
Cases, discussion & exam tips.
Read an image case and commit to your call, debate management, swap exam-day experiences, and share what worked when you studied — a friendly place to pressure-test your reasoning before the exam.
- Threads
- 63
- Comments
- 0
threads posted
replies shared

Child with deep leg pain — what is this lesion?
What's your diagnosis? Reveal the casetap
A child presents with several weeks of deep distal leg pain, worse at night and eased by anti-inflammatories. This is the radiograph. What is your differential and next step?
Image cases
 Image case
Image caseThree ankle films, three fibula fractures — the classification?
These three ankle radiographs (A, B, C) each show a fibular fracture at a different level. What classification system does this illustrate, and why does the level of the fibular fracture matter for ankle stability?
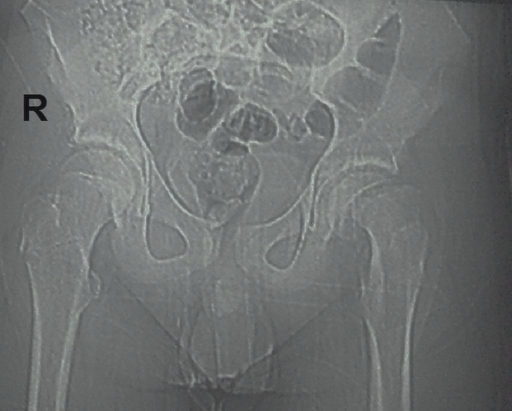 Image case
Image caseAdolescent with hip and knee pain — what's the call?
An overweight 12-year-old has a few weeks of hip and referred knee pain with a limp, and now stands with the leg slightly externally rotated. This is the AP pelvis. What is the diagnosis, which view best confirms it, and what is the immediate management?
Discussions
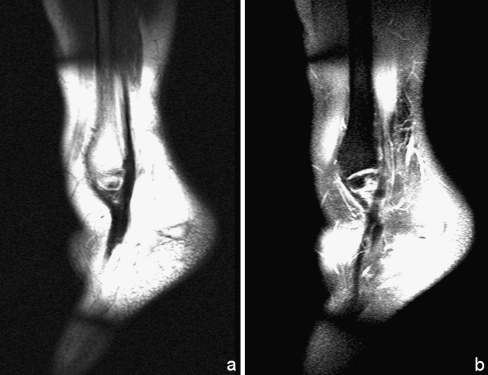
Flexor Tendon Lacerations
hello the rehab protocol doesn't coincide with other literature. as i have it its active extension and passive flexion please check it and confirm
Knee Biomechanics
physical therapy

Proximal humerus fractures in elderly patients: fixation, hemiarthroplasty or reverse TSA?
Recent registry data and RCTs show comparable functional scores between reverse TSA and fixation in selected patients over 70, but with different complication profiles including infection and tuberosity healing. Non-operative management remains viable for low-demand individuals. What factors currently guide your choice between these three options in displaced three- and four-part fractures?
Degenerative lumbar spondylolisthesis with stenosis: decompression alone or with fusion?
Multiple RCTs and meta-analyses indicate similar leg pain relief with decompression alone versus instrumented fusion, yet reoperation rates and sagittal balance concerns persist in certain cohorts. The role of patient-reported instability symptoms continues to divide opinion. Which patient characteristics make you add fusion in your practice?
Chronic lateral ankle instability: anatomic repair or graft reconstruction?
Long-term cohort studies suggest anatomic repair (Broström-type) provides excellent stability in most cases, while reconstruction with tendon graft is reserved for revision or poor tissue quality. Recent comparisons highlight differences in proprioception recovery and return to sport timing. How do you decide between these approaches in high-level athletes versus recreational patients?
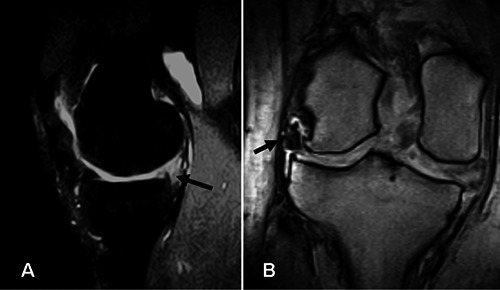
Posterior meniscal root tears: repair indications and technique selection
Biomechanical and clinical series demonstrate that root repair can slow osteoarthritis progression compared with meniscectomy, particularly in younger patients with minimal chondral damage. Suture anchor versus transtibial tunnel techniques show comparable healing rates on second-look arthroscopy. What imaging and patient factors currently lead you to attempt repair versus debridement?
Total knee arthroplasty alignment: mechanical, kinematic or functional?
Landmark RCTs and gait analysis studies have not demonstrated consistent superiority of kinematic over mechanical alignment for patient satisfaction or implant survival. Functional alignment using robotics or navigation is gaining traction but lacks long-term data. Which alignment philosophy do you default to and why?
Moderate slipped capital femoral epiphysis: in-situ pinning or corrective osteotomy?
Long-term follow-up from paediatric registries shows excellent outcomes with in-situ pinning for mild-moderate slips, while corrective osteotomy carries higher avascular necrosis risk. The timing of intervention and slip severity thresholds remain debated. At what slip angle do you consider osteotomy in your unit?
Campanacci grade 2 giant cell tumour around the knee: extended curettage or en-bloc resection?
Multicentre series report low recurrence with aggressive curettage plus phenol or cryotherapy, yet some centres favour resection for lesions with soft-tissue extension or joint involvement. Denosumab use has altered the surgical landscape but introduces its own complications. What is your current threshold for choosing resection over curettage?
Displaced intra-articular distal radius fractures in young adults: volar plating or alternative fixation?
RCTs comparing volar locking plates with dorsal plating or external fixation show similar articular reduction but differing complication rates including tendon irritation. Fragment-specific fixation and arthroscopic assistance are increasingly discussed. Which fracture patterns make you choose something other than standard volar plating?

Femoroacetabular impingement with labral tear: arthroscopic repair versus reconstruction
Prospective cohorts indicate labral repair preserves function better than debridement, while reconstruction is considered for irreparable tissue. Recent evidence questions the benefit of routine capsular closure. How do you decide between repair and reconstruction in borderline dysplasia or revision cases?

Atrophic non-union: when do you add biologics or bone graft substitutes?
Basic science and clinical studies support the use of BMPs or mesenchymal stem cells in selected atrophic non-unions, yet cost-effectiveness and consistent healing rates remain uncertain outside specific indications. Smoking cessation and mechanical stability are still foundational. Which non-union characteristics prompt you to add biological augmentation?