Volar opening-wedge or dorsal closing-wedge extra-articular osteotomy plus structural bone graft for symptomatic distal radius malunion · advanced
- Restoration of three radiographic parameters is the surgical target: volar tilt (normal 11 degrees), radial height (normal 11-12 mm) and radial inclination (normal 22-23 degrees). Under-correction in any plane is the commonest cause of persistent pain and weakness.
- Two principal extra-articular techniques: a volar OPENING-wedge osteotomy (preferred for dorsal angulation, the common Colles pattern — restores volar tilt by wedging open the volar cortex) and a dorsal CLOSING-wedge osteotomy (preferred for the rarer volar angulation, the Smith pattern). Bone graft (tricortical iliac crest wedge, structural allograft or synthetic substitute) fills the opening-wedge defect and is NOT optional there.
- DRUJ dysfunction must be addressed AT THE SAME OPERATION if the malunion has produced ulnar-sided wrist pain, restricted forearm rotation or positive ulnar variance. Options: ulnar shortening osteotomy (most common), wafer resection, or the Sauvé-Kapandji procedure.
- Patient-specific instrumentation (3-D CT templating, custom cutting guides and patient-specific plates) significantly improves accuracy of correction in complex multiplanar deformity — the standard deviation of angular correction falls from approximately 5 degrees with free-hand technique to about 2 degrees when guided.
- The 'cortical step' on the volar radius is the volumetric marker of dorsal malunion. A corrective osteotomy is EXTRA-ARTICULAR for most malunions; INTRA-ARTICULAR osteotomy is reserved for young patients with a discrete articular step and no significant radiocarpal arthritis.
- Positive ulnar variance greater than 2 mm after correction is poorly tolerated; perform a concurrent ulnar shortening osteotomy in the same anaesthetic if pre-op variance is positive or expected to remain positive after correction.
When & Why
Indication. A distal radius malunion becomes a surgical indication when ALL THREE of the following are present — deformity beyond acceptable limits, symptoms attributable to that deformity, and failure of non-operative management (rest, activity modification, hand therapy, a trial of splinting or medication). Deformity thresholds that justify surgery:
- Dorsal tilt greater than 10-15 degrees, radial shortening greater than 3-5 mm, loss of radial inclination greater than 5 degrees, or an intra-articular step greater than 2 mm. Absolute indications. Dorsal angulation greater than 20-25 degrees with significant functional impairment and no radiocarpal arthritis; radial shortening greater than 5 mm with positive ulnar variance and ulnocarpal abutment; an intra-articular step greater than 2 mm in a young patient (under 45-50) with a discrete fragment and preserved cartilage; disabling DRUJ dysfunction (loss of pronosupination, painful clicking, arthrosis) at least partly due to the malunion; and midcarpal instability (VISI) secondary to the malunion. Relative indications. Radial shortening 3-5 mm with mild-to-moderate symptoms; dorsal tilt 10-20 degrees with weakness; concurrent carpal tunnel syndrome from the malunited volar cortex (a volar osteotomy decompresses simultaneously); and patient preference for correction after detailed counselling. Contraindications. Absolute: established radiocarpal or DRUJ arthritis (a salvage procedure — partial/total wrist fusion or arthroplasty — is preferred), active infection, or medical unfitness for anaesthesia with no reversible component. Relative: a heavy smoker unwilling to stop (markedly elevated nonunion risk — offer a cessation programme first), pre-existing complex regional pain syndrome (predicts worse outcomes — proceed cautiously), significant osteopenia that may compromise fixation, and low functional demand with tolerable symptoms. Consent. Discuss nonunion, under- or over-correction, tendon rupture (FPL, EPL), neurovascular injury (median nerve, radial artery), DRUJ symptoms persisting, plate-related symptoms requiring removal, complex regional pain syndrome, stiffness, and the prolonged recovery — often 6-12 months to maximal improvement. Setup. Supine, arm abducted on a hand table, upper-arm tourniquet (250-300 mmHg), image intensifier on the opposite side with full AP and lateral access throughout. General or regional (axillary brachial plexus) anaesthesia; consider a supplemental regional catheter for post-op analgesia. Pre-operative templating is mandatory: bilateral PA, lateral and oblique radiographs; CT with 3-D reconstruction for any complex or multiplanar deformity; measure the contralateral radial height, volar tilt, inclination and ulnar variance; and calculate the osteotomy wedge size, location and correction angle. Patient-specific cutting guides and pre-contoured plates can be manufactured from the CT data.
The Operation
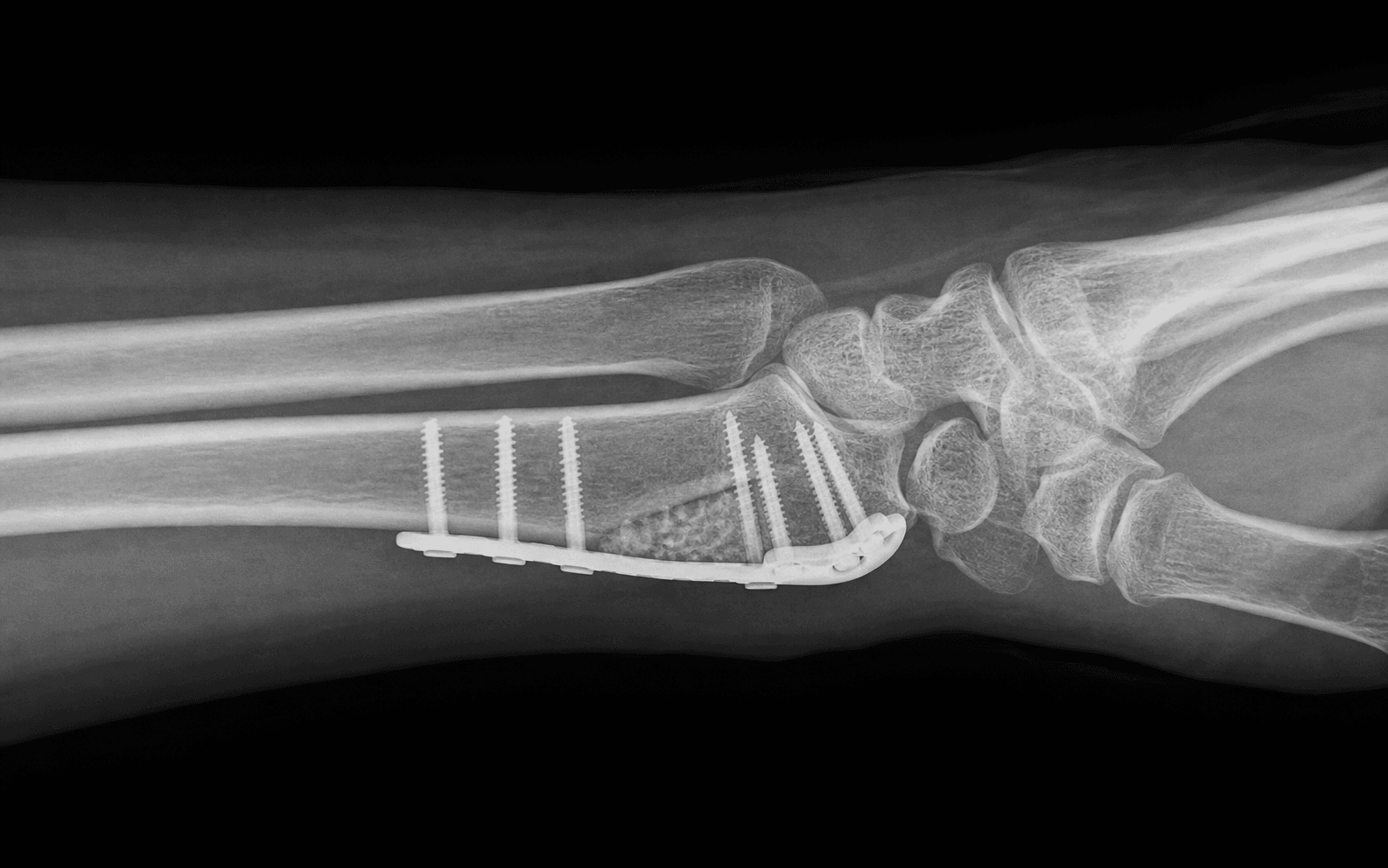
The goal is to restore the three radiographic parameters, neutralise ulnar variance and address any DRUJ pathology — in one operation. The workhorse for the common dorsal (Colles) malunion is the volar opening-wedge osteotomy: expose the distal radius through a volar Henry approach, cut the metaphysis leaving the dorsal cortex as a hinge, open the wedge to the templated height, pack in a structural graft, and lock a volar plate with its distal edge proximal to the watershed line.
Volar opening-wedge osteotomy — operative sequence
- Supine, arm abducted on a hand table, upper-arm tourniquet (250-300 mmHg), image intensifier on the opposite side with full AP and lateral access throughout.
- General or regional (axillary brachial plexus) anaesthesia; consider a regional catheter for post-op analgesia.
- Re-confirm the templated correction against intra-operative imaging before scrubbing — osteotomy level, wedge size, planned volar tilt/radial height/inclination, and any concurrent DRUJ procedure.
- A standard volar Henry approach between FCR and the radial artery; elevate the pronator quadratus from its radial origin (radial-to-ulnar), preserving it for later repair over the plate.
- Extend the exposure distally into the carpal tunnel only if a concurrent release is planned.
- Structures at risk in this layer: the median nerve and FPL on the volar surface, the radial artery (retract radially with brachioradialis), and the palmar cutaneous branch of the median nerve (emerges between FCR and the radial artery — protect with a sub-FCR approach).
- On fluoroscopy, mark the osteotomy line in the metaphysis — perpendicular to the long axis of the radius in the coronal plane and at the apex of the deformity in the sagittal plane.
- The typical reference is 15-20 mm proximal to the articular surface; confirm the needle marker in BOTH AP and lateral before cutting. Too distal enters the radiocarpal joint; too proximal risks the median nerve and FPL and gives poor fixation.
- With a thin oscillating saw — cooled with saline to avoid thermal necrosis — cut perpendicular to the long axis, stopping at (but not breaching) the dorsal cortex, which is left intact as a hinge.
- Confirm the cut is complete and the distal fragment is mobile on the dorsal hinge (complete the cut with an osteotome if needed). Breaching the dorsal cortex risks the EPL tendon and the extensor compartments.
- Insert a small laminar spreader or osteotome and gradually open the volar cortex; the dorsal cortex acts as the hinge. Open symmetrically to the templated height.
- Rough rule (guidance only): 1 mm of opening corresponds to approximately 1 degree of tilt correction. Confirm volar tilt restoration on the lateral fluoroscopic image; radial height and inclination correct automatically as the wedge opens.
- Shape the structural graft — tricortical iliac crest autograft is the gold standard; structural allograft, synthetic calcium-phosphate wedges or cancellous chips are alternatives — to fit the wedge defect.
- Impact it gently so it is fully seated and flush with the volar cortex; it provides the structural support that holds the correction and restores radial height. An oversized graft overdistends the soft tissues; an undersized or non-structural graft collapses with loading.
- Insert 2-3 K-wires across the osteotomy and graft for provisional fixation; confirm position on fluoroscopy.
- Apply a pre-contoured volar locking distal radius plate with the DISTAL edge PROXIMAL to the watershed line (the transverse ridge 2-3 mm proximal to the articular surface) to avoid FPL attrition rupture.
- Place distal locking screws in the subchondral bone under fluoroscopy; ensure at least 3-4 bicortical screws proximal to the osteotomy and check that no screw penetrates the dorsal cortex into the extensor compartments.
- Confirm on AP, lateral and oblique: volar tilt approximately 11 degrees, radial height within 2 mm of the contralateral side, radial inclination 22-23 degrees, ulnar variance neutralised, no intra-articular screw penetration, the plate proximal to the watershed line, and the graft well seated.
The distal edge of any volar plate MUST lie proximal to the watershed line, the transverse volar ridge 2-3 mm from the articular surface. A plate or proud distal screw lying distal to it erodes the FPL tendon and causes attritional rupture 3-12 months post-op. Confirm the distal edge position with fluoroscopy before final tightening, and check every screw length in multiple views so none breaches the dorsal cortex toward the extensor compartments. During the exposure itself, protect the median nerve (avoid prolonged forceful retraction — release the carpal tunnel if symptomatic) and retract the radial artery radially with brachioradialis before any bone work.
One millimetre of wedge opening corresponds to approximately one degree of tilt correction in a typical radius (a guide only — always confirm against the pre-op plan and intra-operative imaging). Mark the osteotomy with a needle and verify in BOTH AP and lateral before cutting; the cut is perpendicular to the long axis of the radius at the apex of the deformity.
A dorsal (Colles) malunion is corrected with a volar OPENING-wedge: the shortened volar cortex is wedged open and a structural graft restores length and volar tilt, plating the strong tension side. A dorsal closing-wedge is reserved for the rarer volar (Smith) angulation — it works from the dorsal side and carries EPL risk. Matching the approach to the deformity direction is the first decision.
Variation: dorsal closing-wedge osteotomy (for volar / Smith angulation) - Indication. Volar angulation (Smith pattern) — uncommon.
- Exposure — dorsal. Longitudinal incision centred over Lister's tubercle; release the EPL sheath and retract the EPL tendon; reflect the extensor retinaculum to expose the third and fourth extensor compartments. A posterior interosseous nerve (PIN) neurectomy is often added to denervate the dorsal wrist capsule.
- Cuts. Plan a closing-wedge on the lateral view with the base dorsal and the apex on the volar cortex; make two parallel transverse metaphyseal cuts leaving the volar cortex intact as a hinge, remove the wedge, and close the osteotomy.
- Fixation. A low-profile dorsal plate (to reduce EPL attrition), or K-wires plus a volar neutralisation plate; confirm the correction on fluoroscopy.
EPL rupture after dorsal plating comes from drilling or screw penetration into the third compartment or from a prominent dorsal plate/screw tip. Release the EPL sheath and retract the tendon, measure drill depth and screw length precisely so the dorsal cortex is not breached, use a low-profile plate, and confirm the planned correction on lateral imaging to avoid over-correcting into a Colles pattern.
Variation: intra-articular osteotomy - Indication. A young patient (typically under 45) with a discrete intra-articular step greater than 2 mm, no radiocarpal arthritis, and fragments large enough to hold fixation; best performed within 6-12 months of injury.
- Technique. Volar or dorsal approach depending on the step; capsulotomy to expose the joint; mobilise the displaced fragment and reduce it anatomically under direct vision; fix with headless compression screws, mini-fragment plates or K-wires; confirm reduction with arthroscopy and fluoroscopy. Outcomes are best when cartilage is preserved and correction is early; long-term post-traumatic arthritis risk remains higher than after extra-articular osteotomy. ## Concurrent DRUJ procedure - Decision. Indicated when there is positive ulnar variance with ulnocarpal abutment and/or DRUJ arthrosis; the choice depends on TFCC status, arthrosis, ulnar variance and patient factors.
- Ulnar shortening osteotomy (most common). Separate incision over the distal ulna; transverse or oblique diaphyseal osteotomy; shorten to neutral variance (0-1 mm); dedicated 6-7 hole compression plate.
- Wafer resection (distal ulna arthroplasty). For positive ulnar variance less than 4 mm with TFCC pathology amenable to repair; resect 2-4 mm of the distal ulnar head through a small arthrotomy, preserving the ulnar styloid base and TFCC attachments (arthroscopic option).
- Sauvé-Kapandji. For DRUJ arthrosis with positive variance, or failed ulnar shortening; a distal radioulnar arthrodesis with creation of a proximal ulnar pseudarthrosis (resect 1-1.5 cm of ulna proximal to the arthrodesis).
- Order of procedures. Many surgeons fix the ulnar side first, then correct the radius, so the final ulnar length is confirmed before the radial correction is set.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | 0–14 days | Short-arm volar splint, wrist neutral | Active finger flexion/extension from day 1; elevation and oedema control; wound check at 48–72 h | | 2 | 2–6 weeks | Removable wrist splint for comfort; sutures out at 10–14 days | Formal hand therapy from 2–4 weeks — active and passive wrist ROM, scar care; radiographs at 2 and 6 weeks | | 3 | 6–12 weeks | Splint for heavy tasks only | Grip strengthening from 6 weeks once union is evident; return to light activities at 6–8 weeks | | 4 | 12 weeks+ | Night splint only if needed | Graded return to manual work and sport at 3–6 months; plate removal (if symptomatic) at 6–12 months | Rehabilitation goals are wrist flexion 60-70 degrees and extension 50-60 degrees, pronation and supination 70-80 degrees each, and grip strength to 70-80 percent of the contralateral side. Most patients return to desk work by about 6 weeks and to manual work by 3-6 months.
- Incidence
- 3-5% after volar plating generally; lower when the watershed line is respected
- Recognition
- Loss of active thumb IP flexion; sudden onset typically 3-12 months post-op
- Prevention and management
- Prevention: distal plate edge proximal to the watershed line; check screw lengths on multiple views. Management: EIP-to-FPL transfer or palmaris longus interposition graft — primary repair is rarely possible as the rupture is attritional within the tendon substance
- Incidence
- 1-3% after dorsal plating; also reported after non-operative fracture treatment
- Recognition
- Loss of active thumb IP extension; inability to lift the thumb off the table
- Prevention and management
- Prevention: confirm dorsal screw length; protect/retract EPL in the dorsal approach; use low-profile plates. Management: EIP-to-EPL transfer; primary repair may be possible at a discrete site
- Incidence
- 10-20% free-hand; 5-10% with patient-specific guides
- Recognition
- Persistent dorsal tilt, shortening or lost inclination on post-op imaging; persistent symptoms
- Prevention and management
- Prevention: 3-D CT templating and patient-specific guides; intra-operative fluoroscopic confirmation. Management: if symptomatic and significant, a revision osteotomy (much more difficult)
- Incidence
- 5-10%
- Recognition
- Excess volar tilt (greater than 15-20 degrees) producing volar carpal malalignment; rarely carpal tunnel compression
- Prevention and management
- Prevention: intra-operative imaging; compare with the contralateral wrist. Management: rarely needs revision; symptomatic cases may require correction
- Incidence
- Less than 5% in opening-wedge with structural graft; up to 10-15% in smokers
- Recognition
- Pain at the osteotomy site beyond 3-4 months; radiographic lucency at the osteotomy
- Prevention and management
- Prevention: structural bone graft; rigid plate fixation; smoking cessation before surgery. Management: bone grafting and revision fixation; consider a bone stimulator (low-intensity pulsed ultrasound or PEMF)
- Incidence
- 10-20% if not addressed at the index operation
- Recognition
- Ulnar-sided wrist pain, restricted pronosupination, painful clicking, positive ballottement
- Prevention and management
- Prevention: pre-op DRUJ assessment and a concurrent procedure when indicated. Management: secondary ulnar shortening, wafer resection, Sauvé-Kapandji or DRUJ arthroplasty
- Incidence
- 1-3%
- Recognition
- Numbness in the median distribution; thenar weakness; positive Phalen/Tinel
- Prevention and management
- Prevention: avoid prolonged forceful retraction; prophylactic carpal tunnel release if pre-op symptoms. Management: splinting, steroid injection, surgical release if persistent
- Incidence
- 2-5%
- Recognition
- Disproportionate pain, stiffness, vasomotor changes and swelling beyond the expected course
- Prevention and management
- Prevention: vitamin C 500 mg daily for 50 days (some evidence after distal radius fracture); early mobilisation. Management: multimodal — physiotherapy, NSAIDs, bisphosphonates, sympathetic blocks, neuropathic agents
- Incidence
- 20-40% long-term
- Recognition
- Pain, irritation, or FPL/EPL symptoms related to the implant
- Prevention and management
- Prevention: low-profile plate; watershed-line position (volar). Management: plate removal after union, typically 6-12 months post-op
- Incidence
- Common; significant in 5-10%
- Recognition
- Reduced wrist flexion, extension, pronation or supination versus the contralateral side
- Prevention and management
- Prevention: early mobilisation; hand therapy; elevation and oedema control. Management: intensive therapy, dynamic splinting; consider manipulation under anaesthesia if severe at 4-6 months
- Incidence
- 10-30% have some donor-site pain
- Recognition
- Pain, numbness, haematoma or rarely hernia at the harvest site
- Prevention and management
- Prevention: minimise harvest dissection; use allograft or synthetic substitute in selected patients. Management: usually self-limiting; analgesics; rare surgical management of haematoma or hernia
Viva & Exam Focus
RADIUSRADIUS — Pre-operative planning parameters
WEDGEWEDGE — Choosing the osteotomy direction
The trap: accepting residual dorsal tilt greater than 5-10 degrees because the wedge was undersized or the plate was applied before the target correction was reached. The fix: confirm the wedge on fluoroscopy matches the pre-op plan — volar tilt should be restored to roughly 11 degrees. Under-correction causes persistent midcarpal instability, extension weakness and ulnocarpal abutment.
The trap: failing to recognise that the malunion has shortened the radius (usually an impacted dorsal fracture) so ulnar-sided pain persists unless the radius is lengthened or the ulna shortened. The fix: calculate pre-op ulnar variance; if greater than 2 mm positive, plan a concurrent ulnar shortening or wafer resection and confirm neutral variance on intra-operative imaging.
The trap: correcting the radius but leaving a symptomatic DRUJ with restricted pronosupination, a positive ballottement, or arthrosis. The fix: assess the DRUJ clinically (ballottement, piano-key, press test) and on CT (pronation, supination, neutral) and plan ulnar shortening, wafer or Sauvé-Kapandji in the same anaesthetic when significant.
The trap: a prominent volar plate or distal screw causing attritional FPL rupture — the commonest tendon complication of volar plating. The fix: position the distal plate edge proximal to the watershed line, check screw lengths so none breaches the dorsal cortex, and use low-profile plates; exchange any screw that is too long.
The trap: attritional EPL rupture from drilling or screw penetration into the third compartment, or from prominent dorsal screw tips. The fix: confirm screw length in multiple views so the dorsal cortex is not breached; in the dorsal approach release the EPL sheath and protect/retract the tendon. EPL rupture is also reported after non-operative distal radius fractures.
The trap: an opening- or closing-wedge that fails to unite — usually from inadequate fixation, smoking, or absent/non-structural graft. The fix: use structural graft in the opening-wedge, ensure rigid fixation with at least 3 cortical screws on each side of the osteotomy, and counsel smokers to stop — nicotine impairs healing.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old right-hand-dominant electrician sustained a distal radius fracture 8 months ago, treated non-operatively. He now has dorsal tilt of 25 degrees, radial shortening of 6 mm, and a 3 mm intra-articular step. He has pain, weakness, and cannot return to work. How do you manage this?”
“A 38-year-old woman had a distal radius ORIF with a volar locking plate 14 months ago. She has been told she has a malunion with 18 degrees of dorsal tilt. She has wrist pain, weakness, and cannot return to her work as a chef. What is the most appropriate management?”
“A 52-year-old man with a distal radius malunion has 22 degrees of dorsal tilt, radial shortening of 5 mm, and DRUJ symptoms with positive ballottement and a press test. Non-operative management has failed. Describe your surgical plan.”
Key diagnosis points
- Three radiographic parameters: volar tilt (normal 11 degrees), radial height (11-12 mm), radial inclination (22-23 degrees)
- Operate when deformity is significant AND symptoms are present AND non-operative management has failed
- Thresholds: dorsal tilt greater than 10-15 degrees, radial shortening greater than 3-5 mm, intra-articular step greater than 2 mm
- Assess the DRUJ — ballottement, press test, piano-key, pronosupination; CT for arthrosis
- Carpal alignment: dorsal malunion commonly produces DISI, which corrects as volar tilt is restored
Pre-operative planning
- Bilateral wrist radiographs (PA, lateral, oblique) — measure all three parameters against the uninjured side
- CT with 3-D reconstruction is mandatory for multiplanar or complex deformity
- Patient-specific cutting guides and pre-contoured plates improve accuracy in complex cases
- Rule out radiocarpal arthritis — a salvage procedure may be more appropriate
- MRI or arthroscopy for TFCC and chondral assessment in intra-articular malunion
Indications
- Dorsal tilt greater than 10-15 degrees, radial shortening greater than 3-5 mm, or intra-articular step greater than 2 mm
- Failed non-operative management (rest, splinting, hand therapy)
- DRUJ dysfunction with restricted pronosupination, ulnocarpal abutment or arthrosis
- Midcarpal instability (VISI) from severe dorsal malunion
- Concurrent carpal tunnel syndrome from the malunited volar cortex
Technique — volar opening-wedge key steps
- Volar (Henry) approach between FCR and the radial artery; elevate pronator quadratus
- Mark the osteotomy at the metaphysis (15-20 mm proximal to the articular surface) on fluoroscopy
- Cut with a thin saw, leaving the dorsal cortex as a hinge
- Open the wedge with a laminar spreader; correct volar tilt, radial height and inclination
- Insert structural tricortical iliac crest graft
- Provisional K-wires; apply a volar locking plate with the distal edge proximal to the watershed line
- Confirm correction on AP and lateral fluoroscopy
- Address the DRUJ concurrently (ulnar shortening, wafer, or Sauvé-Kapandji)
Variations & concurrent procedures
- Dorsal closing-wedge: for volar angulation (Smith) — less common; EPL risk
- Intra-articular osteotomy: for young patients with a discrete step and no arthritis — arthroscopy aids reduction
- Patient-specific 3-D guided: complex multiplanar deformity; reduced correction error
- Concurrent ulnar shortening: when positive variance persists after correction
- Concurrent carpal tunnel release: when pre-op CTS symptoms are present
Special cases
- Intra-articular malunion in a young patient: arthroscopy to assess cartilage; anatomical reduction with headless screws; best within 6-12 months of injury
- Concurrent CTS: extended volar approach to release the carpal tunnel and correct the deformity
- Elderly low-demand: consider allograft or synthetic wedges to avoid iliac crest harvest morbidity
- Sauvé-Kapandji: for DRUJ arthrosis with positive variance; create a proximal pseudarthrosis
- Smoking: strong risk factor for nonunion; mandatory cessation before and after surgery
Background & Evidence
The deformity is three-dimensional. A distal radius malunion is a three-plane problem — the classic teaching is to address three radiographic parameters, but the real deformity may include components in the sagittal, coronal and axial planes plus rotation. The operative targets and thresholds: | Parameter | Normal | Significant malunion threshold | Surgical target | |-----------|--------|--------------------------------|-----------------| | Volar tilt | 11 degrees (range 8-12) | Dorsal tilt greater than 10-15 degrees | Restore to within 5 degrees of normal | | Radial height | 11-12 mm | Shortening greater than 3-5 mm | Restore to within 2 mm of contralateral | | Radial inclination | 22-23 degrees | Loss greater than 5 degrees | Restore to normal | | Ulnar variance | 0-1 mm neutral | Positive greater than 2 mm | Neutralise | | Intra-articular step | 0 mm | Step greater than 2 mm | Less than 1 mm | | Radial rotation | Aligned with ulna | Malrotation of the distal fragment | Restore alignment | Pattern recognition. The Colles pattern (dorsal angulation, radial shortening, loss of inclination) is by far the most common and is treated with a volar opening-wedge at the metaphysis. The Smith pattern (volar angulation) is less common and is treated with a dorsal closing-wedge. A Barton-type intra-articular malunion is rare — intra-articular osteotomy only in young patients with preserved cartilage. A die-punch malunion (a depressed lunate facet fragment) is technically demanding intra-articular correction. Osseous anatomy. The osteotomy belongs in the metaphysis — distal to the pronator quadratus insertion, proximal to the subchondral bone. The volar cortex is the shortened side in a typical Colles malunion, which is where the opening-wedge is made. The watershed line is a transverse volar ridge 2-3 mm proximal to the articular surface; the distal edge of any volar plate must lie proximal to it. Neurovascular anatomy. In the volar approach, the median nerve, FPL, radial artery and the palmar cutaneous branch of the median nerve are at risk. In the dorsal approach, the EPL (third compartment), extensor compartments 2-4, the PIN (often resected for capsular denervation) and the dorsal branch of the ulnar nerve are at risk. DRUJ anatomy — the TFCC, the dorsal and volar radioulnar ligaments, the ulnar styloid (base non-union is common but usually asymptomatic) and the ECU subsheath — must all be assessed when ulnar-sided pathology is suspected. Carpal alignment. A malunion with dorsal tilt produces a compensatory carpal malalignment — most often a dorsal intercalated segment instability (DISI), less often a volar intercalated segment instability (VISI, which may signal scapholunate or lunotriquetral injury). Correcting the radial tilt usually resolves the adaptive carpal malalignment. A dorsal tilt greater than 20-30 degrees can produce a volar midcarpal instability with a painful clunk; restoring volar tilt is the key to managing it.
- Volar opening-wedge
- Dorsal angulation (Colles pattern) — most common
- Dorsal closing-wedge
- Volar angulation (Smith pattern) — rare
- Patient-specific (3-D)
- Complex multiplanar deformity; revision cases
- Volar opening-wedge
- Volar (Henry)
- Dorsal closing-wedge
- Dorsal (between 3rd and 4th extensor compartments)
- Patient-specific (3-D)
- Either — guided by the deformity
- Volar opening-wedge
- Structural tricortical iliac crest; structural allograft or substitute alternatives
- Dorsal closing-wedge
- Cancellous autograft chips; the removed bone forms the graft
- Patient-specific (3-D)
- Structural or cancellous depending on the technique
- Volar opening-wedge
- Volar locking plate with structural graft — very stable
- Dorsal closing-wedge
- Plate plus compression — stable but smaller contact area
- Patient-specific (3-D)
- Pre-contoured plate; often more bone contact
- Volar opening-wedge
- FPL attritional rupture over a prominent plate — meticulous distal plate position
- Dorsal closing-wedge
- EPL rupture from dorsal drilling or prominent screw tips
- Patient-specific (3-D)
- Plate designed to sit proximal to the watershed line
- Volar opening-wedge
- Moderate — free-hand technique
- Dorsal closing-wedge
- Moderate — free-hand technique
- Patient-specific (3-D)
- High — custom guides/plates reduce error
Outcomes of corrective osteotomy. Pooled case-series evidence (systematic review, Lozano-Calderon 2006, PENDING PMID) reports approximately 70-90 percent good-to-excellent results for pain relief and restoration of grip strength. Most series report 60-80 percent of patients achieving meaningful pain reduction, an average grip-strength improvement of 30-50 percent of the contralateral side, and modest gains in the flexion-extension arc (typically 10-20 degrees), with more predictable correction of pronosupination when the DRUJ is addressed. 3-D CT templating with custom guides improves accuracy — the standard deviation of angular correction falls from approximately 5 degrees (free-hand) to 2 degrees (guided) in comparative series — and patient-specific plates allow precise pre-contoured fixation, particularly in multiplanar deformity.
References
Outcome after corrective osteotomy for malunited fractures of the distal end of the radius
- Case series of corrective osteotomy for malunited distal radius fractures with a mean follow-up of 4.5 years
- Good-to-excellent results in approximately 80% of patients; pain relief was the most consistent outcome
- Grip strength improved to approximately 70% of the contralateral side; range of motion showed modest gains
Corrective osteotomy for intra-articular malunion of the distal part of the radius
- Case series of intra-articular corrective osteotomy for malunited distal radius fractures with an articular step greater than 2 mm
- Best outcomes in young patients (under 45) with early correction and no radiocarpal arthritis at the time of surgery
- Intra-articular osteotomy restored articular congruity and improved DASH scores; functional outcomes were comparable to extra-articular osteotomy in selected patients
Three-dimensional virtual planning of corrective osteotomies of distal radius malunions: a systematic review and meta-analysis
- Systematic review and meta-analysis of 3-D virtual planning for corrective osteotomy of distal radius malunion
- Three-dimensional planning significantly improved accuracy of correction compared with two-dimensional techniques
- Patient-specific guides and pre-contoured plates reduced the standard deviation of angular correction from approximately 5 degrees to 2 degrees
Corrective osteotomy is an effective method of treating distal radius malunions with good long-term functional results
- Long-term cohort (minimum 5 years) of corrective osteotomy for distal radius malunion
- Durable pain relief and functional improvement in the majority of patients
- Progression to radiocarpal arthritis in approximately 15% at long-term follow-up
What surgical technique to perform for isolated ulnar shortening osteotomy after distal radius malunion: a systematic review
- Systematic review of ulnar shortening osteotomy techniques for ulnocarpal abutment after distal radius malunion
- Transverse osteotomy with compression plating was the most commonly reported technique, with reliable pain relief and grip improvement
- Plate removal was required in up to 30% of cases for hardware-related symptoms