Terminal extensor tendon disruption at the DIP joint — splinting first, fixation only when the joint has subluxated | intermediate
- The mainstay of treatment for BOTH soft-tissue (tendinous) and most bony mallet injuries is CONTINUOUS DIP extension splinting for 6 to 8 weeks, followed by 2 to 6 weeks of night and activity splinting. The DIP is held in slight hyperextension while the PIP is left completely free.
- Any interruption of full DIP extension RESTARTS THE CLOCK. If the finger flexes even momentarily while the splint is off, the full 6 to 8 week period begins again — skin care must be done with the DIP supported flat on a table, never hanging free.
- Operative treatment is reserved for a bony fragment involving more than approximately one third of the articular surface WITH volar (palmar) subluxation of the distal phalanx, or for an OPEN injury. Fragment size alone, without subluxation, is increasingly managed non-operatively.
- The classic late deformity is a SWAN-NECK: a persistent DIP extension lag combined with PIP hyperextension, produced when an attenuated terminal tendon transfers extensor force proximally to the central slip through the lateral bands.
- “Mechanism is forced flexion of an actively extended DIP ('baseball finger'), avulsing the terminal extensor tendon from the dorsal base of the distal phalanx. Active DIP extension is lost, but passive extension is full and painless.
- “Do NOT default to surgery for a bony mallet. The operative trigger is volar subluxation of the distal phalanx on a true lateral radiograph, not fragment size alone — splint even large fragments if the joint is congruent.
- “Splint in SLIGHT hyperextension only. Excessive extension devascularises the thin dorsal skin over the DIP, causing blistering and pressure necrosis. Inspect the skin at every review.
- “Even chronic or neglected mallet fingers (present for weeks to months) deserve a trial of continuous splinting — many still heal. Do not assume it is too late.
When & Why
Definition and mechanism. A mallet finger is a disruption of the terminal extensor tendon at its insertion on the dorsal base of the distal phalanx, at the DIP joint. The hallmark is loss of active DIP extension with preserved passive extension. The classic mechanism is a sudden forced flexion force applied to an actively extended fingertip — the ball-strike injury that gives it the nickname baseball finger. A direct blow to the dorsum of the DIP or a laceration can also produce it. The lesion is either tendinous (soft-tissue) — rupture of the terminal tendon itself — or bony — avulsion of a fragment of the dorsal base of the distal phalanx with the tendon still attached to it. The mainstay is non-operative. All closed soft-tissue (tendinous) mallets (Doyle Type I), most bony mallets provided the joint is congruent (no volar subluxation), and delayed presentations (even weeks to months old) are treated with continuous DIP extension splinting. Operative treatment is selective. Reserve fixation for: - A large bony fragment involving more than approximately one third of the articular surface WITH volar (palmar) subluxation of the distal phalanx — the subluxated, unstable joint is the real indication
- Open injuries — Doyle Types II and III (laceration or tissue loss)
- A subset of failures of a genuine, concordant trial of splinting
- Selected paediatric transepiphyseal fractures that are significantly displaced The one principle that drives every decision. Volar subluxation of the distal phalanx on a true lateral radiograph — not fragment size alone — is the operative trigger. A fragment involving approximately one third or more of the surface WITHOUT subluxation is increasingly managed non-operatively, because the evidence shows fragment size alone does not dictate outcome. Do not operate simply for cosmesis of a dorsally prominent fragment.
- Continuous DIP extension splinting
- Soft-tissue mallet (Doyle I); most bony mallets without subluxation; many chronic mallets
- Operative fixation
- Large bony fragment with volar subluxation (Doyle IVc); open injuries (II, III); selected failures
- Continuous DIP extension splinting
- DIP held in slight hyperextension, PIP free, continuous for six to eight weeks then wean
- Operative fixation
- Extension-block (Ishiguro) percutaneous pinning; ORIF with screw or pull-out suture; direct repair for open injuries
- Continuous DIP extension splinting
- Community, hand therapy or clinic
- Operative fixation
- Operating theatre or procedure room with imaging
- Continuous DIP extension splinting
- Good or excellent result in the large majority; a small residual extension lag is acceptable
- Operative fixation
- Restores joint congruity; fixation in a small distal phalanx is technically demanding
- Continuous DIP extension splinting
- Skin maceration or necrosis; residual lag; swan-neck; non-concordance restarts the clock
- Operative fixation
- Pin-tract infection, wire migration or breakage, nail-matrix injury, stiffness, DIP arthritis
- Continuous DIP extension splinting
- Sport with the splint in situ once comfortable
- Operative fixation
- Protected until wires are removed (about six weeks) and the fragment is stable
Consent. Specifically counsel on residual extension lag, swan-neck deformity, the risk of pin-tract infection and wire migration or breakage, nail deformity from nail-matrix injury, DIP stiffness and arthritis, and the prolonged splintage period. Setup. Supine with the hand on a radiolucent hand table, forearm pronated for a dorsal or midaxial approach to the DIP. A digital block or local infiltration (with or without epinephrine) is usually sufficient for percutaneous pinning and WALANT is well suited; open fixation and open mallet repair may use a digital block or regional/general anaesthesia. An image intensifier is essential for any bony mallet fixation to confirm fragment reduction and joint congruity throughout.
The Operation
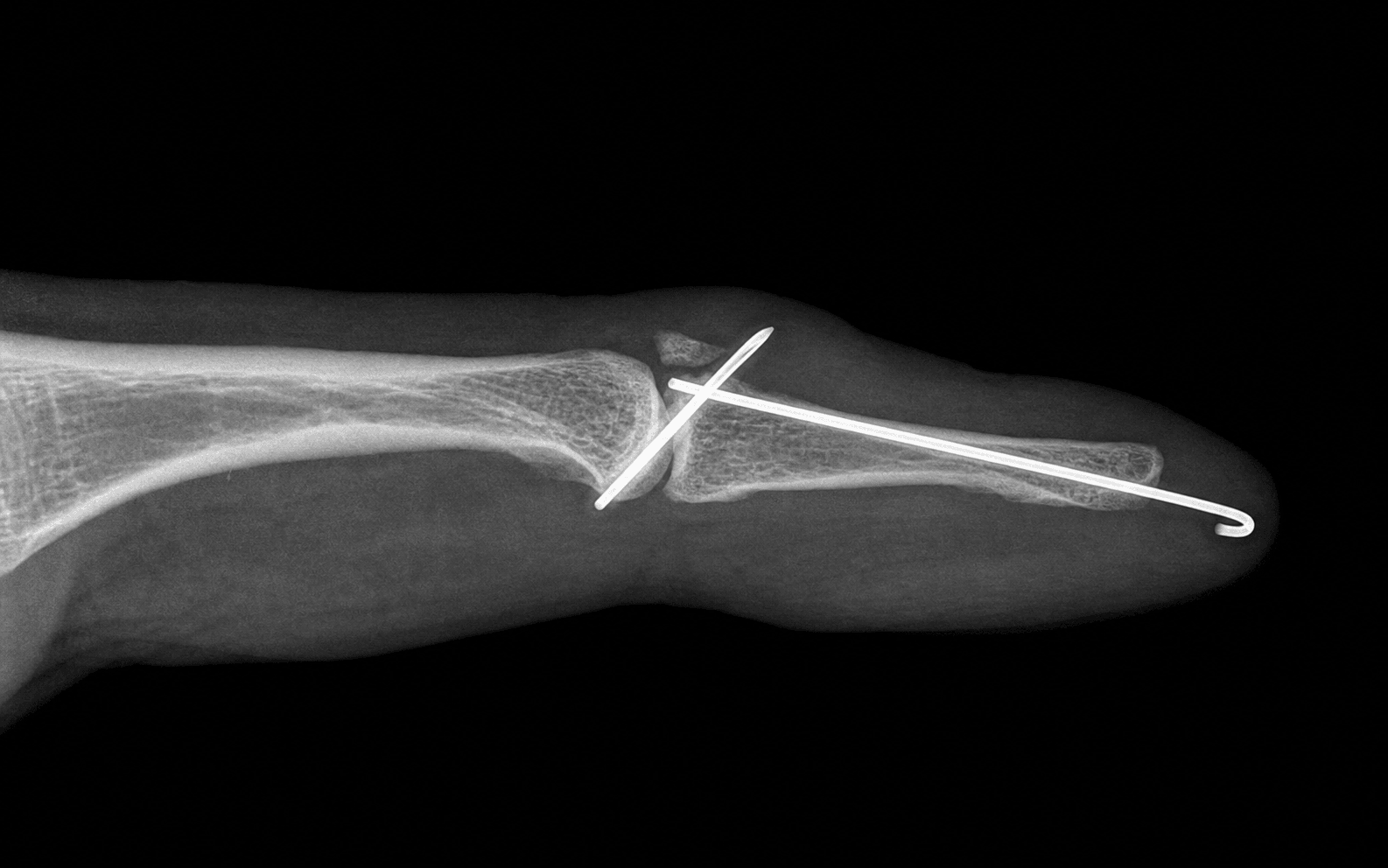
The goal is to restore a congruent DIP joint and hold the terminal tendon under tension while it heals — for most operative cases that means reducing a subluxated bony fragment with extension-block (Ishiguro) percutaneous pinning, with open ORIF or direct tendon repair reserved for the large single fragment and the open injury. The terminal tendon is the confluence of the two lateral bands, inserting on the dorsal base of the distal phalanx — it is this insertion that fails in a mallet. The distal phalanx is small, with a thin dorsal cortex and the nail matrix draped over its volar surface, which is why fixation here is unforgiving and percutaneous pinning is usually preferred over screws. The full anatomy and the mechanism of the secondary swan-neck are covered in Background & Evidence.
A. Extension-block (Ishiguro) percutaneous pinning — the default operation
- Supine, hand on a radiolucent hand table, forearm pronated.
- Digital block or local infiltration (WALANT is well suited); image intensifier available throughout.
- Indication confirmed: a closed bony mallet with volar subluxation (Doyle Type IVc) where the dorsal fragment is large enough to capture but the joint needs reduction.
- Flex and extend the DIP under image; confirm the dorsal fragment and the volar subluxation of the distal phalanx on a true lateral view.
- Volar subluxation is easy to miss on an oblique view — obtain a true lateral before any wire is placed.
- Flexing the PIP positions the terminal tendon and the dorsal fragment so that a block wire can control them.
- Pass a fine K-wire (typically 0.045 inch or 1.0 mm) percutaneously into the dorsal distal aspect of the head of the middle phalanx, angled distally at roughly 40 to 45 degrees.
- This wire acts as an extension block — it stops the dorsal fragment being driven dorsally and proximally when the DIP is extended. Keep it dorsal in the distal middle phalanx; do not drive it volarly or into the PIP joint.
- As the distal phalanx is brought up into extension, the fragment is levered down against the block wire and the joint is reduced.
- Check the articular surface and the restoration of joint congruity on a true lateral fluoroscopic image.
- Drive a second longitudinal K-wire from the tip of the distal phalanx across the DIP joint to hold full extension and maintain the reduction.
- Take care to avoid the nail matrix — pass the wire along the axis that avoids the germinal matrix.
- Bend and cut the wires outside the skin, cap them, and protect the finger in a splint.
By inserting the block wire into the dorsal middle phalanx angled distally while the PIP is flexed, I create a shelf that the displaced dorsal fragment is pushed against as I extend the DIP — the fragment reduces itself. I then lock the reduction with a longitudinal DIP wire, and I always confirm congruity on a true lateral fluoro image before I leave the table.
- Driving the block wire too far volarly or into the PIP joint — keep it dorsal in the distal middle phalanx.
- Failing to achieve a true lateral image — volar subluxation is easy to miss on an oblique view.
- Injuring the nail matrix with the longitudinal DIP wire — pass it along the axis that avoids the germinal matrix.
- Losing reduction when the DIP wire is advanced — re-check after the wire is finally seated.
B. ORIF of a large single fragment — when percutaneous methods cannot secure the reduction
- Use a dorsal curvilinear (S-shaped) or lazy-S incision centred over the DIP, or a midaxial incision.
- Protect the nail matrix — if the incision extends proximal to the eponychial fold, elevate the germinal matrix carefully and avoid damaging it.
- Evacuate the haematoma and clear the fracture bed; identify the dorsal fragment still attached to the terminal tendon, and the dorsal base of the distal phalanx.
- Bring the DIP into extension and anatomically reduce the fragment against the dorsal base; hold it with a fine reduction clamp.
- One or two 1.0 to 1.2 mm K-wires for a small or comminuted fragment.
- A small headless or mini-fragment lag screw for a single large fragment.
- A pull-out suture or wire (Bunnell tie-over) grasping the terminal tendon and exiting through the pulp, tied over a padded button, for a fragment too small for hardware.
- Add a longitudinal DIP transfixion K-wire for about six weeks to unload the fixation while the tendon and bone heal.
- Close the skin; apply a protective splint with the DIP extended and the PIP free.
For a large single fragment I prefer a mini lag screw if the bone will hold it, because it gives compression and early stability. For a small, comminuted fragment I do not chase the bone — I use a pull-out suture through the tendon to re-create the terminal insertion, and I always protect the construct with a longitudinal DIP wire for six weeks. Whatever fixation I choose, I never compromise the nail matrix for exposure.
- Excessive proximal dissection injuring the germinal matrix — nail deformity.
- Overtightening a screw splitting a small fragment — the distal phalanx is unforgiving.
- Leaving the joint subluxated after fixation — re-confirm congruity on a true lateral image.
- Forgetting the protective longitudinal DIP wire — unprotected fixation will fail when the tendon is loaded.
C. Open (laceration) mallet repair — Doyle Types II and III
- Lavage and debride the wound; manage tetanus and antibiotic cover as for any open hand injury.
- The terminal tendon is often retracted only a few millimetres; the skin laceration usually lies at the same level.
- Appose the tendon ends with a 4-0 or 5-0 non-absorbable suture using a modified Kessler or figure-of-eight configuration, taking care to avoid bulk that would limit skin closure.
- Pass a longitudinal K-wire across the DIP in full extension to protect the repair for about six weeks.
- Close the skin and apply a splint; begin active PIP motion from day one to prevent stiffness.
After lavage I repair the tendon under direct vision and then protect it with a DIP wire for six weeks — the tendon-to-tendon or tendon-to-bone healing, not the wire, is what will eventually restore extension. I start PIP movement immediately so the finger does not stiffen proximally.
Aftercare & Complications
Splinting protocol (non-operative and post-operative) | Phase | Timing | Splint | Motion | |-------|--------|--------|--------| | Continuous | First 6–8 weeks | DIP in slight hyperextension, day and night (Stack, custom thermoplastic or aluminium-foam); PIP left free | Active PIP from day one; skin care with DIP supported flat on a table | | Weaning | Next 2–6 weeks | Night and activity splinting (sport, heavy use) | Graded wean — short periods out of the splint while monitored, increasing as active extension is maintained | | After K-wire fixation | — | Protective splint with DIP extended until wires out | DIP transfixion wire (and block wire, if used) removed at about 6 weeks under sterile technique, then active DIP flexion/extension; buddy-tape for protection during weaning | Return to function. Desk and light activity within days (splinted); driving once the patient has safe control of the splinted hand; manual work around six weeks once the joint is stable and any wires are out; contact sport only with a protective splint in situ, typically after about eight weeks or once the fragment is stable. Hand therapy indications. Residual extension lag at the end of continuous splinting (a further extension period); PIP stiffness or a developing swan-neck posture (figure-of-eight or PIP-extension-control splinting); pin-site issues or wire-related discomfort (early review and pin care); chronic or neglected mallet (prolonged supervised splinting programme). Special case — chronic and neglected mallet. Many mallet fingers present late, sometimes weeks to months after injury. A trial of continuous extension splinting for at least eight weeks is still worthwhile — a proportion will gain useful, even complete, extension even when treatment is delayed. If a residual lag and a swan-neck posture persist despite genuine concordant splinting, options include prolonged splinting, a figure-of-eight splint, or, for the symptomatic swan-neck, reconstructive surgery such as a superficialis tenodesis of the PIP. Counsel that a small, functionally insignificant extension lag is an acceptable outcome and is often better than the risks of late surgery. Special case — paediatric mallet (Doyle Type IVa). In children the lesion is frequently a transepiphyseal fracture (a Salter-Harris pattern) rather than a tendon rupture, because the tendon is stronger than the physis. Manage with closed reduction and splinting if significantly displaced; take care to avoid crossing the growth plate with hardware where possible. Union and remodelling potential are excellent. Complications
- Setting
- Common; accepted up to about 10 to 15 degrees if functional
- Recognition
- Inability to actively fully extend the DIP at the end of treatment, often with a small passive lag
- Prevention and management
- Prevention: concordant continuous splintage; correct splint angle. Management: a further period of extension splinting; counsel that a small lag is common and well tolerated
- Setting
- Splint-related; risk rises with marked hyperextension or a tight splint
- Recognition
- Blanching, blistering, breakdown or full-thickness skin loss over the dorsum of the DIP
- Prevention and management
- Prevention: splint in slight hyperextension only; pad prominences; review skin early. Management: relieve pressure, dress the wound; debride necrotic skin; rarely skin cover is needed
- Setting
- Late sequela of untreated or chronic mallet
- Recognition
- DIP flexion lag with PIP hyperextension; the lateral bands drift dorsally
- Prevention and management
- Prevention: early, maintained DIP extension. Management: figure-of-eight splint; for severe symptomatic cases, PIP stabilisation such as a superficialis tenodesis or oblique retinacular ligament reconstruction
- Setting
- K-wire fixation; increases with duration and poor pin care
- Recognition
- Erythema, pain, discharge and looseness at the wire entry site
- Prevention and management
- Prevention: meticulous pin care, protective caps, cap the wire outside skin. Management: oral antibiotics (for example cefalexin); remove loose or infected wires early and convert to splintage
- Setting
- Small K-wires in a tiny, mobile bone
- Recognition
- Loss of reduction on imaging; bent or fractured wire; change in finger posture
- Prevention and management
- Prevention: bend and cut wires cleanly outside the skin; protect with a splint; warn the patient to report catching. Management: remove the migrated wire, reassess reduction, re-pin or splint as indicated
- Setting
- Nail-matrix injury from hardware or proximal dissection
- Recognition
- Split, ridged or absent nail growth; eponychial scarring
- Prevention and management
- Prevention: avoid the germinal matrix with wires and incisions; protect the nail fold. Management: nail ablation or reconstruction for severe deformity
- Setting
- Intra-articular bony mallet, especially if reduction imperfect
- Recognition
- Pain, stiffness and deformity at the DIP; joint-space narrowing and subluxation on imaging
- Prevention and management
- Prevention: anatomical reduction when operating; congruent joint at completion. Management: activity modification; a stiff, painful DIP may eventually need arthrodesis
- Setting
- Prolonged immobilisation and surgical handling
- Recognition
- Reduced active and passive range; PIP flexion contracture
- Prevention and management
- Prevention: keep the PIP free and moving from day one; structured wean of the DIP splint. Management: hand therapy, static progressive splinting, rarely contracture release
Viva & Exam Focus
MALLETMALLET — assessment and management
SPLINTSPLINT — principles of extension splinting
The trap: operating on a bony mallet purely because the dorsal fragment looks large. Fragment size on its own does not predict outcome. The fix: on a true lateral DIP radiograph, look specifically for volar (palmar) subluxation of the distal phalanx — it is the subluxated joint together with a large fragment that drives the decision to operate, not the fragment in isolation.
The rule: splintage must be continuous, day and night. If the patient removes the splint and the DIP flexes even once — including during washing — the entire 6 to 8 week count starts over. The fix: teach skin care with the finger held flat and the DIP supported on a table so the tip never drops; audit concordance at every clinic visit.
The risk: holding the DIP in marked hyperextension, or a splint that is too tight, devascularises the thin dorsal skin over the DIP, producing blistering and full-thickness necrosis. The fix: splint in slight hyperextension only; pad bony prominences; review the skin within the first week and at each change — skin blanching on extension means the angle is too great.
The risk: a longitudinal K-wire crossing the DIP can injure the germinal or sterile nail matrix, producing a deformed nail; a tight dorsal splint can pressure the eponychial fold. The fix: when transfixing the DIP, pass the wire along the axis that avoids the nail matrix and keep the entry point clear of the eponychium; keep splints off the proximal nail fold.
Why it happens: a chronic mallet leaves the terminal tendon lax; extensor force is transmitted proximally to the central slip through the lateral bands, producing PIP hyperextension and a DIP flexion lag. The fix: prevent it by achieving and maintaining DIP extension early; an established swan-neck may be managed with a figure-of-eight splint, or in severe symptomatic cases with PIP stabilisation such as a superficialis tenodesis.
The trap: treating an open (laceration) mallet as a routine closed Type I injury with splintage alone. The fix: an open injury is a different problem — it needs wound lavage and debridement, direct terminal-tendon repair, and usually a longitudinal K-wire across the DIP to hold extension for about 6 weeks while the tendon heals.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old cricketer was struck on the tip of his right ring finger by a ball two days ago. He cannot straighten the end of his finger, but he can bend it normally and passive extension of the DIP is full. A true lateral radiograph shows no fracture and a congruent DIP joint. What is your management?”
“A 42-year-old labourer injured his middle finger a week ago. He cannot extend the DIP. A true lateral radiograph shows a bony mallet with a dorsal fragment involving approximately half of the articular surface and clear volar (palmar) subluxation of the distal phalanx. How do you manage him, and what operation would you offer?”
“A 60-year-old man presents with a mallet deformity of his index finger that he thinks happened about three months ago. He never sought treatment. He now has a DIP extension lag with early PIP hyperextension — a developing swan-neck posture. The joint is congruent on radiograph. What is your management?”
Definition and diagnosis
- Mallet finger = disruption of the terminal extensor tendon at its insertion on the dorsal base of the distal phalanx, at the DIP joint
- Hallmark: loss of active DIP extension with preserved passive extension
- Mechanism: forced flexion of an actively extended DIP ('baseball finger'), or a direct blow or laceration
- Tendinous (soft-tissue) mallet versus bony mallet (avulsion of the dorsal base)
- Always assess a true lateral DIP radiograph for fragment size and, crucially, volar subluxation
Classification (Doyle)
- Type I: closed, soft-tissue, with or without a tiny fragment — splint
- Type II: laceration with tendon continuity preserved or lost — repair
- Type III: deep abrasion with skin and tendon substance loss — repair and cover
- Type IVa: paediatric transepiphyseal fracture — reduce if displaced
- Type IVb: intermediate bony fragment, no subluxation — trial of splinting
- Type IVc: large fragment with volar subluxation — operative fixation
Non-operative (mainstay)
- Continuous DIP extension splint in slight hyperextension for six to eight weeks, then wean over two to six weeks
- The PIP is left free and moved from day one
- Any flexion of the DIP while the splint is off restarts the clock
- Skin care with the DIP supported flat on a table so the tip never drops
- Works for soft-tissue mallets, most bony mallets, and many chronic neglected mallets
Operative indications
- Large bony fragment with volar subluxation of the distal phalanx (Doyle IVc) — the unstable joint must be reduced
- Open injuries (Doyle II and III) — washout, repair and DIP stabilisation
- Selected failures of a genuine concordant splinting trial
- Fragment size alone, without subluxation, is NOT an operative indication
- Cochrane evidence shows no benefit of surgery over splinting for the typical closed mallet
Operative technique — key steps
- Ishiguro extension-block pinning: flex PIP to 90 degrees, pass a dorsal block wire in the distal middle phalanx angled distally, extend the DIP to reduce the fragment, then transfix the DIP with a longitudinal wire
- ORIF: dorsal or midaxial approach, protect the nail matrix, reduce the fragment, fix with a mini screw, K-wires or a pull-out suture
- Open mallet: lavage, tendon repair with 4-0 or 5-0 suture, longitudinal DIP wire for about six weeks
- Always protect fixation with a longitudinal DIP transfixion wire for about six weeks
- Confirm joint congruity on a true lateral image before leaving theatre
Surgical anatomy
- Terminal tendon = confluence of the two lateral bands, inserting on the dorsal base of the distal phalanx
- Extensor zones: Zone I (DIP) is the mallet zone; Zone III (PIP) is the central slip — boutonniere
- Oblique retinacular ligament links DIP extension to PIP extension (Landsmeer's linkage)
- Swan-neck arises as the lax terminal tendon transfers extensor force to the central slip via the lateral bands
- The distal phalanx is small with a thin dorsal cortex and the nail matrix volar — fixation is unforgiving
Danger zones
- Dorsal skin over the DIP: pressure necrosis from marked hyperextension or a tight splint
- Nail germinal matrix: injury from a longitudinal K-wire or proximal dissection
- Volar subluxation: missed on an oblique view — read a true lateral radiograph
- The PIP: stiffens if immobilised — keep it free and moving
- Small K-wires in a tiny mobile bone: migration, breakage and pin-tract infection
Complications
- Residual extension lag: common; a small lag is functionally acceptable
- Dorsal skin maceration or necrosis: prevent by splinting in slight hyperextension and reviewing skin
- Swan-neck deformity: the classic late sequela; figure-of-eight splint, or surgery for severe cases
- Pin-tract infection and wire migration or breakage: pin care, protective caps, early removal of loose wires
- Nail deformity, DIP stiffness and DIP arthritis: counsel pre-operatively
Special cases
- Chronic or neglected mallet: still offer continuous splinting for at least eight weeks — many improve
- Paediatric mallet (IVa): usually a transepiphyseal fracture — reduce if displaced, avoid the physis with hardware
- Congruent bony mallet with a large fragment: splint, do not operate, because fragment size alone does not predict outcome
- Open mallet: a different problem — washout, tendon repair and DIP wire for six weeks
- Return to contact sport only with a protective splint in situ
Background & Evidence
The extensor mechanism over the finger. The extensor tendon flattens over the dorsum of the finger into the extensor expansion (hood). At the level of the proximal phalanx it splits into a central slip (inserting on the base of the middle phalanx) and two lateral bands that pass distally on either side of the PIP. The two lateral bands converge over the dorsum of the middle phalanx to form the terminal (extensor) tendon, which inserts on the dorsal base of the distal phalanx — it is the terminal tendon that is disrupted in a mallet finger. Stabilising ligaments of the expansion. The triangular ligament links the two lateral bands dorsally over the middle phalanx, keeping them from drifting volarly; the transverse retinacular ligament anchors the bands volar to the PIP axis and limits PIP hyperextension; and the oblique retinacular ligament (ORL) runs from the flexor sheath at the proximal phalanx, passes volar to the PIP axis, and joins the terminal tendon, linking DIP extension to PIP extension (Landsmeer's linkage). Why a mallet becomes a swan-neck. When the terminal tendon fails, the DIP cannot extend and sits flexed. With the terminal insertion no longer tensioned, the lateral bands and the extensor force are redirected proximally to the central slip, driving the PIP into hyperextension; loss of the check-rein effect of the oblique and transverse retinacular ligaments compounds this. The net result is the swan-neck posture — DIP flexion lag with PIP hyperextension — the classic late sequela of an untreated or chronic mallet. Extensor tendon zones (Doyle): | Zone | Location | Key structure and classic lesion | |------|----------|----------------------------------| | I | DIP joint | Terminal tendon — mallet finger | | II | Middle phalanx | Lateral bands and terminal tendon | | III | PIP joint | Central slip insertion — boutonniere deformity | | IV | Proximal phalanx | Extensor expansion | | V | MCP joint | Sagittal bands — subluxation of the extensor | | VI | Metacarpal | Extensor digitorum communis | | VII | Wrist | Extensor retinaculum | | VIII | Distal forearm | Muscle bellies | The distal phalanx as a fixation target. The distal phalanx is small, with a thin dorsal cortex and the nail apparatus draped over its volar surface: there is limited bone stock for screws or wires, the germinal matrix of the nail lies volar to the dorsal base (at risk from dorsally placed hardware or a proximal incision), and the tuft is cancellous and does not hold fine hardware well. These constraints explain why percutaneous pinning (which needs only a small footprint of purchase) is often preferred over screw fixation, and why hardware problems dominate the complication list for this tiny bone.
- Description
- Closed, soft-tissue (tendinous), with or without a tiny avulsion fragment
- Typical management
- Continuous extension splinting
- Description
- Laceration, tendon continuity preserved or lost
- Typical management
- Surgical repair
- Description
- Deep abrasion with loss of skin, subcutaneous tissue and tendon substance
- Typical management
- Surgical repair, often soft-tissue cover
- Description
- Paediatric — transepiphyseal fracture (Salter-Harris pattern)
- Typical management
- Closed reduction and splinting if displaced
- Description
- Bony fragment of intermediate size, no volar subluxation
- Typical management
- Trial of continuous splinting
- Description
- Large bony fragment with volar (palmar) subluxation of the distal phalanx
- Typical management
- Operative fixation
Evidence base. - Cochrane systematic review (Handoll and Vaghela): randomised trial evidence for treating mallet finger is limited and insufficient to determine the single best treatment; no trial has shown surgery to be superior to conservative splinting for the typical closed injury.
- Wehbe and Schneider (1984): in a landmark review of mallet fractures, the size of the fracture fragment did not correlate with the clinical result, supporting conservative management of most bony mallets.
- Crawford (1984): the molded polyethylene splint (the basis of the Stack-type splint) holds the DIP in extension while allowing skin care, improving patient concordance — the principle that underpins modern non-operative management.
- Operative series: extension-block (Ishiguro) pinning and ORIF are reported to give good reduction and outcome in bony mallets with volar subluxation, but they are reserved for the minority with an unstable joint.
References
Interventions for treating mallet finger injuries
- Systematic review of randomised trials evaluating treatment for mallet finger injuries
- Found insufficient evidence from randomised trials to determine the single most effective treatment
- No trial demonstrated clear superiority of surgery over conservative splinting for the typical closed mallet
Mallet fractures
- Review of the management of bony (mallet) fractures of the distal phalanx
- Concluded that the size of the fracture fragment did not correlate with the clinical result
- Supported conservative splint management for most mallet fractures
The molded polythene splint for mallet finger deformities
- Described a molded thermoplastic splint holding the DIP in extension while allowing skin care
- Allowed removal for hygiene with the joint supported, improving concordance with continuous splintage
- Became the basis of the widely used Stack-type mallet splint
Mallet deformity of the finger. Five-year follow-up of conservative treatment
- Reported five-year follow-up outcomes of conservatively treated mallet finger deformities
- Found that good functional results can be achieved with continuous extension splintage alone
- Demonstrated that the presence of a bony fragment does not necessarily worsen the outcome with conservative treatment
Acute Mallet Finger Injuries - A Review
- Comprehensive contemporary review of acute mallet finger injuries covering diagnosis, classification and management
- Reinforced that continuous extension splinting remains the mainstay for most closed mallet injuries
- Summarised operative indications and outcomes for extension-block pinning and ORIF in bony mallets with volar subluxation