Oblique Incisions | NV Bundle Protection | Flexor Sheath Exposure
- Zigzag crosses flexion creases obliquely at 45 to 60 degrees with apices at the mid-axial line to prevent scar contracture
- Digital neurovascular bundles lie on each side of the flexor sheath and must be identified and protected from the start
- Preserve A2 and A4 pulleys to prevent bowstringing after flexor tendon repair
- Raise full-thickness skin flaps preserving the subdermal plexus for reliable wound healing
- No true internervous plane exists; dissection stays between the paired digital neurovascular bundles
When & Why
What it exposes. The Bruner volar zigzag approach gives extensile, safe exposure of the entire flexor tendon sheath and the digital neurovascular structures from the distal palm to the fingertip. It is the workhorse exposure for zone 2 flexor tendon repair, pulley reconstruction, selected digital fractures and drainage of flexor sheath infections. Primary indications:
- Zone 2 flexor tendon repair (the most common indication)
- Flexor tendon grafting or staged reconstruction
- A2 or A4 pulley reconstruction
- Digital phalangeal fracture fixation via a volar approach
- Flexor sheath infection drainage (pyogenic flexor tenosynovitis)
- Trigger finger release requiring extensive sheath exposure
- Volar plate repair or reconstruction Why this approach. The zigzag provides wide, extensile exposure of the flexor apparatus while minimising scar contracture across flexion creases. The oblique crossing of each crease allows broad flap elevation and access to both neurovascular bundles. It is preferred over the mid-axial approach whenever extensive volar work or bilateral neurovascular protection is required. Approach variants:
- Standard Bruner — a zigzag crossing the creases with mid-axial apices, used for most flexor tendon and sheath procedures.
- Extended proximal — continued into the palm or wrist, for combined zone 1 to 3 exposure.
- Limited window — fewer zigzags for focal exposure in selected pulley or fracture cases. Contraindications:
- Active infection with skin involvement over the planned incision
- Severe digital swelling precluding safe closure
- Previous volar scars that would compromise flap vascularity
- Isolated dorsal pathology that is better approached dorsally Alternative approaches:
- Mid-axial approach — a straight lateral incision along the mid-axial line elevating a single flap; it avoids crossing creases but gives poorer volar exposure, risks dorsal displacement of the neurovascular bundle, and is less versatile for extensive tendon or sheath work.
- Volar transverse incisions — limited exposure with a higher contracture risk.
- Combined approaches — for complex multi-structure injuries.
The Exposure
The approach works a safe corridor to the flexor sheath that lies between the paired radial and ulnar digital neurovascular bundles. Work proceeds from the skin zigzag through full-thickness flaps to the sheath, then between pulleys.
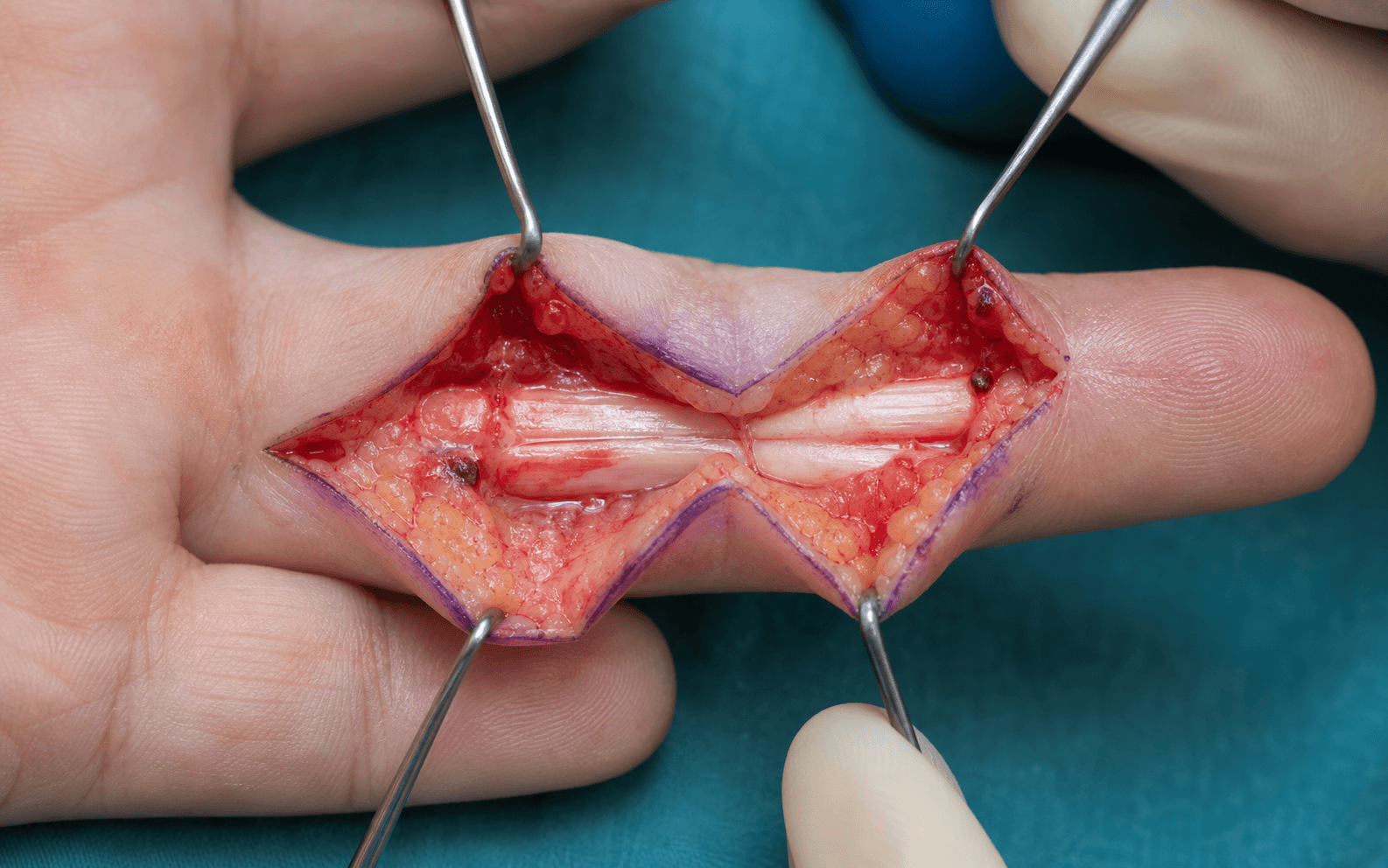
Anatomy. The finger is built around the proximal, middle and distal phalanges; the flexion creases overlie the PIP and DIP joints, and the mid-axial line runs along the lateral aspect of each phalanx, equidistant from the volar and dorsal surfaces. The flexor apparatus comprises FDS (inserting on the middle phalanx) and FDP (inserting on the distal phalanx), constrained by five annular pulleys (A1 to A5) and three cruciate pulleys (C1 to C3). A2 (over the proximal phalanx) and A4 (over the middle phalanx) are biomechanically critical and prevent bowstringing; A1 overlies the MCP joint, A3 the PIP and A5 the DIP. Each digit carries paired radial and ulnar digital arteries and nerves running along the sides of the sheath, just volar to the mid-axial line, with the nerve lying dorsal to the artery; the common digital arteries bifurcate at the web spaces. The volar skin is thick with dense fibrous septa, and the subdermal vascular plexus lies immediately deep to the dermis, so it must be preserved by raising full-thickness flaps. Internervous plane. There is no true internervous plane. Dissection proceeds between the paired digital neurovascular bundles, which define the safe corridor to the flexor sheath; the bundles are the structures to be protected, not crossed.
The Bruner approach is defined by staying between the paired digital neurovascular bundles rather than between muscles of different nerve supply. The critical technical step is early identification and protection of both bundles before any deep work on the flexor sheath.
Exposure sequence
- Supine with the hand on a hand table; upper-arm tourniquet to about 250 mmHg after Esmarch exsanguination; loupe magnification (2.5x minimum) is mandatory throughout.
- Shoulder abducted 90 degrees, elbow extended or slightly flexed, palm up with the digits in comfortable extension; an assistant or lead hand (finger traps if needed) maintains position.
- Mark the mid-axial line on the radial and ulnar sides of each phalanx and the flexion creases at the MCP, PIP and DIP joints.
- Plan zigzag limbs crossing each crease at 45 to 60 degrees, with each apex precisely on the mid-axial mark; limbs are about 1.5 to 2 cm long.
- Extend proximally into the palm with a Y-shaped limb at the distal palmar crease when zone 2 to 3 continuity is needed.
- Equipment: fine Adson or skin hooks, bipolar diathermy, vessel loops, a 15 blade and fine tenotomy scissors.
- Incise the skin along the marked zigzag with a 15 blade.
- Divide the subcutaneous tissue carefully to avoid damaging the subdermal plexus.
- Raise full-thickness radial and ulnar skin flaps down to the flexor sheath, preserving the subdermal vascular plexus on the deep surface of the dermis; thin flaps or over-undermining devascularise the skin edges.
- Identify both the radial and ulnar digital neurovascular bundles at the margins of the exposure before any deep dissection.
- Place a vessel loop around each bundle for gentle retraction and protection; remember the nerve lies dorsal to the artery.
- Use loupe magnification and bipolar haemostasis throughout.
- Expose the flexor sheath from the A1 pulley proximally to the A5 pulley distally.
- Identify the flexor tendons within the sheath (FDS to the middle phalanx, FDP to the distal phalanx).
- Preserve the A2 pulley (over the proximal phalanx) and the A4 pulley (over the middle phalanx) whenever possible.
- Divide A1, A3 or A5 as required for exposure or therapeutic release, for example trigger finger.
- Open the sheath between the pulleys to access the tendons for repair or grafting.
- Irrigate thoroughly and achieve haemostasis with bipolar diathermy.
- Close the skin with fine (5-0 or 6-0) nylon or absorbable sutures, using simple interrupted or everting mattress sutures to prevent inversion; avoid tension on the wound edges.
- Apply a light compressive dressing with the digit exposed for monitoring.
Keep tourniquet time under 120 minutes when possible. Loupe magnification is mandatory for safe identification of the digital neurovascular bundles; poor lighting or inadequate magnification increases the risk of iatrogenic nerve or vessel injury.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Subdermal vascular plexus
- Protection
- Raise full-thickness flaps only; stay immediately deep to the dermis
- Structure at risk
- Digital arteries (volar to nerves)
- Protection
- Identify early; gentle retraction; loupe magnification
- Structure at risk
- Digital nerves (dorsal to arteries)
- Protection
- Vessel-loop protection; avoid excessive stretch
- Structure at risk
- Flexor tendons and A2/A4 pulleys
- Protection
- Preserve A2 (proximal phalanx) and A4 (middle phalanx); reconstruct if sacrificed
- Structure at risk
- Volar plate at PIP and DIP
- Protection
- Limit dissection to what is strictly necessary
Extensile options. Extend proximally by continuing the zigzag into the palm with a Y-shaped limb at the distal palmar crease for zone 2 to 3 access, taking care to protect the common digital vessels and nerves. Extend distally to the fingertip when distal FDP repair or DIP work is required, preserving or reconstructing the A5 pulley if it is divided. Closure. Irrigate, achieve haemostasis, and close the skin without tension using everting mattress or simple interrupted sutures to prevent inversion; apices placed too volarly create a straight scar across the crease and a flexion contracture. Aftercare depends on the procedure: early protected motion after tendon repair reduces adhesions; a splint is used for fracture or pulley work; monitor digital perfusion and sensation and remove sutures at 10 to 14 days. Complications to avoid:
- Scar contracture across a flexion crease from poor incision geometry (apices too volar)
- Digital neurovascular injury from late identification or aggressive retraction
- Flexor tendon bowstringing from loss of A2 and A4 without reconstruction
- Wound edge necrosis from thin flaps or excessive undermining
- Infection in contaminated or infected cases
Procedures Through This Approach
- Zone 2 flexor tendon repair — the principal indication; also primary or delayed repair across zones 1 to 3.
- Flexor tendon grafting or staged reconstruction with a silicone rod.
- A2 or A4 pulley reconstruction using a tendon graft or pulley advancement.
- Volar plate repair or reconstruction.
- Digital phalanx fracture fixation via the volar approach.
- Drainage of pyogenic flexor tenosynovitis.
- Extensive trigger finger release with pulley and sheath work.
Viva & Exam Focus
The Bruner volar zigzag approach provides safe, extensile exposure of the flexor tendon sheath and digital neurovascular structures from the distal palm to the fingertip. The classic angled incisions cross each flexion crease obliquely at 45 to 60 degrees with apices precisely at the mid-axial points on each side of the digit. This geometry distributes scar tension away from the flexion crease and minimises the risk of a contracture that would limit digital flexion. Full-thickness skin flaps are elevated preserving the subdermal plexus, exposing the sheath from the A1 to the A5 pulley. The paired digital neurovascular bundles lie on the radial and ulnar aspects of the sheath and must be identified and protected throughout. The approach is the standard for zone 2 flexor tendon repair, pulley reconstruction, selected digital fractures and drainage of flexor sheath infections. A2 and A4 pulleys are preserved whenever possible because their loss produces bowstringing and loss of active flexion. No true internervous plane exists; dissection occurs between the paired neurovascular bundles.
ZIGZAGZIGZAG — Bruner incision principles
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old carpenter sustains a zone 2 flexor tendon laceration to the index finger. Describe your surgical approach and the key technical points for repair.”
“During a zone 2 flexor tendon repair you find the A2 pulley is severely damaged and cannot be repaired primarily. What are your options and how do you decide?”
“You are planning exposure for a zone 2 flexor tendon repair. What are the advantages of the Bruner approach over the mid-axial approach?”
Incision Geometry
- Zigzag crosses each flexion crease at 45 to 60 degrees
- Apices must sit exactly at the mid-axial line on both sides
- Prevents a longitudinal scar contracture across the crease
- Mark the mid-axial points first before drawing the zigzag
- Limb length about 1.5 to 2 cm depending on digit size
Neurovascular Protection
- Paired radial and ulnar digital neurovascular bundles on each side of the sheath
- Identify both bundles early before any deep dissection
- The nerve lies dorsal to the artery in each bundle
- Use vessel loops for gentle retraction and protection
- Loupe magnification is mandatory throughout
Pulley Management
- Preserve A2 (proximal phalanx) and A4 (middle phalanx) whenever possible
- A1, A3 and A5 may be divided for exposure or therapeutic release
- Critical pulleys prevent flexor tendon bowstringing
- Reconstruct or advance a critical pulley that must be sacrificed
- Test tendon excursion after any pulley work
Flap Elevation
- Raise full-thickness skin flaps down to the flexor sheath
- Preserve the subdermal vascular plexus on the deep surface of the dermis
- Avoid thin flaps or excessive undermining
- Bipolar haemostasis for reliable wound healing
- Close without tension using everting mattress sutures
Indications
- Zone 2 flexor tendon repair (the primary indication)
- Pulley reconstruction and staged tendon grafting
- Digital fracture fixation via a volar approach
- Flexor sheath infection drainage
- Extensile exposure for zone 1 to 3 continuity
Complications to Avoid
- Scar contracture from apices placed too volarly
- Digital neurovascular injury from late identification
- Bowstringing from loss of A2 and A4
- Wound edge necrosis from thin flaps
- Infection in contaminated cases
References
The Zigzag Volar-Digital Incision for Flexor-Tendon Surgery
- Described the classic angled zigzag incision crossing flexion creases obliquely with apices at mid-axial points
- Demonstrated reduced scar contracture risk compared with straight or transverse incisions across creases
- Established the Bruner approach as the standard volar exposure for flexor tendon surgery in the digit
Biomechanical analysis of finger flexor pulley reconstruction
- Demonstrated that loss of both A2 and A4 pulleys produces clinically significant bowstringing and reduced active flexion
- Compared various reconstruction techniques including tendon graft and pulley advancement
- Established principles for deciding when and how to reconstruct critical pulleys during zone 2 procedures
A2 pulley integrity and the strength of flexor tendon repair: a biomechanical study in a chicken model
- Demonstrated that A2 pulley integrity significantly affects the strength of flexor tendon repair in a biomechanical model
Relative contribution of tissue oedema and the presence of an A2 pulley to resistance to flexor tendon movement: an in vitro and in vivo study
- Showed the A2 pulley contributes substantially to resistance to flexor tendon movement, supporting preservation during exposure
The digital palmar oblique incision
- Described oblique incision techniques for digital flexor tendon exposure that minimise neurovascular risk and scar contracture