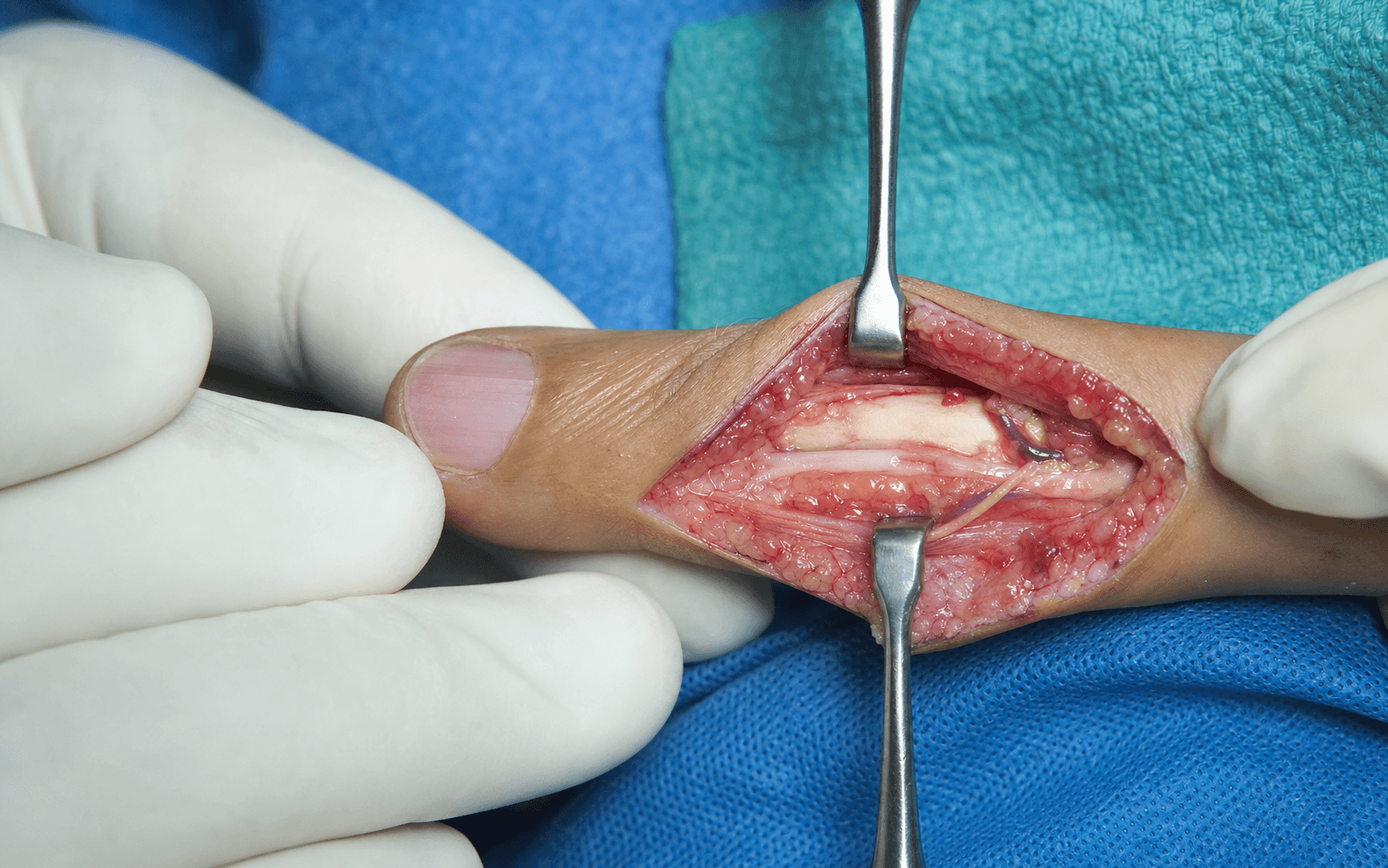
Lateral exposure of the phalanx, flexor sheath and PIP joint collateral ligaments through a non-contact-border incision that keeps the digital neurovascular bundle volar and protected.
- Non-contact border — ulnar for index and middle fingers, radial for ring and little fingers.
- The digital neurovascular bundle lies immediately volar to the mid-axial line and stays volar and protected throughout.
- Cleland ligaments are dorsal to the bundle and Grayson ligaments are volar — they define the two safe dissection planes.
- There is no true internervous plane — all tissues of the digit are supplied by the digital nerves, so safety comes from an interfascical dissection that stays dorsal to the bundle.
- The incision joins the dorsal apices of the flexion creases on the chosen border, so the scar avoids the contact surface of pinch and grasp and will not cause a flexion-contracture crease.
When & Why
What it exposes. The mid-axial approach gives direct lateral access to the phalanx, the flexor tendon sheath and the PIP (and DIP) joint collateral ligaments. It is the workhorse exposure for phalangeal open reduction and internal fixation, PIP collateral ligament repair, volar plate work, flexor sheath exploration and excision of lateral masses. Why the mid-axial line (and not volar or dorsal). Placing the incision on the non-contact border keeps the scar off the working surface of the finger, preventing the painful scar contracture that would impair pinch and grasp. It also keeps the digital neurovascular bundle volar to the incision throughout, so the bundle is protected by remaining dorsal to it, and it reaches the flexor sheath without crossing the volar pulp. A dorsal approach is reserved for the extensor mechanism and dorsal lip fractures; a volar Bruner or straight incision is chosen for flexor tendon repair or volar plate/pulp work. Primary indications. - Phalangeal shaft, neck or base fractures requiring open reduction and internal fixation
- PIP joint fracture-dislocations needing collateral ligament repair or volar plate arthroplasty
- Collateral ligament injuries of the PIP or DIP joint requiring direct repair or reconstruction
- Excision of mucous cysts, giant cell tumours of tendon sheath or other lateral masses
- Flexor tendon sheath exploration or pulley release when a volar approach is undesirable
- Osteomyelitis or septic arthritis drainage of the phalanx or PIP joint Contraindications. Pathology requiring dorsal access (extensor mechanism, dorsal lip fractures), volar pulp or fingertip pathology, previous scarring or infection on the planned mid-axial line, and any case needing circumferential access.
- Dissection plane
- Dorsal to the neurovascular bundle, between Cleland and Grayson ligaments
- Exposes
- Phalanx and flexor sheath
- Dissection plane
- Volar to Cleland ligament
- Exposes
- Collateral ligament repair
- Dissection plane
- Continued along the mid-axial line into the web space
- Exposes
- MP joint or metacarpal head
Alternative approaches. Dorsal approach (extensor tendon repair, dorsal lip fractures, central slip injuries); Bruner volar zigzag (flexor tendon repair, volar plate exposure, pulley reconstruction); volar straight incision (limited volar access); lateral approach with nail-fold elevation (distal phalanx or nail-bed pathology).
The Exposure
Work down through the layers on the non-contact border, identifying and protecting the digital neurovascular bundle early, then develop one of the two interfascial planes — dorsal to Cleland or volar to Grayson — to reach the bone, sheath or joint.
Exposure sequence
- Patient supine with the arm on a hand table; upper-arm tourniquet inflated to 250 mmHg (or 100 mmHg above systolic) after Esmarch exsanguination. Loupe magnification (2.5x or greater) is mandatory throughout.
- Select the non-contact border — ulnar for index and middle, radial for ring and little. Palpate the PIP and DIP joint lines and the digital neurovascular bundle (a longitudinal ridge just volar to the planned line when the finger is flexed).
- Mark the dorsal-most point (apex) of each flexion crease on the chosen border and join them with a straight line — this is the mid-axial line. Tourniquet time should not exceed 120 minutes; document it and release before closure if the procedure exceeds 90 minutes.
- Incise precisely along the mid-axial line, joining the dorsal apices of the flexion creases (typically 3-5 cm for a single phalanx or PIP joint).
- Carry the first pass through skin and subcutaneous fat only, staying on the dorsal margin of the neurovascular bundle.
- Under loupe magnification, identify the digital artery and nerve within the subcutaneous fat immediately volar to the incision (the artery lies dorsal to the nerve).
- Gently dissect them free and encircle with a vessel loop or Penrose drain, retracting the bundle volarly. Check capillary refill of the fingertip after retraction to confirm perfusion, and release retraction every 20 minutes to prevent ischaemic neurapraxia.
- Dorsal to Cleland ligament — divide or elevate the thick fibrous Cleland ligaments from the phalanx to reach the bone or extensor apparatus (used for phalangeal fracture fixation or dorsal pathology).
- Volar to Grayson ligament — divide the Grayson ligaments to reach the flexor sheath (used for flexor tendon exploration or volar plate access). The bundle remains protected volar to this plane.
- For phalangeal exposure, incise and elevate the periosteum subperiosteally, staying on bone and avoiding dorsal over-dissection of the extensor apparatus.
- For flexor sheath exposure, visualise the sheath and preserve the A2 and A4 pulleys when possible, opening only between them if required.
- For joint access, the PIP collateral ligaments may be divided at their volar or dorsal attachment and repaired at closure.
- With the phalanx, sheath or joint exposed, perform the planned procedure (fracture fixation, ligament repair, pulley work, drainage or excision).
- Confirm neurovascular integrity (colour, refill, two-point discrimination) before closure, and repair any collateral ligament that was divided.
The digital artery and nerve lie immediately volar to the mid-axial line and are injured if the plane is lost, causing permanent sensory loss and cold intolerance in the affected hemidigit. Prevention is the whole technique: stay on the non-contact border, identify and loop the bundle in the subcutaneous fat before any deep dissection, retract it gently volarly with a vessel loop, check capillary refill, and release retraction every 20 minutes. With careful technique the permanent neurovascular injury rate is less than 1 percent.
The mid-axial approach is an interfascial dissection rather than an internervous one, because every layer of the digit is supplied by the digital nerves. Once the bundle is identified and retracted volarly, choose the plane dorsal to Cleland ligament (to reach bone or the extensor apparatus) or volar to Grayson ligament (to reach the flexor sheath). Both planes are safe provided the bundle is protected volarly.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Digital neurovascular bundle (artery dorsal to nerve)
- Protection
- Identify early in the subcutaneous fat; vessel loop; gentle volar retraction; check capillary refill; release every 20 minutes
- Structure at risk
- Extensor apparatus
- Protection
- Stay subperiosteal; avoid dorsal over-dissection
- Structure at risk
- Flexor tendons and A2/A4 pulleys
- Protection
- Preserve A2 and A4 pulleys; open the sheath only between them
- Structure at risk
- PIP collateral ligaments
- Protection
- Repair or reconstruct if divided for access
- Structure at risk
- Transverse digital artery at the web space; dorsal sensory branches
- Protection
- Identify and protect before extending into the web
Extensile options. Extend proximally along the same mid-axial line into the web space to reach the metacarpal head and MP joint — identify and protect the transverse digital artery and the dorsal sensory branches at the web. Distal extension is limited by the nail fold; the incision may reach the lateral nail fold for the distal phalanx or DIP joint, but elevating the nail fold risks nail deformity. For circumferential access, a second mid-axial incision on the opposite border is useful for comminuted fractures or wide tumour margins — the two incisions must not meet at the tip or web, to avoid devascularising the skin bridge. Closure. Close skin with interrupted 5-0 or 6-0 nylon or absorbable monofilament, having confirmed the neurovascular bundle lies in its anatomical position without kinking or tension. The flexor sheath and periosteum are not closed routinely; any collateral ligament divided for access is repaired with 3-0 or 4-0 braided suture to bone or soft tissue. Release the tourniquet before closure to achieve haemostasis, and apply a bulky dressing with a dorsal plaster slab or aluminium splint holding the PIP joint in slight flexion. Aftercare. Strict elevation for 48 hours; active range of motion from 48-72 hours unless contraindicated; protective splinting for 3-6 weeks depending on the procedure; suture removal at 10-14 days; oedema control and scar massage from 3 weeks to prevent contracture. Pitfalls and complications. Digital neurovascular injury (less than 1 percent permanent deficit with careful technique); painful scar contracture on the contact surface if the wrong border is chosen; flexor tendon adhesion if the sheath is violated unnecessarily; PIP stiffness from prolonged immobilisation or scarring; nail deformity if extended too far distally; and web-space contracture if the transverse ligament is damaged. Suspected nerve injury recognised intra-operatively is explored immediately; established flexor adhesion is managed with early tenolysis if motion plateaus; PIP stiffness with dynamic splinting and hand therapy; and a functionally limiting scar with Z-plasty revision.
Procedures Through This Approach
- Finger fracture fixation — open reduction and internal fixation of phalangeal shaft, neck or base fractures.
- PIP joint collateral ligament repair or reconstruction, and volar plate arthroplasty for fracture-dislocations.
- Flexor tendon sheath exploration, pulley release or pulley reconstruction.
- Excision of mucous cysts, giant cell tumours of tendon sheath or epidermal inclusion cysts.
- Drainage of septic arthritis or osteomyelitis of the phalanx or PIP joint; bone grafting of non-union; hardware removal. Fixation options through this approach. 1.5 mm or 2.0 mm lag screws for spiral or long oblique fractures; 1.5 mm or 2.0 mm plates for comminuted or transverse fractures; K-wires for simple fractures or temporary stabilisation; suture-anchor repair of collateral ligaments to bone; and volar plate advancement and reattachment for fracture-dislocations.
Viva & Exam Focus
MIDAXIALMIDAXIAL — the lateral digit exposure
PROTECTPROTECT — the digital neurovascular bundle
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old carpenter has a spiral fracture of the proximal phalanx of the ring finger with greater than 2 mm shortening. How would you approach surgical fixation?”
“A 35-year-old athlete has a complete radial collateral ligament rupture of the PIP joint of the index finger, unstable to stress testing in extension. How would you expose and repair it?”
“A 40-year-old musician needs flexor sheath exploration of the little finger for suspected pulley rupture and bowstringing after a laceration. How do you gain safe access while preserving the critical pulleys?”
Incision placement
- Non-contact border: ulnar for index/middle, radial for ring/little
- Join the dorsal-most apices of the flexion creases
- Straight line along the mid-axial border, 3-5 cm for a single phalanx or PIP joint
- Extend proximally into the web or distally to the nail fold only if needed
Neurovascular protection
- Digital artery and nerve lie just volar to the mid-axial line
- Identify the bundle in the subcutaneous fat before deep dissection
- Encircle with a vessel loop or Penrose drain
- Retract volarly and check capillary refill
- Release retraction every 20 minutes to prevent ischaemia
Dissection planes
- Dorsal to Cleland ligament: reach the phalanx or extensor apparatus
- Volar to Grayson ligament: reach the flexor sheath
- Cleland ligaments connect the phalanx to dorsal skin
- Grayson ligaments connect the flexor sheath to volar skin
- No true internervous plane — an interfascical dissection
Danger structures
- Proper digital artery and nerve — protect with a vessel loop
- Flexor tendons and A2/A4 pulleys — preserve when possible
- PIP collateral ligaments — repair if divided for access
- Transverse digital artery at the web — protect during proximal extension
Procedures accessible
- Phalangeal ORIF with lag screws or mini-plates
- PIP collateral ligament repair or reconstruction
- Volar plate arthroplasty for fracture-dislocations
- Flexor sheath exploration and pulley reconstruction
- Tumour or cyst excision on the lateral digit
Closure and aftercare
- Interrupted 5-0 or 6-0 nylon skin closure
- Repair any collateral ligament divided for access
- Bulky dressing with a dorsal blocking splint
- Elevation for 48 hours; early motion at 48-72 hours
- Suture removal at 10-14 days; protective splint for 3-6 weeks
References
Surgical Management of Pachydermodactyly (PDD) via Midaxial Incision: A Case Report
- Midaxial incision provided direct access to the digit for lesion management while maintaining neurovascular protection
- Confirmed the safety and efficacy of the mid-axial approach for lateral digit pathology
Repair of the Thumb Ulnar Collateral Ligament With Suture Tape Augmentation
- Lateral approaches including mid-axial exposure are standard for collateral ligament repair at the thumb MP joint
- Suture tape augmentation enhances stability during reconstruction through protected mid-axial planes
Clinical Characteristics of Pyogenic Flexor Tenosynovitis in Pediatric Patients
- Flexor sheath access via safe lateral planes such as mid-axial minimises neurovascular risk in children
- Preservation of critical pulleys and early motion protocols improve outcomes after sheath exploration
Primary care of the injured hand, part 2
- Early descriptions of lateral mid-axial approaches to the phalanges for fracture and tendon injuries
- Emphasised identification and protection of the digital neurovascular bundle during exposure