Lateral oblique approach and medialising calcaneal tuberosity osteotomy for hindfoot valgus correction — intermediate
- The osteotomy is performed through a lateral oblique incision posterior to the peroneal tendons, directed from superolateral to inferomedial, ending 1-2 cm anterior to the posterior calcaneal tuberosity border. The cut lies posterior and inferior to the posterior facet and must protect the sural nerve (crossing the incision in 70-80 percent of cases) and the lateral calcaneal nerve branches.
- Medial translation of the tuberosity (typically 8-12 mm) medialises the Achilles insertion and shifts the ground reaction force vector medially, converting the Achilles from a valgus deforming force to a neutral or slight varus-correcting force — this is the core biomechanical rationale for correcting flexible hindfoot valgus.
- The medial neurovascular bundle (posterior tibial artery, tibial nerve and its calcaneal branches) lies immediately medial to the osteotomy site; the osteotomy must stop short of the medial cortex and the final cut completed with an osteotome under direct vision to avoid direct or stretch injury to these structures.
- MDCO is almost always performed as part of a reconstruction for stage II PTTD and is combined with FDL transfer to the navicular, spring ligament repair or reconstruction, and frequently lateral column lengthening when forefoot abduction or lateral column shortening is present — isolated MDCO rarely suffices for full deformity correction.
- “Mark the sural nerve pre-operatively with the ankle in plantarflexion and inversion — it crosses the incision line in 70-80 percent of cases and must be mobilised and protected throughout.
- “The osteotomy cut is oriented 45 degrees to the plantar surface, starting 1 cm posterior to the posterior facet and directed toward the plantar-medial calcaneus just anterior to the medial neurovascular bundle — this trajectory protects the sustentaculum and allows safe medial translation.
- “Medial translation greater than 10 mm increases the risk of medial soft-tissue impingement and wound tension on the medial side; most surgeons aim for 8-10 mm and accept slight residual valgus rather than overcorrect into varus.
- “Fixation is typically with one or two 6.5-7.0 mm cannulated partially threaded screws from the tuberosity into the anterior calcaneus; the screws must engage the anterior process or sustentaculum for stable purchase — avoid short screws that fail to cross the osteotomy adequately.
When & Why
A medial displacement calcaneal osteotomy corrects a flexible hindfoot valgus by sliding the posterior tuberosity medially, which medialises the Achilles insertion and turns the Achilles from a deforming valgus force into a corrective one. It is a bony realignment that, on its own, addresses only one component of the deformity — so in practice it is almost always combined with soft-tissue and adjunctive bony procedures for stage II posterior tibial tendon dysfunction (PTTD). Primary indications - Flexible hindfoot valgus in stage II PTTD with preserved subtalar motion.
- Symptomatic flexible flatfoot with hindfoot valgus greater than 5-7 degrees on weight-bearing radiographs.
- Cavovarus correction using the lateralising (reverse) variant of the osteotomy.
- Combined reconstruction where medial column insufficiency and an Achilles valgus vector both need realignment. Concomitant procedures — almost always required - FDL transfer to the navicular or medial cuneiform (restores active inversion).
- Spring ligament repair or reconstruction (direct repair, graft augmentation or internal brace).
- Lateral column lengthening (Evans or Hintermann osteotomy) when forefoot abduction or lateral column shortening is present.
- Gastrocnemius or Achilles lengthening when an equinus contracture contributes to the deformity. The key surgical decision is therefore not whether to do an MDCO, but what to add to it:
For stage II PTTD: MDCO medialises the Achilles vector while FDL transfer, spring ligament repair and (often) lateral column lengthening correct the medial column and forefoot abduction. The combination gives durable correction.
Occasionally used for flexible flatfoot hindfoot valgus without medial column pathology, but higher failure rates — most deformities have several components that MDCO alone cannot address.
The same osteotomy translated laterally corrects a flexible cavovarus hindfoot (for example Charcot-Marie-Tooth), shifting the Achilles vector the opposite way.
Contraindications - Absolute: rigid hindfoot valgus (stage III or IV PTTD) with subtalar arthritis or fixed deformity — these require arthrodesis; active infection or ulceration over the lateral heel; severe peripheral vascular disease precluding safe wound healing.
- Relative: severe osteoporosis increasing nonunion risk; smokers who cannot cease nicotine peri-operatively; isolated hindfoot valgus without medial column pathology (rare — MDCO alone is seldom sufficient). Consent. Discuss sural nerve injury (5-15 percent), nonunion (3-8 percent), hardware prominence requiring removal (10-20 percent), under- or over-correction, wound complications, and the frequent need for concomitant procedures (FDL transfer, lateral column lengthening). Setup. Supine with a bump under the ipsilateral hip to internally rotate the leg, or lateral decubitus with the operative side up; the foot is placed at the end of the table to allow full ankle and subtalar motion. A thigh tourniquet is applied but rarely inflated. General or spinal anaesthesia with a popliteal or ankle block for post-operative analgesia (WALANT is not suitable for this bony procedure). Position a mini C-arm or image intensifier to obtain lateral, axial and Harris heel views intra-operatively, and confirm you can visualise the entire calcaneus and subtalar joint before prepping.
The Operation
The goal: through a lateral oblique approach, expose the calcaneal body posterior to the peroneal tendons, cut the tuberosity obliquely at 45 degrees to the plantar surface (posterior and inferior to the posterior facet), translate the fragment 8-10 mm medially to medialise the Achilles insertion, and fix it with cannulated screws — almost always as part of a staged PTTD reconstruction. The exposure is laid out step by step below.
Operative sequence
- Supine with an ipsilateral hip bump (internally rotates the leg) or lateral decubitus; foot at the end of the table for full ankle and subtalar motion; thigh tourniquet applied but rarely inflated.
- With the foot in plantarflexion and inversion, palpate and mark the sural nerve course on the skin — it crosses the incision in 70-80 percent of patients and must be protected throughout.
- A 5-7 cm oblique incision starting about 2 cm posterior to the tip of the lateral malleolus, directed toward the plantar-medial calcaneus and ending 1-2 cm anterior to the posterior border of the calcaneal tuberosity.
- The incision lies posterior to the peroneal tendons and crosses the sural nerve in most patients.
- Identify the sural nerve in the subcutaneous fat and mobilise it on a vessel loop, retracting it anteriorly or posteriorly as its course dictates.
- Preserve visible lateral calcaneal nerve branches and avoid excessive flap undermining, which risks wound-edge necrosis.
- Retract the peroneal tendons anteriorly with a blunt Hohmann or Langenbeck retractor protected by a rubber dam; expose the lateral wall from the posterior facet margin to the tuberosity, using the peroneal tubercle as an anterior landmark.
- Elevate periosteum sharply in a single layer and place two Hohmann retractors — one superiorly beneath the posterior facet and one inferiorly at the plantar border — to shield the soft tissues during the cut.
- Confirm the level on a lateral fluoroscopic view: the cut starts about 1 cm posterior and inferior to the posterior facet, remaining at least 8-10 mm clear of the joint, angled 45 degrees to the plantar surface.
- The trajectory aims toward the plantar-medial calcaneus just anterior to the sustentaculum, which protects the sustentaculum and allows safe medial translation.
- Make the lateral cut with a narrow oscillating saw under direct vision, stopping 2-3 mm short of the medial cortex.
- Complete the cut with a broad osteotome, feeling the controlled give as the medial cortex breaches; keeping the osteotome anterior to the sustentaculum protects the medial neurovascular bundle.
- Translate the tuberosity medially 8-10 mm with a lamina spreader or bone hook; confirm correction on an axial (Harris) heel view — the tuberosity should sit directly under the talus in neutral or slight valgus.
- Hold the position with a 1.6 mm or 2.0 mm K-wire from the tuberosity into the anterior calcaneus and confirm translation on lateral and axial views before definitive fixation.
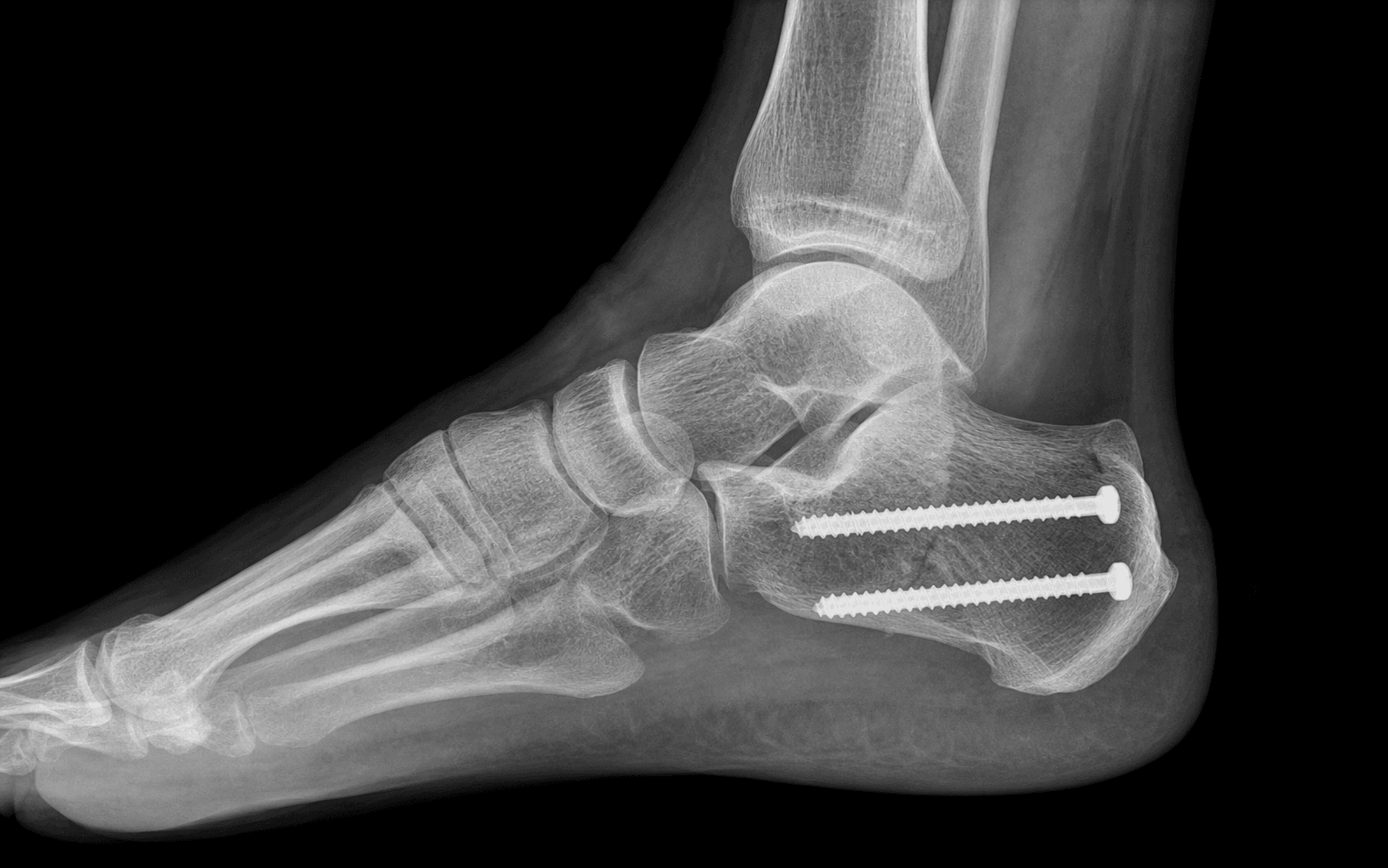
- Insert one or two 6.5-7.0 mm cannulated partially threaded screws (typically 50-60 mm) over the K-wires, engaging the anterior process or sustentaculum for stable purchase.
- With two screws use a divergent configuration (one into the anterior process, one into the sustentaculum); countersink the heads to reduce hardware prominence, and confirm compression with no subtalar or calcaneocuboid penetration on fluoroscopy.
- Irrigate, confirm haemostasis, and close the subcutaneous layer with absorbable suture, taking care not to catch the sural nerve; close the skin with non-absorbable suture or staples.
- Apply a bulky compressive dressing and a below-knee posterior splint with the ankle in neutral.
The posterior tibial artery, tibial nerve and their calcaneal branches lie immediately medial to the osteotomy, protected only by the medial cortex and periosteum. Stop the saw 2-3 mm short of the medial cortex and complete the cut with an osteotome under direct vision, keeping the trajectory anterior to the sustentaculum. Never drive a saw or osteotome across the medial wall blindly — direct laceration or stretch causes plantar numbness, vascular compromise or chronic tarsal tunnel pain (incidence less than 1 percent, but devastating when it occurs).
With the foot in plantarflexion and inversion the sural nerve is easier to palpate along the lateral border of the Achilles. Mark its course on the skin, then identify it in the subcutaneous fat immediately after incision and mobilise it onto a vessel loop. Once the nerve is controlled, the rest of the exposure is safe — never cut blindly in the subcutaneous plane. Routine identification and protection cut symptomatic injury from roughly 22 percent down to 4 percent.
Structures at risk in the lateral calcaneal approach
- Where: subcutaneous, along the lateral border of the Achilles, crossing the incision obliquely 1-2 cm anterior to the posterior calcaneal border. - Risk: transection or traction — lateral foot numbness and a painful neuroma (up to 15-20 percent when not identified; 5-15 percent in modern series). - Protect: mark in plantarflexion and inversion, mobilise on a vessel loop, preserve visible branches.
- Where: the posterior tibial artery, tibial nerve and calcaneal branches lie immediately medial to the osteotomy, shielded only by the medial cortex and periosteum. - Risk: direct laceration or stretch — plantar numbness, vascular compromise, chronic tarsal tunnel pain (less than 1 percent). - Protect: stop the saw short of the medial cortex and complete the cut with an osteotome under direct vision; never breach the medial wall blindly.
- Where: terminal branches supply the lateral heel skin and the incision itself. - Risk: division — chronic lateral heel dysaesthesia and wound pain that can persist for years. - Protect: preserve visible subcutaneous branches; avoid excessive retraction and deep cautery in the subcutaneous plane.
- Where: peroneus longus and brevis run in their sheath immediately anterior to the incision, behind the lateral malleolus. - Risk: subluxation, abrasion or partial laceration from aggressive retraction — post-operative tendinopathy or instability. - Protect: retract anteriorly with a blunt retractor protected by a rubber dam; do not place the retractor on the tendon substance.
- Where: the posterior facet lies superior and slightly anterior to the ideal osteotomy plane. - Risk: entering the joint creates iatrogenic arthritis and alters subtalar mechanics. - Protect: keep the cut at least 8-10 mm inferior and posterior to the facet margin; confirm the start point 1 cm posterior and inferior to the facet on fluoroscopy.
- Where: cross the medial calcaneal tuberosity just medial to the translated fragment. - Risk: excessive translation (greater than 10-12 mm) stretches or compresses them — tarsal tunnel syndrome or vascular compromise. - Protect: limit translation to 8-10 mm; release the flexor retinaculum if more correction is genuinely required.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation and loading | Rehabilitation | |-------|--------|----------------------------|----------------| | Immediate | 0-2 weeks | Below-knee splint or cast, non-weight-bearing; strict elevation for 48-72 hours | Wound review at 10-14 days; transition to a removable boot once the wound is stable | | Protected | 2-8 weeks | Touch weight-bearing in a boot from 2-6 weeks | Active ankle and subtalar range of motion from 2 weeks; radiographs at 6 weeks | | Progressive | 8-12 weeks | Gradual progression to full weight-bearing in orthotics by 10-12 weeks | Intrinsic and peroneal strengthening; custom medial-arch orthotics | | Return to activity | 3-6 months | Full weight-bearing in supportive orthotics | Low-impact activity from 3 months; running and sport from 4-6 months | Milestones and red flags - Milestones: 2 weeks — wound healed, in a boot, gentle range of motion; 6 weeks — radiographic evidence of early union, progress weight-bearing; 3 months — full weight-bearing with a near-normal gait.
- Red flags: increasing pain at the osteotomy site, wound breakdown, or new neurological symptoms — investigate promptly with imaging and clinical review. Most patients return to desk work by about 6 weeks and to heavy manual work by 12-16 weeks; full recovery of function is expected by 6-9 months in uncomplicated cases. Complications
- Incidence
- 5-15%
- Recognition
- Lateral foot numbness, painful neuroma, positive Tinel sign along the incision
- Prevention and management
- Prevention: mark and protect the nerve with a vessel loop, preserve branches. Management: neurolysis or neurectomy for a painful neuroma; desensitisation for mild symptoms
- Incidence
- 3-8%
- Recognition
- Persistent pain at the osteotomy beyond 3 months; no bridging callus at 3-6 months
- Prevention and management
- Prevention: optimise comorbidities, two-screw fixation, smoking cessation. Management: revision fixation with bone graft if symptomatic at 6 months
- Incidence
- 10-20%
- Recognition
- Painful palpable screw heads laterally; skin irritation over the lateral heel
- Prevention and management
- Prevention: countersink heads, use low-profile implants. Management: hardware removal after radiographic union (usually greater than 6 months)
- Incidence
- 5-10%
- Recognition
- Persistent hindfoot valgus on weight-bearing radiographs; ongoing medial foot pain
- Prevention and management
- Prevention: adequate 8-10 mm translation plus concomitant soft-tissue reconstruction. Management: revision osteotomy or conversion to arthrodesis if symptomatic
- Incidence
- less than 3%
- Recognition
- Iatrogenic hindfoot varus with lateral foot overload and peroneal symptoms
- Prevention and management
- Prevention: limit translation to 8-10 mm and accept slight residual valgus. Management: lateralising revision osteotomy if symptomatic
- Incidence
- less than 1%
- Recognition
- Plantar numbness, vascular compromise, tarsal tunnel symptoms
- Prevention and management
- Prevention: complete the osteotomy with an osteotome under direct vision, limit translation. Management: explore and repair if recognised intra-operatively; tarsal tunnel release if late compression
- Incidence
- 2-5%
- Recognition
- Wound edge separation, erythema, discharge (higher in smokers and diabetics)
- Prevention and management
- Prevention: meticulous soft-tissue handling, layered closure, smoking cessation. Management: local wound care and antibiotics; return to theatre for debridement if deep infection
Viva & Exam Focus
LATERALLATERAL — approach and osteotomy landmarks
FIXATEFIXATE — fixation and post-operative protocol
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old woman with stage II PTTD presents with flexible hindfoot valgus of 9 degrees, medial foot pain and inability to perform a single-leg heel rise. Weight-bearing radiographs show 15 degrees of forefoot abduction. What is your surgical plan?”
“During MDCO the osteotomy cut enters the subtalar joint on the lateral fluoroscopic view. How do you recognise this intra-operatively and what is your management?”
“A 48-year-old man 9 months after MDCO with FDL transfer complains of persistent medial foot pain and inability to perform a single-leg heel rise. Standing radiographs show 6 degrees of residual hindfoot valgus and no evidence of osteotomy union. What is your diagnosis and surgical plan?”
Indications and contraindications
- Stage II PTTD with flexible hindfoot valgus greater than 5-7 degrees and preserved subtalar motion
- Combined with FDL transfer, spring ligament reconstruction and often lateral column lengthening
- Cavovarus correction uses the lateralising (reverse) variant
- Rigid deformity (stage III/IV) or subtalar arthritis contraindicates MDCO — requires arthrodesis
Surgical anatomy and danger zones
- Sural nerve crosses the lateral incision in 70-80 percent — mark pre-operatively and protect with a vessel loop
- Osteotomy starts 1 cm posterior and inferior to the posterior facet; stay at least 8-10 mm from the joint
- Medial neurovascular bundle lies immediately medial — complete the final cut with an osteotome under direct vision
- Peroneal tendons lie anterior to the incision — retract with a protected blunt retractor
- Medial translation of 8-10 mm is ideal; greater than 12 mm risks medial impingement and wound tension
Operative technique — critical steps
- Lateral oblique incision 5-7 cm posterior to the peroneal tendons; identify the sural nerve first
- Elevate periosteum in one layer; place Hohmann retractors superiorly and inferiorly
- Saw cut stops short of the medial cortex; complete with an osteotome feeling the controlled breach
- Translate the tuberosity 8-10 mm medially; confirm on the axial (Harris) heel view
- Fix with one or two 6.5-7.0 mm cannulated partially threaded screws engaging the anterior process or sustentaculum
- Countersink screw heads to reduce hardware prominence
Fixation principles
- Partially threaded screws provide compression across the osteotomy
- Screws must engage the anterior process or sustentaculum — short screws fail
- Two divergent screws are preferred when bone quality is poor or in revision cases
- Fluoroscopic confirmation of position, length and compression is mandatory before closure
Complications and prevention
- Sural nerve injury (5-15 percent): identify and protect in every case; preserve branches
- Nonunion (3-8 percent): optimise comorbidities, use two screws, enforce smoking cessation
- Hardware prominence (10-20 percent): countersink heads; remove after union if symptomatic
- Under-correction: ensure adequate translation and address every component of the deformity
- Medial neurovascular injury (less than 1 percent): never drive instruments across the medial cortex blindly
Post-operative protocol and evidence
- Non-weight-bearing 2 weeks, then protected weight-bearing in a boot until 8-10 weeks
- Active ROM from 2 weeks once the wound is healed; radiographs at 6 weeks
- Combined MDCO plus FDL transfer achieves 75-85 percent good to excellent results at 5-10 years
- 8-10 mm medial translation reduces the Achilles valgus moment arm by 25-35 percent
- Sural nerve identification reduces symptomatic injury from 22 percent to 4 percent
Background & Evidence
Biomechanical rationale. Medial translation of the calcaneal tuberosity shifts the Achilles insertion medially, reducing its valgus moment arm and converting the Achilles from a deforming force into a corrective one. Cadaveric work shows that 8-10 mm of displacement corrects hindfoot valgus alignment and reduces medial column overload without significantly altering subtalar kinematics when combined with appropriate soft-tissue procedures; translation beyond about 12 mm adds medial soft-tissue impingement and wound tension without further corrective benefit. Clinical outcomes. Combined MDCO with FDL transfer and spring ligament reconstruction achieves good to excellent results in 75-85 percent of stage II PTTD patients at 5-10 year follow-up, with significant improvement in AOFAS scores, hindfoot alignment and patient-reported function. Isolated MDCO without addressing the posterior tibial tendon and spring ligament has higher failure rates and is not recommended. Nonunion and complication rates. Nonunion rates range from 2-8 percent in modern series with stable screw fixation; risk factors include smoking, diabetes and inadequate screw purchase. Sural nerve injury occurs in 5-15 percent when the nerve is not specifically protected. Hardware prominence requiring removal occurs in 10-20 percent of cases.
- MDCO + FDL transfer
- 25-35 points
- Isolated MDCO
- 15-20 points
- With lateral column lengthening
- 30-40 points
- MDCO + FDL transfer
- 8-12 degrees
- Isolated MDCO
- 5-8 degrees
- With lateral column lengthening
- 10-15 degrees
- MDCO + FDL transfer
- 3-6%
- Isolated MDCO
- 5-10%
- With lateral column lengthening
- 4-8%
- MDCO + FDL transfer
- 5-12%
- Isolated MDCO
- 8-15%
- With lateral column lengthening
- 6-14%
- MDCO + FDL transfer
- 10-18%
- Isolated MDCO
- 15-25%
- With lateral column lengthening
- 12-20%
- MDCO + FDL transfer
- 80-85%
- Isolated MDCO
- 60-70%
- With lateral column lengthening
- 75-82%
References
Long-term results of medial displacement calcaneal osteotomy with flexor digitorum longus transfer for stage II posterior tibial tendon dysfunction
- Retrospective review of 129 feet at mean 5.2 years follow-up
- Good to excellent results in 79 percent of patients with combined MDCO and FDL transfer
- Hindfoot valgus corrected from mean 11 degrees to 3 degrees; AOFAS score improved 28 points
Calcaneal osteotomy for the treatment of posterior tibial tendon dysfunction: a biomechanical and clinical study
- Cadaveric model demonstrating that 10 mm of medial calcaneal displacement reduces the Achilles valgus moment arm by approximately 30 percent
- Clinical series of 25 patients showed radiographic correction of hindfoot valgus and improved medial column loading
Results of calcaneal osteotomy and flexor digitorum longus transfer for the treatment of stage II posterior tibial tendon dysfunction
- Original description of the combined procedure in 19 patients
- All patients demonstrated improved alignment and function at short-term follow-up
- Established MDCO plus FDL transfer as the standard reconstruction for flexible flatfoot
Sural nerve injury after calcaneal osteotomy: incidence and prevention
- Retrospective review of 68 calcaneal osteotomies with a 12 percent incidence of sural nerve symptoms
- Nerve identification and protection reduced symptomatic injury from 22 percent to 4 percent
Nonunion after medial displacement calcaneal osteotomy: risk factors and management
- Review of 142 MDCO procedures with a 5.6 percent nonunion rate
- Smoking, diabetes and single-screw fixation were independent risk factors for nonunion