Anterior / Brachialis-Splitting | Proximal-to-Distal-Third Shaft | Workhorse for Anterior Plating & MIPO
- Use and versatility: the anterolateral or anterior approach is the workhorse for the proximal-third and middle-third humeral shaft and extends distally via a brachialis split. It is the preferred corridor for anterior plating and anterior MIPO, and it spares the radial nerve in the spiral groove (which the posterior approach exposes directly).
- Internervous plane, proximal versus distal: proximally the plane is the deltopectoral interval (deltoid equals axillary nerve; pectoralis major equals medial and lateral pectoral nerves). Distally the brachialis is split in line with its fibres — there is no true internervous interval within brachialis, but the split is safe because the lateral part is radial-innervated and the medial part musculocutaneous-innervated (dual innervation, Leonello 2007), so each half keeps its nerve supply.
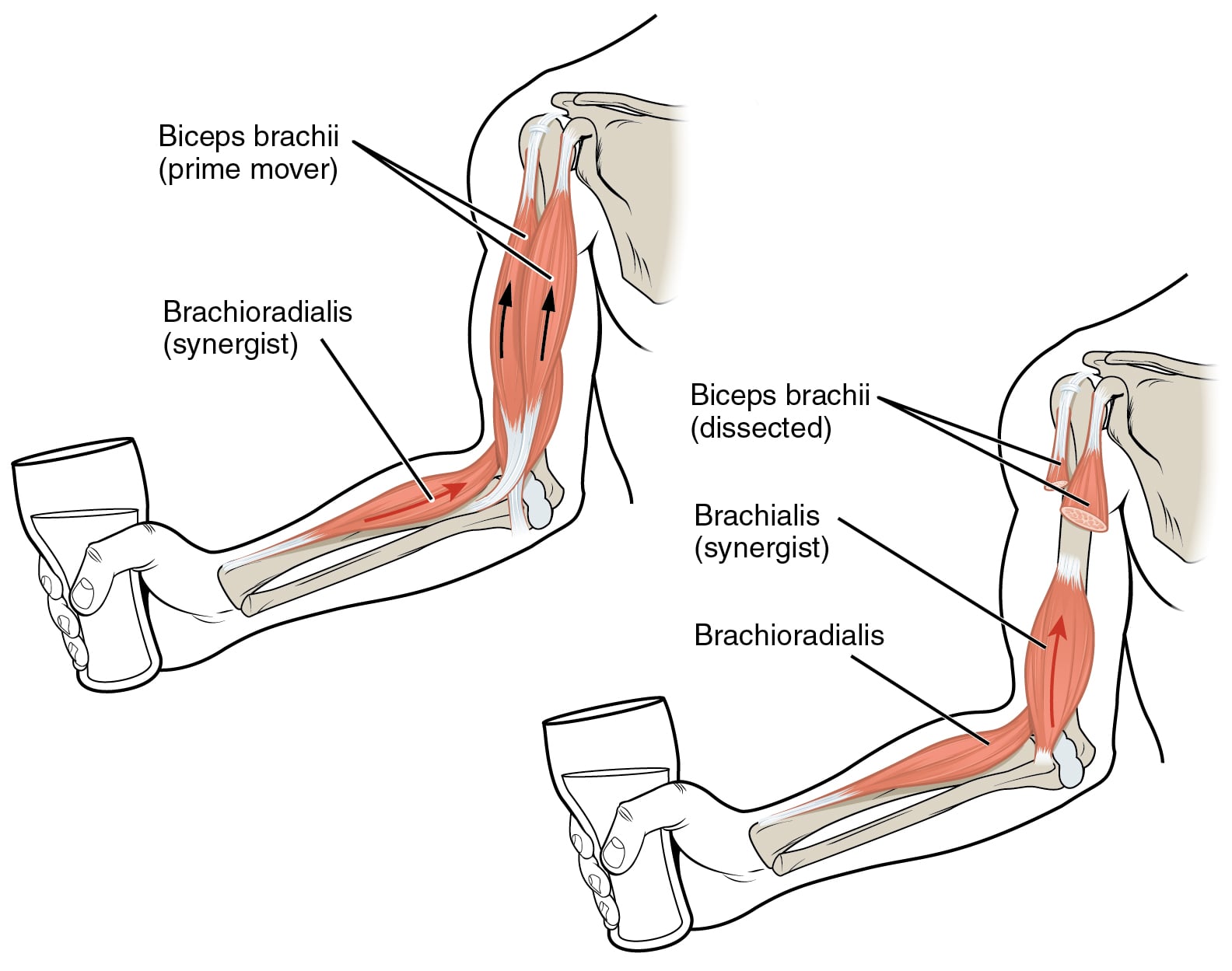
- Superficial dissection: develop lateral to biceps brachii; retract biceps medially to protect the musculocutaneous nerve, which runs on the deep surface of biceps between it and brachialis. The lateral antebrachial cutaneous nerve (terminal musculocutaneous) emerges lateral to biceps distally — protect it.
- Deep dissection: brachialis is split to reach the anterior humeral cortex; leaving the lateral fibres on the bone cushions and shields the radial nerve, which is piercing the lateral intermuscular septum to run anterior in the distal third.
- Radial nerve at the distal extent: in the distal third the radial nerve lies in the interval between brachialis (medially) and brachioradialis (laterally), having pierced the septum about 10 cm proximal to the lateral epicondyle. Distal screws and distal extension threaten it — identify or protect it before distal fixation.
- Proximal danger — anterior circumflex humeral vessels and axillary nerve: proximally the ascending branch of the anterior circumflex humeral artery runs along the inferior border of subscapularis and the lateral lip of the bicipital groove; the axillary nerve passes about 5 to 7 cm distal to the acromion deep to deltoid — avoid over-vigorous proximal and lateral retraction.
- “The classic teaching trap: the claim that the anterior approach to the humerus has an internervous plane in its distal part is false — there is no true internervous interval; the brachialis is split and is safe only because of its dual innervation (radial lateral half, musculocutaneous medial half).
- “Why choose anterior over posterior for the shaft: anterior keeps the radial nerve out of the field for proximal-to-middle-third fractures (the nerve is posterior in the groove) and is the corridor for anterior MIPO; choose posterior when you must directly explore or decompress the radial nerve, or fix the distal third.
- “Musculocutaneous nerve protection equals retracting biceps medially as a unit; it lies on the deep surface of biceps. The lateral antebrachial cutaneous nerve (its continuation) is the structure injured by aggressive lateral retraction distally.
- “Anterior MIPO: a distal window in line with the lateral border of biceps avoids the radial nerve provided dissection stays anterior to the brachialis muscle belly and the nerve is not levered against the septum.
When & Why
What it exposes. The anterolateral (anterior) approach gives direct access to the whole anterior humeral diaphysis — extensile from the coracoid and deltopectoral interval proximally to the anterior distal humerus distally. It is the workhorse for anterior plating of proximal-third and middle-third shaft fractures, for anterior MIPO, and (via the brachialis-splitting extension) for many distal-third shaft fractures. Why anterior rather than posterior. Anterior keeps the radial nerve out of the operative field for proximal-to-middle-third fractures, because the nerve is posterior in the spiral groove; the patient lies supine (no lateral or prone positioning); it is the established corridor for anterior MIPO; and it allows extension to the shoulder proximally and the elbow distally on one supine set-up.
Open reduction and internal fixation of proximal-third and middle-third humeral shaft fractures; anterior MIPO (minimally invasive plate osteosynthesis); fixation of many distal-third shaft fractures via the brachialis-splitting extension; biopsy or excision of anterior diaphyseal lesions; non-union and malunion surgery requiring anterior plate access.
Keeps the radial nerve out of the operative field for proximal-to-middle-third fractures (the nerve is posterior in the spiral groove); the patient lies supine; it is the established corridor for anterior MIPO; and it allows extension proximally to the shoulder and distally to the elbow on one supine set-up.
When the radial nerve must be directly explored, decompressed, or repaired (for example an open fracture with palsy, or a secondary palsy after manipulation), or for distal-third fractures needing maximal exposure and direct nerve visualisation, the posterior (triceps-splitting or triceps-sparing) approach is generally preferred.
Distal-third comminution where bicortical distal screws endanger the radial nerve; very proximal fractures better served by a deltopectoral or deltoid-split shoulder exposure; prior anterior surgery with scarred musculocutaneous or lateral antebrachial cutaneous nerves.
- Anterolateral / anterior
- Proximal-third and middle-third shaft; anterior MIPO
- Posterior
- Distal-third shaft; direct radial nerve exploration or repair
- Anterolateral / anterior
- Out of field mid-shaft; at risk only distally
- Posterior
- Directly visualised in the spiral groove
- Anterolateral / anterior
- Deltopectoral proximally; brachialis split distally (dual innervation, no true interval)
- Posterior
- No true internervous plane (all triceps heads radial); triceps split or reflected
- Anterolateral / anterior
- Supine
- Posterior
- Lateral or prone
- Anterolateral / anterior
- Coracoid to anterior distal humerus
- Posterior
- Olecranon to deltoid insertion
The Exposure
Work down through the layers along the lateral border of biceps, retracting biceps and the musculocutaneous nerve medially, then split the brachialis to reach the anterior cortex. The split is the heart of the exposure: it is safe not because of a true internervous interval (there is none within brachialis) but because brachialis is dual-innervated — the lateral part radial, the medial part musculocutaneous (Leonello 2007) — so each half keeps its nerve, and the lateral fibres left on the bone shield the radial nerve.
Exposure sequence
- Supine on a radiolucent table, the arm on an arm-board or across the chest; a small bump under the scapula assists proximal access. Image intensifier comes from the head or the contralateral side.
- Surface landmarks: the coracoid process and deltopectoral groove proximally, the lateral border of biceps brachii in the arm, and the lateral epicondyle distally — the incision lies along the line joining these.
- Tailor incision length to the fracture: a proximal-third fracture needs the deltopectoral-derived proximal segment; a distal-third fracture needs the brachialis-splitting distal segment; MIPO uses short proximal and distal windows only.
- Incise skin and subcutaneous fat along the lateral border of biceps; protect the lateral antebrachial cutaneous nerve distally where it emerges lateral to biceps.
- Open the deep fascia of the arm along the lateral edge of biceps.
- Retract biceps medially as a unit, carrying the musculocutaneous nerve (which runs on its deep surface, between biceps and brachialis) safely out of the field. Never dissect between the two heads of biceps.
- The brachialis now lies exposed over the anterior humeral shaft.
- Develop the deltopectoral interval — the cephalic vein is taken laterally with deltoid in most descriptions; protect the ascending branch of the anterior circumflex humeral artery at the inferior border of subscapularis and the lateral lip of the bicipital groove.
- Beware the axillary nerve, about 5 to 7 cm distal to the acromion deep to deltoid — limit lateral deltoid retraction.
- Split the brachialis longitudinally in the midline, in line with its fibres, down to bone.
- Sweep the medial half (musculocutaneous-innervated) medially and the lateral half (radial-innervated) laterally, staying subperiosteal.
- Keep the lateral fibres draped over the distal bone to shield the radial nerve, and expose the flat anterior cortex for reduction and plate application.
- Distally, the radial nerve now lies in the interval between brachialis (medially) and brachioradialis (laterally), having pierced the lateral intermuscular septum about 10 cm proximal to the lateral epicondyle — identify or deliberately protect it before placing any distal bicortical screw, and stay anterior to the brachialis belly.
- For MIPO: make only a proximal and a distal window and tunnel the plate submuscularly under brachialis along the anterior cortex, reducing indirectly and preserving the periosteal blood supply for secondary (callus) healing.
- Reapproximate the split brachialis loosely over the plate — it does not require tight repair, and tight closure risks compartment tension.
- Repair the deep fascia along the lateral border of biceps; subcutaneous and skin closure as standard.
- Document radial, musculocutaneous and lateral antebrachial cutaneous nerve function in recovery.
If the examiner asks for the internervous plane, name the deltopectoral interval proximally (deltoid equals axillary nerve; pectoralis major equals pectoral nerves) and then state plainly that there is no true internervous interval distally — the brachialis is split, and that split is safe only because of brachialis dual innervation (lateral half radial, medial half musculocutaneous). Claiming a true distal plane is the classic error.
The musculocutaneous nerve lies on the deep surface of biceps, between biceps and brachialis. Retract biceps medially as one unit and it is carried safely out of the field; never dissect between the two heads of biceps. Its terminal branch, the lateral antebrachial cutaneous nerve, is the structure injured by aggressive lateral retraction distally.
Dangers & Extensions
Structures at risk, by layer
- Where it is at risk
- Distal third (between brachialis and brachioradialis); bicortical distal screws; distal extension
- Protection strategy
- Leave lateral brachialis fibres on bone; identify or protect the nerve before distal fixation; keep dissection anterior to brachialis
- Where it is at risk
- Deep surface of biceps if biceps is split or retracted roughly
- Protection strategy
- Retract biceps medially as one unit; never dissect between its heads
- Where it is at risk
- Lateral to biceps just proximal to the elbow during distal exposure
- Protection strategy
- Identify and protect during subcutaneous dissection distally; gentle lateral retraction
- Where it is at risk
- Proximal extent at the lateral lip of the bicipital groove and inferior subscapularis
- Protection strategy
- Ligate or cauterise deliberately during proximal deltopectoral extension
- Where it is at risk
- Deep to deltoid, about 5 to 7 cm distal to the acromion, during proximal extension
- Protection strategy
- Limit lateral deltoid retraction; stay in the deltopectoral plane proximally
For any distal extension or distal bicortical screw, treat the radial nerve as present in the field: it has crossed from posterior to anterior through the lateral intermuscular septum in the distal third to lie between brachialis and brachioradialis. Either positively identify it, or keep the lateral brachialis fibres interposed and confirm screw trajectory away from the posterolateral cortex. Most iatrogenic palsies in anterior humeral surgery occur distally.
Extensile options. Extend proximally into the deltopectoral interval to reach the proximal third, surgical neck and shoulder (minding the axillary nerve and anterior circumflex vessels). Extend distally toward the elbow through the brachialis split — but here the radial nerve enters the field between brachialis and brachioradialis, so it must be identified or protected before any distal work. For MIPO, only short proximal and distal windows are used and the plate is tunnelled submuscularly under brachialis. Closure. Reapproximate the split brachialis loosely over the plate, repair the deep fascia along the lateral border of biceps, and close the skin. Document the radial, musculocutaneous and lateral antebrachial cutaneous nerves in recovery.
Procedures Through This Approach
- Humeral shaft fixation — anterior plating of proximal-third and middle-third shaft fractures, the principal use of this exposure.
- Anterior MIPO — proximal and distal windows with submuscular plate tunnelling under brachialis, preserving periosteal blood supply.
- Distal-third shaft fractures via the brachialis-splitting extension, with deliberate radial-nerve protection.
- Biopsy or excision of anterior diaphyseal lesions, and non-union or malunion surgery needing anterior plate access.
- When the radial nerve must be directly explored or repaired, convert to the posterior approach to the humerus or use radial nerve exploration.
Viva & Exam Focus
LARMBrachialis split safety
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are plating a middle-third humeral shaft fracture through an anterolateral approach. What is your internervous plane, and is the brachialis split safe?”
“A patient develops a radial nerve palsy after anterior plating of a distal-third humeral shaft fracture. How can this approach injure the radial nerve when the nerve is posterior?”
Plane and layers
- Proximal: deltopectoral interval
- Superficial: lateral to biceps; retract biceps and the musculocutaneous nerve medially
- Deep: split brachialis (dual innervation — radial lateral, musculocutaneous medial)
- Bone: flat anterior humeral cortex
Dangers
- Radial nerve — distal third (between brachialis and brachioradialis) and distal screws
- Musculocutaneous nerve — deep to biceps
- Lateral antebrachial cutaneous nerve — lateral to biceps distally
- Axillary nerve and anterior circumflex humeral vessels — proximal extension
Uses
- Anterior plating of proximal and middle-third shaft fractures
- Anterior MIPO (proximal and distal windows, submuscular tunnel)
- Distal-third fractures via the brachialis split (with nerve protection)
- Biopsy or excision of anterior diaphyseal lesions
References
Brachialis is dual-innervated — the anatomical basis of the safe split
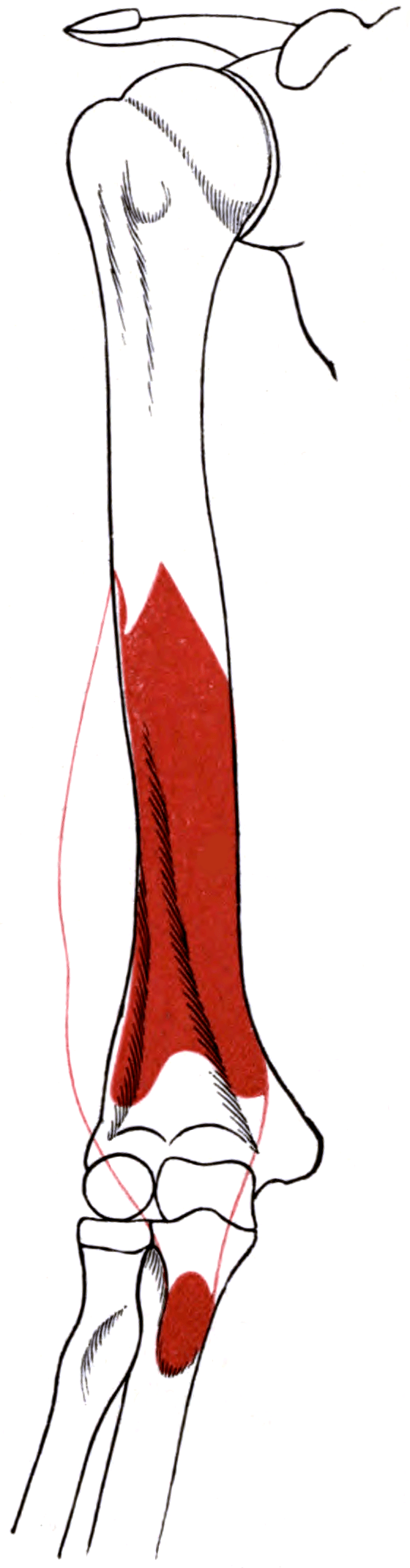
- Brachialis consistently has two heads: a larger superficial head (proximal origin, distal tendinous insertion on the ulnar tuberosity) and a smaller deep head inserting on the coronoid.
- In every specimen a branch of the radial nerve supplied the inferolateral fibres of the deep head, in addition to the dominant musculocutaneous supply.
- This dual innervation defines an internervous-style plane within brachialis: a midline split keeps the medial part musculocutaneous-innervated and the lateral part radial-innervated, refining the anterior and anterolateral surgical approaches to the humerus.
Humeral shaft approaches and MIPO — the anterior corridor
- The classic MIPO corridor for the humerus is anterior, performed with proximal and distal windows and submuscular plate tunnelling that preserves periosteal blood supply for secondary (callus) healing.
- ORIF with a compression plate retains a clear role for simple AO type-A patterns; MIPO and intramedullary nailing are alternatives with their own trade-offs.
- Recognising the advantages and disadvantages of each technique guides selection of the appropriate surgical approach and implant.
Surgical exposures in orthopaedics — the anatomic approach (humerus)
The layered anterior arm anatomy, the deltopectoral proximal extension, and the radial-nerve relationships in the distal third described on this page reflect standard, well-established surgical-anatomy teaching (Hoppenfeld and AO Foundation descriptions) rather than a single cited trial. The cadaveric innervation data are from Leonello et al. and the approach and MIPO synthesis from Orapiriyakul et al.