Prone position | Sural nerve at risk | Posterior malleolus and pilon access
- Prone positioning is essential — the posterior malleolus and posterior tibial plafond cannot be reached directly supine.
- The sural nerve and short saphenous vein run together in the subcutaneous plane of this interval and must be identified and protected before any deep dissection.
- The deep internervous plane lies between the peroneal tendons (superficial peroneal nerve) laterally and flexor hallucis longus (tibial nerve) medially.
- The posterior tibial neurovascular bundle lies medial to FHL — all dissection stays lateral to the FHL tendon to protect it.
- Direct buttress plating of the posterior malleolus prevents posterior talar subluxation and restores posterior column stability.
When & Why
What it exposes. The posterolateral approach gives direct access to the posterior malleolus, the posterior tibial plafond and the distal fibula in the prone position. It is the workhorse exposure for posterior malleolar fixation, posterior pilon fragments and combined fibular-plus-posterior plating in trimalleolar injuries. When to use it. Indications are a posterior malleolar fragment involving greater than 25 percent of the articular surface or with greater than 2 mm of articular step-off, large posterior pilon fragments extending into the metaphysis, and trimalleolar patterns where the fibula and posterior malleolus can be fixed through a single interval. Posterior malleolar fixation restores the posterior tibial buttress, reduces posterior talar instability and improves outcomes. Approach variants. Three patterns cover most cases: the standard posterolateral incision (between peronei and FHL) for most posterior malleolar fractures; an extended proximal incision along the posterior fibula for high-energy posterior pilon fragments; and a combined incision used for both posterior malleolar and fibular plating in trimalleolar fractures. Position & landmarks. Prone on a radiolucent table with full C-arm access from both medial and lateral sides, all pressure points padded, the affected ankle in slight plantarflexion over a bolster and the foot overhanging the table end. Palpate the lateral malleolus (lateral boundary), the Achilles tendon (medial boundary), the posterior calcaneal tuberosity and the distal fibular shaft. The incision runs midway between the lateral malleolus and the Achilles tendon, typically 8 to 12 cm and centred over the posterior malleolus or fracture site.
Prone positioning gives true direct visualisation of the posterior plafond and malleolus and allows buttress plating. In trimalleolar fractures the same posterolateral incision can often carry both the posterior malleolar buttress plate and the lateral fibular plate, avoiding a second incision and its skin bridge — provided the soft-tissue envelope allows it.
The Exposure
Work from prone positioning down through the interval between the peroneal tendons and flexor hallucis longus, protecting the sural nerve superficially and the posterior tibial neurovascular bundle deep, to expose and buttress-plate the posterior malleolus.
Exposure sequence
- Prone is mandatory — the posterior malleolus and posterior tibial plafond cannot be reached directly supine. Confirm the patient is fit for prone (no cervical spine injury, cardiovascular stability).
- Use chest rolls or a Wilson frame; pad every pressure point — face, chest, pelvis, patellae, ankles and toes. Position arms with shoulders abducted less than 90 degrees and elbows flexed.
- Place the affected ankle in slight plantarflexion over a padded bolster to relax the posterior structures, with the foot overhanging the table end to allow free dorsiflexion and plantarflexion during reduction. Slight knee flexion relaxes the gastrocnemius-soleus complex.
- Confirm a radiolucent table with full C-arm access from both sides. A high-thigh tourniquet is optional — consider tourniquet-free surgery if vascular assessment is needed.
- Alternative: lateral decubitus with the affected side up allows combined posterolateral and anterolateral access without repositioning, at the cost of some posterior exposure.
- Draw a longitudinal incision exactly midway between the lateral malleolus and the Achilles tendon, 8 to 12 cm long and centred over the posterior malleolus or fracture site.
- Use the bony landmarks for orientation — lateral malleolus (lateral boundary), Achilles tendon (medial boundary), posterior calcaneal tuberosity (distal) and distal fibular shaft (proximal).
- Precise midline placement matters: too far lateral risks the peroneal tendons, too far medial risks the Achilles. The sural nerve lies in the midline of this interval and is most vulnerable during the initial skin incision.
- Plan extension now — proximally along the posterior border of the fibula for combined fibular plating or posterior pilon access, distally toward the calcaneus if posterior subtalar access is needed.
- Incise the skin midway between the lateral malleolus and the Achilles, carrying dissection through subcutaneous fat with careful bipolar haemostasis to keep a dry field.
- Identify the sural nerve and short saphenous vein together in the subcutaneous plane — they run in the midline of the interval and must be found before deepening the dissection. In thin patients the nerve may be visible or transilluminable running with the vein.
- Protect the nerve with a vessel loop or gentle Penrose retraction. Do not skeletonise it or stretch it. Once identified, use blunt Metzenbaum dissection in the plane immediately superficial to the deep fascia.
- The sural nerve (sensory to the lateral foot, fifth toe and dorsolateral ankle) is the structure most commonly injured in this approach — injury causes numbness and a painful neuroma. Distal extension may divide lateral calcaneal branches and cause heel numbness.
- After protecting the sural nerve, incise the deep fascia in line with the skin incision.
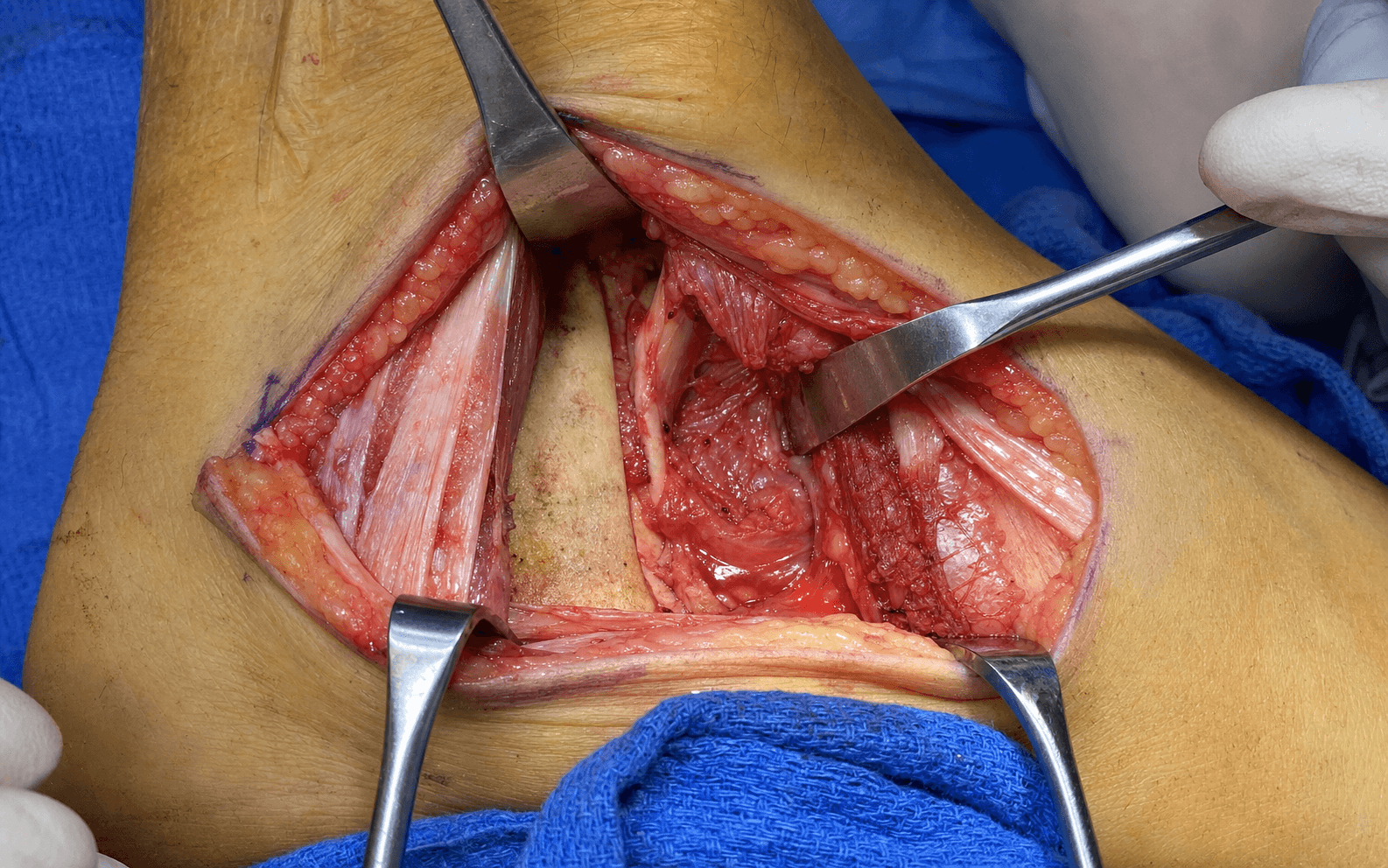
- Identify the peroneal tendon sheath laterally and the flexor hallucis longus muscle belly medially, then develop the plane between the peroneal tendons and the FHL belly with blunt dissection.
- This is a true internervous plane — peroneus brevis (superficial peroneal nerve) laterally and FHL (tibial nerve) medially. Both muscles are retracted rather than divided, minimising denervation risk: the peroneal compartment is retracted laterally and the FHL medially.
- Confirm the FHL belly by its characteristic bipennate appearance and by flexing the great toe.
- Retract the FHL medially. The posterior tibial neurovascular bundle lies medial to FHL, so stay strictly lateral to the FHL tendon at all times — this is the fundamental safety principle of the approach.
- Subperiosteal elevation of the posterior capsule and periosteum exposes the posterior malleolus and the posterior tibial plafond.
- For posterior pilon fragments, extend proximally between the peroneal muscles and the FHL origin on the fibula to reach metaphyseal extension. The FHL muscle belly is the indicator of proximity to the neurovascular bundle.
- The posterior fragment is often reduced indirectly by ligamentotaxis with dorsiflexion and an anterior drawer force on the talus; direct visualisation then confirms reduction and lets you remove any interposed soft tissue or osteochondral debris.
- For depressed fragments, use a bone tamp through the fracture line or a separate cortical window. Hold reduction with provisional K-wires.
- Apply a buttress plate (3.5 mm reconstruction plate or anatomic posterior malleolar plate) to the posterior surface, with screws directed anteriorly to capture the fragment and engage the anterior cortex. Small peripheral fragments may be fixed with posterior-to-anterior cannulated screws; posterior pilon variants need longer buttress plates extending proximally into the metaphysis. Confirm reduction with fluoroscopy, accepting less than 2 mm of articular step-off.
- Close in layers — copious saline irrigation and meticulous haemostasis, the deep fascia loosely to avoid compartment syndrome, subcutaneous tissue approximated carefully around the sural nerve to prevent entrapment, and skin with interrupted non-absorbable sutures or staples. Apply a well-padded posterior splint with the ankle in neutral dorsiflexion.
The sural nerve is the commonest structure injured in this approach; it runs with the short saphenous vein in the midline of the interval, only millimetres deep, so it is most at risk during the initial incision. Identify and loop it before any deep dissection. Deeply, the posterior tibial neurovascular bundle lies medial to FHL — staying lateral to the FHL tendon at every step is what keeps that bundle safe.
The flexor hallucis longus muscle belly is the landmark that tells you where the posterior tibial neurovascular bundle is. Because the bundle lies medial to FHL, retracting FHL medially and staying lateral to it exposes the posterior malleolus while keeping the bundle protected.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Sural nerve and short saphenous vein (midline of interval)
- Protection
- Identify before deepening; vessel loop; gentle retraction; never skeletonise
- Structure at risk
- Posterior tibial neurovascular bundle (medial to FHL)
- Protection
- Stay lateral to FHL at all times; retract FHL medially
- Structure at risk
- Peroneal artery branches
- Protection
- Ligate small branches if encountered; preserve the major vessels
- Structure at risk
- Posterior capsule and deltoid ligament
- Protection
- Protect during reduction; repair if possible for stability
Extensile options. Extend proximally along the posterior border of the fibula to reach the metaphyseal extension of posterior pilon fragments or to carry fibular plating through the same interval. Extend distally toward the calcaneus for posterior subtalar joint access — this risks the lateral calcaneal branches of the sural nerve (heel numbness). For trimalleolar fractures the same posterolateral incision can carry both posterior malleolar and lateral fibular plating, so plan the skin bridge carefully. Closure and aftercare. Irrigate copiously, achieve meticulous haemostasis, close the deep fascia loosely to avoid compartment syndrome, approximate subcutaneous tissue carefully around the sural nerve, and close skin with interrupted sutures or staples. Apply a well-padded posterior splint with the ankle in neutral dorsiflexion. Strict elevation for 48 to 72 hours, non-weight-bearing for 6 to 12 weeks depending on fixation stability and fracture pattern, early ankle range-of-motion exercises once the wound is stable, and serial radiographs to assess union and talar position.
Procedures Through This Approach
- Ankle fracture ORIF — trimalleolar — posterior malleolar buttress plating, often combined with fibular plating through the same incision.
- Pilon ORIF — fixation of large posterior pilon fragments extending into the metaphysis.
- Combined fibular and posterior plating in trimalleolar injuries, via the proximal extension along the posterior fibula.
- Reconstruction of the posterior tibial plafond and access to posterior talar body fragments.
Viva & Exam Focus
POSTEROLATPOSTEROLATERAL ANKLE — surgical steps
DANGERDANGER structures — layer by layer
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old presents with a trimalleolar ankle fracture after a fall from height. CT shows a posterior malleolar fragment involving 35 percent of the plafond with 3 mm of step-off. How would you approach the posterior fragment?”
“A 35-year-old polytrauma patient has a high-energy pilon fracture with a large posterior fragment extending into the metaphysis. CT shows the fragment involves 40 percent of the plafond. How would you plan surgical access?”
“Following a posterolateral approach for posterior malleolar fixation, the patient reports numbness on the lateral border of the foot and a painful tingling sensation. What is your assessment and management?”
Patient position
- Prone position is mandatory for direct posterior access
- Pad all pressure points — face, chest, pelvis, knees, ankles, toes
- Affected ankle slightly plantarflexed over a padded bolster
- Radiolucent table with C-arm access from both medial and lateral sides
- Tourniquet optional — consider tourniquet-free for vascular assessment
Incision and superficial dissection
- Incision midway between the lateral malleolus and the Achilles tendon
- Length 8 to 12 cm centred over the posterior malleolus
- Identify the sural nerve and short saphenous vein in the subcutaneous fat
- Protect the sural nerve with a vessel loop — the most commonly injured structure
- Do not skeletonise the nerve excessively
Deep internervous plane
- Between peroneus brevis (superficial peroneal nerve) laterally and FHL (tibial nerve) medially
- A true internervous plane — retract rather than divide
- FHL is the critical deep landmark — identified by great-toe flexion
- Stay lateral to FHL throughout — the bundle is medial to FHL
- Elevate FHL medially to expose the posterior plafond
Danger structures
- Superficial: sural nerve and short saphenous vein
- Deep: posterior tibial neurovascular bundle (medial to FHL)
- Peroneal artery branches may require ligation
- Posterior capsule — protect during reduction
- Lateral calcaneal nerve branches with distal extension
Fixation principles
- A buttress plate on the posterior surface prevents posterior talar subluxation
- Screws directed anteriorly to capture the fragment
- Accept less than 2 mm of articular step-off
- Bone-graft metaphyseal voids in pilon variants
- Combined lateral plating is possible through the same approach for trimalleolar fractures
Closure and aftercare
- Loose fascial closure to avoid compartment syndrome
- Careful subcutaneous approximation around the sural nerve
- Posterior splint with the ankle neutral
- Elevation for 48 to 72 hours
- Non-weight-bearing for 6 to 12 weeks
References
Application of the posterolateral approach in the surgical treatment of ankle fractures
- The posterolateral approach provides direct visualisation and improved reduction quality for posterior malleolar fragments in ankle fractures
Modified posterolateral approach to the ankle: a novel approach to minimise soft tissue dissection
- The modified posterolateral approach minimises soft tissue dissection while preserving safe access to the posterior malleolus and tibial plafond
Posterolateral versus posteromedial approach for posterior malleolus fixation in trimalleolar fractures of the ankle
- The posterolateral approach for posterior malleolus fixation in trimalleolar fractures provides excellent visualisation with outcomes comparable to the posteromedial approach
Posterior plating via the posterolateral approach for posterior malleolar fractures: effect on flexor hallucis longus morphology and function — a cohort study
- Posterior plating via the posterolateral approach for posterior malleolar fractures allows safe FHL preservation with good functional outcomes