Hybrid technique — limited arthroscopy (diagnosis and subacromial decompression) plus a mini-open deltoid-splitting repair, or a pure mini-open repair without arthroscopy · intermediate
- The operation is for a full-thickness symptomatic rotator cuff tear that has failed non-operative care. It is ideal for small to medium (1 to 3cm) crescent-shaped tears with good tissue quality in a primary repair.
- It is a hybrid: limited arthroscopy (diagnostic glenohumeral arthroscopy and subacromial decompression) followed by a mini-open deltoid-splitting repair through a 3 to 5cm incision. A pure mini-open variant skips the arthroscopy and uses a 4 to 6cm incision.
- The deltoid split MUST stay within 5cm of the acromion to protect the axillary nerve, which lies 5 to 7cm inferior to the acromion on the deep surface of deltoid. This is the single most important safety landmark.
- Double-row suture-bridge repair provides superior biomechanical strength and roughly halves the re-tear rate of single-row repair for medium tears, so it is the preferred construct.
When & Why
Indication. A full-thickness, symptomatic rotator cuff tear requiring surgical repair that has failed non-operative management (3 to 6 months of physiotherapy, NSAIDs and at least one injection), in a medically fit patient with realistic expectations. The tear must be one you can repair through a limited exposure. The ideal tear for mini-open repair is a small to medium (1 to 3cm) crescent-shaped tear that reduces to the footprint without complex mobilisation, with good tissue quality, in a primary repair (no prior failed surgery with scarring), in a patient with adequate bone for anchor fixation and a mobile tendon. Relative contraindications. Large or massive tears (greater than 5cm) that need extensive mobilisation, complex L-shaped or reverse-L patterns that are hard to read through a small incision, irreparable tears, severe osteoporosis (inadequate anchor purchase), active infection, significant glenohumeral arthritis (arthroplasty may be better), and a surgeon inexperienced in the technique. The one decision that matters — which approach. Every technique repairs the same tear; the choice is how you get to it:
Limited arthroscopy plus a 3 to 5cm deltoid-splitting repair. Gives direct visualisation and palpation of tissue quality, easier suture passage, lower cost, a shorter learning curve, and is well suited to resource-limited settings.
Camera-only repair through portals — preserves deltoid entirely, least pain, best cosmesis. Needs specialised equipment and a steep learning curve; outcomes are equivalent to mini-open in experienced hands.
A 5 to 7cm deltoid split for extensive exposure. Reserved for massive or complex tears needing wide mobilisation, revision surgery with scarring, or bone grafting — greater deltoid morbidity.
Choose mini-open when the surgeon is more comfortable with direct visualisation, arthroscopic equipment is limited, the tear is a small to medium crescent, or the setting is resource-limited. Choose arthroscopic when the surgeon is expert and deltoid preservation is desired. Choose full open for massive, complex or revision tears. Preoperative planning. Clinically assess symptom duration and mechanism (traumatic versus degenerative), active and passive ROM, rotator cuff strength (supraspinatus, infraspinatus, subscapularis), impingement signs and any atrophy. Image with X-rays (AP, lateral, axillary, outlet) to assess arthritis, acromial morphology and superior migration, and MRI (the gold standard) to grade tear size, pattern, retraction and muscle quality. Plan the approach (hybrid versus pure mini-open), the repair construct (single-row versus double-row), and the anchors (4.5 to 5.5mm; 2 to 4 anchors). Counsel the patient on expected outcomes (85 to 90 percent good or excellent results), the 10 to 30 percent re-tear risk (size- and quality-dependent), the rehabilitation (4 to 6 weeks in a sling, passive ROM only initially, strengthening after 12 weeks, full recovery 12 to 18 months), and the alternatives (non-operative management, arthroscopic repair, full open repair).
Mini-open shares the advantages of both worlds: direct visualisation and palpation (you can see and feel tissue quality and repair tension — feedback lost with the arthroscopic camera), easier suture passage and knot tying under vision, lower cost, and a shorter learning curve. The trade-off is that it still violates deltoid, so it is best for small to medium crescent tears rather than massive or complex patterns.
The Operation
The goal: position the patient, establish the portals and the mini-open incision, perform the arthroscopic diagnosis and decompression (in the hybrid technique), split deltoid within the axillary-nerve safe zone to expose the tear, mobilise and prepare the footprint, repair the cuff with a double-row suture bridge, then close deltoid soundly. The exposure is laid out in full as the first steps below — it is the heart of the operation.
Operative sequence
- Supine with the back elevated 60 to 70 degrees to simulate a seated position; head secured in a foam headrest or horseshoe with the cervical spine neutral to avoid brachial plexus stretch.
- Affected shoulder at the edge of the table for circumferential access; the arm rests in 20 to 30 degrees of abduction, neutral rotation, on a padded arm board that allows free manipulation.
- Pad ischial tuberosities, heels and elbows; monitor blood pressure on the contralateral arm and keep the mean arterial pressure above 70mmHg (the upright position risks hypotension and cerebral hypoperfusion).
- Secure the patient with a hip strap to prevent sliding.
- Mark the acromion (anterolateral and posterolateral corners, lateral edge), the clavicle, the AC joint, the coracoid and the scapular spine.
- Hybrid technique — establish a posterior portal (2cm inferior and 1cm medial to the posterolateral acromion, in the soft spot) and a lateral portal (mid-lateral acromion, 2 to 3cm inferior), then plan a 3 to 5cm anterolateral mini-open incision from the anterolateral corner of the acromion, extending distally in Langer's lines.
- Pure mini-open — a single 4 to 6cm anterolateral incision from the anterolateral acromion along the deltoid fibres (slightly longer, as there is no arthroscopic decompression phase).
- Perform diagnostic glenohumeral arthroscopy to assess the tear from the articular side and to address any concurrent intra-articular pathology (biceps, labrum, chondral damage).
- Move to the subacromial space: bursectomy, confirm the tear size and pattern from the bursal side, and perform subacromial decompression with acromioplasty if there is a hook or spur.
- Address the biceps (tenotomy or tenodesis) and the AC joint (distal clavicle excision) as planned. This arthroscopic phase is the decompression half of the hybrid procedure.
- Through the mini-open incision, split deltoid in the raphe between the anterior and middle fibres (the natural interval), parallel to the fibres, for 2 to 4cm distally from the acromion.
- Keep the split within 5cm of the acromion. The axillary nerve exits the quadrangular space and runs on the deep surface of deltoid 5 to 7cm inferior to the acromion; extending the split beyond 5cm risks direct injury.
- Place stay sutures in the deltoid margins as you split, to mark them for anatomic closure; retract with self-retaining retractors (mini-Gelpi, Army-Navy).
- Open the bursa to expose the cuff tear and the greater tuberosity.
- Define the tear pattern (crescent, U-shaped, L-shaped, reverse-L) and test whether the tendon reduces to the footprint with gentle traction.
- If it does not reach without tension, mobilise in stepwise fashion: release bursal adhesions to the acromion, deltoid and coracoacromial ligament (blunt dissection, sharp as needed); release the coracohumeral ligament at the rotator interval for anterosuperior tightness; perform limited capsular releases from the bursal side for significant retraction.
- For U-shaped or L-shaped tears, perform margin convergence (side-to-side repair of the free margins) before the footprint repair, converting the U to a crescent and reducing medial-lateral tension.
- Suprascapular-nerve safety: the nerve runs 2 to 3cm medial to the glenoid in the spinoglenoid notch — limit medial and posterior capsular releases to avoid a neuropraxia.
- Bring the arm into extension (20 to 30 degrees) and external rotation to deliver the greater tuberosity anteriorly into the mini-incision — critical for footprint access.
- Clear the torn tendon stump, fibrous scar and bursal adhesions with a rongeur or curette.
- Decorticate to a punctate bleeding surface using a curette or small (3.5 to 4.0mm) burr — superficial cortex removed to bleeding cancellous bone. Avoid excessive decortication, which weakens anchor purchase (especially in osteoporotic bone).
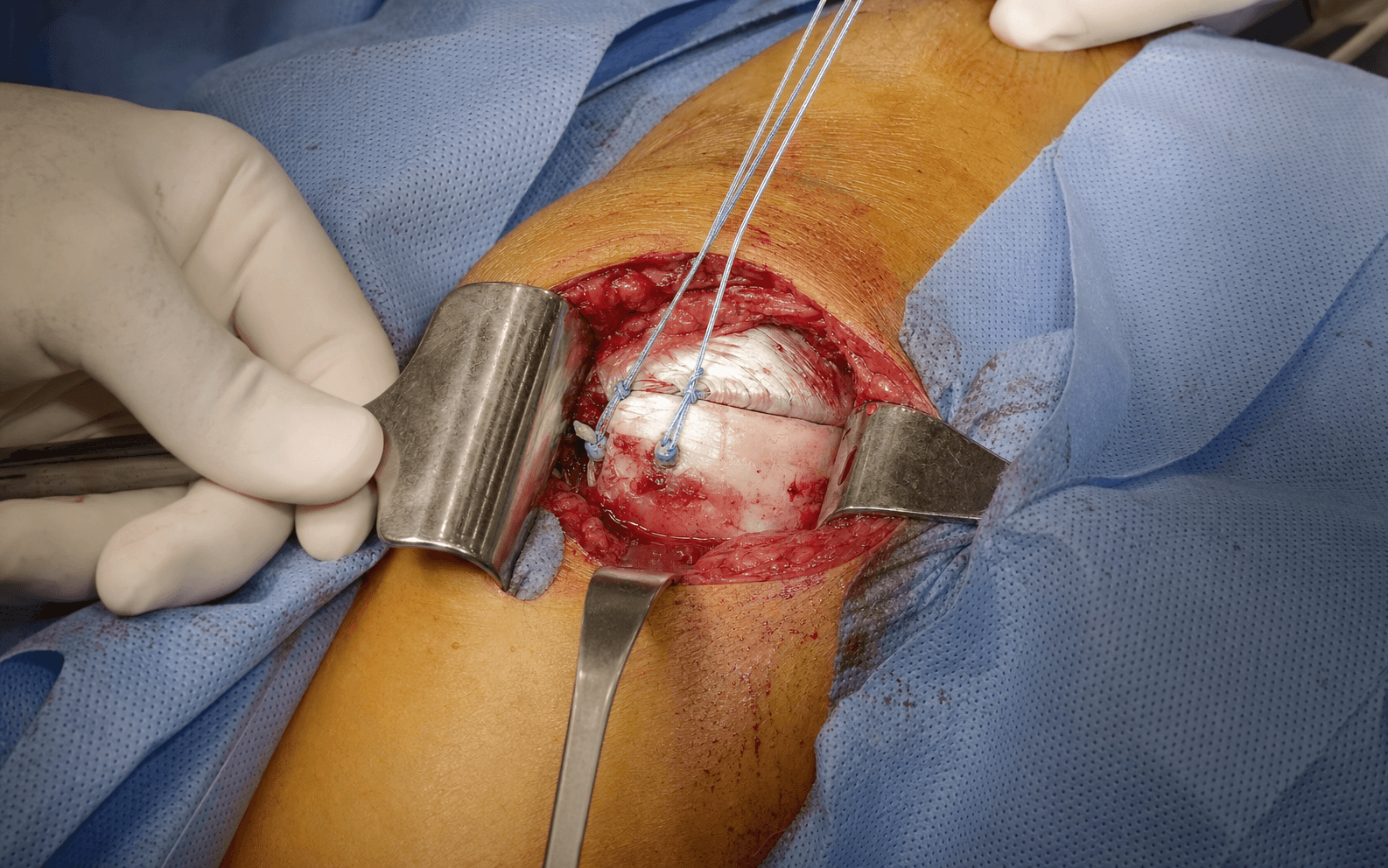
- Double-row suture bridge (preferred for medium tears): place 2 medial anchors at the articular margin and pass mattress sutures; then place 2 knotless lateral anchors 10 to 15mm lateral at the footprint edge, capturing the free medial limbs to form a compression bridge across the whole 2 to 3cm footprint.
- Single-row (small tears, under 2cm, or poor bone): 2 to 3 anchors at the lateral footprint edge, 5 to 10mm apart, at the 45-degree deadman angle for optimal pullout resistance, with mattress sutures 1cm from the tendon edge and a minimum 5mm tissue bridge between passes.
- Insert anchors with #2 braided non-absorbable high-strength sutures (FiberWire, Orthocord); confirm solid purchase by pulling before tying.
- Tie sliding-locking knots (SMC, Roeder) backed up with a minimum of 3 alternating half-hitches on alternating posts, plus 2 backup throws (5 to 6 total), seated flush with a knot pusher.
- Tension is critical: reduce the tendon to the footprint with firm contact but do not over-tighten. The tendon should look pink and perfused; a white, blanched appearance means ischaemia from over-tensioning — release, mobilise further, and re-tie.
- Re-approximate the anterior and middle deltoid fibres anatomically using the stay sutures as guides — no gaps, no overlap.
- Use heavy non-absorbable sutures (#0 or #1 Ethibond, FiberWire or Hi-Fi) — never absorbable (Vicryl loses strength too quickly). Interrupted horizontal mattress or figure-of-8, spaced 5 to 8mm apart through substantial muscle.
- Palpate the closure: it should feel solid with no separation on arm movement, secure but not ischaemic.
- Close the bursal layer (2-0 absorbable if adequate tissue) and the subcutaneous layer (2-0 absorbable, bury knots, achieve haemostasis).
- Skin: subcuticular 3-0 or 4-0 absorbable monofilament (Monocryl), optional skin adhesive.
- Dress with a sterile dressing; immobilise in a sling with a pillow in neutral rotation. Consider a subacromial injection of local anaesthetic (20mL of 0.25 percent bupivacaine) for postoperative analgesia.
The axillary nerve exits the quadrangular space and runs on the deep surface of deltoid, a mean of about 5cm (range 5 to 7cm) inferior to the acromion. Keep the deltoid split within 5cm of the acromion, retract gently, and respect the inferior bursal reflection (the nerve lies immediately beyond it). If the nerve is seen on the deep surface of deltoid, the split is too distal — back out. Most axillary nerve injuries are neuropraxias that recover over 3 to 6 months.
Deltoid detachment causes weakness, chronic pain, a visible or palpable defect, and often needs difficult revision surgery. Prevent it with heavy non-absorbable sutures in a mattress configuration, substantial tissue bites, anatomic re-approximation, and protection during early rehabilitation. Even a small mini-open split needs a closure as strong as a full open repair.
A white, blanched tendon at the repair means ischaemia from over-tensioning. It will not heal, and it raises the risk of suture cut-through and anchor pull-out. Recognise it under direct vision (the mini-open advantage), cut the knots, mobilise further, and re-tie until the tendon is pink and perfused. If the tendon still will not reduce without excessive tension, accept a partial repair or consider augmentation — a lower-tension partial repair beats an over-tight complete repair that fails.
Aftercare & Complications
Rehabilitation. Rehabilitation protects the healing tendon-bone interface and is identical in principle to arthroscopic or open repair. | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 — Protection | 0 to 6 weeks | Sling day and night | Pendulums only (wk 0 to 2); therapist-assisted passive ROM (wk 2 to 6): forward flexion to 90 to 120 degrees, external rotation 30 to 40 degrees. No abduction, no active ROM, no lifting | | 2 — Active-assisted | 6 to 12 weeks | Wean the sling over 1 to 2 weeks | Pulley, cane and wall walks; progress to active ROM to 140 to 160 degrees; gentle isometrics from week 8 to 12 (20 to 30 percent effort) | | 3 — Strengthening | 12 to 16 weeks | None for light tasks | Active ROM against gravity; Theraband and light dumbbells (0.5 to 1kg); scapular stabilisation | | 4 — Advanced | 16+ weeks | None | Progressive weights (1 to 5kg); sport- and work-specific patterns; proprioception and endurance | Return to unrestricted activities of daily living at about 4 to 5 months, manual labour and non-contact sports at 6 months, and contact or overhead sports at 9 to 12 months. Full biological healing takes 12 to 18 months. The most common rehabilitation error is being too aggressive (early active ROM, resistance before 12 weeks, sport before 6 months); prolonged immobilisation beyond 6 weeks causes stiffness. Complications
- Recognition
- Recurrent pain and weakness at 3 to 6 months; loss of active ROM; MRI or ultrasound shows a gap or fluid at the repair
- Prevention
- Adequate mobilisation to reduce tension; double-row for medium tears; optimise biology (smoking cessation, diabetic control); counsel realistic expectations
- Management
- Conservative first — many partial re-tears are asymptomatic. Revision repair if young, symptomatic and acute with good tissue; arthroplasty if elderly, chronic or arthritic
- Recognition
- Progressive loss of passive and active ROM beyond the expected postop limits, more than 20 degrees different from the other side, most evident at 3 to 6 months
- Prevention
- Early passive ROM (pendulums week 1, passive flexion weeks 2 to 6); avoid immobilisation beyond 6 weeks; structured physiotherapy
- Management
- Aggressive physiotherapy and NSAIDs; corticosteroid injection after 3 months; manipulation under anaesthesia after 6 months; arthroscopic capsular release if refractory
- Recognition
- Weakness and pain on abduction or forward flexion; a palpable defect at the split site; visible deltoid wasting; denervation on EMG
- Prevention
- Limit the split to 2 to 4cm and within 5cm of the acromion; strong closure with heavy non-absorbable sutures; protect during early rehab
- Management
- Acute detachment (under 6 weeks): urgent surgical re-repair with advancement, anchors to acromion if needed. Chronic: physiotherapy; revision is difficult. Axillary nerve injury: observe 3 to 6 months, EMG at 3 months, exploration or grafting if no recovery at 6 months
- Recognition
- Superficial: erythema, warmth, drainage, dehiscence. Deep: fever, severe pain, raised inflammatory markers; positive aspiration cultures
- Prevention
- Prophylactic IV cefazolin within 60 minutes of incision; meticulous sterile technique; haemostasis; glucose and smoking control
- Management
- Superficial: oral antibiotics and local wound care. Deep: admission, IV antibiotics, urgent debridement (retain anchors if possible), 6 to 12 weeks of antibiotics; the repair may fail — manage as salvage
- Recognition
- Continued pain beyond 6 months with an intact repair on MRI/ultrasound and normal ROM; positive AC joint, biceps or impingement tests; possible cervical referral
- Prevention
- Adequate acromioplasty if indicated; address biceps and AC joint pathology; low-profile or knotless lateral anchors; counsel realistic expectations
- Management
- Investigate (MRI, cervical imaging, subacromial or AC joint injection). Physiotherapy, NSAIDs and activity modification; arthroscopic debridement, distal clavicle excision or biceps tenotomy if a source is identified
- Recognition
- Early fixation loss or anchor migration on X-ray; late gradual re-tear, pain or mechanical symptoms; palpable prominence
- Prevention
- Size the anchor to the bone (5.5mm in osteoporotic bone); 45-degree deadman angle; avoid over-torquing; limited decortication; verify purchase by pulling
- Management
- Early pull-out: revision with repositioning, larger anchors, bone grafting if defective. Intra-articular anchor: remove arthroscopically and re-repair. Tuberosity fracture: protected immobilisation if stable, ORIF if displaced
- Recognition
- Separating wound edges, persistent drainage, erythema beyond 10 to 14 days, a suture granuloma, a raised thick scar
- Prevention
- Tension-free subcuticular closure; haemostasis; sterile dressing; smoking cessation and diabetic control; patient education
- Management
- Local wound care and risk-factor correction; secondary closure or reclosure if deep; remove exposed sutures; scar massage, silicone sheets or corticosteroid injection for hypertrophic or keloid scars
Expected outcomes. Around 85 to 90 percent of patients achieve significant pain relief and report good or excellent satisfaction, 80 to 85 percent return to their previous functional level, and about 90 percent regain functional ROM (forward flexion above 120 degrees). Strength improves gradually over 12 to 18 months and may not fully normalise. Structural healing (re-tear rates). Overall 10 to 30 percent depending on tear characteristics: small tears (under 1cm) 5 to 10 percent, medium tears (1 to 3cm) 15 to 25 percent, large tears (3 to 5cm) 30 to 40 percent, and massive tears (over 5cm) 40 to 60 percent — massive tears are generally not done mini-open. Double-row constructs lower the re-tear rate by about 10 to 15 percent versus single-row. Good prognosis favours small or medium crescent tears, acute or traumatic onset, good tissue quality, minimal fatty infiltration (Goutallier 0 to 1), minimal retraction, a non-smoker, good bone, and rehab compliance. Poor prognosis favours large or massive tears, chronic degenerative tears, poor tissue, advanced fatty infiltration (Goutallier 3 to 4), significant retraction (Patte 3), smoking, diabetes, osteoporosis, non-compliance, and a workers' compensation claim. Meta-analyses show equivalent structural healing and functional outcomes between arthroscopic and mini-open repair in experienced hands; surgeon experience matters more than the technique chosen.
Viva & Exam Focus
SPLITSPLIT — deltoid safety principles
ANCHORSANCHORS — double-row repair technique
Exits the quadrangular space and runs on deltoid's deep surface 5 to 7cm inferior to the acromion. Protection: keep the deltoid split within 5cm of the acromion and retract gently.
Passes through the suprascapular notch and runs 2 to 3cm medial to the posterior glenoid rim in the spinoglenoid notch. Protection: avoid aggressive medial and posterior capsular releases during mobilisation.
Enters coracobrachialis 3 to 8cm distal to the coracoid tip (variable). Protection: limit anterior dissection beyond the coracoid and stay aware during subscapularis work.
Runs in the deltopectoral groove. Protection: only at risk in the deltopectoral variant — identify it and protect it (take it laterally with deltoid or medially with pectoralis).
The anchor insertion site, at risk in osteoporotic bone. Protection: avoid over-decortication, use an appropriate anchor size (4.5 to 5.5mm), limit anchor density, and insert at the 45-degree deadman angle.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old manual labourer has a 2cm crescent-shaped supraspinatus tear on MRI with minimal retraction and good tissue quality, having failed 4 months of physiotherapy. What are the advantages and disadvantages of mini-open repair compared with arthroscopic repair for this patient?”
“After placing your medial-row anchors and tying the knots, the tendon looks white and blanched at the repair site. What is the problem and how do you manage it?”
“As you close the deltoid split, the fellow suggests 2-0 Vicryl absorbable sutures 'to avoid suture removal'. What is your response and what is the correct deltoid closure technique?”
Indication
- Full-thickness symptomatic tear failing 3 to 6 months of non-operative care
- Ideal: small to medium crescent tear (1 to 3cm), good tissue, primary, mobile
- Surgeon preference and resource setting drive the choice
- Avoid: large or massive tears, complex U or L shapes, irreparable tears
Key anatomy
- Deltoid split: raphe between anterior and middle fibres, 2 to 4cm, within 5cm of the acromion
- Axillary nerve: 5 to 7cm inferior to the acromion on deltoid's deep surface
- Suprascapular nerve: 2 to 3cm medial to the glenoid
- Greater-tuberosity footprint: 2 to 3cm AP by 1 to 2cm ML; arcuate-artery supply
Critical steps
- Hybrid: limited arthroscopy (diagnosis and decompression) then mini-open repair
- Mini-open incision 3 to 5cm; deltoid split 2 to 4cm in the raphe, within 5cm of the acromion
- Mobilise (adhesions, coracohumeral ligament, limited capsular releases) to reach the footprint without tension
- Footprint prep: arm extension and ER, decorticate to punctate bleeding, avoid over-removal
- Double-row: medial anchors at the articular margin, knotless lateral 10 to 15mm lateral — suture bridge
- Mattress 1cm from edge, 5mm tissue bridge, pink not blanched
- Deltoid closure: heavy non-absorbable #0 to #1, mattress, 5 to 8mm spacing
Danger zones
- Axillary nerve (5 to 7cm below the acromion) — limit the split to within 5cm
- Suprascapular nerve (2 to 3cm medial to the glenoid) — limit medial releases
- Musculocutaneous nerve (3 to 8cm distal to the coracoid) — limit anterior dissection
- Greater-tuberosity fracture — avoid over-decortication, size the anchor, 45-degree angle
- Over-tensioned repair (blanching) — mobilise adequately
Technique pearls
- Mini-open advantages: direct visualisation and palpation, easier suturing, lower cost, shorter learning curve
- Mini-open disadvantages: violates deltoid, limited exposure, intermediate pain and stiffness
- Arm extension and ER deliver the tuberosity anteriorly for footprint access
- Tag deltoid edges with stay sutures for anatomic closure
Complications
- Re-tear 10 to 30 percent — mobilise well, double-row for medium tears, optimise biology, rehab compliance
- Deltoid dysfunction 1 to 2 percent — strong non-absorbable closure, limit the split
- Stiffness 5 to 10 percent — early passive ROM, avoid immobilisation beyond 6 weeks
- Infection 0.5 to 1.5 percent — prophylactic antibiotics, sterile technique, urgent debridement if deep
- Nerve injury under 1 percent — axillary (split over 5cm), suprascapular (medial releases); document and monitor
Post-op protocol
- Phase 1 (0 to 6 weeks): sling, passive ROM only — pendulums, supine slides to 90 to 120 degrees
- Phase 2 (6 to 12 weeks): wean sling, active-assisted then active ROM, isometrics from week 8
- Phase 3 (12 to 16 weeks): strengthening (Theraband, 0.5 to 1kg weights)
- Phase 4 (16+ weeks): advanced strengthening — unrestricted 4 to 6 months, sports 6 to 9 months
Exam tips
- Mini-open is hybrid (arthroscopy plus mini-open) or pure mini-open — state which
- Outcomes are equivalent to arthroscopy and open in experienced hands
- Direct visualisation and palpation is the primary advantage
- Deltoid closure is as critical as the cuff repair — heavy non-absorbable sutures
- Never extend the deltoid split beyond 5cm below the acromion
Background & Evidence
Overview. Rotator cuff repair reattaches a torn cuff tendon (most often supraspinatus) to its footprint on the greater tuberosity. The cuff consists of supraspinatus (superior facet), infraspinatus (posterosuperior) and teres minor (posteroinferior) on the greater tuberosity, with subscapularis on the lesser tuberosity. The footprint measures roughly 2 to 3cm anteroposteriorly by 1 to 2cm medial-laterally, and the bone is supplied by the arcuate artery (a branch of the anterior and posterior circumflex humeral arteries). Degenerative tears occur most often in older patients (often more than 60 years) and are frequently multipatterson; traumatic tears occur at any age. Mini-open repair is suited to the small to medium crescent end of this spectrum. Tear classification governs whether mini-open is appropriate.
- Dimension
- Under 1cm
- Typical re-tear rate
- 5 to 10 percent
- Mini-open suitability
- Ideal
- Dimension
- 1 to 3cm
- Typical re-tear rate
- 15 to 25 percent
- Mini-open suitability
- Ideal (preferred for mini-open)
- Dimension
- 3 to 5cm
- Typical re-tear rate
- 30 to 40 percent
- Mini-open suitability
- Difficult — arthroscopic or full open usually better
- Dimension
- Over 5cm
- Typical re-tear rate
- 40 to 60 percent
- Mini-open suitability
- Not suited to mini-open — full open or arthroscopic
Tear pattern is read at arthroscopy or through the mini-incision: a crescent tear reduces simply to the footprint and is ideal for mini-open; U-shaped and L-shaped (and reverse-L) tears have a longitudinal component and need margin convergence (side-to-side repair of the free margins before footprint fixation) to reduce tension. Complex patterns are hard to read and repair through a limited incision.
- Description
- Tendon stump close to the bony insertion
- Implication
- Easily repairable, low tension
- Description
- Stump retracted to the level of the glenoid rim
- Implication
- Needs mobilisation, usually repairable
- Description
- Stump retracted medial to the glenoid rim
- Implication
- Significant retraction, harder to repair, high tension
- Muscle appearance
- Normal muscle, no fat
- Prognostic implication
- Good healing potential
- Muscle appearance
- Some fatty streaks
- Prognostic implication
- Good healing potential
- Muscle appearance
- More muscle than fat
- Prognostic implication
- Acceptable
- Muscle appearance
- As much muscle as fat
- Prognostic implication
- Predicts poorer healing
- Muscle appearance
- More fat than muscle
- Prognostic implication
- Predicts poor healing — often irreparable
References
Arthroscopic versus mini-open rotator cuff repair: a comprehensive review and meta-analysis
- Meta-analysis of 5 Level I-III comparative studies (MEDLINE/PubMed 1966-2006) with minimum 1-year (mean over 2-year) follow-up, all outcome scores converted to a 100-point scale
- NO significant difference in functional outcome scores between all-arthroscopic and mini-open repair groups
- NO significant difference in complication rates between the two techniques
Prospective randomised comparison of arthroscopic versus mini-open rotator cuff repair of the supraspinatus tendon
- RCT of 34 patients (17 per arm; mean age 60 years) with isolated supraspinatus tears; arthroscopic double-row vs mini-open transosseous repair, identical standardised rehabilitation
- Less early NSAID use at week 1 in the arthroscopic group, but the mini-open group had LOWER pain scores from weeks 4 to 8 (p less than 0.05)
- At 6 months Constant-Murley score, range of motion and MRI healing (3 of 16 re-ruptures in EACH group) were equivalent between techniques
Clinical and structural outcomes after arthroscopic single-row versus double-row rotator cuff repair: a systematic review and meta-analysis of level I randomized clinical trials
- Meta-analysis of 7 Level I RCTs (524 shoulders) comparing single-row with double-row repair
- Imaging-confirmed re-tear rate 25.9% (68/263) single-row vs 14.2% (37/261) double-row; relative risk 1.76 (95% CI 1.25-2.48, p=0.001) favouring double-row, driven mainly by partial-thickness re-tears
- NO significant difference in ASES, UCLA or Constant score improvement between constructs
The outcome and repair integrity of completely arthroscopically repaired large and massive rotator cuff tears
- 18 patients with tears over 2cm repaired arthroscopically, assessed by validated ultrasound protocol at minimum 12 and 24 months
- Recurrent defects in 17 of 18 shoulders; ASES improved from 48.3 to 84.6 at 1 year despite non-healing
- Results deteriorated by 2 years (mean ASES fell to 79.9; forward elevation fell from 152 to 142 degrees), linking large tear size to high re-tear and late decline
Useful boundaries of the subacromial bursa (axillary nerve safe-zone anatomy)
- Cadaveric study (17 specimens) mapping the subacromial bursa relative to the acromion and circumflex (axillary) nerve
- Mean distance from all points of the acromion to the axillary nerve was approximately 5cm; the subdeltoid bursal reflection lay a mean of 0.8cm (range 0-1.4cm) above the nerve
- Authors explicitly recommend coupling the bursal reflection landmark to published safe deltoid-split distances during mini-open rotator cuff repair to avoid axillary nerve injury
Open versus arthroscopic rotator cuff repair: a comparative view of 96 cases
- Comparative study of open and arthroscopic rotator cuff repair in 96 cases
- Mini-open and arthroscopic repairs achieved equivalent functional outcomes with similar complication rates
Arthroscopically assisted rotator cuff repair: correlation of functional results with integrity of the cuff
- Early description of the mini-open (arthroscopically assisted) technique
- 88 percent good or excellent results, with intact repairs correlating with better outcomes
All-arthroscopic versus mini-open rotator cuff repair: a long-term retrospective outcome comparison
- Long-term retrospective comparison of all-arthroscopic and mini-open repair
- No significant differences in UCLA scores, patient satisfaction or re-tear rates between techniques
All-arthroscopic versus mini-open rotator cuff repair: a retrospective review with minimum 2-year follow-up
- Retrospective comparison with minimum 2-year follow-up
- Similar healing rates (92 percent arthroscopic vs 93 percent mini-open) and functional outcomes
Arthroscopic versus mini-open rotator cuff repair: a comparison of clinical outcome
- Comparison of arthroscopic and mini-open repair clinical outcomes
- Equivalent ASES and UCLA scores, with slightly less pain in the arthroscopic group at early follow-up
Arthroscopically assisted mini-open rotator cuff repair
- Technical description of the hybrid mini-open technique with arthroscopic decompression
- Good outcomes and low complication rates reported