Beach Chair | Axillary Nerve 5-7 cm Rule | Limited Split with Stay Sutures
- The axillary nerve winds around the surgical neck 5-7 cm distal to the lateral border of the acromion — the split must stay proximal to this and be tagged.
- There is no true internervous plane — the entire deltoid is supplied by the axillary nerve, so safety is purely mechanical (limited split length plus a stay suture).
- A heavy non-absorbable stay suture at the distal apex of the split is the single most important step: it stops the split propagating and stretching the nerve.
- The coracoacromial ligament is divided close to the acromion to open the subacromial space; it is not repaired.
- Secure deltoid reattachment to the acromion (transosseous sutures or anchors) is mandatory — detachment produces deltoid drop and abduction weakness.
When & Why
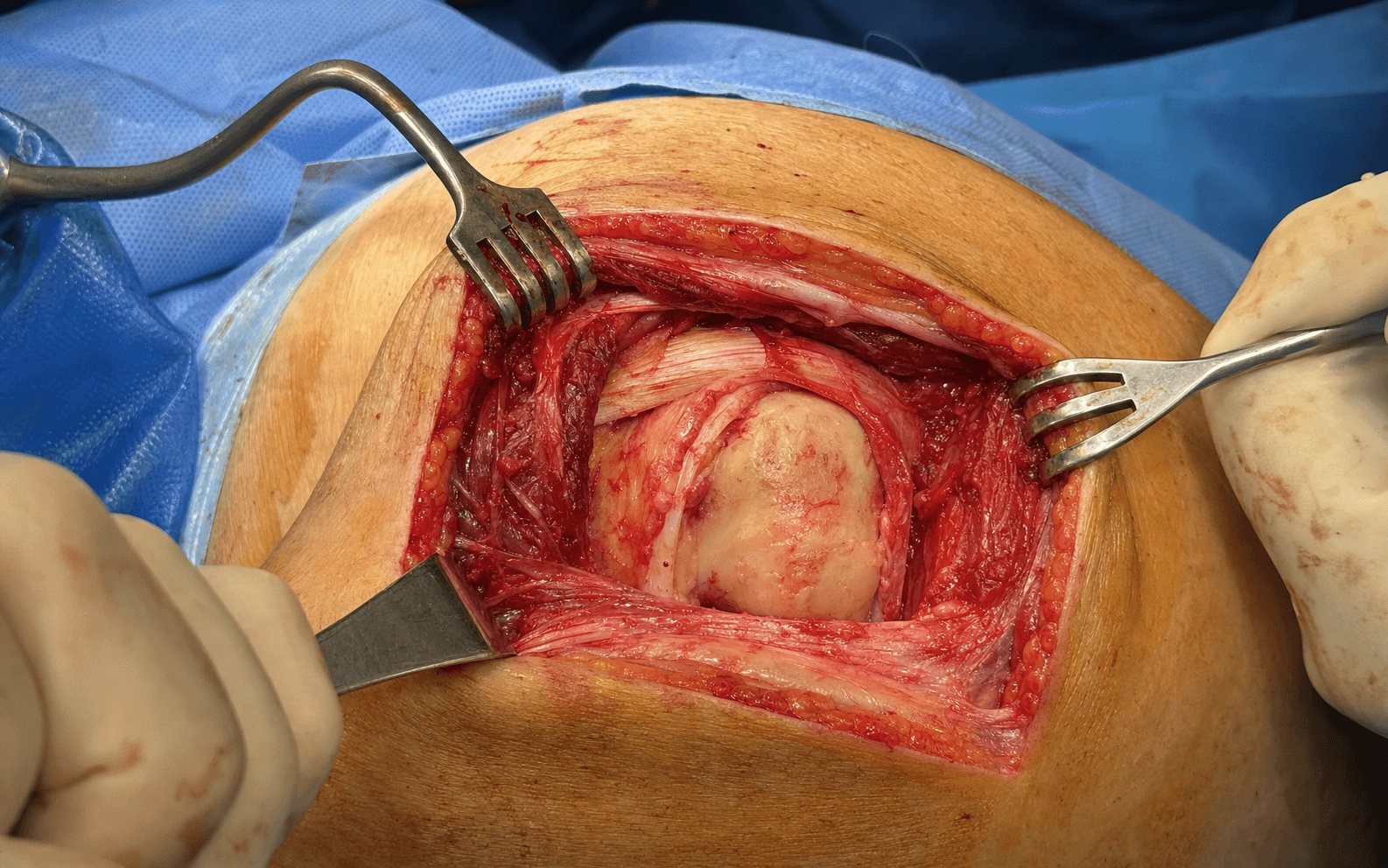
What it exposes. The anterosuperior deltoid-split approach gives direct, limited access to the supraspinatus tendon, the rotator interval (containing the long head of biceps), the superior humeral head and the greater tuberosity. It works by splitting the deltoid in line with its fibres from the anterolateral corner of the acromion, without extensively violating the deltoid origin. Why this approach is chosen. It is the classic exposure for mini-open rotator cuff repair and greater tuberosity fixation — it allows excellent visualisation for tendon mobilisation, anchor placement and tuberosity reduction while preserving the majority of the deltoid. The limited split keeps the axillary nerve safe when the 5-7 cm rule is respected, and the beach chair set-up allows easy conversion to or from arthroscopy. Primary indications:
- Mini-open or open rotator cuff repair (supraspinatus and rotator interval tears)
- Greater tuberosity fracture fixation (displaced fragments)
- Subacromial decompression when arthroscopic equipment is unavailable
- Biceps tenodesis or tenotomy in conjunction with cuff work
- Limited proximal humerus fracture exposure (greater tuberosity component)
- Revision of failed mini-open cuff repairs Contraindications:
- Large or massive rotator cuff tears requiring extensive mobilisation (consider open or arthroscopic)
- Infraspinatus or teres minor pathology (needs a posterior or combined approach)
- Severe glenohumeral arthritis requiring arthroplasty (different exposure)
- Active infection or poor skin quality over the acromion
- Patient unable to tolerate beach chair positioning (severe kyphosis, cervical instability) Alternative approaches:
- Arthroscopic approach — preferred for most rotator cuff repairs and decompression
- Deltopectoral approach — for anterior shoulder, proximal humerus fractures, arthroplasty
- Posterior approach — for infraspinatus, teres minor, or posterior glenoid
- Extended lateral approach — when more distal humeral exposure is required Position & landmarks. Beach chair at 60-70 degrees upright, table tilted 10-15 degrees reverse Trendelenburg, head secured in neutral (Mayfield or similar), all pressure points padded (occiput, scapulae, sacrum, heels), and the arm draped free with a full range of motion available. The blood pressure cuff sits on the non-operative arm; a tourniquet is not usually required for shoulder approaches. Palpate and mark the acromion (its whole outline, with the anterolateral corner as the start of the split), the coracoid process (anterior and medial), the deltoid tuberosity on the humerus (the distal limit of safe exposure), and the clavicle if proximal extension is planned. The C-arm or arthroscopy tower is positioned from the opposite side or the head of the table.
Beach chair positioning carries risks of cerebral hypoperfusion when the head is raised above heart level, brachial plexus injury from arm positioning, and pressure sores. Maintain systolic blood pressure above 90 mmHg or mean arterial pressure within 20 percent of baseline, secure the head in neutral, and document all protective measures.
The Exposure
Work down through the layers from the anterolateral acromion, splitting the deltoid in line with its fibres, tagging the distal apex before any deep work, and opening the subacromial space by dividing the coracoacromial ligament. The defining feature is that there is no internervous plane — every deltoid fibre is supplied by the axillary nerve — so the whole safety strategy is mechanical: a short split and a tagged apex.
Exposure sequence
- Beach chair at 60-70 degrees with the head secured and the arm draped free; the surgeon stands on the operative side with the assistant opposite.
- Mark the whole acromion (anterolateral corner is the split origin), the coracoid, the deltoid tuberosity and the clavicle if proximal extension is planned.
- Make a 4-6 cm longitudinal incision from the anterolateral corner of the acromion distally in line with the deltoid fibres; curve it slightly anteriorly if more anterior access is needed.
- Incise skin and divide subcutaneous fat directly onto the deltoid fascia.
- Identify and protect any cutaneous branches of the axillary nerve that cross the incision.
- Incise the deltoid fascia in line with the muscle fibres and use an assistant-held (not self-retaining) retractor to expose the deltoid belly.
- Split the deltoid fibres longitudinally starting at the anterolateral acromion edge; do not exceed 4-5 cm in length.
- At the distal apex of the split place a heavy non-absorbable stay suture (number 1 or 2 braided polyester) that encircles the distal fibres — this acts as a mechanical barrier that stops the split propagating under retraction and protects the axillary nerve.
- The suture is left in place until closure.
- The subacromial bursa lies immediately beneath the deltoid; excise or open it widely to expose the supraspinatus tendon and the superior humeral head.
- Take care not to damage the underlying rotator cuff during this step.
- Identify the coracoacromial ligament running from the coracoid to the acromion and divide it close to the acromion with diathermy or scissors.
- This opens the anterior subacromial space and allows anterior acromioplasty if indicated; the ligament is not repaired.
- Open the rotator interval if needed to expose the long head of biceps or to mobilise the supraspinatus.
- Inspect the supraspinatus tendon for tears, quality and mobility, and expose the greater tuberosity for fracture work or anchor placement.
The axillary nerve exits the quadrilateral space and winds around the surgical neck of the humerus 5-7 cm distal to the lateral border of the acromion. Any deltoid split must stay proximal to this — limit it to less than 5 cm from the acromion edge, place a heavy stay suture at the apex, and use gentle intermittent retraction. Nerve injury causes deltoid paralysis and sensory loss over the lateral shoulder (regimental badge area).
Because there is no internervous plane, the stay suture at the distal apex of the split is the single most important step for nerve protection. It is a mechanical stop: it prevents the split from extending distally under retraction forces, which is exactly how the axillary nerve gets stretched. Place it before any deep dissection and leave it until closure.
The absence of a true internervous plane is the defining feature of this approach. All deltoid fibres are innervated by the axillary nerve after it exits the quadrilateral space. Safety is therefore entirely mechanical: limit the split to less than 5 cm, tag the apex, and avoid vigorous or prolonged retraction.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Axillary nerve — terminal branches, 5-7 cm distal to acromion
- Protection
- Limit split to less than 5 cm, tag the apex, gentle intermittent retraction
- Structure at risk
- Musculocutaneous nerve (enters coracobrachialis 3-5 cm distal to coracoid tip)
- Protection
- Stay lateral to the coracoid; avoid medial dissection beyond the coracoid base
- Structure at risk
- Cephalic vein (deltopectoral groove)
- Protection
- Identify and retract laterally if the incision drifts anteriorly into the deltopectoral interval
- Structure at risk
- Supraspinatus tendon and long head of biceps
- Protection
- Handle the cuff gently; protect the insertion during drilling and anchor placement; identify and protect or tenodese the biceps
- Structure at risk
- Suprascapular nerve (suprascapular notch)
- Protection
- Not directly at risk, but retraction injury is possible — avoid aggressive medial retraction
Extensile options. Extend proximally along the anterior acromion or the clavicle for acromioclavicular joint work, distal clavicle excision, or partial elevation of the deltoid origin from the clavicle. Distal extension beyond 5 cm risks the axillary nerve — if more distal humeral exposure is required, abandon the split and use the deltopectoral approach instead, always respecting the tagged stay suture so the split cannot propagate. The approach cannot reach the infraspinatus or teres minor without a separate posterior approach. Closure. The deltoid split is closed by tying the distal stay suture first. The deltoid origin is then reattached to the acromion with heavy non-absorbable sutures passed through transosseous bone tunnels or via suture anchors in the acromion — the repair must withstand early active abduction. Subcutaneous tissue is closed in layers and skin with absorbable or non-absorbable sutures. After rotator cuff repair the arm is placed in a sling with an abduction pillow, and pendulum exercises begin within 24-48 hours unless contraindicated.
Failure of deltoid repair leads to deltoid detachment from the acromion: a characteristic cosmetic deformity (deltoid drop), significant abduction weakness, and often the need for complex revision reconstruction. Secure transosseous or anchor repair at the index procedure is therefore mandatory.
Procedures Through This Approach
- Mini-open rotator cuff repair — the principal operation done through this exposure (supraspinatus and rotator interval tears).
- Open rotator cuff repair — for larger tears approached through the same deltoid-split interval.
- Greater tuberosity ORIF — displaced greater tuberosity fractures.
- Subacromial decompression and acromioplasty — when arthroscopic equipment is unavailable.
- Biceps tenodesis or tenotomy — open or mini-open, in conjunction with cuff work.
- Limited proximal humerus fracture exposure and rotator interval or capsular procedures.
- Key steps
- Split, divide CA ligament, place anchors, repair tendon
- Specific risks
- Axillary nerve, cuff tendon quality
- Closure emphasis
- Secure deltoid repair to acromion
- Key steps
- Split, reduce greater tuberosity, screw or anchor fixation
- Specific risks
- Axillary nerve, fragment comminution, articular screw penetration
- Closure emphasis
- Deltoid repair critical
- Key steps
- Split, divide CA ligament, resect anterior acromion
- Specific risks
- Axillary nerve, deltoid origin
- Closure emphasis
- Deltoid reattachment to acromion
Viva & Exam Focus
DELTOIDDELTOID — the exposure, step by step
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old manual worker has a full-thickness supraspinatus tear confirmed on MRI and arthroscopy is not available. Talk me through an anterosuperior deltoid-split approach for repair.”
“During a deltoid-split approach the distal split begins to propagate under retraction. What is your immediate response and how do you protect the axillary nerve?”
“A 42-year-old sustains a greater tuberosity fracture displaced by 1 cm on CT. How would you approach fixation through the anterosuperior deltoid split?”
Patient position
- Beach chair at 60-70 degrees, head secured
- Arm draped free with full motion available
- All pressure points padded (occiput, sacrum, heels)
- C-arm from the opposite side or head of table
- Reverse Trendelenburg 10-15 degrees, systolic BP above 90 mmHg
Axillary nerve protection
- Nerve lies 5-7 cm distal to the lateral acromion edge
- Limit the deltoid split to less than 5 cm from the acromion
- Place a non-absorbable stay suture at the distal split apex
- The stay suture prevents propagation and nerve stretch
- Gentle, intermittent retraction only
Internervous plane
- No true internervous plane exists
- Entire deltoid supplied by the axillary nerve
- Approach is muscle-splitting within a single nerve territory
- Safety is mechanical (length limit plus stay suture)
- Split in line with the deltoid fibres from the acromion
Key danger structures
- Axillary nerve — 5-7 cm rule, tagged split apex
- Musculocutaneous nerve — stay lateral to the coracoid
- Cephalic vein — retract laterally if encountered
- Rotator cuff tendons — protect during drilling
- Long head of biceps — identify and protect
Closure requirements
- Tie the distal stay suture first
- Reattach deltoid to acromion with transosseous sutures or anchors
- Secure repair withstands early active abduction
- Failure causes deltoid drop, abduction weakness, cosmetic deformity
- Revision reconstruction is complex if repair fails
Procedures and limitations
- Mini-open rotator cuff repair (supraspinatus and interval)
- Greater tuberosity ORIF
- Subacromial decompression and acromioplasty
- Cannot reach infraspinatus or teres minor
- Distal extension limited by the axillary nerve
References
A less invasive surgery for rotator cuff tear: mini-open repair
- Mini-open deltoid-split repair provided good to excellent results for rotator cuff tears with low axillary nerve injury rates when the limited-split and stay-suture principles were followed.
The rotator cuff. Full-thickness tears. Mini-open repair
- Mini-open repair through the anterosuperior deltoid split is a reliable technique for full-thickness rotator cuff tears with low complication rates when the 5-7 cm axillary nerve rule is respected.
The posterior branch of the axillary nerve: an anatomic study
- Anatomic study mapping the axillary nerve branches and defining the safe zones and limits for deltoid-splitting surgical approaches to the shoulder.
Neurologic complications of shoulder surgery
- Review highlighting the axillary nerve injury risk during deltoid split approaches and the critical importance of limiting split length to less than 5 cm from the acromion.