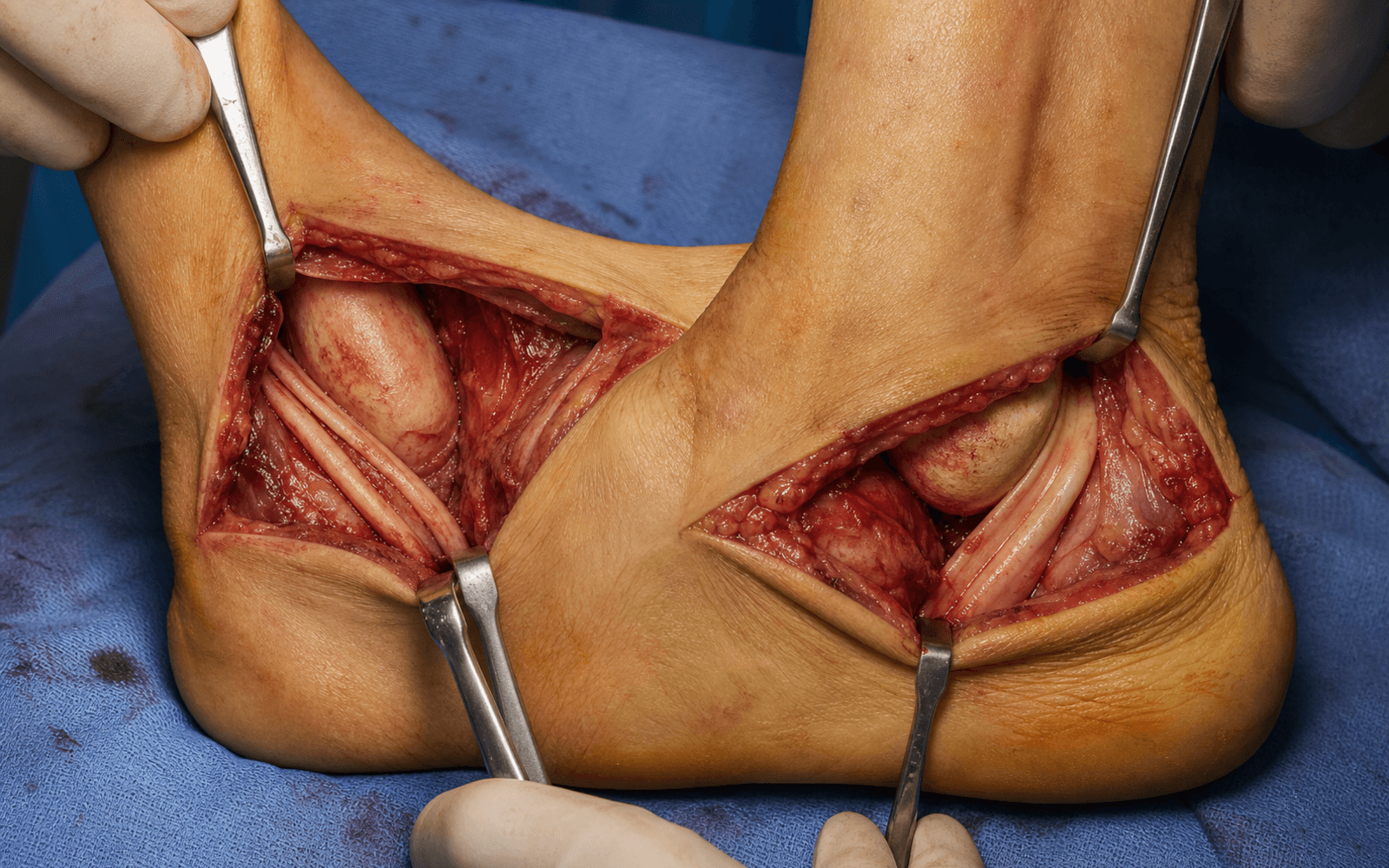
Medial posterior tibial tendon sheath and lateral peroneal retinaculum — protecting the tarsal tunnel neurovascular bundle and the sural nerve
- There is no classical internervous plane on either side — dissection stays within the tendon sheaths, so the danger is the adjacent neurovascular structures, not a muscle interval.
- Medial approach: protect the tarsal tunnel neurovascular bundle, which lies between flexor digitorum longus and flexor hallucis longus.
- Lateral approach: identify and protect the sural nerve, which crosses about 2 cm distal to the tip of the lateral malleolus.
- Retinacular repair is mandatory on both sides — repair the flexor retinaculum medially and the superior peroneal retinaculum laterally to prevent bowstringing and subluxation.
- Both retinacula are tested intra-operatively by ranging the ankle and subtalar joint before closure.
When & Why
What each side exposes. The medial approach opens the posterior tibial tendon (PTT) sheath behind the medial malleolus, giving access to the PTT, the flexor digitorum longus (FDL) tendon, and the contents of the tarsal tunnel. The lateral approach opens the peroneal tendon sheath behind the lateral malleolus, giving access to the peroneus longus and brevis, the retromalleolar groove, and the superior peroneal retinaculum (SPR). Why these approaches are chosen. The posterior tibial tendon runs in a sheath directly behind the medial malleolus, so direct access requires the medial route. The peroneal tendons run in a retromalleolar groove behind the lateral malleolus, and the lateral approach exposes them while protecting the sural nerve. Both approaches preserve the tendon sheaths so the retinacula can be repaired at closure — the key to preventing post-operative bowstringing and subluxation. Three approach variants. - Medial approach — behind the medial malleolus over the PTT sheath, for PTTD debridement, FDL harvest and transfer.
- Lateral approach — behind the lateral malleolus over the peroneal sheath, for peroneal repair, groove deepening and retinacular reconstruction.
- Combined — both medial and lateral incisions for complex bilateral tendon pathology or combined reconstruction. Indications — medial approach. - Posterior tibial tendon dysfunction (PTTD) stages I to II for debridement and repair.
- FDL harvest for tendon transfer in flatfoot reconstruction.
- Posterior tibial tendon transfer for foot drop or cavus correction.
- Tarsal tunnel release for tarsal tunnel syndrome.
- Excision of an accessory navicular or os tibiale externum. Indications — lateral approach. - Peroneal tendon tears or tendinopathy requiring repair.
- Peroneal tendon subluxation or dislocation requiring groove deepening.
- Superior peroneal retinacular reconstruction.
- Peroneus longus to brevis transfer for chronic tears.
- Harvest of peroneus longus for tendon grafting. Contraindications. Active infection over the proposed incision; severe soft tissue compromise requiring an alternative route; previous surgery with distorted anatomy (relative); and any situation where the neurovascular structures cannot be safely protected. Alternatives include endoscopic tendon sheath procedures for selected tendinopathies, percutaneous techniques for limited debridement, and combined medial and lateral incisions for complex reconstruction. Position and landmarks. The patient is positioned supine with an ipsilateral hip bump — internally rotate the leg for the medial approach, externally rotate it for the lateral approach. Apply a thigh tourniquet (inflated to 250 to 300 mmHg after exsanguination), flex the knee 20 to 30 degrees over a bolster, and place the foot at the end of a radiolucent table. Isolated lateral work can use the lateral decubitus position; simultaneous medial and lateral work is done prone. - Medial landmarks: medial malleolus tip; the PTT palpable behind and inferior to the malleolus with the foot in plantarflexion and inversion; the navicular tuberosity (the PTT insertion) 2 to 3 cm anterior and inferior to the malleolus; and the tarsal tunnel, running from 2 cm proximal to the medial malleolus distally to the abductor hallucis.
- Lateral landmarks: lateral malleolus tip; the peroneal tendons palpable in the retromalleolar groove with resisted eversion; the peroneal tubercle on the calcaneus separating longus and brevis; and the sural nerve, crossing 2 cm distal to the lateral malleolus tip in the subcutaneous tissue.
- Incisions: medial — a longitudinal incision 1 cm posterior to the medial malleolus, from 4 cm proximal to the tip to 3 cm distal toward the navicular (8 to 12 cm); lateral — a longitudinal incision 1 cm posterior to the lateral malleolus, from 4 cm proximal to the tip to 3 cm distal toward the peroneal tubercle (8 to 12 cm).
The Exposure
Work down through the layers behind each malleolus, opening the tendon sheath in line with the skin incision and protecting the adjacent neurovascular structures, then deliver the tendon for the planned procedure.
Anatomy you must know first Bony anatomy. The medial malleolus carries the posterior groove for the posterior tibial tendon. The flexor retinaculum stretches from the medial malleolus to the calcaneus and forms the roof of the tarsal tunnel. Laterally, the lateral malleolus has a retromalleolar groove deepened by a fibrocartilaginous ridge that contains the peroneal tendons; the peroneal tubercle on the calcaneus separates the peroneus longus and brevis distally. Tendon anatomy — medial (posterior) compartment. - Posterior tibial tendon: inserts on the navicular, cuneiforms and metatarsal bases; the primary invertor and arch supporter.
- Flexor digitorum longus: lies deep and lateral to the PTT; harvested for transfer in PTTD.
- Flexor hallucis longus: the most lateral and deepest of the three; lies lateral to the neurovascular bundle. Tendon anatomy — lateral compartment. - Peroneus longus: superficial, crossing under the cuboid to reach the plantar foot.
- Peroneus brevis: deeper, inserting on the fifth metatarsal base.
- Both tendons share a common sheath proximal to the peroneal tubercle. Tarsal tunnel contents, from anterior to posterior — memorise this order, because safe medial dissection depends on it: 1. Tibialis posterior tendon.
- Flexor digitorum longus tendon.
- Posterior tibial artery and veins.
- Tibial nerve (dividing into medial and lateral plantar nerves).
- Flexor hallucis longus tendon. The neurovascular bundle therefore sits between FDL and FHL. Laterally, the sural nerve crosses 2 cm distal to the lateral malleolus tip and is sensory to the lateral foot; peroneal artery branches may lie deep to the tendons. There is no major motor nerve at risk in the lateral approach. ### Internervous plane There is no classical internervous plane on either side — the dissection is performed within the tendon sheath itself. - Medial: open the PTT sheath and incise the flexor retinaculum longitudinally. The tarsal tunnel neurovascular bundle lies between FDL and FHL; protect it by identifying that interval and retracting the bundle gently as the procedure demands.
- Lateral: open the common peroneal tendon sheath and incise the superior peroneal retinaculum. The sural nerve is the only structure at risk, protected by identifying it in the subcutaneous tissue 2 cm distal to the lateral malleolus.
Medial exposure sequence
- Make a longitudinal incision 1 cm posterior to the medial malleolus, centred over the posterior tibial tendon sheath.
- Extend 4 cm proximal to the malleolus tip and 3 cm distal toward the navicular, placing the incision directly over the sheath.
- Incise skin and subcutaneous tissue; identify and protect any saphenous nerve branches.
- The flexor retinaculum appears as a thick fibrous band — incise it longitudinally in line with the skin to expose the PTT sheath.
- The neurovascular bundle lies between FDL (anterior) and FHL (posterior) — identify this interval.
- Protect the posterior tibial artery and tibial nerve with gentle retraction and a vessel loop around the bundle.
- The PTT lies in its sheath immediately anterior to the neurovascular bundle — incise the sheath longitudinally and deliver the tendon for debridement or repair.
- For FDL harvest, identify the FDL deep and lateral to the PTT and harvest it at the knot of Henry in the midfoot.
Lateral exposure sequence
- Make a longitudinal incision 1 cm posterior to the lateral malleolus, centred over the peroneal tendon sheath.
- Extend 4 cm proximal to the malleolus tip and 3 cm distal toward the peroneal tubercle; mark the expected course of the sural nerve before incising.
- Incise skin and subcutaneous tissue and identify the sural nerve in the distal wound, about 2 cm distal to the lateral malleolus tip.
- Protect it with a vessel loop and gentle retraction; the SPR is the fibrous thickening over the tendons.
- Incise the superior peroneal retinaculum longitudinally in line with the skin incision to open the common peroneal sheath.
- The peroneus longus lies superficial and the peroneus brevis lies deeper against the fibula.
- Deliver the tendons into the wound and assess the retromalleolar groove depth.
- If groove deepening is required, elevate a periosteal flap from the posterior fibula, deepen the groove with a burr, then replace the flap; repair the retinaculum with non-absorbable suture or anchors to the fibular periosteum.
The two structures that define these approaches are the tarsal tunnel neurovascular bundle medially (posterior tibial artery, veins and tibial nerve, lying between FDL and FHL) and the sural nerve laterally (crossing 2 cm distal to the lateral malleolus tip). Identify the FDL–FHL interval early medially and the sural nerve in the distal wound laterally, protect each with a vessel loop, and use gentle retraction only. Injury medially causes plantar numbness, intrinsic weakness and possible vascular compromise; injury laterally causes lateral foot numbness and a painful neuroma.
The flexor retinaculum (medial) and the superior peroneal retinaculum (lateral) are critical stabilisers. Both must be repaired at closure using non-absorbable suture or anchors — failure to repair the peroneal retinaculum leads to tendon subluxation in up to 30 percent of cases. Test the repair intra-operatively by ranging the ankle and subtalar joint through full dorsiflexion, plantarflexion, inversion and eversion.
Dangers & Extensions
Structures at risk, by side and layer.
- Layer
- Skin / subcutaneous
- Structure at risk
- Saphenous nerve branches
- Protection
- Gentle handling; protect crossing branches
- Layer
- Deep
- Structure at risk
- Tarsal tunnel neurovascular bundle (posterior tibial artery, veins, tibial nerve)
- Protection
- Identify the interval between FDL and FHL early; vessel loop; gentle retraction only
- Layer
- Tendon sheath
- Structure at risk
- Flexor digitorum longus (deep to PTT)
- Protection
- Identify and protect during PTT work; transect distal to the knot of Henry if harvesting
- Layer
- Skin / subcutaneous
- Structure at risk
- Sural nerve (about 2 cm distal to the lateral malleolus tip)
- Protection
- Identify in the distal wound before deep dissection; vessel loop; minimal retraction
- Layer
- Retinaculum
- Structure at risk
- Superior peroneal retinaculum
- Protection
- Repair with non-absorbable suture or anchors to the fibular periosteum to prevent subluxation
- Layer
- Deep
- Structure at risk
- Peroneal artery branches
- Protection
- Stay within the sheath; avoid aggressive deep retraction
Extensile options. - Medial, proximal: extend along the posteromedial border of the tibia; the interval stays between FDL and FHL with the neurovascular bundle protected — useful for proximal tendon pathology or combined procedures with tibial osteotomy.
- Medial, distal: extend toward the navicular and midfoot along the PTT to its insertion — useful for accessory navicular excision, distal tendon work or spring ligament repair.
- Medial, plantar: extend into the arch for knot of Henry access during FDL harvest.
- Lateral, proximal: extend along the peroneal compartment; the sural nerve is not at risk proximally — useful for proximal peroneal pathology.
- Lateral, distal: extend toward the peroneal tubercle and fifth metatarsal base, where longus and brevis separate — useful for distal peroneal work or peroneus longus harvest.
- Groove-deepening modification: elevate a posterior fibular periosteal flap, deepen the groove with a burr to a 5 to 6 mm depth, replace the flap, and repair the retinaculum over the tendons.
- Combined: for complex bilateral pathology, position the patient prone or stage lateral decubitus then supine, using separate incisions that each follow the principles above. Closure. Medial: irrigate, repair the PTT sheath with absorbable suture if opened, repair the flexor retinaculum with non-absorbable suture to prevent bowstringing, close subcutaneous tissue and skin, and apply a compressive dressing and posterior splint with the foot in slight plantarflexion and inversion. Lateral: irrigate, repair the SPR with non-absorbable suture or suture anchors to the fibular periosteum, test stability by ranging the ankle and subtalar joint, close in layers, and apply a compressive dressing and posterior splint with the foot in neutral or slight eversion. Post-operative protocol. Non-weight bearing in a splint or cast for 4 to 6 weeks depending on the procedure (longer for repair, shorter for debridement), transition to a walking boot with gradual weight bearing, and begin physical therapy for tendon strengthening and proprioception at 6 to 8 weeks. Follow up at 2 weeks for wound check and suture removal, 6 weeks for radiographs and weight-bearing progression, 12 weeks for functional review, and 6 months for strength testing and return to sport.
- Incidence
- 5 to 15 percent if retinaculum not repaired
- Prevention
- Meticulous retinacular repair
- Treatment
- Revision retinacular reconstruction
- Incidence
- 2 to 5 percent
- Prevention
- Protect the neurovascular bundle; avoid excessive retraction
- Treatment
- Observation, night splint, revision release if persistent
- Incidence
- 2 to 4 percent
- Prevention
- Careful soft tissue handling, antibiotics
- Treatment
- Irrigation and debridement, antibiotics
- Incidence
- 3 to 8 percent
- Prevention
- Protected weight bearing, gradual strengthening
- Treatment
- Revision repair or transfer
- Incidence
- 3 to 5 percent
- Prevention
- Protect the nerve, minimal retraction
- Treatment
- Observation, excision if symptomatic
Failure to repair the superior peroneal retinaculum is the most common cause of post-operative peroneal tendon subluxation. Test the repair by ranging the ankle through full dorsiflexion and plantarflexion and the subtalar joint through inversion and eversion — if the tendons sublux during testing, revise the repair with suture anchors or a periosteal flap augmentation.
Procedures Through This Approach
Through the medial approach: - Posterior tibial tendon debridement and repair for tendinopathy.
- Flexor digitorum longus transfer for PTTD reconstruction.
- Posterior tibial tendon transfer for foot drop.
- Tarsal tunnel decompression.
- Accessory navicular excision with tendon advancement.
- Spring ligament repair or reconstruction. Through the lateral approach: - Peroneal tendon debridement and repair.
- Peroneal groove deepening for recurrent subluxation.
- Superior peroneal retinacular reconstruction.
- Peroneus longus to brevis transfer.
- Peroneal tendon tenodesis for chronic tears.
- Harvest of peroneus longus for tendon grafting.
Viva & Exam Focus
MEDIAL PTTMEDIAL APPROACH — PTT and the tarsal tunnel
LATERAL PERLATERAL APPROACH — peroneal tendons
Tibialis posterior tendon, flexor digitorum longus tendon, posterior tibial artery and veins, tibial nerve, flexor hallucis longus tendon. The neurovascular bundle lies between FDL and FHL — this order is the key to safe dissection during the medial approach.
Approximately 2 cm distal to the tip of the lateral malleolus, in the subcutaneous tissue. It must be identified and protected during the lateral approach; injury causes lateral foot numbness and neuroma pain.
Failure to repair the superior peroneal retinaculum leads to post-operative tendon subluxation or dislocation in up to 30 percent of cases. Repair is tested intra-operatively by ranging the ankle and subtalar joint, using non-absorbable suture or anchors.
At the knot of Henry in the midfoot, distal to the master knot where FDL and FHL cross. The tendon is transected distal to this point and transferred proximally to augment or replace the posterior tibial tendon.
5 to 6 mm. The groove is deepened with a burr after elevating a posterior fibular periosteal flap; the flap is replaced and the retinaculum repaired over the tendons to maintain stability.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old woman presents with progressive flatfoot deformity and medial ankle pain. MRI shows posterior tibial tendon tendinosis with spring ligament attenuation. How would you approach surgical reconstruction?”
“A 28-year-old athlete presents with recurrent peroneal tendon subluxation after multiple ankle sprains. Examination confirms tendon dislocation with ankle dorsiflexion and eversion. How would you approach surgical stabilisation?”
“A 45-year-old patient has both posterior tibial tendon dysfunction and peroneal tendon subluxation after a high-energy injury. How would you plan and execute combined surgical approaches?”
Medial approach landmarks
- Incision 1 cm posterior to the medial malleolus
- Tarsal tunnel neurovascular bundle between FDL and FHL
- Posterior tibial tendon in its sheath, anterior to the neurovascular bundle
- FDL lies deep and lateral to the PTT
- Repair the flexor retinaculum at closure
Lateral approach landmarks
- Incision 1 cm posterior to the lateral malleolus
- Sural nerve crosses 2 cm distal to the lateral malleolus tip
- Peroneus longus superficial, brevis deeper
- Retromalleolar groove deepened to 5 to 6 mm if required
- Repair of the superior peroneal retinaculum is mandatory
Tarsal tunnel contents (anterior to posterior)
- Tibialis posterior tendon (most anterior)
- Flexor digitorum longus tendon
- Posterior tibial artery and veins
- Tibial nerve (medial and lateral plantar branches)
- Flexor hallucis longus tendon (most posterior)
Danger structures
- Tarsal tunnel neurovascular bundle — identify between FDL and FHL
- Sural nerve — identify 2 cm distal to the lateral malleolus
- FDL tendon — protect during PTT procedures
- Peroneal groove — deepen if subluxation is present
- Both retinacula — repair with non-absorbable suture or anchors
Closure principles
- Medial: repair the flexor retinaculum to prevent bowstringing
- Lateral: repair the peroneal retinaculum to prevent subluxation
- Test stability after retinacular repair
- Compressive dressing and posterior splint
- Non-weight bearing 4 to 6 weeks depending on the procedure
Procedures through each approach
- Medial: PTT debridement, FDL transfer, tarsal tunnel release
- Medial: accessory navicular excision, spring ligament repair
- Lateral: peroneal repair, groove deepening, retinacular reconstruction
- Lateral: peroneus longus to brevis transfer, tendon harvest
- Combined: complex reconstruction requiring both sides
References
Guidelines, registries and global practice Tendon disorders of the hindfoot are managed worldwide according to principles that converge across examination systems. The medial approach for posterior tibial tendon dysfunction and the lateral approach for peroneal pathology are standard techniques taught in advanced orthopaedic practice and equivalent curricula. Side-by-side principles (where guidance converges).
- Position on tendon approaches
- CT or MRI for pre-operative planning of tendon pathology; protect neurovascular structures in all approaches; retinacular repair is mandatory for peroneal procedures
- Position on tendon approaches
- Soft tissue handling principles apply; staged procedures for combined medial and lateral pathology; early protected mobilisation after tendon repair
- Position on tendon approaches
- Evidence supports combined bony and tendon procedures for PTTD; groove deepening plus retinacular repair for recurrent peroneal subluxation
Registry and population evidence. - PTTD affects approximately 3 to 5 percent of adults over 50 years, with higher prevalence in obese and diabetic populations.
- Peroneal tendon pathology is identified in 10 to 15 percent of patients with chronic lateral ankle instability.
- Long-term outcomes after FDL transfer and calcaneal osteotomy show 70 to 80 percent maintained correction at 10 years. Global practice variation. In high-resource settings, MRI, endoscopic assistance and dedicated tendon anchors are common. In resource-limited settings, the same anatomical principles apply using standard instruments, with careful attention to retinacular repair and neurovascular protection. Consent (globally applicable). Discuss sural nerve injury (3 to 5 percent, mostly transient), tarsal tunnel neurovascular injury (less than 2 percent), post-operative tendon subluxation if the retinaculum is not repaired (5 to 15 percent), wound infection (2 to 4 percent), and the possibility of revision surgery or arthrodesis if reconstruction fails.
For the operative surgery station, describe both the medial and lateral approaches: incision placement, the neurovascular structures at risk (the tarsal tunnel bundle medially, the sural nerve laterally), the requirement for retinacular repair, and the procedures performed through each approach. Know the order of tarsal tunnel contents and the distance of the sural nerve from the lateral malleolus.
Flexor Digitorum Longus Transfer for Posterior Tibial Tendon Dysfunction
- FDL transfer combined with medial calcaneal osteotomy achieved 80 to 90 percent good to excellent results at 2 to 5 year follow-up
- Tendon transfer alone without bony correction had higher failure rates in stage II PTTD
- Post-operative tendon excursion averaged 60 to 70 percent of normal
- Patient satisfaction exceeded 85 percent when combined procedures were used
Peroneal Tendon Subluxation: Surgical Treatment and Outcomes
- Superior peroneal retinacular repair or reconstruction achieved stable tendons in 85 to 95 percent of cases
- Groove deepening was required in 40 percent of recurrent cases
- Sural nerve injury occurred in 4 percent and was mostly transient
- Return to sport averaged 4 to 6 months after retinacular reconstruction
Tarsal Tunnel Syndrome: Diagnosis and Surgical Outcomes
- Surgical decompression achieved good to excellent results in 70 to 80 percent of patients with positive electrodiagnostic studies
- Space-occupying lesions identified in 20 to 30 percent of cases at surgery
- Incomplete release was the most common cause of failure
- Post-operative scar tethering occurred in 5 to 10 percent
Peroneal Groove Deepening: Technique and Results
- Periosteal flap groove deepening with retinacular repair achieved stable tendons in 92 percent at 2 years
- Average groove depth increased from 2 mm to 5.5 mm post-operatively
- No recurrent subluxation in patients with adequate retinacular repair
- Complications included transient sural neuritis in 6 percent
Long-term Outcomes of Posterior Tibial Tendon Reconstruction
- Combined FDL transfer and medial calcaneal osteotomy maintained correction in 78 percent at 10 years
- Progressive flatfoot deformity recurred in 22 percent, mostly in obese patients
- Patient-reported outcomes remained good despite some radiographic deterioration
- Conversion to triple arthrodesis occurred in 8 percent at long-term follow-up