Lateral approach posterior to the fibula · intermediate
- Peroneus brevis is ANTERIOR in the retromalleolar groove and inserts at the 5th metatarsal base; it is the tendon most commonly torn — the classic C-shaped longitudinal split from compression between the longus posteriorly and the fibula laterally. Longus is POSTERIOR, coursing under the foot to the 1st metatarsal base and medial cuneiform.
- The superior peroneal retinaculum (SPR) is the PRIMARY soft-tissue restraint and must be repaired or reattached in every subluxation case — restoring it is what controls dislocation.
- Groove deepening is a selective adjunct, not a default: reserve it for a flat or convex (shallow, less than 5 mm) groove. Adding it routinely does not improve outcomes and lengthens operating time (Cho 2014, Level II).
- The sural nerve crosses the posterolateral ankle close to the tendons and is the most at-risk structure — its course is highly variable with no reliable fixed landmark, so identify it early and protect it with vessel loops throughout.
- During groove deepening, maintain 3–4 mm of anterior cortex (palpate frequently) and limit deepening to 3–5 mm to avoid an iatrogenic fibular fracture or cortical perforation.
- Immobilise post-operatively in slight eversion (5–10°) and neutral dorsiflexion to offload the SPR repair and reduce tension on the reconstruction.
When & Why
Indication. Symptomatic peroneal tendon pathology — recurrent subluxation or dislocation with documented superior peroneal retinaculum (SPR) insufficiency, or a symptomatic longitudinal tendon tear — that has failed conservative management (physiotherapy with peroneal strengthening and proprioception, bracing, activity modification and at least one injection) over 3–6 months. In high-demand athletes and military personnel, an acute complete SPR rupture or an acute dislocation with a bony avulsion is usually managed operatively from the outset because non-operative treatment carries a high redislocation rate. Absolute indications
- Recurrent peroneal tendon subluxation or dislocation with documented SPR insufficiency
- Symptomatic longitudinal peroneal tendon tear greater than 50% width after failed conservative management
- Acute complete SPR rupture in a high-demand athlete or military personnel
- Peroneal tendon dislocation with an associated avulsion fracture requiring fixation Relative indications
- Chronic peroneal tenosynovitis refractory to conservative treatment
- A tendon tear less than 50% width with mechanical symptoms
- A shallow retromalleolar groove (less than 5 mm depth) with symptomatic subluxation
- Failure of prior conservative management: physiotherapy, bracing, activity modification, injections Contraindications. Absolute: active infection overlying the surgical site; severe peripheral vascular disease with inadequate perfusion; medical comorbidities prohibiting surgery. Relative: uncontrolled diabetes with poor wound-healing potential; heavy tobacco use; poor patient compliance with post-operative restrictions; significant ankle arthritis requiring a different approach; a neuropathic (Charcot) ankle. Pre-operative assessment. Clinically, look for swelling posterior to the lateral malleolus, ecchymosis and a visible or palpable subluxation; palpate for tendon tenderness and reproduce subluxation with circumduction (dorsiflexion plus eversion reproduces the snap, and resisted eversion is painful). Assess associated lateral ligament injury (anterior drawer, talar tilt) and test function (single-leg heel raise, toe-walking) and lateral foot sensation in the sural distribution. Image with weight-bearing AP, lateral and mortise ankle plus AP and lateral foot radiographs (look for the os peroneum and avulsion fractures); an MRI is critical — axial sequences assess tendon tears, tenosynovitis, SPR integrity and groove depth; ultrasound gives a dynamic real-time view of subluxation (operator-dependent); and a CT is used to measure retromalleolar groove depth when deepening is contemplated (less than 5 mm is shallow). Key MRI findings are T2 hyperintensity (tendinosis), a longitudinal split (the tram-track sign), a torn or attenuated SPR, a flat or convex groove, and any ankle effusion, lateral malleolar marrow oedema or os peroneum. Match the operation to the pathology. The single most important decision is whether the groove needs deepening at all — it usually does not.
- Recommended operation
- Groove deepening plus SPR repair or reconstruction
- Recommended operation
- SPR repair or reconstruction alone (bone-tunnel technique) — groove deepening adds no benefit (Cho 2014)
- Recommended operation
- Debridement and tubularization, plus SPR repair if subluxation coexists
- Recommended operation
- Debridement with side-to-side repair to the adjacent intact tendon, or allograft augmentation
- Recommended operation
- Excision of diseased tendon with tenodesis or an FDL/FHL transfer; allograft reconstruction for a complete double rupture
Setup & positioning. Position lateral decubitus with the affected side up (preferred — gravity assists exposure and optimal visualisation) or supine with a bump under the ipsilateral hip (easier anaesthesia access). Apply a thigh tourniquet to 250–300 mmHg and pad all bony prominences (add an axillary roll if lateral). Consent specifically for sural nerve injury or a painful neuroma, wound complications from the thin lateral skin, recurrent subluxation from an inadequate SPR repair, residual eversion weakness, and ankle stiffness.
The Operation
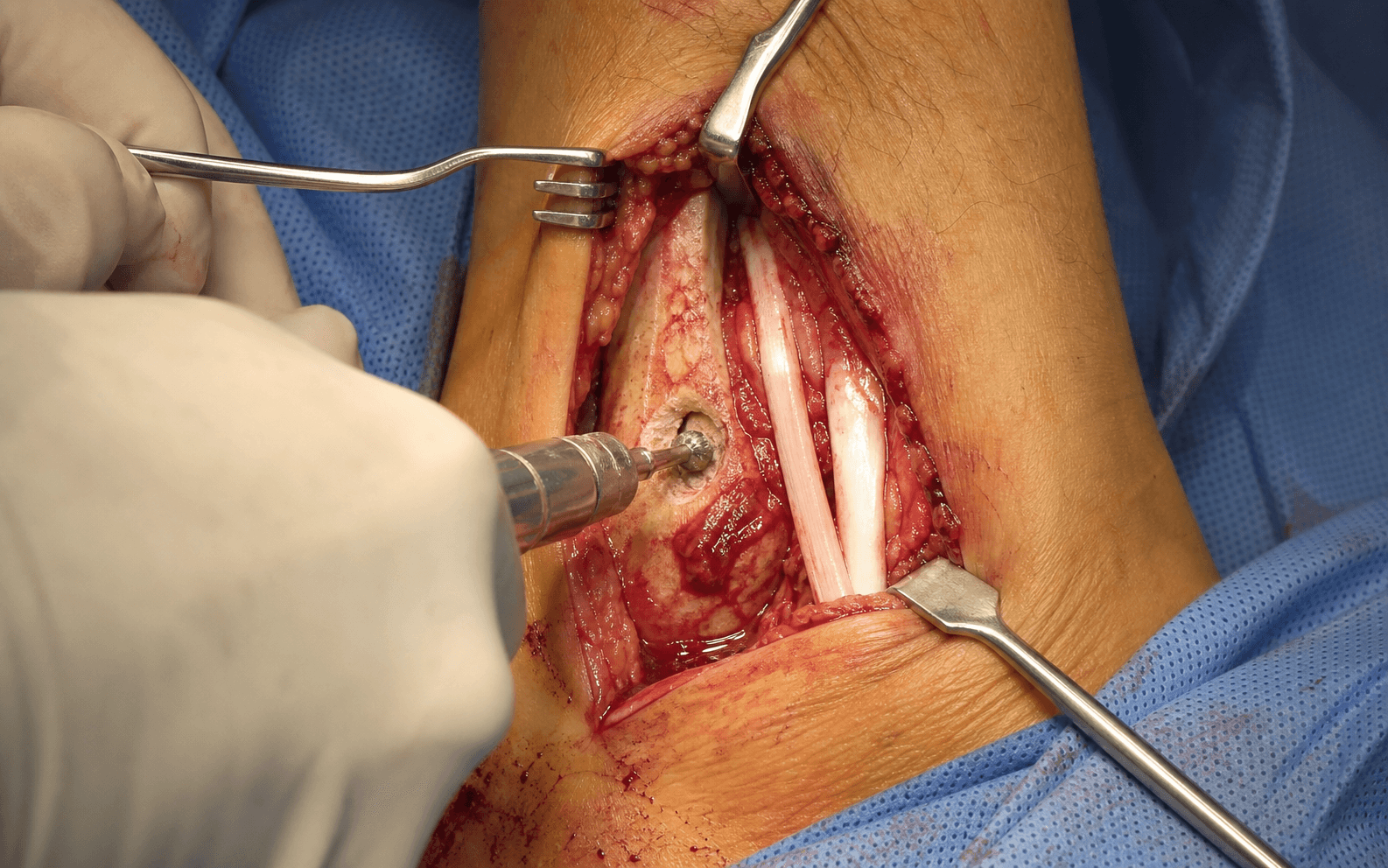
The goal: expose the tendons through the lateral approach posterior to the fibula, identify and protect the sural nerve, repair any tendon tear, selectively deepen a flat or convex groove, and then — the indispensable step — reconstruct the SPR so the tendons track stably through full range of motion. The exposure is laid out in full as the first steps below (and in depth on the approach to the posterior tibial and peroneal tendons page).
Operative sequence
- Position lateral decubitus with the affected side up (gravity assists exposure), or supine with a bump under the ipsilateral hip; apply and prepare a thigh tourniquet (250–300 mmHg) and pad all bony prominences.
- Mark four landmarks: the lateral malleolus tip; the peroneal tendon course posterior to the fibula; the EXPECTED course of the sural nerve (it crosses the posterolateral ankle close to the tendons and is highly variable, so do not rely on a fixed distance); and a curvilinear 6–8 cm incision centred on the lateral malleolus.
- Make a curvilinear incision centred on the lateral malleolus, about 4 cm proximal to 2–4 cm distal; sharp dissection through skin only, raising full-thickness flaps (thin flaps over the malleolus necrose).
- FIRST priority after the skin: identify the sural nerve and lesser saphenous vein in the posterior subcutaneous tissue, protect them with vessel loops, and retract gently throughout — sural nerve injury is the most commonly reported complication.
- Lateral ankle skin is thin with limited vascularity, so handle it gently to prevent edge necrosis, and control the lesser saphenous vein with bipolar to avoid a haematoma.
- Identify the superior peroneal retinaculum (SPR) — the fibrous band overlying the retromalleolar groove. In chronic subluxation it is usually torn or attenuated; document its status, as this guides the reconstruction.
- Incise the SPR longitudinally at the midline, creating superior and inferior flaps for later repair, and expose both tendons in the groove.
- Avoid excessive distal dissection — the calcaneofibular ligament lies deep to the tendons distally.
- Inspect both tendons along their full length. Brevis (ANTERIOR): look for the classic C-shaped longitudinal split, tenosynovitis and degenerative change. Longus (POSTERIOR): look for tears, os peroneum fracture or diastasis, and an intratendinous ganglion.
- Perform a dynamic examination — plantar- and dorsiflex and invert/evert the ankle while observing tracking and subluxation; this also reveals groove depth and SPR competence.
- Brevis is involved in roughly half of cases, both tendons in about a third, and longus alone in about a fifth.
- Tear less than 50% width: debride frayed edges and tubularize with a running 3-0/4-0 absorbable suture (side-to-side repair).
- Tear greater than 50% width: debride non-viable tissue and repair side-to-side to the adjacent intact tendon, or consider allograft augmentation.
- Severe degeneration greater than 75%: excise the diseased segment and perform a tenodesis (brevis-to-longus) or an FDL/FHL transfer.
- Perform an aggressive synovectomy — remove all inflamed synovium to prevent recurrent tenosynovitis. Preserve all viable tissue; over-resection causes eversion weakness.
- Reserve deepening for recurrent subluxation with a shallow (flat or convex) groove less than 5 mm deep — it is NOT a routine step.
- Using a high-speed burr with a rounded tip, remove cancellous bone from the posterior fibular surface to create a smooth U-shaped channel 3–5 mm deeper.
- CRITICAL: maintain 3–4 mm of anterior (lateral) cortex — palpate the cortex every 30–60 seconds to avoid perforation; smooth all edges; irrigate intermittently with saline to prevent thermal necrosis.
- Test tendon tracking — the tendons should remain in the groove through full range of motion. Deepening without restoring the SPR will NOT control dislocation.
- The SPR repair is the ESSENTIAL step for preventing recurrent subluxation — advance and reattach the retinaculum to its posterior fibular footprint.
- Choose the technique by tissue quality (the three options are set out below the timeline).
- Position the ankle in neutral dorsiflexion and SLIGHT EVERSION (5–10°) during the repair to avoid over-tensioning — over-tightening compresses the tendons and causes pain and stiffness.
- Before closure, perform a full dynamic assessment — ideally with the tourniquet deflated, as swelling can mask instability.
- Plantar- and dorsiflex and invert/evert the ankle fully while observing the tendons; they should remain stable in the groove without subluxation.
- If subluxation persists, reassess groove depth, SPR tension and the need for augmentation BEFORE closure.
- Achieve meticulous hemostasis with bipolar cautery — avoid excessive cautery near the sural nerve, which causes thermal neuropraxia.
- Irrigate thoroughly; close the deep fascia over the tendons with 2-0 absorbable if tissue quality allows (optional), the subcutaneous layer with 3-0 absorbable, and the skin with a 3-0/4-0 subcuticular or 3-0 nylon.
- Excellent hemostasis matters — a haematoma increases infection and CRPS risk, and a tension-free closure prevents necrosis of the thin lateral skin.
- Apply a well-padded short-leg splint or CAM walker boot with the ankle in SLIGHT EVERSION (5–10°) and neutral dorsiflexion — slight eversion offloads the SPR repair.
- Apply a compressive dressing, elevate the leg, and keep the patient non-weight-bearing initially.
- Avoid excessive plantarflexion (equinus contracture risk); inadequate immobilisation risks SPR failure and recurrent subluxation.
SPR repair — three options. Pick by tissue quality; whichever you choose, repair with the ankle in neutral dorsiflexion and slight eversion.
Advance the inferior flap posteriorly and superiorly, overlap it onto the superior flap, and secure with 2-0 non-absorbable suture to create a doubled, tensioned restraint.
Create a 3–5 mm tunnel in the posterior fibula about 1 cm proximal to the tip, pass the SPR through it, and secure with a suture anchor or transosseous sutures for robust mechanical fixation.
Harvest a 3–4 mm lateral strip of Achilles tendon (or use allograft), and weave it through a bone tunnel or anchor it to the fibula to supplement the native repair.
- Why it is at risk
- Crosses the posterolateral ankle close to the tendons and Achilles (cadaveric mean about 18 mm from the lateral border of the Achilles at its insertion — Webb 2000), running with the lesser saphenous vein; course is highly variable
- How to protect it
- Identify early with vessel loops; keep the incision along the peroneal tendons (not too posterior); gentle retraction; minimal cautery
- Why it is at risk
- Runs with the sural nerve posteriorly, superficial to the deep fascia; injury causes a significant haematoma
- How to protect it
- Identify and protect with the sural nerve; control with bipolar if injured; preserve skin-flap vascularity
- Why it is at risk
- Thin skin over the lateral malleolus with limited subcutaneous tissue and vascularity
- How to protect it
- Full-thickness flaps; avoid excessive retraction; meticulous hemostasis; careful tension-free closure
- Why it is at risk
- Lies deep to the groove during deepening; perforation weakens the fibula and risks fracture
- How to protect it
- Maintain 3–4 mm of cortical thickness; palpate the cortex every 30–60 seconds during burring; limit deepening to 3–5 mm
- Why it is at risk
- Lies deep to the peroneal tendons distally, running from the fibula tip to the lateral calcaneus
- How to protect it
- Avoid excessive distal dissection; preserve the lateral ligament complex during SPR reconstruction
The sural nerve is the most at-risk structure in lateral ankle surgery. It crosses the posterolateral ankle close to the peroneal tendons and the Achilles (a cadaveric mean of about 18 mm from the lateral border of the Achilles at its insertion, crossing lateral about 9.8 cm proximally — Webb 2000) and runs with the lesser saphenous vein. Its course is highly variable with no reliable fixed landmark, so do not trust a measured distance — identify it early by careful dissection, protect it with a vessel loop, retract gently and use minimal cautery nearby. Most injuries are a transient neuropraxia; a painful neuroma may need excision with burial in muscle.
Groove deepening is selective, not routine. When it is indicated (a flat or convex groove less than 5 mm deep), deepen only 3–5 mm and maintain at least 3–4 mm of anterior cortex: palpate the lateral fibular surface every 30–60 seconds, burr smoothly with intermittent saline irrigation, and use fluoroscopy if available. A perforation or propagating crack is an iatrogenic fracture — assess stability; a stable non-displaced defect can be managed with extended non-weight-bearing, while a displaced fracture needs ORIF with a lateral plate.
Repair the SPR with the ankle in neutral dorsiflexion and slight eversion (5–10°). Slight eversion relaxes the reconstructed retinaculum so it is not over-tensioned, then holds the repair in the protected position for immobilisation.
The restraint that holds the tendons in the groove is the SPR, not the groove. Anatomic SPR repair or reattachment alone gives good-to-excellent results and low recurrence (Cho 2014, Park 2021). Add groove deepening only for a flat or convex groove, or for intrasheath subluxation (Raikin 2009) — adding it to SPR repair for a normal groove did not improve outcomes and lengthened tourniquet time (Cho 2014).
Aftercare & Complications
Rehabilitation | Phase | Timing | Weight-bearing & immobilisation | Therapy focus | |-------|--------|----------------------------------|---------------| | 1 | 0–2 weeks | Short-leg splint or CAM boot in slight eversion and neutral dorsiflexion; non-weight-bearing with crutches | Elevation, ice and ankle pumps of the non-operative joints; multimodal analgesia; DVT prophylaxis if high-risk; sutures out at 10–14 days | | 2 | 2–6 weeks | Tendon-repair-only: begin partial weight-bearing at week 2–3; groove deepening: non-weight-bearing to week 4; progress 25% body weight per week | Gentle active-assisted ROM from week 4 (plantar/dorsiflexion in the boot); avoid inversion; start with a 10–15° arc | | 3 | 6–12 weeks | Full weight-bearing in the boot by week 6; wean to a supportive shoe by week 8 if ROM is adequate and pain controlled | Progressive active ROM in all planes (full dorsiflexion/plantarflexion by week 8); isometric then resistance-band peroneal strengthening; proprioception from week 8 | | 4 | 3–6 months | Lace-up ankle brace for sport initially (3–6 months), weaned as confidence builds | Plyometrics, cutting and figure-8 drills, sport-specific training; return to sport at 4–6 months once peroneal strength is greater than 85% and the single-leg hop is greater than 90% of the other side | Good-to-excellent results are reported in the large majority after anatomic SPR repair, with the AOFAS hindfoot score typically improving from the high 50s into the low 90s (Cho 2014, Raikin 2009, Hu and Xu 2018). A minority have residual symptoms (mild pain, scar tenderness, subjective instability), and most athletes return to sport around 3–6 months depending on the procedure performed. Complications
- Recognition
- Numbness over the lateral foot or 5th toe, dysesthesia, a painful neuroma, a positive Tinel over the nerve
- Prevention
- Early identification with vessel loops; keep the incision along the tendon course (not too posterior); gentle retraction; minimal cautery near the nerve
- Management
- Most are neuropraxia — observe 3–6 months; desensitisation; neuroma excision with burial in muscle; primary repair if clearly divided
- Recognition
- Return of lateral pain with activity, palpable or visible subluxation on eversion, a snapping sensation, MRI showing a failed SPR
- Prevention
- Robust SPR repair or reconstruction (the key step); adequate groove deepening if indicated; repair with the ankle in slight eversion; 6–8 weeks of post-op protection
- Management
- Revision surgery if symptomatic — reassess groove depth, augment the SPR with an Achilles strip or allograft, consider a bone-block procedure, address compliance
- Recognition
- Wound-edge necrosis (usually less than 1 cm), healing delayed beyond 3 weeks, erythema or purulent drainage if infected
- Prevention
- Full-thickness skin flaps; avoid excessive retraction; meticulous hemostasis to prevent haematoma; tension-free closure; compression dressing
- Management
- Local wound care for small areas; debridement if necrosis is greater than 1 cm; antibiotics only for clinical infection; VAC or skin graft for larger defects
- Recognition
- Reduced dorsiflexion or plantarflexion, difficulty with stairs and inclines, end-range pain; develops during immobilisation
- Prevention
- Immobilise in neutral dorsiflexion; early ROM at 6 weeks; avoid immobilisation beyond 8 weeks; structured physiotherapy
- Management
- Progressive physiotherapy (ROM and stretching); night splint if equinus is developing; manipulation under anaesthesia if severe (rare); usually improves by 3–6 months
- Recognition
- A crack or pop during burring with a visible fracture line; delayed sudden pain, swelling and inability to weight-bear
- Prevention
- Maintain 3–4 mm of anterior cortex; palpate frequently during deepening; limit deepening to 3–5 mm; smooth controlled burring; consider fluoroscopy
- Management
- Stable and non-displaced: CAM boot non-weight-bearing 6–8 weeks; displaced: ORIF with a lateral plate; delay weight-bearing until union (8–12 weeks)
- Recognition
- Reduced eversion strength, difficulty on uneven surfaces, subjective lateral instability, a lateral foot slap
- Prevention
- Preserve tendon substance (avoid over-resection); adequate tendon repair; early protected ROM at 6 weeks; structured strengthening at 8–12 weeks; avoid over-tightening the SPR
- Management
- Progressive peroneal strengthening physiotherapy; proprioception and balance training; an ankle brace for activities initially; usually improves over 6–12 months
- Recognition
- Disproportionate pain, swelling, temperature and colour changes, allodynia, hair and nail changes; diagnose by Budapest criteria
- Prevention
- Minimise surgical trauma; excellent hemostasis; early mobilisation when appropriate; adequate analgesia; vitamin C (conflicting evidence)
- Management
- Early aggressive physiotherapy (most important); desensitisation; neuropathic agents (gabapentin, pregabalin); sympathetic blocks if severe; multidisciplinary care; majority improve over 6–12 months
Risk-factor mitigation. Patient factors driving wound and nerve complications include diabetes (wound complications around 15% versus 5%), smoking (around 12% versus 5%), obesity, neuropathy and prior lateral ankle surgery (which roughly doubles the sural nerve injury risk). The surgical drivers of failure are an inadequate SPR repair, a poorly placed incision (too posterior risks the nerve, too anterior compromises exposure), perforation or fracture from excessive groove deepening, and a haematoma from poor hemostasis. Red flags requiring urgent assessment
- Sudden increase in pain with swelling — fracture, DVT or infection
- Fever, wound drainage or increasing erythema — infection
- A palpable or visible tendon subluxation — repair failure
- Disproportionate pain, colour changes or allodynia — CRPS
- Calf swelling, tenderness or a positive Homan sign — DVT
- Worsening numbness or paraesthesia — nerve injury Follow-up
- 6 weeks — clinical review plus radiographs if groove deepening was performed
- 3 months — assess ROM and strength; plan return to activity
- 6 months — functional assessment and return-to-sport clearance
- 1 year — final outcome assessment and patient satisfaction
Viva & Exam Focus
BREVISBREVIS — peroneus brevis anatomy
GROOVEGROOVE — selective deepening technique
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old netball player presents with recurrent lateral ankle pain and a snapping sensation. MRI shows peroneal tendon subluxation and a longitudinal tear of peroneus brevis. How would you manage this?”
“What is the anatomy of the peroneal tendons and the superior peroneal retinaculum? Why is the SPR critical for preventing subluxation?”
“You are performing groove deepening and suddenly feel the burr break through. What has happened and how do you manage it?”
Indications
- Recurrent subluxation or dislocation with documented SPR insufficiency
- Symptomatic longitudinal tear greater than 50% width after 3–6 months of failed conservative care
- Acute complete SPR rupture in a high-demand athlete or military personnel
- Chronic tenosynovitis refractory to conservative management
- A shallow (less than 5 mm) flat or convex groove with symptomatic subluxation
Key anatomy
- Brevis: ANTERIOR, inserts at the 5th MT base — at risk for the C-shaped tear from compression between longus and fibula
- Longus: POSTERIOR, courses under the foot to the 1st MT base and medial cuneiform — check the os peroneum
- SPR: PRIMARY restraint, from the posterior fibular ridge to the lateral calcaneus; torn or attenuated in chronic subluxation
- Sural nerve: crosses the posterolateral ankle close to the tendons, highly variable — the MOST at-risk structure
- Groove: a deep concave groove buttresses the tendons; a flat or convex groove is the mechanical risk factor
Critical steps
- Lateral decubitus (or supine with a bump), thigh tourniquet, mark a 6–8 cm incision posterior to the fibula
- Curvilinear incision 4 cm proximal to 2–4 cm distal to the lateral malleolus — identify the sural nerve EARLY with vessel loops
- Longitudinal SPR incision creating superior and inferior flaps; expose brevis (anterior) and longus (posterior)
- Dynamic assessment of tears, tenosynovitis and subluxation; test groove depth and SPR competence
- Tendon repair: less than 50% tubularize; greater than 50% side-to-side or allograft; greater than 75% tenodesis or transfer; thorough synovectomy
- Groove deepening: 3–5 mm deeper, maintain 3–4 mm of anterior cortex, smooth the edges, palpate frequently
- SPR reconstruction: bone-tunnel technique, advance posteriorly, secure with anchors, repair in neutral dorsiflexion and slight eversion
- Dynamic stability test before closure — tendons must track in the groove through full ROM without subluxation
Danger zones
- Sural nerve: highly variable, no reliable landmark — identify early and protect with vessel loops throughout
- Lesser saphenous vein: runs with the sural nerve — control with bipolar, preserve flap vascularity
- Lateral ankle skin: thin, limited vascularity — full-thickness flaps, tension-free closure
- Anterior fibular cortex: during deepening — maintain 3–4 mm, palpate every 30–60 seconds
- Calcaneofibular ligament: deep to the tendons distally — avoid excessive distal dissection
Technique pearls
- Brevis is ANTERIOR, longus is POSTERIOR — brevis is at highest risk for the C-shaped tear
- SPR repair is the critical step — anatomic retinacular repair alone reliably controls dislocation
- Groove deepening is selective (flat or convex groove), not routine — 3–5 mm deeper, 3–4 mm cortex preserved
- Bone-tunnel SPR technique: 1 cm proximal to the fibula tip, advance posteriorly, robust anchor fixation
- Repair position: neutral dorsiflexion plus slight eversion (5–10°) to offload the SPR
- Dynamic intra-op test: full ROM must not sublux the tendons
- Immobilise in a CAM boot in slight eversion, non-weight-bearing 4 weeks (longer if groove deepening)
Complications
- Sural nerve injury (5–10%) — most common; usually a transient neuropraxia resolving by 3–6 months
- Recurrent subluxation (5–15%) — from an inadequate SPR repair; revision needs augmentation plus or minus a bone block
- Wound complications (5–8%) — thin skin; full-thickness flaps and tension-free closure
- Ankle stiffness (10–20%) — immobilise in neutral dorsiflexion, early ROM at 6 weeks
- Iatrogenic fibular fracture (less than 2%) — ORIF if displaced, extended non-weight-bearing if stable
- Peroneal weakness (5–8%) — preserve tendon substance; improves over 6–12 months
- CRPS (1–3%) — early physiotherapy, desensitisation, neuropathic agents
Post-op protocol
- Week 0–2: non-weight-bearing in a CAM boot or splint (slight eversion, neutral dorsiflexion); elevate, ice; sutures out at 10–14 days
- Week 2–4: non-weight-bearing if groove deepening; may start partial weight-bearing if tendon repair only; gentle ROM from week 4
- Week 4–6: progress to partial then full weight-bearing in the boot; active-assisted ROM (avoid forceful inversion)
- Week 6–12: full weight-bearing, wean from the boot at week 8; begin peroneal strengthening and proprioception
- Month 3–6: sport-specific training; return to sport at 4–6 months (strength greater than 85%, hop greater than 90%)
- Follow-up: 6 weeks (clinical plus or minus XR), 3 months (ROM/strength), 6 months (RTS), 1 year (final)
Exam tips
- 'The SPR is the indispensable restraint — I always restore it anatomically; I reserve groove deepening for a flat or convex groove'
- 'The sural nerve is my first priority after skin incision — I identify it early and protect it with vessel loops throughout'
- 'For groove deepening I maintain 3–4 mm of anterior cortex by frequently palpating the lateral fibular surface'
- 'I prefer a bone-tunnel or anchor SPR reattachment to restore the retinaculum to its fibular footprint'
- Evidence: SPR repair with versus without groove deepening gave EQUIVALENT outcomes (Cho 2014, Level II)
- Classification: Eckert-Davis grades I–III of acute SPR injury (grade III is a bony avulsion of the posterolateral fibula)
- Sural nerve symptoms are the most commonly reported complication (usually transient); recurrent dislocation from an inadequate SPR repair is the key surgical failure
Background & Evidence
Pathoanatomy. Peroneal tendon disorders — tendinosis, longitudinal tears, subluxation or dislocation, and a painful os peroneum — are strongly associated with hindfoot varus, chronic lateral ligament instability, an enlarged peroneal tubercle and a low-lying peroneus brevis muscle belly, all of which should be sought and corrected to prevent recurrence (Roster 2015). In the retromalleolar groove the brevis sits anterior and the longus posterior; the brevis is compressed between the longus and the fibula, which is why it carries the classic C-shaped longitudinal split. The superior peroneal retinaculum is the primary restraint, running from the posterior fibular ridge to the lateral calcaneus, and a flat or convex retromalleolar groove reduces the bony buttress and predisposes to subluxation. Eckert-Davis classification of acute SPR injury. Acute injury is graded by the integrity of the SPR and its fibular attachment — the lesion you must address at operation.
- Pathology
- SPR stripped off the lateral fibula with an elevated periosteal sleeve; tendons dislocate into the pocket — the most common grade
- Implication
- Soft-tissue repair or reattachment of the SPR-periosteal sleeve
- Pathology
- Distal fibrocartilaginous ridge (rim) elevated together with the retinaculum
- Implication
- Reattach the retinaculum and rim to the fibula
- Pathology
- Cortical avulsion fracture of the posterolateral fibula attached to the retinaculum
- Implication
- Reduce and fix the bony fragment (seen on the mortise view or axial CT)
Intrasheath subluxation. Raikin (2009) defined intrasheath subluxation — painful snapping with an INTACT retinaculum, missed on static imaging and diagnosed on dynamic ultrasound. Type A: the tendons switch their relative position within the sheath; Type B: the longus subluxes through a longitudinal split in the brevis. Of his 14 patients, 13 had a convex (not concave) groove intra-operatively, and this is the one clear indication in which groove deepening (with retinacular reefing) is the primary corrective step. What the evidence actually shows
- The SPR is the indispensable restraint. Anatomic SPR repair or reattachment alone gives good-to-excellent results and low recurrence (Cho 2014, Park 2021); the older claim that groove deepening alone is curative is not supported.
- Groove deepening is an adjunct, not a default — indicated chiefly for a flat or convex (shallow) groove, or for intrasheath subluxation with a convex groove (Raikin 2009). Adding it to SPR repair did not improve scores in the one comparative trial and lengthened operating time (Cho 2014).
- Concomitant tears need an algorithm, not a single technique (Redfern and Myerson 2004), and coexisting hindfoot varus, lateral instability or a prominent peroneal tubercle must be corrected (Roster 2015). Outcome benchmarks. The AOFAS hindfoot score typically improves from the high 50s pre-operatively into the low 90s post-operatively (Cho 2014, Raikin 2009, Hu and Xu 2018). Recurrent dislocation after anatomic SPR repair is low (single-digit percentages in the reattachment series), and most failures are re-injuries (Park 2021). Sural nerve symptoms are the most frequently reported complication and are usually a transient neuropraxia (Park 2021, Roster 2015). Guidelines, registries & global practice
- No high-level society guideline (AAOS, BOA/BOFAS, AOFAS, EFORT) mandates a single technique, and there is no implant registry for this soft-tissue procedure; practice follows the evidence above.
- Groove deepening, yes or no — many UK/European (BOFAS-aligned) and Asian centres favour SPR repair alone for a normal-depth groove and reserve deepening for a flat or convex groove, while some North American practice deepens more liberally. The comparative evidence (Cho 2014) supports the selective approach.
- Open versus tendoscopic deepening — tendoscopic deepening and SPR procedures are increasingly used in specialist centres; reported outcomes are comparable but the evidence remains lower level.
- Acute primary repair — for an acute Eckert-Davis grade injury in a high-demand athlete, early operative repair is widely favoured over non-operative cast treatment because non-operative management carries a high redislocation rate.
References
Acute rupture of the peroneal retinaculum
- Operative series of 73 acute superior peroneal retinaculum (SPR) injuries defining the still-used three-grade classification
- Grade I: SPR with periosteum elevated or stripped off the lateral fibula (tendons dislocate into the pocket) — most common
- Grade II: distal fibrocartilaginous ridge (rim) elevated with the retinaculum
- Grade III: cortical avulsion fracture of the posterolateral fibula attached to the retinaculum
- Surgical repair was successful in all but three cases
Comparison of outcome after retinaculum repair with and without fibular groove deepening for recurrent dislocation of the peroneal tendons
- Prospective comparative study of 29 patients with recurrent traumatic dislocation: 13 SPR repair plus groove deepening (group A) versus 16 SPR repair alone (group B)
- AOFAS improved 59.3 to 92.2 (group A) and 58.5 to 91.3 (group B) — no significant difference between groups
- VAS and time to return to sport (about 3 months) were equivalent; tourniquet time was significantly shorter without deepening (29.5 versus 42.2 min)
- Both techniques gave good outcomes for recurrent traumatic dislocation
Treatment of recurrent peroneal tendon dislocation by peroneal retinaculum reattachment without fibular groove deepening
- 36 patients with recurrent dislocation treated by anatomic SPR reattachment alone
- 34 of 36 fully recovered with no re-subluxation; the 2 failures were re-injuries during sport
- No evertor weakness and no loss of ankle motion; one transient sural nerve injury that resolved by 6 months
- AOFAS, VAS and Foot Function Index all improved significantly
Intrasheath subluxation of the peroneal tendons
- Defined intrasheath subluxation: painful snapping with an INTACT retinaculum, diagnosed on dynamic ultrasound
- Type A — tendons switch their relative position within the sheath; Type B — longus subluxates through a longitudinal split in brevis
- 14 patients treated by groove deepening with retinacular reefing; mean AOFAS improved 61 to 93 and VAS 6.8 to 1.2 at mean 33 months
- 13 of 14 had a convex (not concave) retromalleolar groove intra-operatively
The management of concomitant tears of the peroneus longus and brevis tendons
- 28 patients (29 feet) with combined longus and brevis tears, mean follow-up 4.6 years
- Proposed a treatment algorithm based on whether one usable tendon remains, excursion of the proximal muscle, and ankle or hindfoot alignment
- Mean postoperative AOFAS 82; 91% regained normal or moderate peroneal strength; instability corrected in all
- Severe loss with no usable tendon and no proximal excursion may require tenodesis, allograft, or staged grafting rather than direct repair
Treatment of chronic subluxation of the peroneal tendons using a modified posteromedial groove deepening technique
- 21 patients treated with a posteromedial osteocartilaginous-flap deepening that preserves the lateral edge of the groove
- AOFAS improved from 55.0 to 93.6 with no recurrent subluxation
- Demonstrates a soft-tissue-sparing deepening alternative to lateral burring
Anatomy of the sural nerve and its relation to the Achilles tendon
- Cadaveric study of 30 limbs
- Sural nerve lay a mean 18.8 mm from the lateral border of the Achilles tendon at the calcaneal insertion
- It crossed lateral to the Achilles tendon about 9.8 cm proximally, with significant individual variation
The peroneal tubercle: description, classification, and relevance to peroneus longus tendon pathology
- Study of 114 calcanei
- The peroneal tubercle was present in 90% and classified as flat, prominent, concave or tunnel
- A prominent tubercle is implicated in peroneus longus tendinopathy and os peroneum pathology
Split lesions of the peroneus brevis tendon in chronic ankle laxity
- Demonstrated that a neglected peroneus brevis split tear is a cause of residual posterolateral pain after ligament surgery
Peroneal tendon injuries: an evaluation of 49 tears in 41 patients
- Prospective surgical series of 49 tears in 41 patients
- Mean AOFAS improved from 52 to 90
- No significant difference in outcome between longus, brevis and combined tears
Peroneal tendon disorders
- Narrative review of the full spectrum of peroneal tendon disorders (tendinosis, tears, subluxation or dislocation, painful os peroneum)
- Strong association with hindfoot varus, lateral ligament instability, an enlarged peroneal tubercle and a low-lying peroneus brevis muscle belly