Supine position | Dorsal cutaneous nerves at risk | Subperiosteal exposure of shaft, neck and head
- The patient is positioned supine with a tourniquet (250-300 mmHg) and the foot at the end of the table for fluoroscopic access; the dorsal cutaneous nerves are the structures most at risk and must be identified and protected in the subcutaneous plane.
- There is no true internervous plane — the approach works in an extra-compartmental, subperiosteal plane. The purely sensory dorsal cutaneous nerves (branches of the superficial peroneal nerve) are mobilised and protected rather than used as a landmark.
- The extensor digitorum longus and brevis tendons are retracted medially or laterally and never divided, since division causes extensor lag and claw toe.
- One longitudinal incision placed in the intermetatarsal space can expose two adjacent rays; two parallel incisions require a skin bridge of at least 5 mm to avoid necrosis.
- All deep dissection is strictly subperiosteal to protect the dorsalis pedis and dorsal metatarsal arteries in the intermetatarsal spaces and the tenuous retrograde blood supply to the metatarsal head.
When & Why
What it exposes. The dorsal approach gives direct, extensile access to the shafts, necks and heads of the second to fifth metatarsals, from the tarsometatarsal joint proximally to the metatarsophalangeal joint distally. It is the workhorse exposure for forefoot reconstructive surgery and central-ray trauma. Why dorsal. The approach is superficial and relatively bloodless under tourniquet, exploits the natural interval between the extensor tendons, and allows one incision to address two adjacent rays when placed in the intermetatarsal space. No major motor nerve is at risk, and the incision can be extended proximally or distally as required. The plantar approach is rarely used for the lesser metatarsals because it crosses weight-bearing skin and gives poorer access; the medial approach is reserved for the first ray and the lateral approach for the fifth metatarsal base. Primary indications - Weil osteotomy for lesser metatarsalgia and metatarsal length abnormalities
- Open reduction and internal fixation of central-ray metatarsal fractures (neck, shaft or head)
- Surgical management of Freiberg disease (infraction of the lesser metatarsal head)
- Metatarsal head resection for intractable plantar keratosis or Freiberg collapse
- Partial or complete ray amputation for infection, tumour or severe deformity
- Revision surgery for malunion, non-union or a failed previous osteotomy Contraindications and alternatives - Active infection in the skin over the planned incision (consider staging or an alternative)
- Severe peripheral vascular disease with a non-palpable dorsalis pedis pulse (assess perfusion first)
- Previous surgery with extensive scarring that would require a different plane
- Isolated first ray pathology (use the medial approach instead) Approach variants - Single ray — a longitudinal incision directly over one metatarsal, for an isolated fracture or a single Weil osteotomy.
- Two-ray access — one incision placed in the intermetatarsal space between adjacent metatarsals, for a Weil osteotomy of two rays or a central fracture.
- Extended proximal — extended to the tarsometatarsal joint, for Lisfranc involvement or proximal fractures. Position and landmarks. Position the patient supine on a radiolucent table with a thigh or calf tourniquet applied before exsanguination, and place the foot at the very end of the table so the C-arm can obtain true AP, oblique and lateral views of the forefoot from the opposite side without obstruction. Inflate the tourniquet to 250-300 mmHg after exsanguination, slightly plantarflex the ankle to relax the extensor tendons, and pad all pressure points. Palpate and mark the metatarsal heads (palpable on the plantar aspect with dorsal projections), trace the shafts proximally to the tarsometatarsal joints, note the course of superficial dorsal veins to avoid them, and mark the incision directly over the target metatarsal or in the intermetatarsal space. Keep tourniquet time to less than 90 minutes where possible, as prolonged inflation increases the risk of nerve palsy and muscle damage; in patients with peripheral vascular disease consider operating without a tourniquet.
The Exposure
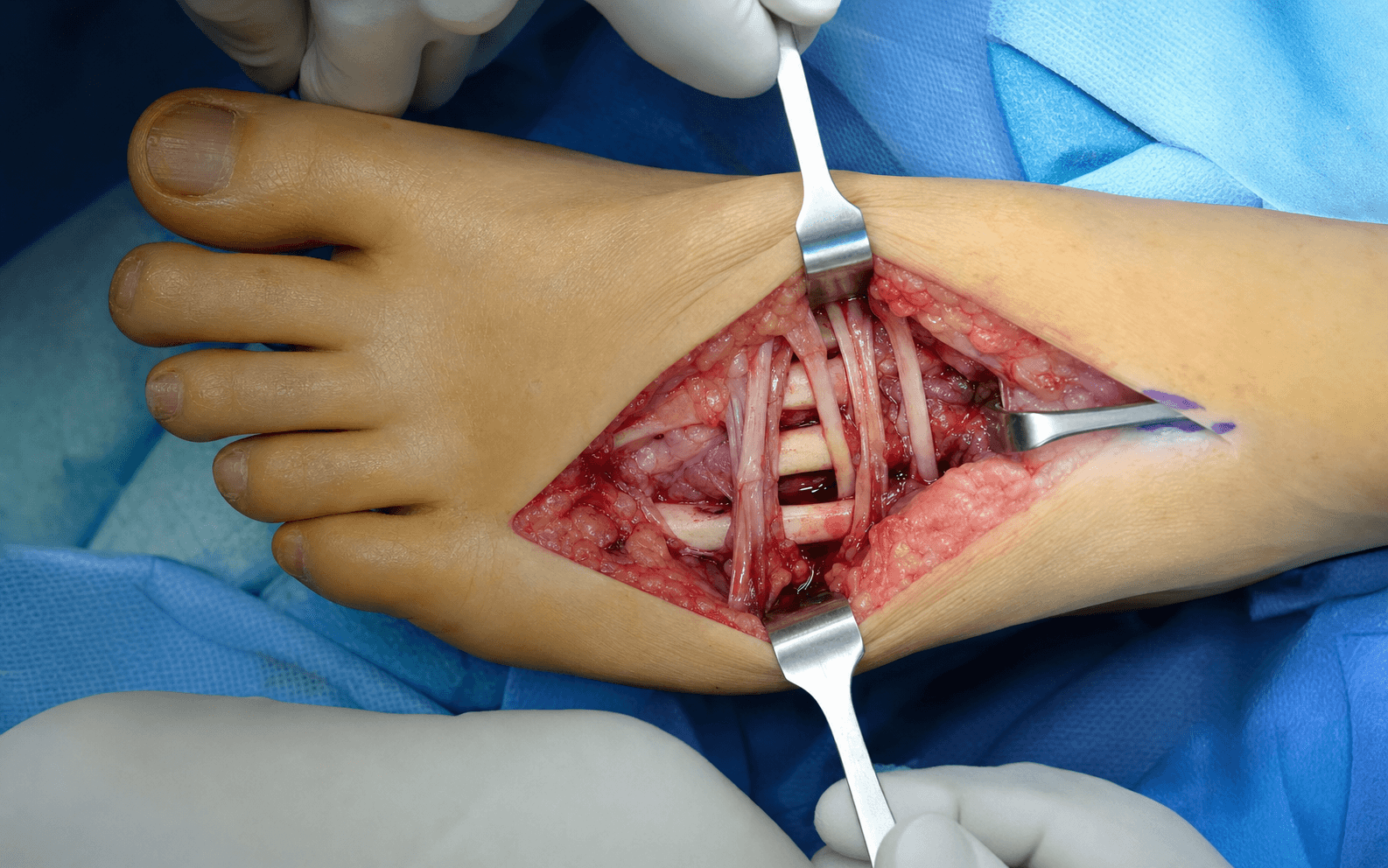
Work down through the layers along the dorsum of the forefoot, protecting the dorsal cutaneous nerves in the subcutaneous plane, retracting the extensor tendons, and then dissecting strictly subperiosteally on bone to the neck and head.
Exposure sequence
- With the patient supine, tourniquet inflated and the foot at the end of the table, make a longitudinal incision directly over the target metatarsal, or in the intermetatarsal space for two-ray access.
- Length is typically 4 to 6 cm centred over the surgical target — the neck for a Weil osteotomy, the shaft for a fracture — and may be extended proximally to the tarsometatarsal joint if base access is required.
- A single intermetatarsal incision exposes two adjacent rays; two parallel incisions need a skin bridge of at least 5 mm to avoid necrosis. Avoid cutting directly through visible superficial veins.
- Identify the dorsal cutaneous nerves (medial, intermediate and lateral branches of the superficial peroneal nerve) in the subcutaneous fat — they cross the field only a few millimetres deep and are purely sensory.
- Mobilise each nerve gently with a vessel loop or Penrose drain and retract it to the side. Use bipolar haemostasis away from the nerve, and never apply self-retaining retractors to the nerve.
- Incise the fascia overlying the extensor tendons longitudinally.
- Identify the extensor digitorum longus tendon over the metatarsal, pass a loop around it and retract it medially or laterally; identify and retract the extensor digitorum brevis insertion where it crosses the field. The tendons are never divided — division causes extensor lag and claw toe. Preserve the juncturae tendinum where possible to maintain coordinated toe extension.
- Incise the periosteum longitudinally along the dorsal surface of the metatarsal shaft and elevate subperiosteally with a periosteal elevator, staying in contact with bone at all times.
- Staying on bone protects the dorsalis pedis artery (which continues as the deep plantar artery in the first intermetatarsal space) and the dorsal metatarsal arteries, which run deep to the extensor tendons in the intermetatarsal spaces. Ligate only small branches as needed.
- Carry the elevation distally to the metatarsal neck and head as the procedure demands. The neck is the site of the Weil osteotomy and a common site for stress fractures; the head has a tenuous retrograde blood supply from the shaft and capsule.
- Limit circumferential periosteal stripping to what the procedure requires to preserve head vascularity — this is critical in Freiberg disease, where the head is already compromised.
- For a Weil osteotomy expose the neck dorsally and apply the osteotomy guide; for a fracture clear the fracture site and reduce under direct vision; for head resection partially release the collateral ligaments and deliver the head.
- Confirm reduction, rotation, fixation and the metatarsal parabola with intra-operative fluoroscopy in AP, oblique and lateral views.
- Restoring the metatarsal cascade is essential: shortening one ray by greater than 2 to 3 mm relative to its neighbours risks transfer metatarsalgia. Check that screw fixation does not penetrate the plantar cortex or enter the joint.
The dorsal cutaneous nerves are purely sensory but cross the operative field only a few millimetres deep, and injury causes numbness or a painful neuroma on the dorsum of the foot — a recognised and debilitating complication. Identify every branch early in the subcutaneous plane, mobilise and loop it gently, avoid diathermy near the nerve, never clamp self-retaining retractors onto it, and release retraction regularly.
The dorsal approach relies on intermuscular and subperiosteal dissection rather than a true internervous plane. The dorsal cutaneous nerves are sensory branches of the superficial peroneal nerve and are protected, not used as a landmark; the extensor tendons are retracted rather than divided. The safety principle is identification and protection of the sensory nerves in the subcutaneous layer, followed by strict subperiosteal dissection on bone — this avoids the deep peroneal nerve (which lies more laterally and supplies EDB) and protects the tenuous retrograde blood supply to the metatarsal head.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Dorsal cutaneous nerves (medial, intermediate, lateral; superficial peroneal)
- Protection
- Identify early, mobilise with a vessel loop, avoid cautery and self-retaining retractors
- Structure at risk
- Extensor digitorum longus and brevis tendons
- Protection
- Identify, loop and retract medially or laterally; never divide
- Structure at risk
- Dorsalis pedis and dorsal metatarsal arteries (intermetatarsal spaces)
- Protection
- Stay strictly subperiosteal on bone; ligate only small branches
- Structure at risk
- Metatarsal head blood supply (retrograde from shaft and capsule)
- Protection
- Limit circumferential elevation; preserve capsular attachments, especially in Freiberg disease
- Structure at risk
- MTP joint capsule and collateral ligaments
- Protection
- Incise only as needed; over-release risks instability and head avascular necrosis
Extensile options. Extend proximally to the tarsometatarsal joint to access the metatarsal base or the Lisfranc joint complex — useful for proximal shaft fractures, Lisfranc injuries involving the central rays, or a proximal osteotomy. Distal extension is limited by the toe: for head access the incision stops at the metatarsophalangeal joint crease, and further distal exposure needs a separate toe incision or a plantar approach. The interosseous muscles are not violated unless a ray amputation is planned. Closure. Close in layers: reapproximate the periosteum over the osteotomy or hardware where possible, close the fascia loosely to avoid compartment syndrome, allow the extensor tendons to fall back into position, close the subcutaneous layer carefully to avoid catching the dorsal cutaneous nerves, and close the skin with interrupted nylon or absorbable suture. Apply a sterile compressive dressing. Weight-bearing status depends on the procedure — non-weight-bearing for 4 to 6 weeks after a Weil osteotomy or fracture fixation, protected weight-bearing earlier after head resection — with early toe range of motion once wounds are stable, and serial radiographs to monitor healing and length maintenance.
Procedures Through This Approach
- Weil osteotomy — distal oblique metatarsal osteotomy for lesser metatarsalgia and length correction.
- ORIF of central-ray metatarsal fractures — neck, shaft or head fixation with mini-fragment plates or K-wires.
- Surgical management of Freiberg disease — metatarsal head resection or osteochondral grafting with minimal periosteal stripping.
- Partial or total ray amputation for infection, tumour or severe deformity.
- Excision of intractable plantar keratosis, elevation and grafting of depressed articular fragments, and debridement of osteomyelitis or non-union.
Viva & Exam Focus
DORSALDORSAL — the lesser-metatarsal exposure
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old woman with central metatarsalgia has failed conservative treatment and imaging shows a long second metatarsal. Describe how you would perform the dorsal approach and a Weil osteotomy.”
“A 28-year-old footballer sustains a displaced fracture of the third metatarsal neck after a tackle. Describe your surgical approach and fixation strategy.”
“A 16-year-old gymnast presents with Freiberg disease of the second metatarsal head with collapse and a loose body. How would you approach the surgical management?”
Patient position
- Supine on a radiolucent table with the foot at the end
- Thigh or calf tourniquet inflated to 250-300 mmHg
- Slight ankle plantarflexion to relax the extensor tendons
- C-arm from the opposite side for AP, oblique and lateral views
- Keep tourniquet time less than 90 minutes
Incision planning
- Longitudinal dorsal incision over the target metatarsal or in the intermetatarsal space
- One intermetatarsal incision accesses two adjacent rays
- Maintain a skin bridge of at least 5 mm between parallel incisions
- Length 4 to 6 cm centred over the surgical target (neck or shaft)
- Extend proximally to the tarsometatarsal joint if base access is required
Danger structures
- Dorsal cutaneous nerves (medial, intermediate, lateral) — identify early and protect with vessel loops
- Extensor digitorum longus and brevis tendons — retract, never divide
- Dorsalis pedis and dorsal metatarsal arteries — protected by the subperiosteal plane
- Metatarsal head blood supply — limit circumferential periosteal elevation
- MTP joint capsule and collateral ligaments — preserve for stability and vascularity
Internervous plane
- No true classical internervous plane
- The approach is extra-compartmental and subperiosteal
- Dorsal cutaneous nerves are sensory only — mobilise and protect
- Extensor tendons are retracted rather than divided
- Stay on bone to protect the deep neurovascular structures
Key procedures
- Weil osteotomy — 30-degree oblique, 2 to 3 mm shortening, single screw fixation
- Metatarsal fracture ORIF — dorsal mini-fragment plate or crossed screws
- Freiberg surgery — head resection or grafting with minimal periosteal stripping
- Ray amputation — extend the incision and divide the interossei and plantar structures
- Always confirm the metatarsal parabola and length with fluoroscopy
Closure and complications
- Layered closure protecting the dorsal cutaneous nerves
- Loose fascial closure to avoid compartment syndrome
- Nerve injury — numbness or painful neuroma (less than 5 percent with careful technique)
- Transfer metatarsalgia — avoid with precise length restoration
- Extensor lag or claw toe — prevented by tendon retraction, not division
References
Weil's osteotomy versus distal metatarsal metaphyseal osteotomy for the treatment of metatarsalgia. A metaanalysis of outcome and complications.
- Meta-analysis showed Weil osteotomy achieves good pain relief for metatarsalgia with low transfer metatarsalgia rates when shortening is limited to 2-3 mm and the metatarsal parabola is restored
Results of two different surgical techniques in the treatment of advanced-stage Freiberg's disease.
- Dorsal approach head resection for advanced Freiberg disease provided reliable pain relief with preservation of capsular attachments to maintain vascularity of the remaining metatarsal
[Weil's metatarsal osteotomy in the treatment of metatarsalgia].
- Original description of the Weil metatarsal osteotomy performed through the dorsal approach for metatarsalgia with emphasis on precise shortening to restore the metatarsal parabola
[Fixation of displaced fifth metatarsal shaft and neck fractures].
- Dorsal plating via the dorsal approach achieved stable fixation and good functional outcomes in displaced metatarsal shaft and neck fractures with anatomic reduction