Anterior calcaneal osteotomy with structural graft for forefoot abduction and talonavicular uncoverage in flexible flatfoot · advanced
- The Evans osteotomy is made approximately 1.5 cm (12 to 15 mm) proximal to the calcaneocuboid (CC) joint — too proximal violates the subtalar joint; too distal risks CC joint subluxation and graft instability.
- Lateral column lengthening is indicated when forefoot abduction exceeds 40 percent talonavicular uncoverage on a weight-bearing AP radiograph that will not be corrected by medial displacement calcaneal osteotomy (MDCO) alone.
- In adults it is almost never performed in isolation — combine it with an MDCO for hindfoot valgus and an FDL transfer to the navicular for the posterior tibial tendon in stage II disease.
- Over-lengthening (a graft greater than 8 to 10 mm) produces lateral column overload, calcaneocuboid arthritis and stiffness; the typical adult graft is 6 to 8 mm, sized intra-operatively to bring uncoverage below 20 percent.
- The sural nerve (crossing the lateral calcaneus 2 to 3 cm proximal to the CC joint) and the peroneal tendons must be identified and protected throughout.
- Tricortical iliac crest autograft has the highest union rate (greater than 95 percent) but donor morbidity in 15 to 20 percent of patients; structural allograft is acceptable in lower-demand patients.
When & Why
Indication. Symptomatic flexible flatfoot (stage II posterior tibial tendon dysfunction, PTTD) with forefoot abduction and talonavicular uncoverage greater than 40 percent on a weight-bearing AP radiograph, persistent medial arch collapse and activity-limiting pain that has failed a fair trial of orthotics and physical therapy — usually as part of a comprehensive reconstruction with MDCO and an FDL transfer. Relative indications include an adolescent or young adult with progressive symptomatic flexible flatfoot, and isolated residual forefoot abduction producing symptoms after a previous hindfoot correction. Assess the whole deformity before committing. Lateral column lengthening corrects forefoot abduction and talar head coverage — it does not correct hindfoot valgus or restore the posterior tibial tendon. Decide whether the foot is genuinely flexible and whether the hindfoot, the spring ligament and any equinus contracture also need addressing at the same sitting.
Symptomatic flexible flatfoot with forefoot abduction and talonavicular uncoverage greater than 40 percent that has failed orthotics and therapy. Joint-preserving reconstruction (MDCO plus lateral column lengthening plus FDL transfer) is the right operation.
Progressive symptomatic deformity before skeletal maturity. Mosca's long-term data show durable correction; smaller grafts (5 to 7 mm) usually suffice because of ligamentous laxity.
A rigid flatfoot with subtalar or midtarsal arthritis requires arthrodesis, not lengthening. Lengthening a stiff foot only adds stiffness without correcting the deformity, and active infection or severe vascular insufficiency also preclude it.
Relative contraindications to weigh carefully are smoking or poorly controlled diabetes (optimise first, or consider allograft with supplemental fixation), previous subtalar or calcaneal surgery that distorts the landmarks, and any patient unable to comply with a 6 to 8 week non-weight-bearing protocol. Consent specifically for sural nerve injury (3 to 7 percent), peroneal tendon irritation, calcaneocuboid arthritis (3 to 5 percent), graft nonunion (5 to 10 percent), overcorrection with lateral column pain, and the need for non-weight-bearing for 6 to 8 weeks. Setup. Supine with a bump under the ipsilateral hip to internally rotate the leg, or lateral decubitus if combined with medial procedures. Apply a thigh tourniquet, and prep and drape the foot free. General or spinal anaesthesia with popliteal and saphenous blocks gives good post-operative analgesia. Position the C-arm for AP, lateral and oblique views — and plan for a simulated weight-bearing AP view (plantar pressure on the forefoot), which is essential to judge talonavicular coverage intra-operatively.
The Operation
The goal is to lengthen the lateral column of the calcaneus through an anterior (Evans) osteotomy, distracting it with a structural trapezoidal graft until the navicular covers the talar head, while protecting the sural nerve and peroneal tendons and staying out of the calcaneocuboid and subtalar joints. The exposure is laid out in the steps below.
Operative sequence
- Supine with an ipsilateral hip bump (or lateral decubitus for combined medial work), thigh tourniquet, C-arm set up for AP, lateral and oblique views.
- Palpate the anterior calcaneal process and the calcaneocuboid (CC) joint; the osteotomy will lie 12 to 15 mm proximal to that joint.
- A simulated weight-bearing AP view (pushing up on the forefoot with the heel on the table) is the key intra-operative check of talar head coverage.
- A 6 to 8 cm longitudinal incision along the lateral calcaneal wall, centred over the planned osteotomy, beginning at the anterior process and extending proximally toward the peroneal tubercle.
- Place it about 1 cm distal to the point where the sural nerve crosses, to keep the nerve out of the line of the cut.
- Identify the sural nerve in the subcutaneous plane under loupe magnification and loop it with a vessel loop — it crosses the lateral calcaneus obliquely 2 to 3 cm proximal to the CC joint, with the lesser saphenous vein.
- Expose the peroneus brevis and longus tendons and elevate them subperiosteally as a single sleeve with the superior peroneal retinaculum.
- Place a Hohmann retractor on the anterior calcaneal process to hold the tendons anterior and protect them during distraction.
- Elevate the periosteum from the lateral calcaneal wall. Confirm the CC joint by palpation and fluoroscopy.
- Pass a K-wire 15 mm proximal to the joint, parallel to the articular surface, under fluoroscopic control — this wire is the osteotomy guide and confirms both the level and the trajectory before any bone is cut.
- Using a thin oscillating saw, cut from lateral to medial parallel to the K-wire, aiming slightly distal and lateral toward the sinus tarsi floor.
- Leave the medial cortex intact and complete it with an osteotome to avoid over-penetrating into the medial soft tissues and the subtalar joint.
- Insert a laminar spreader and gently open the osteotomy, mobilising the anterior process while protecting the peroneal tendons and sural nerve and preserving the long plantar ligament and plantar fascia.
- Open until the talar head is adequately covered on the simulated weight-bearing AP fluoroscopic view, then measure the gap — in most adults 6 to 8 mm is sufficient; greater than 10 mm is rarely needed and risks CC subluxation and lateral overload.
- Harvest a tricortical iliac crest autograft (or prepare structural allograft) shaped as a trapezoid with the wider base oriented laterally.
- Impact it into the osteotomy with the cortical surface facing laterally, and reduce the anterior fragment over the graft so it is held firmly in the void.
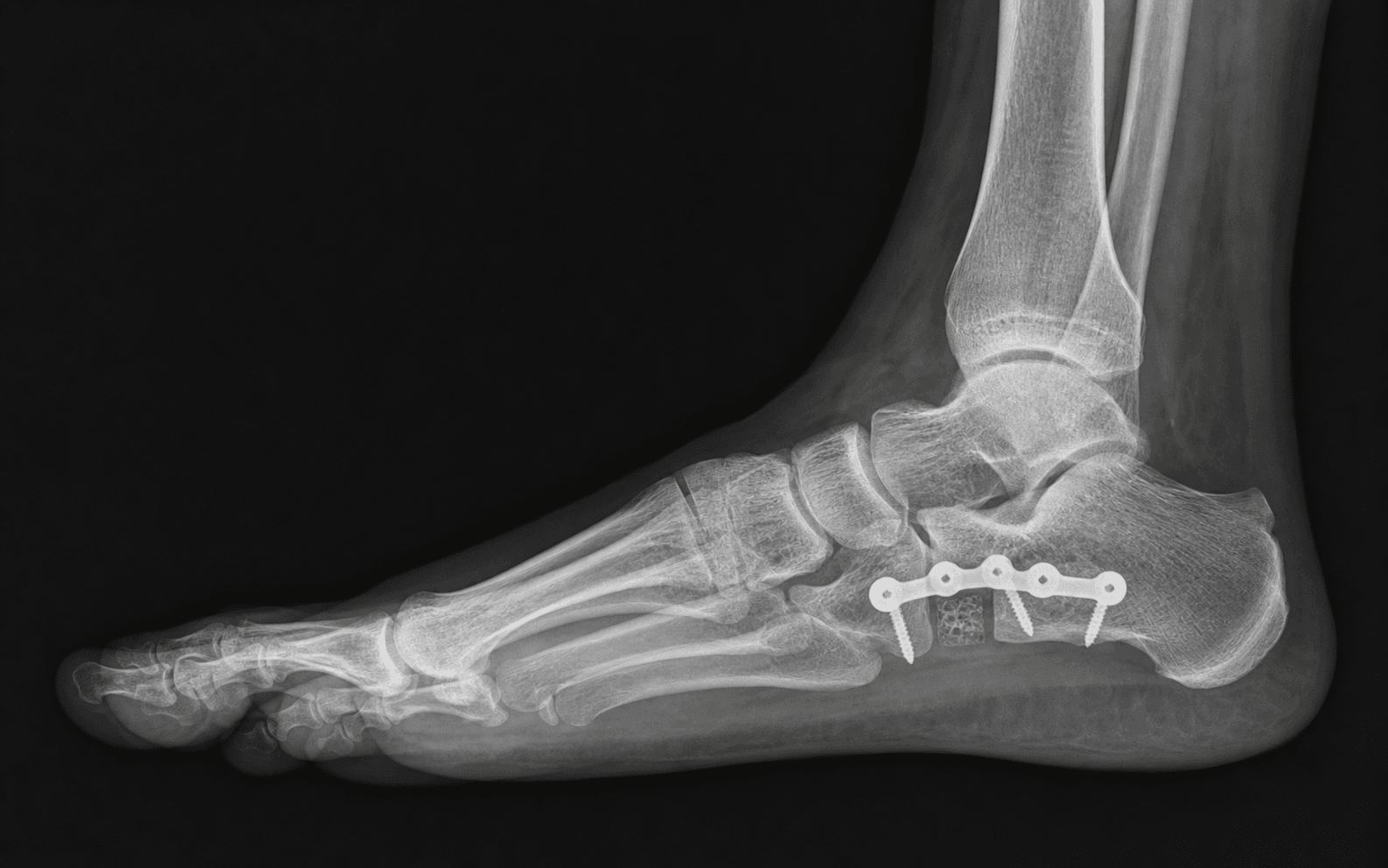
- Place a 3.5 mm cortical screw from the anterior calcaneal process into the posterior calcaneal body, compressing the graft; a low-profile plate is an alternative when more stability is needed.
- The screw must not violate the subtalar joint — confirm the trajectory fluoroscopically.
- Final AP, lateral and oblique fluoroscopy confirms graft position, screw placement, talonavicular coverage and no CC joint subluxation.
- Close in layers over a drain if needed, and apply a bulky compressive dressing with a posterior splint.
- In stage II PTTD the typical sequence is MDCO first, then lateral column lengthening, then an FDL transfer to the navicular, then spring ligament repair or augmentation if attenuated, and a gastrocnemius recession if a Silfverskiold test is positive.
- Re-take the simulated weight-bearing views after the hindfoot is corrected, since graft sizing depends on the corrected alignment.
- Sural nerve — transection or stretch neuritis: identify it under loupe magnification and protect it with a vessel loop before any retraction.
- Peroneal tendons — injury or subluxation from aggressive retraction: keep them elevated as a subperiosteal sleeve with the retinaculum and held anterior with a Hohmann retractor.
- Calcaneocuboid joint — an osteotomy less than 10 mm from the joint risks capsular disruption, subluxation and graft instability; the capsule is the only restraint once the cut is opened.
- Over-distraction — a graft greater than 10 mm produces CC strain, lateral column overload and eventual arthritis; if the CC joint opens on the oblique view, downsize the graft.
- Subtalar joint — a proximal or medially directed cut enters the posterior facet; aim the osteotomy slightly distal and lateral toward the sinus tarsi floor and confirm the trajectory fluoroscopically before completing the cut.
Confirm the osteotomy level with a K-wire under fluoroscopy before cutting. After distraction, obtain a simulated weight-bearing AP view by pushing up on the forefoot with the heel on the table, measure the gap, and select a graft that reduces talonavicular uncoverage to less than 20 percent. If the gap feels excessive or the CC joint opens on the oblique view, downsize the graft by 1 to 2 mm — over-lengthening is the most common cause of late lateral column pain.
The osteotomy must remain parallel to the calcaneocuboid joint surface. An oblique cut that converges plantarly creates a plantarflexion moment on the anterior fragment that exacerbates the flatfoot deformity rather than correcting it. Confirm the plane with the K-wire guide before you commit to the saw.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation & weight-bearing | Therapy | |-------|--------|--------------------------------|---------| | 1 | 0 to 6 weeks | Non-weight-bearing in a below-knee cast or removable boot | Elevation and ice for swelling; sutures out at 2 weeks; gentle ankle and subtalar range of motion out of the cast at 4 weeks if the graft is stable | | 2 | 6 to 12 weeks | Transition to partial then full weight-bearing in a boot by 10 to 12 weeks, with radiographic confirmation of graft position | Custom orthotic with medial arch support and lateral forefoot posting; begin strengthening and proprioception | | 3 | 3 to 6 months | Return to normal footwear with an orthotic | Full activities by 4 to 6 months; monitor for lateral column pain or CC joint symptoms at each visit | Return to function. Sedentary work at 8 to 10 weeks, manual labour at 4 to 6 months, and sport at 6 to 9 months with orthotic support. Adolescents often return to sport faster (4 to 6 months). Complications
- Incidence
- 3 to 7 percent
- Recognition
- Numbness or painful dysaesthesia along the lateral foot and heel; a positive Tinel sign at the incision
- Prevention and management
- Prevention: identify the nerve under loupe magnification and protect it with a vessel loop throughout. Management: if transected, primary repair or bury the proximal end in muscle; a painful neuroma may need excision and burial after 3 months
- Incidence
- 3 to 8 percent
- Recognition
- Lateral foot pain and stiffness with reduced subtalar motion; CC joint narrowing or subluxation on the oblique view
- Prevention and management
- Prevention: limit the graft to 6 to 8 mm, confirm intra-operative coverage, and keep the osteotomy at least 10 mm from the joint. Management: activity modification, orthotics, CC joint injection; arthrodesis for refractory arthritis
- Incidence
- 5 to 10 percent (higher with allograft)
- Recognition
- Loss of correction with recurrent forefoot abduction and pain at the osteotomy site; radiographic lucency or collapse at 3 months
- Prevention and management
- Prevention: tricortical autograft with good endosteal contact, stable screw fixation, and biologics in smokers. Management: revision with autograft and plate fixation; consider a bone stimulator
- Incidence
- 4 to 6 percent
- Recognition
- Pain under the fifth metatarsal base, callosity, reduced push-off
- Prevention and management
- Prevention: avoid grafts greater than 10 mm; confirm coverage fluoroscopically and downsize if the lateral column feels too long. Management: orthotics with lateral forefoot posting; rarely a revision shortening osteotomy
- Incidence
- 2 to 5 percent
- Recognition
- Lateral ankle pain, snapping and swelling along the peroneal tendons; a positive resisted eversion test
- Prevention and management
- Prevention: subperiosteal elevation of the tendons with the retinaculum and protection with a Hohmann retractor. Management: rest, NSAIDs, therapy; refractory cases need tenolysis or retinacular repair
- Incidence
- 3 to 5 percent
- Recognition
- Loss of subtalar and midfoot motion, lateral foot pain, difficulty on uneven ground
- Prevention and management
- Prevention: limit lengthening to the measured requirement and preserve the plantar ligaments. Management: aggressive physiotherapy and night splinting; rarely arthrolysis
Viva & Exam Focus
EVANSEVANS — osteotomy landmarks and execution
LENGTHENLENGTHEN — decision making and pitfalls
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old woman with stage II posterior tibial tendon dysfunction has progressive medial arch collapse and forefoot abduction. The standing AP radiograph shows 55 percent talonavicular uncoverage. She has failed 6 months of orthotics and therapy. What is your surgical plan, and how do you determine the size of the lateral column lengthening graft?”
“During an Evans osteotomy you have distracted 9 mm and the simulated weight-bearing AP view shows good talonavicular coverage, but the calcaneocuboid joint appears to open slightly on the oblique view. What do you do?”
“A 35-year-old man has an Evans osteotomy with a tricortical autograft for flexible flatfoot. At 4 months he has persistent pain at the osteotomy site and radiographs show a persistent lucent line through the graft-host interface. What is your diagnosis and management?”
Indications
- Stage II PTTD with greater than 40 percent talonavicular uncoverage on the standing AP, failed conservative care
- Forefoot abduction and arch collapse refractory to orthotics and therapy
- Flexible deformity suitable for joint-preserving reconstruction
- Usually combined with MDCO and an FDL transfer — isolated lengthening is rarely indicated in adults
Critical anatomy
- Osteotomy 12 to 15 mm proximal to the CC joint, parallel to the joint line
- Sural nerve crosses the lateral calcaneus 2 to 3 cm proximal to the CC joint — identify and protect
- Peroneal tendons lie anterior and superior — elevate subperiosteally with the retinaculum
- The CC joint capsule is the sole stability once the osteotomy is distracted — too distal a cut risks subluxation
- The subtalar joint lies proximal and medial — aim the cut slightly distal and lateral
Graft selection & sizing
- Typical adult graft height 6 to 8 mm; greater than 10 mm risks CC arthritis and lateral overload
- Tricortical iliac crest autograft: greater than 95 percent union, donor morbidity 15 to 20 percent
- Structural allograft: 85 to 92 percent union, no donor morbidity — add biologics in higher-risk patients
- The intra-operative simulated weight-bearing AP view determines the exact size needed
- Trapezoidal graft with the wider base lateral restores arch and talar head coverage
Danger zones
- Sural nerve — transection or neuroma in 3 to 7 percent; identify under loupe and protect
- CC joint — subluxation or arthritis from an osteotomy less than 10 mm from the joint or a graft greater than 10 mm
- Peroneal tendons — injury or subluxation from aggressive retraction; protect with a retinacular sleeve
- Subtalar joint — penetration from a proximal or medially directed cut; confirm trajectory fluoroscopically
- Over-lengthening — lateral overload and fifth metatarsal pain; downsize if the CC joint opens
Complications
- Sural neuritis or neuroma: 3 to 7 percent — prevent by deliberate identification and protection
- CC joint arthritis: 3 to 8 percent — limit the graft to 6 to 8 mm and confirm coverage intra-operatively
- Graft nonunion or collapse: 5 to 10 percent — prefer autograft, stable fixation, optimise biology
- Lateral column overload: 4 to 6 percent — avoid grafts greater than 10 mm; use lateral forefoot posting orthotics
- Peroneal tendonitis: 2 to 5 percent — subperiosteal elevation and protection during distraction
Post-operative milestones
- Week 0 to 6: non-weight-bearing in cast or boot; sutures out at 2 weeks; gentle ROM at 4 weeks
- Week 6 to 12: progressive weight-bearing to full; custom orthotic with medial arch and lateral posting
- Month 3 to 6: normal footwear; full activities by 4 to 6 months; sport at 6 to 9 months
- Adolescents: smaller grafts (5 to 7 mm) often suffice; faster healing and return to sport
Background & Evidence
Pathoanatomy. Posterior tibial tendon dysfunction is the most common cause of adult acquired flatfoot deformity, typically presenting in women over 40. The posterior tibial tendon fails first, the spring ligament and deltoid attenuate, and unopposed peroneal brevis pulls the forefoot into abduction, uncovering the talar head and collapsing the medial arch. Stage II disease — a flexible hindfoot with valgus, forefoot abduction and the too-many-toes sign — is the setting in which lateral column lengthening is used; the rigid stages need arthrodesis instead.
- Alignment
- Painful tenosynovitis; normal alignment; mild medial swelling
- Typical management
- Rest, orthotic, NSAIDs; tenosynovectomy if refractory
- Alignment
- Flexible flatfoot — hindfoot valgus, forefoot abduction, too-many-toes sign
- Typical management
- MDCO plus lateral column lengthening plus FDL transfer (and spring ligament or gastrocnemius work as needed)
- Alignment
- Fixed (rigid) flatfoot deformity
- Typical management
- Subtalar or triple arthrodesis
- Alignment
- Ankle involvement — deltoid insufficiency with valgus tilt of the talus
- Typical management
- Extended arthrodesis including the ankle
Biomechanical rationale. Lengthening the lateral column restores the medial longitudinal arch by increasing the distance between the calcaneus and the forefoot, reducing forefoot abduction and improving navicular coverage of the talar head. Cadaveric studies show that a 6 to 8 mm lengthening reduces talonavicular uncoverage from about 50 percent to less than 20 percent and raises the medial cuneiform height by 4 to 6 mm. Clinical outcomes. Performed as part of a comprehensive reconstruction (MDCO plus lateral column lengthening plus FDL transfer), AOFAS scores rise from the low 40s pre-operatively to the mid-80s at two years, with union rates exceeding 90 percent for tricortical autograft. Isolated lateral column lengthening without correcting hindfoot valgus gives inferior results and higher revision rates.
- Union rate
- Greater than 95 percent
- Donor morbidity
- 15 to 20 percent (pain, haematoma, lateral femoral cutaneous nerve injury)
- Best for
- Young, active, high-demand reconstruction
- Union rate
- 85 to 92 percent
- Donor morbidity
- None
- Best for
- Older patients, smokers, or when autograft is contraindicated
- Union rate
- Greater than 90 percent
- Donor morbidity
- Same donor site as the standard Evans
- Best for
- When trapezoidal fit is poor or extra stability is required
- Union rate
- Greater than 90 percent (short-term data)
- Donor morbidity
- None
- Best for
- Emerging option in select centres; limited long-term data
Adolescent flexible flatfoot. Lateral column lengthening is particularly effective in adolescents with progressive symptomatic flexible flatfoot; Mosca's long-term data support excellent durability when it is performed before skeletal maturity. Smaller grafts (5 to 7 mm) often suffice because of ligamentous laxity, autograft is preferred and well tolerated, and it may be combined with a medial reefing or Kidner procedure when the navicular is prominent. Good to excellent results exceed 90 percent at 10 to 15 years when graft size is controlled and the soft tissues balanced. Key evidence. Mosca (2010) reported greater than 90 percent good-to-excellent results at up to 15 years in adolescents with controlled graft size. Dolan (2007) showed AOFAS improvement from 42 to 84 when lateral column lengthening was combined with MDCO and FDL transfer. Thomas (2001) demonstrated that grafts greater than 10 mm produce calcaneocuboid subluxation and increased joint pressure. Vora (2006) found autograft union of 97 percent versus allograft 87 percent with equivalent clinical scores at two years, and Haas (1998) showed that deliberate sural nerve identification reduces neuritis from 15 percent to 3 percent.
References
Graft Position and Short-term Radiographic Outcomes After Pediatric Calcaneal Lengthening for Symptomatic Flexible Flatfoot: A Retrospective Comparative Study
- Graft position significantly affects short-term radiographic correction in pediatric calcaneal lengthening for flexible flatfoot
- Retrospective comparative study demonstrates importance of precise graft placement
Risk Factors for Failure of Calcaneal Lengthening Osteotomy in Children and Adolescents With Planovalgus Foot Deformity: A Retrospective Study
- Identified risk factors for failure of calcaneal lengthening osteotomy in planovalgus deformity
- Retrospective analysis highlights patient selection criteria for successful outcomes
Treatment of Symptomatic Flexible Flat Foot in Pediatrics with A Modified Mosca's Lateral Column Lengthening
- Modified Mosca lateral column lengthening effective for symptomatic flexible flatfoot in pediatrics
- Technique modifications lead to improved clinical and radiographic outcomes
Quality of Life after Flatfoot Surgery in the Pediatric Population
- Flatfoot surgery including calcaneal lengthening improves quality of life in pediatric patients
- Demonstrates long-term functional benefits of joint-preserving reconstruction