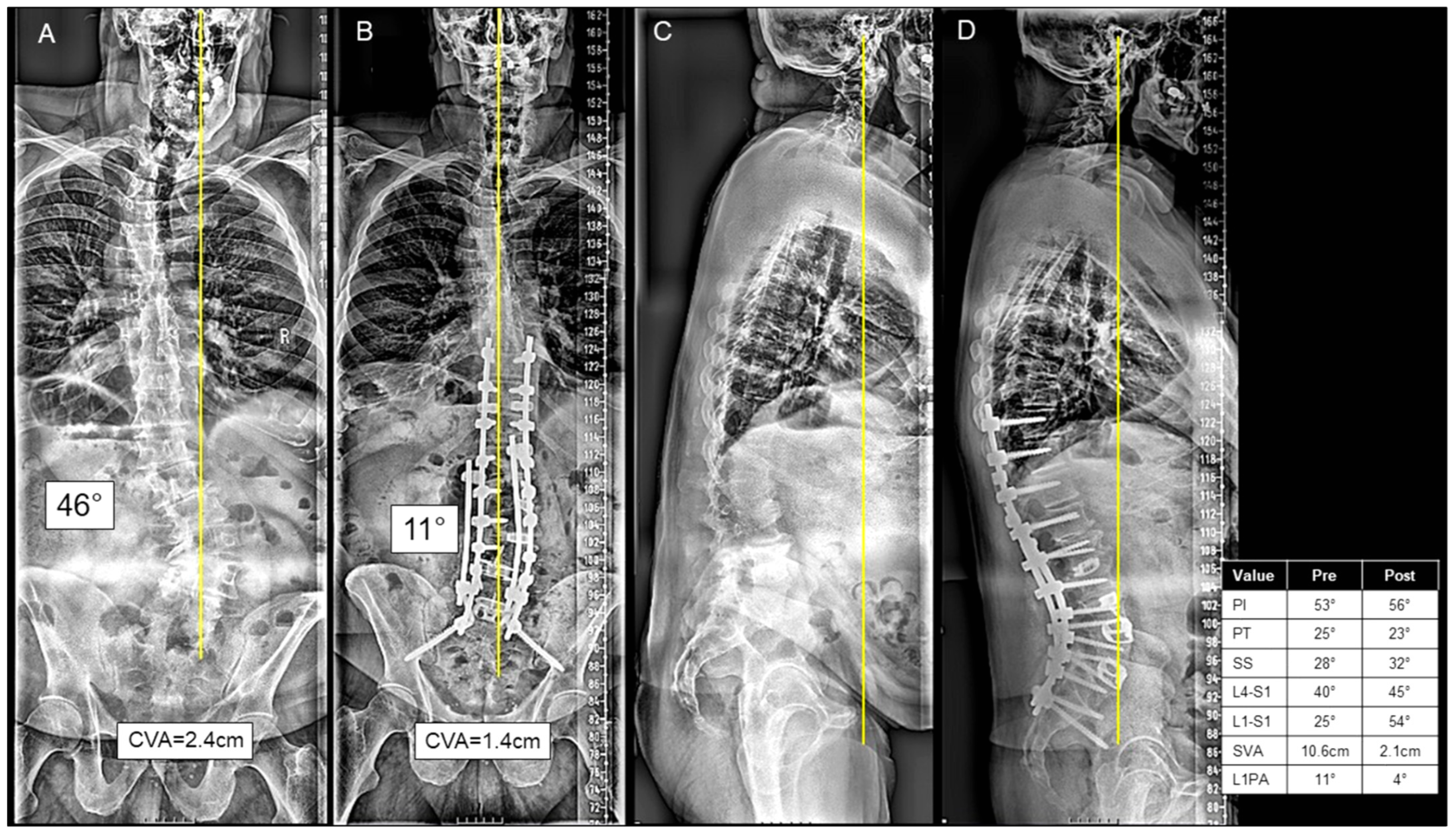
Adult spinal deformity: which alignment targets still matter?
The SRS-Schwab classification gave us sagittal modifiers (PI-LL mismatch, SVA, PT) that drove surgical goals for years, but more recent work suggests rigid adherence to all three may lead to unnecessary long fusions in older patients. For a 68-year-old with degenerative scoliosis and PI-LL mismatch but acceptable SVA, where are people drawing the line — full correction, limited anterior column realignment, or just neural decompression?
Single-row vs double-row rotator cuff repair: does it still matter?
Biomechanical studies clearly favour double-row constructs for load-to-failure and footprint restoration, but clinical outcome data at 2-5 years has been remarkably equivocal across a number of RCTs. Some argue the re-tear gap only matters in large and massive tears. For a U-shaped supraspinatus tear of moderate size in a 55-year-old labourer, are people still reaching for double-row or has the pendulum swung?
Flexible nails vs external fixation for paediatric femoral shaft fractures in children over 11
TENS nailing works brilliantly for school-age children, but once you hit the early teen years with heavier body weight and longer lever arms, the redisplacement and malunion rates start creeping up. Some centres advocate for submuscular plating or even temporary external fixation in this grey zone. For a 13-year-old at 65 kg with a mid-diaphyseal transverse fracture, what's your go-to and what sways the decision?

Biopsy tract contamination in bone tumours: how paranoid should we be?
Most musculoskeletal oncology guidelines emphasise longitudinal incisions and avoiding contamination planes during biopsy, but I've seen cases where meticulous technique wasn't possible (prior unplanned biopsy at another centre) and the patient still did well after wide excision including the tract. Tumour board discussions often become quite heated about resecting versus observing a biopsy tract that may or may not harbour microscopic disease. How aggressively do people actually manage this in practice?
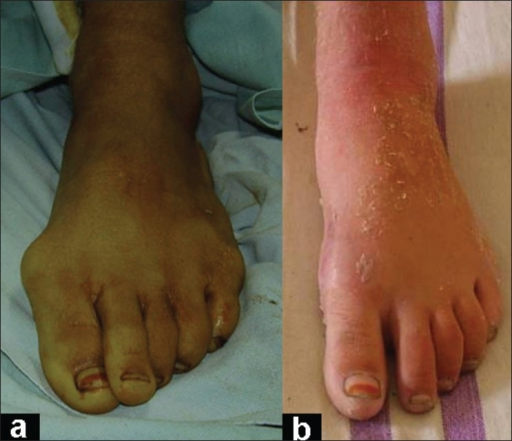
Scarf vs Lapidus for moderate hallux valgus: the DMAA debate
The Lapidus procedure has seen a resurgence for hallux valgus, offering first TMTJ fusion and powerful correction at the apex of the deformity. But for an elevated DMAA some argue a distal or biplanar osteotomy addresses the articular angle more directly, while comparative data show higher non-union rates and longer recovery for Lapidus than for a Scarf osteotomy. For a 45-year-old woman with an intermetatarsal angle of 14 degrees and a moderately elevated DMAA, are you fusing or still osteotomising?

Cervical myelopathy from disc herniation: when is surgery unavoidable?
The AOSpine CSM study and subsequent analyses have shown that patients with mild myelopathy can remain stable for years with conservative management, while surgery offers faster recovery of function. But shared decision-making with patients is genuinely difficult when symptoms are intermittent — many are hesitant about an anterior cervical discectomy and fusion in their 50s. How are people counselling these patients, and are there specific clinical or radiological red flags that tip you firmly toward surgical recommendation?
Hamstring vs bone-patellar tendon-bone for primary ACL reconstruction in young athletes
BTB grafts have the longest track record and registry data consistently shows lower re-rupture rates, but the donor-site morbidity (anterior knee pain, kneeling difficulty) remains a real concern, particularly for athletes in sports requiring kneeling. Hamstring grafts have evolved with newer fixation devices and quadruple-bundle techniques narrowing the gap. For an 18-year-old footballer, what graft are you selecting and how much does sport-specific demand drive that choice?