Reverse-Ponseti (Dobbs) serial casting, tendo-Achilles tenotomy and percutaneous talonavicular pinning for the rigid rocker-bottom flatfoot | advanced
- Congenital vertical talus (CVT) is a RIGID rocker-bottom flatfoot with an irreducible dorsal dislocation of the navicular on a vertically orientated talus and a fixed equinus hindfoot. The rigidity and the persistent talonavicular dislocation on a forced plantar flexion lateral radiograph separate it from the flexible oblique talus, which reduces on forced plantar flexion.
- The modern standard is the reverse-Ponseti (Dobbs) method: serial weekly manipulation and casting to stretch the dorsolateral soft tissues and seat the navicular onto the talar head, followed in theatre by percutaneous tendo-Achilles tenotomy and percutaneous talonavicular pinning (with a limited open reduction if closed reduction is incomplete). This has largely replaced the extensive single-stage soft-tissue release.
- About half of all CVT cases are syndromic or neuromuscular. Always screen for an underlying cause — neural tube defect (myelomeningocele), arthrogryposis, cerebral palsy, and syndromes such as Larsen and Beals — and examine the spine and hips before treating the foot in isolation.
- The talus has a tenuous blood supply and is at risk of avascular necrosis from extensive peritalar dissection. The move to the minimally invasive Dobbs method was driven in large part by reducing this risk and the stiffness that followed extensive releases.
When & Why
Indication. Symptomatic, confirmed true congenital vertical talus — a rigid rocker-bottom flatfoot with a persistent dorsal talonavicular dislocation on a forced plantar flexion lateral radiograph (idiopathic or syndromic), that has not corrected with an initial trial of manipulation and casting. The flexible look-alikes (oblique talus, positional calcaneovalgus) reduce on forced plantar flexion and are managed without surgery. Absolute indications. A confirmed true CVT that is rigid with a persistent talonavicular dislocation on the forced plantar flexion view (idiopathic or syndromic); failure of the deformity to correct after an initial trial of manipulation and casting; or an older infant or toddler presenting late with an established deformity. Relative indications. A mild or partially reducible deformity, where a short course of casting may fully correct the talonavicular joint so that only a percutaneous tenotomy and pinning are needed; and syndromic or neuromuscular CVT, where the same pathway applies but with a lower threshold for a limited open reduction and explicit counselling on a higher recurrence rate. Contraindications. Absolute: a flexible oblique talus (reduces on forced plantar flexion and is NOT a CVT — observation, stretching, occasional casting); a fully correctable structural positional deformity such as a severe positional calcaneovalgus foot; or an untreatable, life-limiting underlying condition where foot surgery would not be in the child's interest (a rare, multidisciplinary decision). Relative: severe skin compromise over the dorsum of the foot (defer casting until the skin recovers), or a medically unstable neonate (delay until the child is fit for sedation or anaesthesia). The one decision that matters — exclude the flexible foot. This is the single most important judgement and the most commonly examined point. The forced plantar flexion lateral radiograph resolves it:
- CVT (vertical talus)
- Rigid and irreducible
- Oblique talus
- Flexible, partially reducible
- Positional calcaneovalgus
- Flexible, easily correctable
- CVT (vertical talus)
- Fixed dorsal dislocation
- Oblique talus
- Subluxation, reducible
- Positional calcaneovalgus
- Reduced, normal
- CVT (vertical talus)
- Fixed equinus
- Oblique talus
- Mild calcaneus or valgus
- Positional calcaneovalgus
- Calcaneus and valgus, flexible
- CVT (vertical talus)
- Talonavicular stays dislocated; talar axis stays off the first metatarsal (diagnostic)
- Oblique talus
- Talonavicular reduces; talar axis aligns with the first metatarsal
- Positional calcaneovalgus
- Normal alignment throughout
- CVT (vertical talus)
- Fixed
- Oblique talus
- Present at rest, correctable
- Positional calcaneovalgus
- Absent
- CVT (vertical talus)
- Reverse-Ponseti casting then limited surgery
- Oblique talus
- Observation, stretching, occasional casting
- Positional calcaneovalgus
- Observation and passive stretching; resolves spontaneously
The forced plantar flexion lateral radiograph is the defining investigation. In true CVT the talonavicular joint stays dislocated dorsally and the talar axis fails to align with the first metatarsal — the talus stays vertical. In oblique talus the joint reduces and the axis aligns. Add AP and lateral neutral views for comparison, and a maximum dorsiflexion lateral view to show the fixed hindfoot equinus.
Do not label a foot as a fixed CVT until you have radiographically confirmed the talonavicular joint will not reduce on forced plantar flexion. Positional calcaneovalgus and oblique talus are flexible and are managed non-operatively — sending one of them to theatre is the classic exam trap.
Screen the whole child, not just the foot. Because about half of CVT cases are syndromic or neuromuscular, examine the spine for a neural tube defect, the hips for associated dysplasia, and look for arthrogryposis, cerebral palsy, Larsen or Beals syndrome. Arrange spinal and hip imaging and involve paediatrics (and neurology or genetics where relevant) before treating the foot in isolation. Consent specifically for the need for multiple weekly casts, the percutaneous tenotomy and pinning under sedation, the six-to-eight-week cast, the subsequent prolonged bracing commitment, and the risks of recurrence, residual deformity, talar avascular necrosis, stiffness, wound problems and pin-tract infection. Setup. The serial casting is performed without anaesthesia on a settled infant (often after a feed), in an outpatient setting. For the theatre procedure — percutaneous tenotomy and talonavicular pinning — position the child supine with the leg free, under sedation or a light general anaesthetic with full sterile precautions. Mini C-arm fluoroscopy is mandatory to confirm reduction of the talonavicular joint and correct K-wire placement.
The Operation
The goal: stretch the tight dorsolateral structures and seat the navicular onto the talar head by serial casting, then in theatre confirm and pin the talonavicular reduction under fluoroscopy, correct the residual hindfoot equinus with a percutaneous tendo-Achilles tenotomy, and hold the correction in a long-leg cast — preserving the tenuous talar blood supply throughout. The exposure that matters is the fluoroscopically guided reduction of the talonavicular joint, completed percutaneously when possible and through a small limited dorsolateral incision over the joint when closed reduction is incomplete.
Operative sequence
- Confirm true CVT on the forced plantar flexion lateral view — the talonavicular joint stays dislocated and the talar axis stays off the first metatarsal. Exclude the flexible oblique talus, which reduces.
- Examine the spine, hips and the whole child for an underlying cause; arrange spinal and hip imaging and involve paediatrics.
- Manipulate the foot into forefoot plantar flexion and adduction around the talar head, with counter-pressure on the lateral talar head — the opposite mechanics to a clubfoot cast.
- Apply a long-leg plaster cast with the knee flexed, holding the foot in the maximally corrected position; the hindfoot equinus is NOT corrected yet.
- Change the cast weekly, each time advancing the correction; typically four to seven casts are needed (an average of about five).
- Under mini C-arm fluoroscopy, assess whether the navicular now sits on the talar head after the final cast.
- If closed reduction is incomplete, make a small limited dorsolateral incision over the talonavicular joint and gently lever the navicular onto the talar head — take care NOT to dissect widely around the talar head and neck, to protect its end-arterial blood supply.
- Confirm a true reduction of the talonavicular joint in two planes on fluoroscopy before relying on any wire.
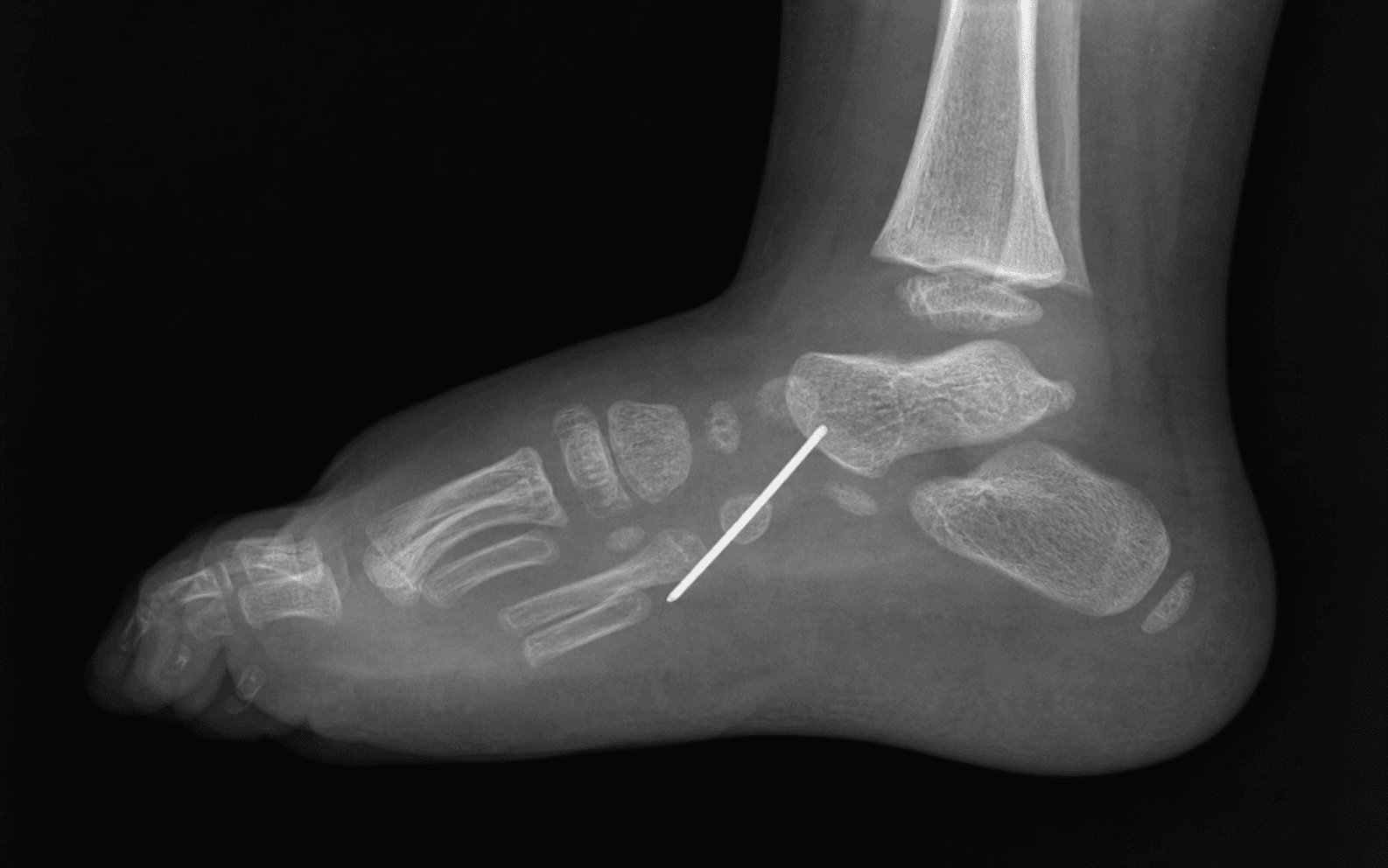
- Pass a smooth K-wire across the talonavicular joint from the navicular into the talar head and neck, securing the reduced joint.
- Confirm wire position and joint reduction on mini C-arm in two planes.
- Perform a percutaneous tendo-Achilles tenotomy to correct the fixed hindfoot equinus — identical in principle to the Ponseti clubfoot tenotomy.
- The heel comes down into dorsiflexion once the cord is released; this equinus is corrected LAST, only after the talonavicular joint is reduced and pinned.
- Apply a long-leg cast with the knee flexed and the foot in the corrected position, the K-wire incorporated and bent at the skin.
- The cast and wire are retained for six to eight weeks. Counsel parents on cast care, elevation and red-flag signs (fever, foul smell, loosening of the cast, exposed wire).
- At six to eight weeks, remove the K-wire (typically in clinic) and apply a short further period of casting if correction needs consolidation.
- Transition to a foot abduction orthosis (a reverse-last or moulded ankle-foot orthosis), worn full-time initially then night-time for years — mirroring the Ponseti bracing principle and the single most important factor in preventing recurrence.
The talus has a precarious, largely end-arterial blood supply through the neck and the tarsal sinus, with limited collateral flow to the body. Extensive peritalar dissection — the historical open release — is the principal cause of avascular necrosis of the talar body. Prefer the reverse-Ponseti method and, when the joint will not reduce closed, a limited gentle open reduction over any extensive capsular release. Preserving the peritalar soft tissues matters more than avoiding a small incision.
In clubfoot the deformity points inward and downward, so Ponseti casting abducts and supinates the forefoot around the talar head. In CVT the deformity points the opposite way — the forefoot is dorsiflexed and abducted and the talonavicular joint is dislocated dorsally — so the correction is in the OPPOSITE direction: you plantarflex and adduct the forefoot to bring the navicular around and onto the talar head, stretching the tight dorsolateral structures. Correct the hindfoot equinus last with a percutaneous tenotomy, exactly as in Ponseti but in reverse.
- Correcting the equinus before the talonavicular joint is reduced forces a rocker-bottom rather than a true reduction — the equinus is corrected LAST.
- Over-forcing the tight dorsolateral structures risks pressure sores and skin necrosis — serial gentle correction over weeks is the point.
- Pinning a joint that is not truly reduced because reduction was not confirmed in two planes on fluoroscopy.
- K-wire migration and pin-tract infection — bend and pad the wire, incorporate it in the cast, and review at the scheduled interval.
Aftercare & Complications
Casting and bracing protocol | Phase | Timing | Immobilisation | Milestones | |-------|--------|----------------|------------| | Theatre cast | 0 to 6 to 8 weeks | Long-leg cast, knee flexed, K-wire incorporated and bent | Parents counselled on cast care and red-flag signs | | Wire removal | 6 to 8 weeks | K-wire removed in clinic; short further cast if needed | Confirm maintained talonavicular reduction | | Bracing | Months to years | Foot abduction orthosis / moulded AFO — full-time, then night-time | Compliance is the key modifiable factor preventing recurrence | | Surveillance | Through growth | None; review for recurrence, equinus, footwear fit | Forced plantar flexion lateral view if recurrence suspected | Surveillance and follow-up. Review regularly through growth for recurrence (return of forefoot abduction and rocker-bottom), equinus and footwear fit, with radiographic surveillance — again the forced plantar flexion lateral view — when recurrence is suspected. Lifelong follow-up is appropriate, as recurrence, avascular necrosis and stiffness can declare themselves years later. Special case — neuromuscular and syndromic CVT. The reverse-Ponseti pathway still applies, but the threshold for a limited open reduction is lower and the recurrence rate is higher. Treat the foot in the context of the whole child: seating and mobility goals, the natural history of the underlying condition (for example, muscle imbalance in cerebral palsy or arthrogryposis), and the likely need for later soft-tissue balancing or bony surgery. Counsel families honestly — the goal in a syndromic or neuromuscular foot is a plantigrade, braceable, painless foot, and a perfect radiographic reduction may not be achievable or necessary. Special case — late presentation. A child presenting after walking age, or with a long-standing rigid deformity, may not fully correct with casting alone. These feet more often require an open reduction through a limited dorsolateral and medial approach, with soft-tissue balancing, and may need later bony correction. The principles are unchanged: reduce the talonavicular joint, correct the equinus, preserve the talar blood supply, and brace. Complications
- Incidence
- Lower with the minimally invasive method; higher after extensive release
- Recognition
- Pain and stiffness of the hindfoot; radiographic sclerosis, fragmentation and shortening of the talar body over months to years
- Prevention and management
- Prevention: minimise peritalar dissection; prefer the reverse-Ponseti method and limited open reduction. Management: observation and activity modification in mild cases; salvage such as arthrodesis only for severe symptomatic collapse later
- Incidence
- Higher in neuromuscular and syndromic feet and with poor bracing compliance
- Recognition
- Return of the rocker-bottom and forefoot abduction; the talonavicular joint re-dislocates on a forced plantar flexion view
- Prevention and management
- Prevention: confirm intraoperative reduction on fluoroscopy; enforce full-time then night-time bracing. Management: repeat serial casting and re-pinning for early recurrence; for established recurrence, a limited or more extensive open reduction with soft-tissue balancing
- Incidence
- Commoner after extensive release; reduced with the Dobbs method
- Recognition
- Reduced subtalar and ankle range of motion; difficulty with footwear and activity
- Prevention and management
- Prevention: avoid extensive capsular dissection; the minimally invasive method preserves motion. Management: physiotherapy and activity-based mobilisation; accept a well-aligned but somewhat stiff foot over a mobile but deformed one
- Incidence
- Risk in extensive open release over tight dorsal skin
- Recognition
- Edge necrosis, dehiscence or full-thickness skin loss over the dorsal incision
- Prevention and management
- Prevention: minimise the incision; handle tight dorsal skin gently; avoid over-tight closure. Management: local wound care; rarely skin grafting or flap cover for significant loss
- Incidence
- Low with meticulous pin and cast care
- Recognition
- Erythema and discharge around the K-wire; loosening of the cast; fever in severe cases
- Prevention and management
- Prevention: bend and pad the wire, incorporate it in the cast, review at the scheduled interval, counsel parents on red-flag signs. Management: oral antibiotics and pin care for mild infection; wire removal and intravenous antibiotics if needed for severe infection
- Incidence
- Variable; commoner in syndromic or neuromuscular feet
- Recognition
- Persistent forefoot abduction, residual equinus or incomplete talonavicular reduction at the end of treatment
- Prevention and management
- Prevention: confirm full intraoperative reduction and adequate equinus correction; adhere to bracing. Management: targeted repeat casting or limited surgery for the specific residual element; set realistic expectations in neuromuscular feet
Recurrence is the main late failure and is highest with non-compliant bracing and in neuromuscular or syndromic feet. Set expectations from the outset, emphasise full-time then night-time bracing at every visit, and commit to long-term follow-up — recurrence, avascular necrosis and stiffness can declare themselves years later.
Viva & Exam Focus
VERTICALVERTICAL — recognising congenital vertical talus
REVERSEREVERSE — the Dobbs (reverse-Ponseti) method
The trap: calling a flexible foot "vertical talus" and sending it to theatre. Oblique talus looks similar at rest but is reducible. The fix: a forced plantar flexion lateral radiograph — in oblique talus the talonavicular joint reduces and the talar axis aligns with the first metatarsal; in true CVT it does not.
The trap: treating the convex sole as the problem. The fix: the rocker-bottom is the result of the vertical talus and the uncorrected hindfoot equinus. Reduce the talonavicular joint and correct the equinus and the rocker-bottom resolves — there is no direct "sole" procedure.
The trap: operating on the foot in isolation in a child with an undiagnosed neural tube defect or syndrome. The fix: examine the spine, hips and the rest of the child — about half of CVT cases are associated with myelomeningocele, arthrogryposis, cerebral palsy, Larsen or Beals syndrome.
The hazard: the talus has a precarious end-arterial blood supply. Extensive peritalar capsular release and dissection around the talar neck jeopardise it. The risk: AVN of the body — fragmenting, shortening, pain and a stiff hindfoot years later. The minimally invasive Dobbs method was designed to minimise this dissection.
The trap: applying standard clubfoot casting mechanics. The fix: in clubfoot you abduct and supinate the forefoot around the talar head; in CVT you plantarflex and adduct the forefoot to bring the navicular onto the talar head, stretching the tight dorsolateral structures, then correct the equinus last with an Achilles tenotomy.
Why it differs: neuromuscular imbalance and abnormal muscle forces (peroneal and extensor over-pull) drive recurrence, compounded by bracing non-compliance. Implication: recurrence and residual deformity are more frequent than in idiopathic feet — counsel on mandatory full-time then night-time bracing and a higher re-operation rate from the outset.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A newborn is referred with a rigid rocker-bottom right foot. The forefoot is abducted and dorsiflexed, the hindfoot is in fixed equinus, and you can feel a firm medial prominence in the sole that does not reduce with manipulation. How do you confirm the diagnosis and establish the initial management?”
“Talk me through the Dobbs reverse-Ponseti method for an idiopathic congenital vertical talus, step by step.”
“A child with a myelomeningocele and a congenital vertical talus has completed the reverse-Ponseti casting and had a percutaneous tenotomy and talonavicular pinning. At 18 months there is clear recurrence of the rocker-bottom deformity. How do you manage this?”
Key diagnosis points
- CVT = a rigid rocker-bottom flatfoot: vertical talus, fixed dorsal talonavicular dislocation, fixed hindfoot equinus
- Diagnostic test = forced plantar flexion lateral radiograph: talonavicular stays dislocated and talar axis stays off the first metatarsal
- Oblique talus is flexible and REDUCES on forced plantar flexion — managed non-operatively; do not call it CVT
- Positional calcaneovalgus foot is fully correctable and resolves spontaneously — no surgery
- Incidence roughly 1 in 10,000; bilateral in about half; about half are syndromic or neuromuscular
Always screen for a cause
- Neural tube defect (myelomeningocele) — examine the spine
- Arthrogryposis, cerebral palsy — examine tone and joints throughout
- Syndromes — Larsen (multiple joint dislocations), Beals (contractural arachnodactyly)
- Examine the hips for associated dysplasia and arrange spinal and hip imaging
- Treat the foot within the context of the whole child and the underlying diagnosis
Surgical anatomy
- Talus: long axis nearly vertical and parallel to the tibia; talar head bulges into the plantar arch producing the rocker-bottom
- Navicular: dislocated dorsally and laterally onto the talar neck, irreducible
- Hindfoot: calcaneus fixed in equinus; corrected last by percutaneous tendo-Achilles tenotomy
- Forefoot: abducted and dorsiflexed by tight long toe extensors and peronei — the target of casting
- Talar blood supply is end-arterial through the neck and tarsal sinus — extensive dissection risks avascular necrosis
Why it is 'reverse' Ponseti
- Clubfoot: abduct and supinate the forefoot around the talar head; CVT: plantarflex and adduct the forefoot — the opposite direction
- Borrowed from Ponseti: serial gentle casting and correction of equinus last with a percutaneous tenotomy
- Phase one: four to seven weekly casts to seat the navicular onto the talar head
- Phase two: percutaneous tendo-Achilles tenotomy and percutaneous talonavicular pinning (limited open reduction if incomplete)
- Phase three: long-leg cast with wire for six to eight weeks, then foot abduction orthosis for years
Operative technique — key steps
- Confirm true CVT on the forced plantar flexion view; exclude flexible oblique talus
- Serial weekly casting — plantarflex and adduct the forefoot around the talar head; correct the equinus last
- Confirm talonavicular reduction on fluoroscopy in two planes; limited open reduction if incomplete
- Percutaneous K-wire across the talonavicular joint to hold reduction
- Percutaneous tendo-Achilles tenotomy to correct the residual hindfoot equinus
- Long-leg cast with knee flexed, wire incorporated, for six to eight weeks
- Wire removal then foot abduction orthosis — full-time then night-time for years
Danger zones
- Talar blood supply: extensive peritalar dissection is the principal cause of talar avascular necrosis — keep dissection minimal
- Correcting the equinus before the talonavicular joint is reduced forces a rocker-bottom, not a true reduction
- Pinning an unreduced joint because reduction was not confirmed in two planes on fluoroscopy
- The dorsolateral structures are tight and contracted — over-forcing risks pressure sores and skin necrosis
- K-wire migration and pin-tract infection — bend and pad the wire, review the cast at the scheduled interval
Complications
- Talar avascular necrosis: lower with the minimally invasive method; recognised after extensive release
- Recurrence or incomplete reduction: commoner in neuromuscular and syndromic feet and with poor bracing compliance
- Stiffness: reduced with the Dobbs method; commoner after extensive release
- Wound problems and pin-tract infection: minimised by limited dissection and meticulous pin and cast care
- Residual deformity: accept a well-aligned but somewhat stiff foot over a mobile but deformed one
Special cases
- Neuromuscular or syndromic CVT: same pathway, lower threshold for limited open reduction, higher recurrence — goal is a plantigrade, braceable, painless foot
- Late presentation (after walking age): casting alone often insufficient; may need limited open reduction and later bony correction
- Bracing compliance is the single most important modifiable factor in preventing recurrence
- Lifelong follow-up for recurrence, avascular necrosis and stiffness through growth
- The reverse-Ponseti method has largely replaced the historical extensive single-stage soft-tissue release
Background & Evidence
Epidemiology. Congenital vertical talus is rare, with an incidence commonly cited at roughly 1 in 10,000 live births. It is bilateral in about half of cases and roughly equally distributed between the sexes. About half of all cases are syndromic or neuromuscular rather than idiopathic, which is why screening the whole child is mandatory. Pathoanatomy — the deformity in three dimensions. Understanding the pathoanatomy is what makes the reduction make sense. The deformity is a fixed dorsal and lateral dislocation of the navicular on the talus, with the talus itself tipped into vertical alignment and the hindfoot locked in equinus.
- The talus: its long axis is nearly vertical, lying close to the long axis of the tibia rather than running forward to the toes; the talar head and neck point plantarward and medially into the plantar arch, producing the firm medial sole prominence and the rocker-bottom.
- The talonavicular joint: the navicular is dislocated dorsally and laterally onto the talar neck, not sitting in front of the talar head where it belongs; the capsule is tight and contracted dorsolaterally and attenuated on the plantar side.
- The hindfoot: the calcaneus is fixed in equinus — the tendo-Achilles and the posterior ankle capsule are tight and will not allow the heel down.
- The forefoot: abducted and dorsiflexed relative to the hindfoot, held there by the tight long toe extensors (extensor hallucis longus, extensor digitorum longus) and the peronei — the very structures the serial casting stretches. The vascular hazard. The talus is the structure most at risk in any CVT surgery. Its blood supply is largely through vessels entering the neck and the tarsal sinus, with limited collateral flow to the body. The historical extensive release stripped and incised widely around the talar head and neck; the consequence was a recognisable rate of avascular necrosis of the talar body. The entire rationale for moving to the minimally invasive Dobbs method was to obtain reduction while leaving the peritalar soft tissues and the talar blood supply as undisturbed as possible. Why the shift away from extensive release. Historically, CVT was treated by an extensive single-stage open soft-tissue release — lengthening of the long toe extensors and peronei, release of the talonavicular and calcaneocuboid capsules, a posterior release for equinus, and reduction held with multiple K-wires. While it could correct alignment, it carried real risks: talar avascular necrosis from extensive peritalar dissection, marked stiffness, wound problems over tight dorsal skin, and a not-trivial recurrence rate. The minimally invasive Dobbs method was developed specifically to obtain comparable correction with far less dissection. Important caveats in the evidence. The best-reported results are in idiopathic CVT; outcomes in syndromic and neuromuscular feet are less consistent, with higher recurrence and residual deformity. Recurrence is closely tied to orthosis compliance — families who do not maintain full-time then night-time bracing recur more often. Long-term follow-up studies are still maturing; mid-term correction is excellent, but lifelong surveillance for recurrence, avascular necrosis and stiffness is appropriate.
References
Early results of a new method of treatment for idiopathic congenital vertical talus
- The foundational description of the reverse-Ponseti method: serial manipulation and casting, then a percutaneous tendo-Achilles tenotomy and percutaneous talonavicular pinning with a limited open reduction if closed reduction was incomplete
- Reported good clinical and radiographic correction of idiopathic CVT with minimal soft-tissue dissection
- Established the modern standard that has largely replaced extensive single-stage soft-tissue release
Idiopathic CVT should be treated first by serial casting and limited surgery rather than by an extensive open release, reducing the dissection-related risks of talar avascular necrosis and stiffness.
Surgical correction of congenital vertical talus under age 2 years
- Described a single-stage dorsal open reduction of the talonavicular dislocation in infants under 2 years of age
- An influential pre-Dobbs surgical standard emphasising early reduction through a dorsal approach
- Set the historical benchmark for open reduction against which the later minimally invasive method was compared
Single-stage open reduction can correct CVT in infants but involves greater dissection than the reverse-Ponseti method; it remains an option when casting fails or for late-presenting rigid deformity.
Congenital vertical talus (instructional review)
- Authoritative instructional review defining the pathoanatomy of the vertical talus and the rigid rocker-bottom deformity
- Established the radiographic diagnosis and the role of the forced plantar flexion view
- Documented the historical extensive soft-tissue release that preceded the minimally invasive era
The review codified the pathoanatomy and diagnostic principles examiners still test today, and frames why a less invasive method was sought.
Treatment of congenital vertical talus: comparison of minimally invasive and extensive soft-tissue release procedures at minimum five-year follow-up
- Direct comparison of the minimally invasive Dobbs method against the historical extensive single-stage soft-tissue release, with a minimum five-year follow-up
- Demonstrated that the minimally invasive method achieved comparable radiographic correction with fewer complications and better ankle motion than extensive release
- Found that extensive release had higher rates of talar avascular necrosis and stiffness, supporting the shift to the reverse-Ponseti approach
The Dobbs minimally invasive method provides durable correction of CVT with lower rates of avascular necrosis and stiffness than extensive soft-tissue release, confirming it as the preferred surgical approach.