Deformity correction and arthrodesis of the Charcot foot using superconstruct principles · advanced
- Eichenholtz staging determines surgical timing: Stage I (fragmentation, active inflammation) is a relative contraindication to reconstructive arthrodesis — operate during Stage II-III (coalescence and consolidation) when the inflammatory process has settled and bone has some healing capacity. Stage 0 (clinical inflammation with normal radiographs) requires immobilisation and offloading, not surgery, unless there is acute instability or impending ulceration over a displaced fragment.
- Superconstruct principles (Sammarco and Conti): (1) extend the arthrodesis beyond the zone of Charcot injury to include uninvolved joints, (2) use the strongest possible fixation — intramedullary beams, large-diameter screws, plantar plates, bolts, (3) accept prolonged immobilisation with non-weight-bearing for 8 to 12 weeks minimum in most cases, (4) resect enough bone to fully correct the deformity and eliminate the plantar prominence. These principles are essential because Charcot bone is osteopenic, mechanically poor, and biologically unforgiving.
- The rocker-bottom deformity from midfoot (Lisfranc and tarsometatarsal) Charcot collapse creates a plantar bony prominence that ulcerates in the insensate foot — this is the single most common indication for surgery. A plantar ulcer over a bony prominence will not heal with antibiotics or dressings alone while the underlying mechanical cause persists; either exostectomy (simple prominence resection) or formal arthrodesis with deformity correction is required.
- Intramedullary beaming (rods or nails placed retrograde through the calcaneus and up the tibia) provides axial load-sharing fixation that is biomechanically stronger than plate-and-screw constructs alone — it is the preferred strategy for hindfoot and ankle Charcot reconstructions where bone quality is severely compromised.
- “The most common Charcot pattern is Sanders Type 2 — tarsometatarsal (Lisfranc) joint involvement producing the classic rocker-bottom midfoot deformity. Know the five Sanders patterns for the viva: forefoot, TMT, midtarsal, hindfoot, and calcaneus.
- “Total-contact casting (TCC) is the gold-standard non-operative management for acute Charcot (Eichenholtz Stage 0 to I) and for offloading plantar ulcers. Surgery is reserved for deformity that cannot be accommodated in a brace or cast, or for ulcers that fail to heal despite adequate offloading.
- “Surgery in active Charcot (Eichenholtz Stage I) carries catastrophic risk of worsening fragmentation, nonunion, and deep infection. Wait until the foot cools clinically and radiographs show coalescence or consolidation (Stage II to III) before elective reconstruction. The exception is acute Charcot with instability or fracture-dislocation threatening the skin, which may need urgent external fixation.
- “Amputation (below-knee or above-knee) remains the final common pathway for failed reconstruction, uncontrollable infection, or a non-salvageable foot. Up to a quarter of patients with Charcot foot may eventually require some level of amputation — this must be part of the consent discussion.
When & Why
Timing is everything. The Eichenholtz stage sets the clock for surgery. Acute Charcot (Stage 0 to I) is a medical, not a surgical, problem — immobilise and offload in a total-contact cast until the foot cools. Elective reconstructive arthrodesis is deferred to Stage II to III (coalescence and consolidation), when the inflammatory cascade has settled and the bone has regained enough biology to hold fixation and fuse. Operating on a hot, actively fragmenting Stage I foot converts a manageable collapse into an infected nonunion with hardware failure. Absolute indications for reconstruction - Unbraceable deformity — a fixed rocker-bottom or hindfoot deformity that cannot be accommodated in a CROW boot, custom AFO, or total-contact cast.
- Recurrent or non-healing plantar ulcer over a bony prominence despite adequate offloading (at least 3 months of TCC or a CROW boot).
- Deep infection with osteomyelitis in the Charcot foot — debridement with or without concurrent stabilisation.
- Acute instability or fracture-dislocation threatening the soft tissues — urgent external fixation even in Eichenholtz Stage I. Relative indications: a patient declining prolonged offloading, recurrent ulceration despite brace compliance, progressive deformity on serial radiographs despite immobilisation, or inability to wear any footwear. Contraindications (elective reconstruction) - Absolute: Eichenholtz Stage I (active fragmentation) — catastrophic fixation failure and worsening deformity; uncontrolled infection with systemic sepsis; critical ischaemia (ABI less than 0.45 or absolute toe pressure less than 30 mmHg) without planned revascularisation.
- Relative: Eichenholtz Stage 0 with no instability (treat non-operatively first); HbA1c greater than 10 percent; active smoking; end-stage renal disease on dialysis; limited or no ambulatory potential (amputation may be more appropriate). Which operation, and why. Every reconstruction begins from the same logic — remove the plantar prominence and realign the foot to plantigrade. The choice is how much you fuse:
Resection of the plantar bony prominence alone, without arthrodesis. Quick and low-morbidity, it preserves joint mobility — for an isolated prominence with a non-healing ulcer in a braceable foot. It recurs in 30 to 50 percent at 2 to 3 years if the underlying deformity is left uncorrected.
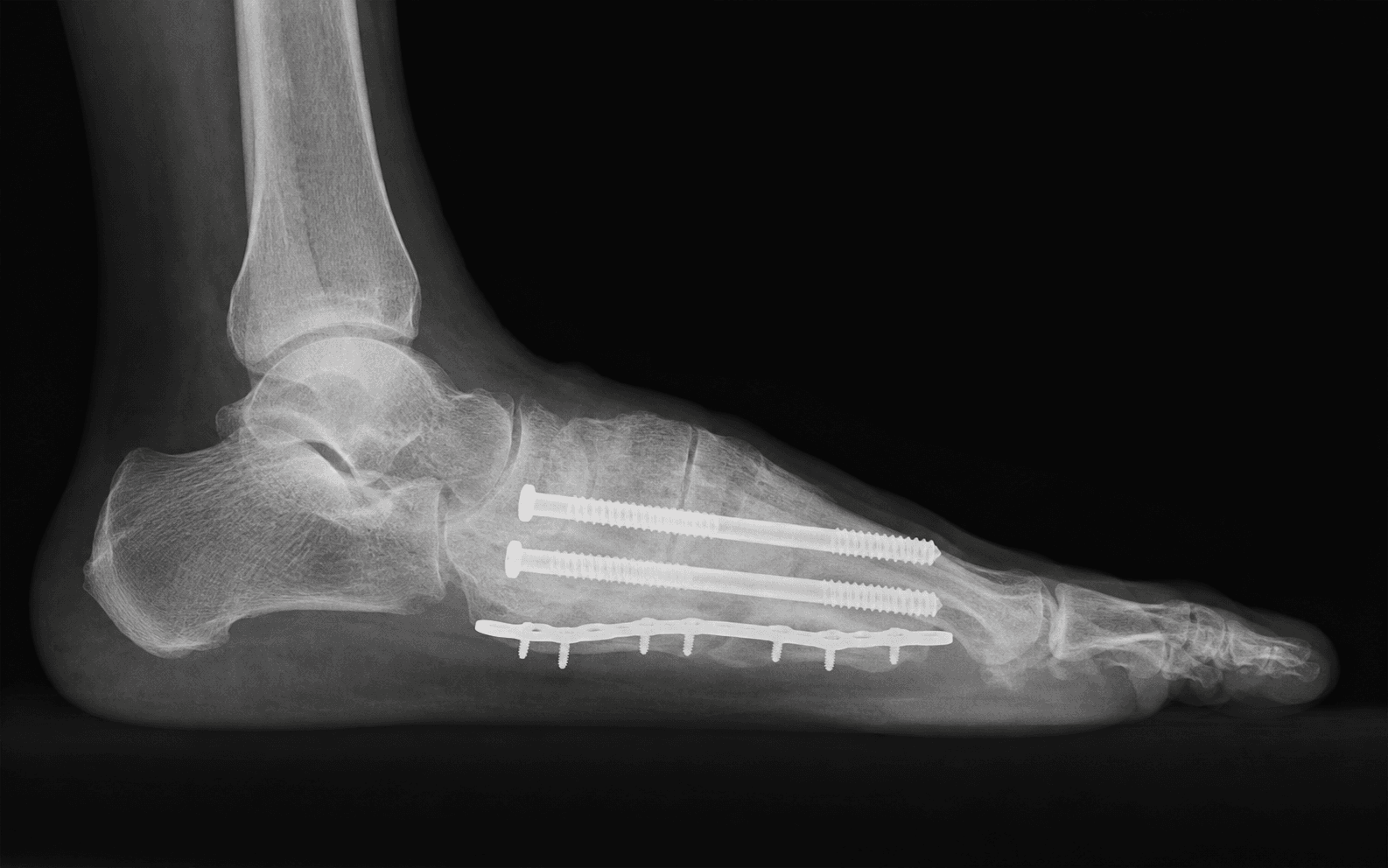
The definitive procedure for an unbraceable Sanders Type 2 rocker-bottom foot: correct the deformity, eliminate the plantar prominence, and build a stable plantigrade foot with plates, large screws and a medial column bolt, extended beyond the Charcot zone.
A retrograde tibiotalocalcanear intramedullary nail — the ultimate superconstruct — for Sanders Type 4 ankle and subtalar destruction with valgus collapse, or salvage after a failed midfoot fusion.
- Exostectomy
- No — removes the prominence only; the underlying deformity persists
- Arthrodesis
- Yes — corrects alignment and eliminates the prominence
- Exostectomy
- 60 to 80 percent initially
- Arthrodesis
- 80 to 90 percent when the deformity is corrected
- Exostectomy
- 30 to 50 percent at 2 to 3 years
- Arthrodesis
- 10 to 20 percent if fusion is solid
- Exostectomy
- Preserved
- Arthrodesis
- Sacrificed at the fused joints
- Exostectomy
- Minimal (local resection only)
- Arthrodesis
- Adequate for fixation (Stage II to III)
- Exostectomy
- 4 to 6 weeks (partial weight-bearing)
- Arthrodesis
- 12 to 16 weeks (non-weight-bearing)
- Exostectomy
- 30 to 50 percent (recurrent prominence)
- Arthrodesis
- 10 to 20 percent (nonunion, infection)
- Exostectomy
- Isolated prominence, braceable foot, compliant patient
- Arthrodesis
- Unbraceable deformity, recurrent ulcer, instability
Pre-operative optimisation. The Charcot patient is a high-risk host — optimise before you cut. Target HbA1c below 8 to 9 percent, confirm perfusion with ABI and toe pressures (revascularise first if ABI less than 0.45 or toe pressure less than 30 to 40 mmHg), correct nutrition (albumin above 3.0 g/dL, pre-albumin above 15 mg/dL), mandate smoking cessation, and screen for infection. If an ulcer is present, take deep cultures and image for osteomyelitis before planning a definitive fusion — infected bone must be cleared first, often in a staged (debridement then delayed fusion) sequence. Imaging. Weight-bearing radiographs of both feet (AP, lateral, oblique) measure the deformity; CT maps fragmentation, bone stock and joint involvement for hardware planning; MRI separates Charcot from osteomyelitis (both show marrow oedema) and identifies abscess or sinus tracts; a labelled white-cell scan distinguishes infection from Charcot when MRI is equivocal. Consent. Be honest about magnitude: deep infection up to 30 percent, nonunion 10 to 40 percent, wound breakdown 15 to 25 percent, and a real possibility that the reconstruction fails and amputation is ultimately required — up to a quarter of Charcot patients come to some level of amputation. Recovery is prolonged: non-weight-bearing for months, and six months or more before full function. Setup. Supine with a sandbag under the ipsilateral buttock to internally rotate the leg and bring the dorsum of the foot into the field; a bump under the knee relaxes the popliteal structures if a posterior approach is needed. Thigh tourniquet at 250 to 300 mmHg, kept under 90 to 120 minutes in the diabetic, vasculopathic limb. General or spinal anaesthesia with a popliteal sciatic and saphenous block for post-operative analgesia. C-arm from the contralateral side for lateral views and from the foot end for AP — fluoroscopy is used throughout.
The Operation
The goal is to remove the plantar prominence, realign the medial column to a plantigrade foot, and stabilise it with fixation strong enough to survive months of protected loading in osteopenic bone. The dominant technique is the dorsal approach to the tarsometatarsal (TMT) joints for a Sanders Type 2 rocker-bottom reconstruction — laid out step by step below, with the exposure as the opening moves. The approach is chosen by Sanders pattern: | Pattern | Primary approach | Joints exposed | |---------|------------------|----------------| | Type 2 (TMT) | Dorsal longitudinal over the TMT joints (1st and 2nd interspace) | First, second and often third TMT joints; naviculocuneiform | | Type 3 (midtarsal) | Dorsal or combined dorsomedial | Talonavicular, naviculocuneiform, calcaneocuboid | | Type 4 (hindfoot) | Lateral (for a TTC nail) with posterior or medial approaches | Subtalar, ankle, tibiotalocalcaneal | | Type 1 (forefoot) | Plantar or dorsal | MTP joints, metatarsal heads |
Operative sequence — midfoot (Sanders Type 2) reconstruction
- Supine, sandbag under the ipsilateral buttock, thigh tourniquet, C-arm available throughout.
- Confirm the deformity and the planned incision with the foot held in the position of deformity.
- Mark a longitudinal dorsal incision over the second TMT joint, centred on the apex of the rocker-bottom deformity as seen on the lateral radiograph.
- Extend proximally to the naviculocuneiform joint and distally to the second metatarsal base as needed.
- For extensive exposure across multiple TMT joints, use two separate dorsal incisions (one over the first TMT, one over the second to fourth TMT) rather than a single long incision with compromised wound edges.
- Carry the incision full-thickness straight down to the extensor retinaculum in the diabetic foot — the dorsal skin is thin and atrophic and must not be undermined.
- Plan around previous ulceration or scar.
- Thin atrophic dorsal skin in the diabetic foot — keep incisions full-thickness and avoid undermining.
- Previous ulceration or scar — plan incisions to avoid compromised skin.
- The dorsalis pedis artery runs in the field between EHL and EDL — identify it before deepening.
- Excessive swelling distorts anatomy — deflate the tourniquet and reassess if needed.
- Deepen through subcutaneous tissue to the extensor retinaculum. Identify and protect the EHL and EDL tendons.
- Locate the dorsalis pedis artery and deep peroneal nerve running between EHL and EDL — tag them with vessel loops and keep them under direct vision throughout.
- Retract EHL medially and EDL laterally. Incise the dorsal joint capsules of the TMT joints longitudinally.
- Clear soft tissue and Charcot debris from the joint surfaces with curettes and rongeurs.
Find the deep peroneal nerve and dorsalis pedis artery between EHL and EDL early, tag them, and keep them under direct vision throughout. Charcot tissue is inflamed and friable — use blunt dissection around the neurovascular structures and sharp dissection only at the joint capsule.
- Before any resection, place a K-wire into the medial cuneiform and another into the talus and check alignment under fluoroscopy to understand the deformity apex and the correction needed.
- Resect the Charcot debris and sclerotic bone from the TMT surfaces with an oscillating saw and osteotomes to create bleeding cancellous bone surfaces that will fuse.
- Remove enough bone to realign the medial column — typically 5 to 15 mm of resection at the apex — and correct the dorsal angulation to bring the forefoot into a plantigrade position relative to the hindfoot.
- Confirm under fluoroscopy that the plantar midfoot prominence has been eliminated.
- Inadequate resection leaves a residual plantar prominence that will re-ulcerate — check from the lateral fluoroscopic view.
- Over-resection destabilises the midfoot and makes length and alignment hard to restore.
- Penetration of the plantar cortex creates a new prominence or weakens the remaining bone.
- The tarsal tunnel structures (tibial nerve and vessels) lie plantar to the resection — protect with a retractor.
- Reduce the TMT joints anatomically and hold with temporary K-wires placed dorsal-to-plantar across each TMT joint.
- Confirm in AP, lateral and oblique views: AP shows TMT alignment and a restored medial column with no residual subluxation; lateral shows a plantigrade foot with no plantar prominence and a corrected Meary angle; oblique confirms the second TMT (the keystone) is reduced.
- Dorsal plates across the second and third TMT joints, and a medial plate along the first TMT joint (medial cuneiform to first metatarsal).
- Large-diameter (4.0 to 6.5 mm) partially threaded cannulated screws across each TMT joint in lag technique, from dorsal-to-plantar or medial-to-lateral depending on trajectory.
- A medial column bolt from the first metatarsal head through the medial cuneiform and into the navicular gives powerful compression across the entire medial column — especially useful when the Charcot zone reaches the naviculocuneiform joint.
- Extend the fixation at least one joint beyond the Charcot zone in both directions (the superconstruct spanning principle).
- Screws penetrating the plantar cortex create new prominences — check length on lateral fluoroscopy.
- Dorsal plates beneath thin skin — use low-profile plates and consider removing them at 9 to 12 months if symptomatic.
- Inadequate purchase in osteopenic Charcot bone — use large-diameter screws, locked constructs and supplementary bolt fixation.
- Failure to span beyond the Charcot zone invites adjacent-joint collapse.
- Fill the arthrodesis bed with autograft (iliac crest or local calcaneal graft).
- In extensive defects, supplement with allograft cancellous chips or BMP-2 on an absorbable collagen sponge, packed into all resection gaps and between the joint surfaces.
- Release the tourniquet, achieve haemostasis, and close in layers.
- Apply a well-padded below-knee posterior splint or cast with the foot in neutral dorsiflexion and slight hindfoot valgus.
Exostectomy — the simpler alternative When the foot is otherwise braceable and the problem is a single plantar prominence with a non-healing ulcer, resect the prominence alone. 1. Approach through a plantar incision directly over the ulcer or prominence. Excise the ulcer en bloc with the underlying bony prominence.
- Resect the plantar bony prominence flush with the surrounding plantar cortex using a rongeur or oscillating saw.
- Confirm fluoroscopically that no residual plantar prominence remains.
- Obtain deep cultures and histology of the resected bone — if osteomyelitis is found, extend the debridement and plan subsequent arthrodesis.
- Close over a drain and apply a total-contact cast.
Always take the specimen for histology and deep cultures. If the bone shows osteomyelitis, exostectomy alone has a high failure rate — plan a staged approach: TCC to heal the wound, then definitive arthrodesis once the infection has cleared.
Hindfoot reconstruction — tibiotalocalcaneal (TTC) nail For Sanders Type 4 ankle and subtalar destruction, or salvage of a failed midfoot fusion, a retrograde TTC nail is the definitive superconstruct. - Approach: lateral trans-fibular. The fibula is osteotomised and the proximal fragment removed (fibular subtraction) to expose the ankle and subtalar joints; a posterolateral incision gives access to the calcaneal tuber nail entry point.
- Joint preparation: resect the tibial plafond, talar dome and subtalar joint surfaces to bleeding bone; correct the hindfoot to neutral or slight valgus.
- Fixation: insert a retrograde nail from the calcaneal tuber, across the subtalar joint, through the talar body and into the tibial medullary canal — spanning calcaneus to tibia. Add anterior locking screws into the talar neck and calcaneus for rotational control.
- Graft: fill the resection defects with autograft and allograft.
- Nail malalignment — the entry point must be central on the calcaneal tuber on both AP and lateral views.
- Talar body penetration or fracture — the Charcot talus is osteopenic and may fracture during reaming.
- Anterior tibial cortex penetration by the nail tip — confirm fluoroscopically.
- Residual plantar prominence after correction — confirm on lateral fluoroscopy before closure.
Intramedullary beaming — protecting the construct Beyond plate-and-screw fixation, intramedullary beaming — smooth or threaded K-wires or small-diameter nails run along the metatarsal canals from dorsal to plantar, crossing the TMT arthrodesis and seating into the cuneiforms or tarsal bones — adds axial load-sharing that protects the construct from bending failure in cyclic loading. It is low-profile (no added hardware prominence) and can be removed in clinic once fusion is confirmed at 6 to 12 months.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Management | |-------|--------|----------------|------------| | 1 | Weeks 0 to 2 | Non-weight-bearing below-knee cast or rigid posterior splint; elevate 48 to 72 hours | Wound check at 5 to 7 days then weekly; multimodal analgesia; continue targeted antibiotics 4 to 6 weeks if a pre-operative ulcer was present | | 2 | Weeks 2 to 8 | Strict non-weight-bearing below-knee cast; cast changes every 2 weeks | Touch-down only (less than 15 kg) from 6 to 8 weeks if early consolidation is seen | | 3 | Weeks 8 to 12 | CROW boot or total-contact cast | Progressive weight-bearing as tolerated, guided by serial radiographs | | 4 | Weeks 12 to 16 plus | Diabetic shoe with custom-moulded insole once fusion is confirmed; CROW boot or orthotics long-term in many | Consider hardware removal of prominent implants at 9 to 12 months once fused | Fusion is confirmed radiographically when bridging trabeculae cross the arthrodesis on three views with no hardware loosening. The fused Charcot foot remains at lifelong risk of ulceration from abnormal pressure distribution, so custom moulded orthotics or a CROW boot continue indefinitely in many patients. ### Total-contact casting — the non-operative gold standard Indications: acute Charcot (Stage 0 to I), plantar ulcer offloading, post-exostectomy protection, and protected weight-bearing after arthrodesis. Technique 1. Apply a thin layer of stockinette over the foot and lower leg — keep the toes visible for monitoring, do not fold back over them. 2. Place felt padding over bony prominences (malleoli, tibial crest, heel), avoiding the ulcerated area. 3. Wrap the foot and leg in two layers of cast padding, moulding the plantar surface to the corrected foot shape. 4. Apply plaster or fibreglass in a below-knee configuration, moulding the cast against the plantar surface to redistribute pressure away from the ulcer or prominence. 5. Change the cast every 1 to 2 weeks for inspection. Complications of TCC: new pressure ulceration (inspect skin at every change), ankle equinus contracture from prolonged immobilisation, and patient non-compliance (difficult for obese patients or those with limited hand function). ### Special situations
Osteomyelitis and Charcot coexist and are hard to separate on MRI alone — both show marrow oedema. If deep bone biopsy or a labelled white-cell scan confirms infection, infection is the primary pathology. Treat with aggressive debridement of infected bone, culture-directed antibiotics for 6 to 8 weeks, and delayed reconstruction after clearance. Never fuse through infected bone — it will fail. If the foot is unstable after debridement, temporary external fixation holds it while the infection is controlled.
ABI less than 0.45 or toe pressure less than 30 to 40 mmHg indicates critical limb ischaemia. Revascularise (angioplasty or bypass) before elective reconstruction, then allow a 2 to 4 week reperfusion period before fusion. In patients who cannot be revascularised, amputation may be the most appropriate option — reconstruction in an ischaemic foot carries catastrophic wound complication rates.
Up to 25 percent of patients develop contralateral involvement. If one foot has been reconstructed and the other becomes active, immobilise the new side in TCC while protecting the reconstructed side in a CROW boot. Bilateral reconstruction is staged — let one side fuse and resume weight-bearing before operating the other. Bilateral non-weight-bearing creates major nursing and mobility challenges, so plan for inpatient rehabilitation.
Complications
- Incidence
- Up to 30 percent
- Recognition
- Wound dehiscence, purulent drainage, fever, rising inflammatory markers; MRI shows marrow signal change around hardware. May present insidiously in the insensate patient.
- Prevention and management
- Prevention: optimise glycaemic control, treat active ulcers before elective fusion, consider staged procedures, perioperative antibiotics. Management: urgent washout and debridement, deep cultures, IV antibiotics; remove hardware if fusion is solid, otherwise convert to external fixation or amputation.
- Incidence
- 10 to 40 percent (site dependent)
- Recognition
- Persistent pain on weight-bearing, hardware loosening or breakage on serial radiographs, no bridging trabeculae across the arthrodesis at 6 months.
- Prevention and management
- Prevention: superconstruct fixation, bone grafting, prolonged non-weight-bearing. Management: revise with a stronger construct, add bone graft or BMP, extend immobilisation; consider amputation if revision fails.
- Incidence
- 5 to 20 percent
- Recognition
- Broken screws, fractured plate or bent nail on radiographs. May be asymptomatic if fusion has occurred, or painful if nonunion is present.
- Prevention and management
- Prevention: strongest fixation from the outset, prolonged non-weight-bearing. Management: if fused, remove broken hardware; if not fused, revise with a more robust construct.
- Incidence
- 15 to 25 percent
- Recognition
- Skin necrosis, wound separation, exposed hardware or bone. Often delayed (2 to 4 weeks post-operatively); insensate patients may not report symptoms.
- Prevention and management
- Prevention: meticulous soft-tissue handling, limit tourniquet time, avoid long single incisions, generous postoperative padding. Management: wound care, negative-pressure therapy, soft-tissue coverage (rotational or free flap) if hardware is exposed.
- Incidence
- 10 to 20 percent after arthrodesis
- Recognition
- Return of plantar ulceration at a new or incompletely corrected site, often from residual deformity or hardware prominence.
- Prevention and management
- Prevention: fluoroscopic confirmation that no plantar prominence remains; remove plantar-sided hardware once fused. Management: TCC, consider revision arthrodesis or exostectomy.
- Incidence
- 5 to 15 percent
- Recognition
- Progressive deformity at a new site adjacent to the fusion mass — a new rocker-bottom or hindfoot valgus as the process activates at adjacent joints.
- Prevention and management
- Prevention: extend fusion beyond the Charcot zone (superconstruct principle). Management: repeat immobilisation (TCC), consider extending the fusion.
- Incidence
- Up to 25 percent overall
- Recognition
- End-stage salvage failure — a non-salvageable foot with uncontrollable infection, nonunion or non-ambulatory status.
- Prevention and management
- Prevention: careful patient selection, optimisation, timely reconstruction before deformity is irrecoverable. Management: below-knee (transtibial) amputation preferred for ambulatory patients; above-knee if knee extension is deficient or thigh involvement is extensive.
Viva & Exam Focus
CHARCOTCHARCOT — assessment and staging
SUPERSUPER — superconstruct principles (Sammarco)
The trap is operating on a hot, swollen, actively fragmenting foot believing early fixation will prevent progression. The reality is that bone is actively resorbing — fixation pulls out, the arthrodesis bed has no healing capacity, and surgery turns a manageable collapse into an infected nonunion with hardware failure. Wait for Stage II to III (clinical cooling, coalescence or consolidation on imaging) before elective reconstruction.
The Charcot patient has peripheral neuropathy and cannot feel wound problems. A dehiscence that in a sensate foot would hurt and prompt early review can progress silently to deep infection and osteomyelitis. Prevention is meticulous soft-tissue handling, avoiding extensive dorsal dissection where skin is thin, considering staged procedures (external fixation first) in high-risk cases, and weekly wound inspection for the first 4 to 6 weeks.
Fixation on the plantar surface — plantar plates or protruding screw tips — creates a new prominence in the insensate foot that ulcerates post-operatively, the very problem the surgery meant to eliminate. Place hardware dorsally or laterally wherever possible; if a plantar plate is required, countersink fully and confirm on fluoroscopy that nothing protrudes below the plantar cortex. Plan to remove plantar-sided hardware once fusion is confirmed, often at 6 to 9 months.
Charcot bone is osteopenic and biologically poor — standard screws cut through cancellous bone and plates break under cyclic loading before fusion is achieved. Apply superconstruct principles: extend the fusion beyond the Charcot zone, use intramedullary nails or beaming for axial load-sharing, supplement plate fixation with multiple points of fixation, accept prolonged non-weight-bearing for 8 to 12 weeks minimum, and bone-graft the arthrodesis bed.
Charcot patients often have pre-existing or recent plantar ulceration with bacterial colonisation of bone, diabetes with impaired immunity and wound healing, and co-existing vascular disease. Deep infection rates after reconstruction reach up to 30 percent across series; hardware removal may be required and the fusion is lost. Two-stage procedures (external fixation to stabilise, then delayed fusion after infection control) may be needed, and some cases end in amputation.
A hot, swollen, erythematous diabetic foot is treated as cellulitis with antibiotics when the true diagnosis is acute Charcot (Stage 0 to I). The distinguishing feature is that Charcot is painless or only mildly uncomfortable in an insensate patient, often with prior Charcot episodes, while cellulitis is typically painful. Maintain a high index of suspicion, compare skin temperature with the contralateral foot, obtain MRI (marrow oedema and microfractures), and immobilise promptly — do not just prescribe antibiotics.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 56-year-old man with Type 2 diabetes presents with a 3-month history of a non-healing plantar midfoot ulcer. He has a rocker-bottom deformity of the left foot with a 2 cm ulcer directly beneath the midfoot prominence. Radiographs show collapsed TMT joints with debris and early coalescence. Temperature measurement shows a 0.5-degree difference from the right foot. He has been in a CROW boot for 10 weeks with no improvement. How do you manage him?”
“A 62-year-old woman with Type 2 diabetes presents with a 4-week history of a hot, swollen left foot after walking through an airport in sandals. She has had diabetes for 18 years with peripheral neuropathy. The left foot is erythematous, swollen and warm to touch, but she says it is not particularly painful. Her GP started oral antibiotics for cellulitis 10 days ago with no improvement. How do you manage this?”
“A 60-year-old man with Type 2 diabetes had a midfoot Charcot reconstruction with TMT arthrodesis 14 months ago at another hospital. Radiographs show solid fusion, but there is a new ulcer on the plantar aspect of the foot just distal to the arthrodesis site, with a bony prominence on the lateral view that was not present on the immediate post-operative films. How do you explain this and manage him?”
Diagnosis and staging
- Eichenholtz Stage 0: clinical inflammation, normal X-rays. Stage I: fragmentation. Stage II: coalescence. Stage III: consolidation.
- A painless warm swollen foot in an insensate diabetic is acute Charcot until proven otherwise.
- Charcot vs cellulitis: Charcot is painless (neuropathy), cellulitis is painful. Both cause erythema and swelling. If in doubt, immobilise and image.
- MRI is the investigation of choice — marrow oedema, microfractures, subluxation. A labelled white-cell scan helps distinguish Charcot from osteomyelitis.
- Sanders patterns: Type 1 forefoot, Type 2 TMT (most common, rocker-bottom), Type 3 midtarsal, Type 4 hindfoot, Type 5 calcaneus.
Non-operative management
- Total-contact casting (TCC) is the gold standard for acute Charcot (Stage 0 to I) and ulcer offloading.
- Cast changes every 1 to 2 weeks. Continue until the foot cools (8 to 12 weeks).
- CROW boot for quiescent Stage III deformity that is stable and braceable.
- Do NOT operate during Eichenholtz Stage I (active fragmentation) — catastrophic fixation failure.
- Ulcer healing requires offloading the mechanical cause. Antibiotics alone do not heal ulcers over bony prominences.
Indications for surgery
- Unbraceable deformity that cannot be accommodated in a CROW boot or AFO.
- Recurrent or non-healing plantar ulcer over a bony prominence despite adequate offloading.
- Deep infection with osteomyelitis in the Charcot foot.
- Acute instability or fracture-dislocation threatening the soft tissues.
- Contraindications: Eichenholtz Stage I, uncontrolled infection, critical ischaemia without revascularisation.
Superconstruct principles (Sammarco)
- Extend the fusion beyond the zone of Charcot injury to include uninvolved joints.
- Use the strongest possible fixation — IM nails, large screws, plates, bolts.
- Accept prolonged immobilisation — non-weight-bearing 8 to 12 weeks minimum.
- Resect sufficient bone to fully correct the deformity and eliminate the plantar prominence.
- Reinforce with bone graft (autograft, allograft or BMP).
Surgical anatomy
- TMT (Lisfranc) complex: medial, middle and lateral columns. The second TMT is the keystone.
- Lisfranc ligament: medial cuneiform to second metatarsal base — destroyed in Type 2 Charcot, producing medial column collapse.
- Dorsalis pedis artery and deep peroneal nerve run between EHL and EDL on the dorsal midfoot — identify and protect during the dorsal approach.
- Sanders Type 2 (TMT) is the most common pattern — rocker-bottom midfoot with a plantar ulcer.
- Hindfoot Charcot (Type 4): tibiotalocalcaneal arthrodesis with an IM nail — retrograde nail from calcaneus through talus into tibia.
Operative technique — key steps
- Pre-op: optimise HbA1c, assess vascular status (ABI, toe pressures), rule out osteomyelitis with MRI.
- Position: supine, sandbag under the buttock, C-arm fluoroscopy available throughout.
- Approach: dorsal longitudinal over the TMT joints for midfoot; lateral trans-fibular for a hindfoot TTC nail.
- Resect Charcot debris and the plantar prominence — check fluoroscopically that no residual bump remains.
- Reduce to plantigrade alignment, hold with temporary K-wires, confirm under fluoroscopy.
- Definitive fixation: plates, large screws, medial column bolt, intramedullary beaming. Extend beyond the Charcot zone.
- Bone graft into all arthrodesis beds. Close in layers. Below-knee non-weight-bearing cast.
Complications
- Deep infection and osteomyelitis: up to 30 percent. Treat with washout, debridement, culture-directed antibiotics, hardware removal if fused.
- Nonunion: 10 to 40 percent. Revise with stronger fixation and bone graft; amputation if revision fails.
- Hardware failure: 5 to 20 percent. Remove if fused, revise if not.
- Wound breakdown: 15 to 25 percent. Insensate patients need weekly visual wound checks.
- Recurrent Charcot at adjacent joints: 5 to 15 percent. May need to extend the fusion.
- Amputation: up to 25 percent overall. Below-knee amputation preferred for ambulatory patients.
Post-operative protocol
- Weeks 0 to 2: non-weight-bearing below-knee cast. Weekly wound inspection.
- Weeks 2 to 8: non-weight-bearing cast. Cast changes every 2 weeks.
- Weeks 8 to 12: transition to a CROW boot with progressive weight-bearing if consolidation is visible on radiographs.
- Weeks 12 to 16 plus: custom diabetic shoe with a moulded insole once fusion is confirmed.
- Hardware removal: consider at 9 to 12 months for prominent dorsal plates or plantar-sided fixation.
Background & Evidence
The disease. Charcot neuroarthropathy is a progressive destruction of bone and joint in an insensate foot, most often in the setting of diabetic peripheral neuropathy. Repeated, unperceived microtrauma in a foot that cannot protect itself drives an inflammatory cycle of bone resorption, fragmentation and collapse. The structural end-point is a deformed, unstable foot — classically the rocker-bottom midfoot (Sanders Type 2, the most common pattern) — whose plantar bony prominence ulcerates under body weight. Up to a quarter of patients develop contralateral involvement, and up to a quarter eventually come to some level of amputation. Surgical anatomy of the midfoot. The tarsometatarsal (Lisfranc) complex — the most common site of Charcot collapse — has three functional columns: the medial (first metatarsal, medial cuneiform, navicular) supporting the medial arch; the middle (second metatarsal keystone, recessed 1 to 2 mm and anchored by the Lisfranc ligament); and the lateral (third to fifth metatarsals, lateral cuneiform, cuboid), the more mobile column. The Lisfranc ligament runs from the plantar medial cuneiform to the base of the second metatarsal; when it is destroyed the medial column drops into rocker-bottom. On the dorsum, the EHL and EDL tendons run superficially and the dorsalis pedis artery and deep peroneal nerve pass between them — the structures identified and protected in the dorsal approach. The blood supply comes from the dorsalis pedis (dorsal midfoot), the medial plantar artery (plantar midfoot and heel), and the perforating branches that connect the two and must be preserved to avoid devascularising bone fragments during correction. Deformity patterns and their consequences. In a Sanders Type 2 rocker-bottom, the medial column collapses through the first and second TMT joints and the navicular and medial cuneiform drop plantarly, producing a convex plantar midfoot prominence that ulcerates beneath the plantar fat pad — loss of the longitudinal arch transfers load from heel to midfoot prominence. A Type 3 midtarsal pattern collapses through the talonavicular and calcaneocuboid joints, producing forefoot abduction and a lateral column ulcer. A Type 4 hindfoot pattern gives progressive hindfoot valgus, talar dome collapse and fibular impingement, with medial malleolar ulceration.
- Clinical features
- Warm, swollen, erythematous foot; pain absent or mild; early inflammation
- Radiographic features
- Normal radiographs or subtle subluxation; bone scan or MRI shows early marrow oedema
- Treatment priority
- Immobilise immediately — total-contact cast. Do NOT operate unless acute instability threatens the skin.
- Clinical features
- Hot, swollen foot; temperature greater than 2 degrees above the contralateral side; joint effusion
- Radiographic features
- Bony fragmentation, subluxation, dislocation; debris and osseous destruction at involved joints
- Treatment priority
- Non-operative — continue TCC. Elective reconstruction is contraindicated. Exception: fracture-dislocation threatening the skin — urgent external fixation.
- Clinical features
- Cooling of the foot; reduced swelling; temperature difference diminishing
- Radiographic features
- Absorption of debris; new bone formation; coalescence of fragments; joint surfaces beginning to fuse
- Treatment priority
- Consider surgery — the foot is cooling and bone is consolidating; elective arthrodesis can be planned once the temperature normalises.
- Clinical features
- Normal temperature; minimal or no swelling; fixed deformity
- Radiographic features
- Consolidated bone; remodelled deformity; stable but malaligned architecture
- Treatment priority
- Surgery indicated if the deformity is unbraceable, there is an ulcer over a prominence, or instability is present.
- Location
- Forefoot (MTP joints)
- Typical deformity
- Dislocated toes, plantar metatarsal heads
- Common presentation
- Metatarsal head ulceration, transfer metatarsalgia
- Location
- Tarsometatarsal (Lisfranc)
- Typical deformity
- Rocker-bottom midfoot, medial column collapse
- Common presentation
- Plantar midfoot ulcer over the bony prominence (most common pattern)
- Location
- Midtarsal (talonavicular, naviculocuneiform)
- Typical deformity
- Lateral column collapse, forefoot abduction
- Common presentation
- Lateral foot ulcer, peritalar subluxation
- Location
- Ankle and subtalar
- Typical deformity
- Posterior tibial tendon insufficiency, hindfoot valgus, ankle instability
- Common presentation
- Medial malleolar or lateral hindfoot ulcer
- Location
- Calcaneus
- Typical deformity
- Posterior calcaneal fragmentation, loss of heel height
- Common presentation
- Posterior heel ulcer, Achilles tendon dysfunction
Key evidence. Total-contact casting remains the first-line treatment for acute Charcot, supported by long-term cohort data (Fabrin) showing most feet stabilise conservatively, with surgery reserved for unbraceable deformity or recurrent ulceration. The case for operative reconstruction rests on the superconstruct concept (Sammarco): standard small-fragment fixation is biomechanically inadequate in osteopenic neuropathic bone, so the arthrodesis must be extended beyond the zone of injury and reinforced with the strongest available fixation, prolonged immobilisation, bone resection to full correction, and bone graft. Contemporary systematic review (Ha) confirms that reconstruction achieves reasonable fusion and limb-salvage rates but carries substantial complication rates — deep infection, wound breakdown, nonunion and amputation — making careful patient selection and pre-operative optimisation essential.
References
Is the Eichenholtz classification still valid for the diabetic Charcot foot?
- Re-examined Eichenholtz's three-stage classification (development/fragmentation, coalescence, consolidation) and confirmed its continued clinical validity for staging diabetic Charcot neuroarthropathy
- Confirmed that natural history progresses from acute inflammatory destruction with hyperaemia and bone resorption to a quiescent stage with consolidation and fixed deformity
- Staging remains the most widely used system for timing surgical intervention — operative reconstruction is deferred until coalescence/consolidation when bone has regained healing capacity
Superconstructs in the treatment of Charcot foot deformity: plantar plating, locked plating, and axial screw fixation
- Defined the superconstruct principles for Charcot arthrodesis: extend fusion well beyond the zone of injury into adjacent uninvolved joints, use the strongest possible fixation (intramedullary nails, large-diameter screws, medial and dorsal plates, plantar plates, bolts), accept prolonged non-weight-bearing immobilisation
- Described surgical technique for Charcot midfoot and hindfoot reconstruction using plantar plating, locked plating and axial screw fixation in poor-quality neuropathic bone
- Emphasised that standard small-fragment fixation is biomechanically inadequate for the osteopenic, mechanically poor Charcot foot
Long-term follow-up in diabetic Charcot feet with spontaneous onset
- Long-term cohort follow-up of diabetic patients with Charcot feet of spontaneous onset managed with non-operative treatment (total-contact casting and Charcot-restraint-orthotic walker)
- Most feet stabilised with conservative treatment; recurrence of ulceration was the main late complication, especially over residual bony prominences
- Surgery (exostectomy or arthrodesis) was reserved for patients with unbraceable deformity or recurrent ulceration over a prominence — supporting TCC as the first-line treatment for acute Charcot
Are the Sanders-Frykberg and Brodsky-Trepman Classifications Reliable in Diabetic Charcot Neuroarthropathy?
- Validated the Sanders-Frykberg five-pattern anatomic classification of Charcot foot (forefoot, tarsometatarsal, midtarsal, hindfoot, calcaneus) and the Brodsky-Trepman scheme
- Confirmed inter-rater and intra-rater reliability of both classifications in contemporary practice, with the Sanders-Frykberg pattern dictating surgical approach and extent of arthrodesis
- Type 2 (TMT/Lisfranc) is the most common pattern, producing the classic rocker-bottom midfoot deformity
Charcot foot reconstruction outcomes: a systematic review
- Systematic review of contemporary Charcot foot reconstruction outcomes across reconstructive techniques (internal fixation, external fixation, and combined constructs)
- Achieved limb salvage in the majority of patients; fusion rates and ulcer healing rates vary with fixation method, anatomic site, and Eichenholtz stage at surgery
- Complication rates are substantial — deep infection, wound breakdown, nonunion, hardware failure and amputation are all reported; careful patient selection and pre-operative optimisation are essential