Titanium elastic nailing for length-stable midshaft fractures in children 5 to 11 years
- Indications are strictly length-stable transverse or short-oblique midshaft fractures in children typically 5 to 11 years of age and weighing less than 50 kg. Length-unstable patterns (spiral, comminuted, long oblique greater than twice the diameter) are better treated with submuscular plating or rigid nailing to avoid loss of reduction.
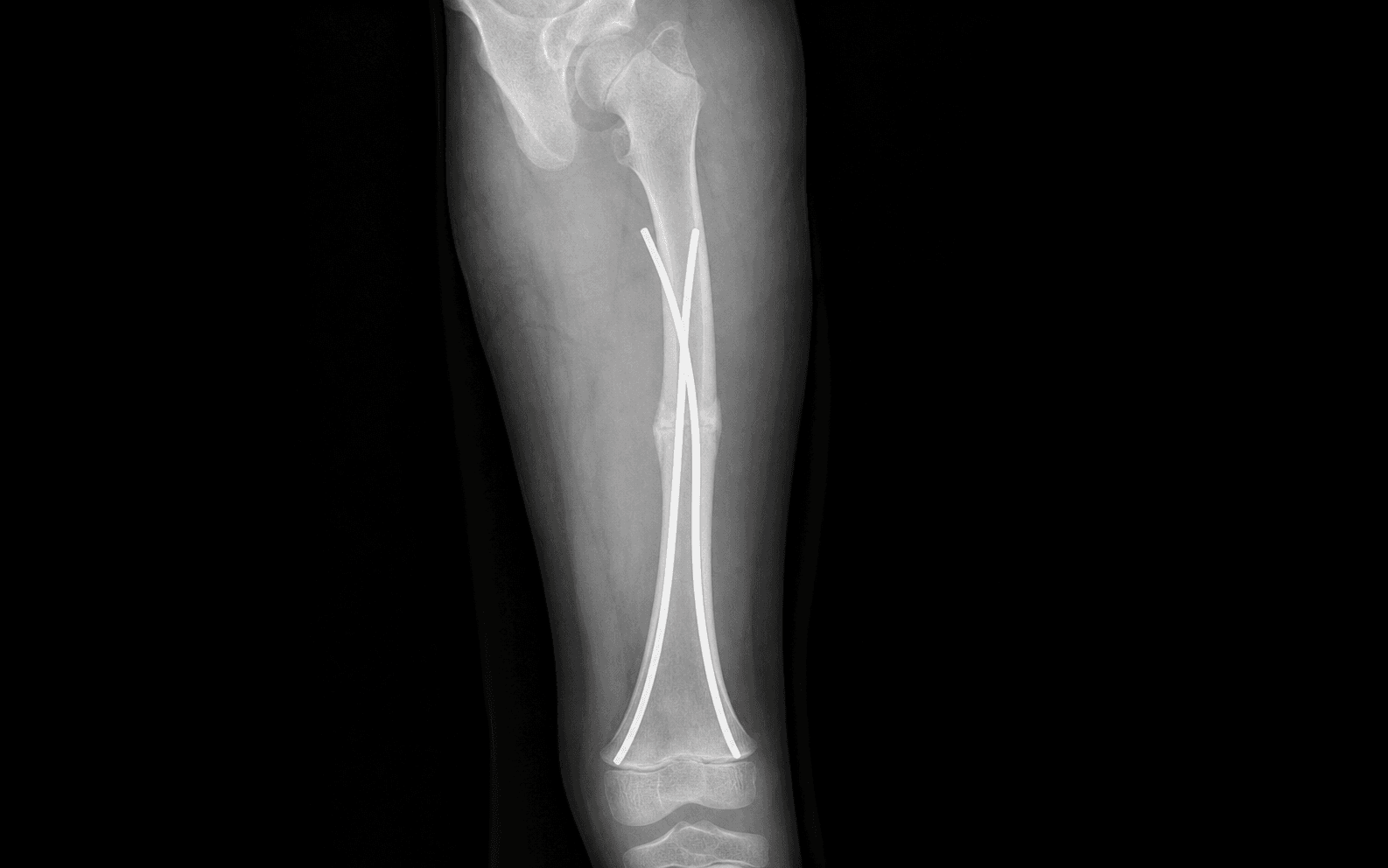
- Two pre-bent titanium elastic nails are inserted retrograde from separate medial and lateral distal metaphyseal entry points distal to the distal femoral physis. Each nail should occupy 30 to 40 percent of the canal diameter and be pre-bent to three times the canal diameter to create balanced three-point fixation.
- The nails must not cross the distal femoral physis. Entry points are placed in the metaphysis 1.5 to 2 cm proximal to the physis on the medial and lateral sides. The nails are advanced past the fracture into the proximal fragment to the level of the greater trochanter or femoral neck junction.
- End caps are used on the nail ends in length-unstable patterns or when early weight bearing is planned. Nail-end irritation and bursitis at the knee are the most common complications requiring reoperation for nail trimming or removal.
When & Why
Indication. A displaced, closed paediatric femoral shaft fracture in a child typically 5 to 11 years old weighing less than 50 kg that is length-stable (transverse or short-oblique midshaft) and either has unacceptable alignment after a trial of closed reduction and spica casting or is unsuitable for casting. Flexible intramedullary nailing lets the child mobilise early, avoids the morbidity of a prolonged spica, and has a union rate greater than 95 percent when the patient is correctly selected. Children less than 5 years, or stable patterns that reduce acceptably, are still managed in a spica. Acceptable alignment after closed reduction (spica is reasonable up to these limits): less than 10 degrees varus/valgus, less than 15 degrees anterior or posterior angulation, and less than 1.5 cm shortening. Beyond these, or when casting would compromise care, fix it. Assess the whole child and the whole fracture before committing. Flexible nailing only works when the fracture is length-stable. Exclude or plan for:
- Length-unstable patterns — spiral, comminuted, or long-oblique fractures where the obliquity is greater than twice the femoral diameter, or comminution involves greater than 50 percent of the circumference. These shorten and angulate under flexible nails and need submuscular plating or a rigid nail.
- Older or heavier children — above 11 years or 50 kg the complication rate (malunion, nail breakage) rises sharply; many centres default to submuscular plating or a lateral-entry rigid nail.
- Open physes with very proximal or distal fractures where nail trajectory risks physeal violation, pathological fractures through a cyst or tumour (biopsy plus alternative fixation), and active infection at the planned entry sites. Contraindicated in length-unstable patterns, in children older than 11 years or heavier than 50 kg (relative — higher failure rates), in active entry-site infection, and in pre-existing neuromuscular conditions with a high risk of nail migration (for example severe spasticity). The one decision that matters. Every flexible nail job is built on the same idea — two retrograde pre-bent nails creating opposing three-point fixation. The choice is really which fixation strategy fits the child and the pattern:
Length-stable transverse or short-oblique midshaft fractures in 5 to 11 year olds weighing less than 50 kg. Closed, percutaneous, elastic splinting; protected weight bearing.
Any age and any pattern — the bridge for length-unstable, comminuted, or older and heavier children. Length-stable (bridge) plating allows immediate weight bearing and a lower malunion rate.
Children older than 11 years and heavier than 50 kg. A rigid, lateral-entry nail avoids the proximal femoral physis and the avascular-necrosis risk of a piriformis-entry nail.
Consent specifically for the 15 to 25 percent risk of nail-end irritation or bursitis at the knee (the commonest reason to return to theatre for trimming or early removal), the planned second procedure to remove the nails at 6 to 12 months, a small risk of malunion or leg-length discrepancy, and (in length-unstable patterns treated against the grain) loss of reduction. Setup. Supine on a radiolucent fracture table or flat-top table, the injured leg prepared free or placed in traction with the contralateral leg abducted or scissored for circumferential fluoroscopic access; a small bump under the ipsilateral buttock neutralises external rotation. C-arm on the contralateral side — confirm true AP and lateral of the hip, fracture and knee are all obtainable without moving the limb, and that both entry points are visible on the same AP view before you incise. General anaesthesia with muscle relaxation for closed reduction; a femoral or fascia-iliaca block may be added for postoperative analgesia but does not replace the general. Apply longitudinal traction with the hip flexed 20 to 30 degrees and slight abduction; for shortening greater than 2 cm use 5 to 10 minutes of sustained traction or a fracture table. Judge rotation from the profile of the lesser trochanter on the AP view, compared with the contralateral side.
The Operation
The goal: reduce the fracture closed, expose the distal femur through two small metaphyseal entry incisions that stay clear of the distal femoral physis, pass two pre-bent titanium elastic nails retrograde across the fracture to create opposing three-point fixation, and stabilise the child in near-anatomic alignment so they can mobilise. The exposure is laid out in full as the opening steps below.
Operative sequence
- Confirm the pattern is length-stable on fluoroscopy, then reduce with traction, abduction and rotation. Do not proceed with nailing if anatomic reduction cannot be achieved.
- If reduction will not hold with traction alone, make a small 2 cm medial incision at the fracture level, pass a pointed reduction clamp, and hold reduction while the first nail is passed — it is far easier than reducing around nails already in the canal.
- Check the rotational profile against the contralateral limb using the lesser trochanter on the AP view.
- The distal femoral physis is the most active growth plate in the lower limb, contributing 70 percent of femoral length and 40 percent of lower-limb length. It lies at the level of the adductor tubercle medially and about 1 cm proximal to the superior pole of the patella laterally (knee flexed 90 degrees).
- Mark two entry points in the metaphyseal flare, each 1.5 to 2 cm proximal to the physis: medial entry 1.5 cm proximal to the adductor tubercle; lateral entry 1.5 cm proximal to the superior pole of the patella.
- Confirm both points sit at the same level on a true AP view before incising. The medial metaphysis is narrower; the lateral metaphysis gives a wider safe corridor.
- Make 2 to 3 cm longitudinal incisions over the medial and lateral distal metaphysis. Incise the fascia and split the muscle fibres down to bone.
- Medial interval — between vastus medialis (anterior) and sartorius/adductor (posterior); it is relatively avascular, but the saphenous nerve and vein cross superficially here — identify and protect them.
- Lateral interval — through the iliotibial band and vastus lateralis, using the lateral supracondylar ridge as a palpable landmark. The femoral artery and vein lie anteromedial, protected by vastus medialis; the sciatic nerve is posterior, protected by the hamstrings.
- Create each entry hole with a 3.2 mm drill or awl, directed proximally at 30 to 40 degrees to the long axis and slightly anterior, with the two holes about 1 cm apart in the sagittal plane to avoid nail collision. Enlarge each with a curved awl or small rongeur.
- Measure the canal at the isthmus (at the junction of the proximal and middle thirds; typically 8 to 12 mm in a 6 to 10 year old). Choose two equal-diameter titanium elastic nails, each 30 to 40 percent of the canal diameter (together 60 to 80 percent canal fill).
- Pre-bend both nails to three times the canal diameter with a smooth, symmetric bend in the same plane, the apex of the bend sited to lie at the fracture level when the nail is fully seated.
- Load the medial nail and advance it by hand or with gentle mallet taps through the entry, across the fracture and into the proximal fragment. It should slide easily — resistance means wrong trajectory or incomplete reduction.
- Rotate the nail so the apex of the bend faces the opposite cortex at the fracture site. Advance until the tip reaches the greater trochanter or femoral neck junction on the AP view, and confirm on the lateral view that it has not perforated the proximal anterior cortex.
- Pass the lateral nail through its separate entry using the same technique. The two nails should cross at the fracture site in opposite directions, creating balanced opposing three-point fixation — each nail contacts the cortex at three points (the entry cortex, the opposite cortex at the apex of the bend, and the far cortex beyond the fracture).
- Confirm on AP and lateral fluoroscopy that both nails have reached the proximal metaphysis without crossing the physis or perforating the cortex. Unequal nail diameters or asymmetric bends produce malalignment.
- In length-unstable patterns, or whenever early weight bearing is planned, apply end caps to both nail ends. The caps screw onto the threaded tips and seat against the metaphyseal cortex, preventing shortening.
- Obtain full-length AP and lateral films. Acceptable alignment: less than 5 degrees varus/valgus, less than 10 degrees anterior or posterior angulation, less than 5 degrees rotation, and less than 1 cm shortening. If alignment is unacceptable, remove one nail, re-reduce and re-insert.
- Trim the nail ends flush with the metaphyseal cortex, or leave 5 mm proud when using end caps. Close the fascia and skin in layers. Apply a light dressing and a knee immobiliser or long-leg cast for comfort in younger children.
Never place an entry distal to the physis and never drive a nail across it — a physeal violation causes growth arrest or angular deformity that may not appear for months. Confirm both entry points are 1.5 to 2 cm proximal to the physis and the nail tips stay clear of it on true AP and lateral before advancing past the fracture. On the medial side, identify and protect the superficial saphenous nerve and vein; the femoral vessels anteromedially are shielded by vastus medialis. Start each entry hole at 30 to 40 degrees and slightly anterior — an eccentric trajectory risks iatrogenic fracture or posterior cortex breach.
Obtain a perfect AP and lateral of the reduced fracture before making any incisions. If reduction will not hold with traction alone, make a small 2 cm medial incision at the fracture level, pass a pointed reduction clamp, and hold reduction while the first nail is passed. This prevents the frustration of trying to reduce the fracture around nails already inserted.
Pre-bending each nail to three times the canal diameter creates the elastic recoil force that maintains reduction through three-point cortical contact — the entry cortex, the opposite cortex at the apex of the bend, and the far cortex beyond the fracture. Two equal nails pre-bent symmetrically and crossing in opposite directions give balanced control of varus/valgus and flexion/extension. Insufficient bend, unequal diameters, or asymmetric bends all lead to loss of reduction.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation & weight bearing | Activity | |-------|--------|----------------------------------|----------| | Early | 0 to 2 weeks | Knee immobiliser or long-leg cast for comfort (under 8 years); removable brace in older children. Touch-down weight bearing for stable fractures; non- or partial weight bearing for unstable patterns until callus (3 to 4 weeks) | Finger and ankle motion; wound dry for 10 to 14 days; sutures out at 12 to 14 days | | Rehabilitation | 2 to 8 weeks | Removable splint; progressive weight bearing as callus forms (usually 4 to 6 weeks) | Active knee and hip range of motion from week 2; physiotherapy for gait and strengthening; full weight bearing by 6 to 8 weeks in stable fractures | | Return to activity | 8 weeks onward | — | Return to school at 2 to 4 weeks; sports at 3 to 6 months once radiographically united and strong | Nail removal is elective at 6 to 12 months once bridging callus is mature and remodelling has begun — earlier removal (before 6 months) risks refracture, and later removal (after 18 months) gets technically harder as bone overgrows the nail ends. Remove earlier if the nails are symptomatic; trimming a prominent end is a valid interim option. Complications
- Incidence
- 15 to 25 percent
- Recognition
- Pain and swelling over the medial or lateral femoral condyle at 4 to 8 weeks; palpable prominent nail end; skin breakdown if severe
- Prevention and management
- Prevention: trim nails flush or use end caps and counsel families pre-operatively. Management: early nail trimming under local or general anaesthesia; definitive removal at 6 to 12 months once union is solid
- Incidence
- 5 to 10 percent
- Recognition
- Clinical deformity at 6 to 8 weeks; radiographic angulation on full-length films; limb-length inequality
- Prevention and management
- Prevention: strict length-stable fracture selection; adequate pre-bend; balanced medial and lateral nails. Management: observation if asymptomatic; corrective osteotomy if greater than 15 degrees or symptomatic at skeletal maturity
- Incidence
- Less than 5 percent
- Recognition
- Measured on full-length standing radiographs at 6 months and 1 year; scanogram for precision
- Prevention and management
- Prevention: equal-diameter nails and symmetric pre-bend; avoid physeal injury. Management: shoe lift for 1 to 2 cm; epiphysiodesis of the contralateral distal femur if projected greater than 2 cm at maturity
- Incidence
- Greater than 20 percent in length-unstable fractures without end caps
- Recognition
- Radiographic shortening or angulation at the first post-operative visit; clinical limp and asymmetry
- Prevention and management
- Prevention: end caps in unstable patterns; supplemental cast or external fixation for 4 to 6 weeks. Management: revision to a submuscular plate or addition of an external fixator if recognised early
- Incidence
- Less than 2 percent
- Recognition
- New fracture line at the entry point on post-operative films; pain and crepitus at the incision
- Prevention and management
- Prevention: enlarge the entry hole adequately; start at 30 to 40 degrees; never hammer against resistance. Management: protected weight bearing or cast if nondisplaced; revision fixation if displaced
- Incidence
- Less than 1 percent
- Recognition
- Erythema, drainage or sinus at the entry site; raised CRP; positive cultures
- Prevention and management
- Prevention: sterile technique; prophylactic antibiotics; meticulous haemostasis. Management: superficial — oral antibiotics and local care; deep — debridement, retain the nail until union, then remove with intravenous antibiotics
- Incidence
- Rare (less than 1 percent)
- Recognition
- Progressive nail extrusion on serial radiographs; acute pain with activity
- Prevention and management
- Prevention: adequate canal fill; correct pre-bend; timely removal at 6 to 12 months. Management: revision nailing or conversion to a plate; remove broken fragments if symptomatic
Length-unstable fractures (spiral, comminuted, long-oblique greater than twice the diameter) shorten and angulate under flexible nails alone — the risk of loss of reduction is up to 30 percent. If you discover instability intra-operatively, either add end caps and protect with a cast or external fixator, or convert to a submuscular plate. Have plating implants available for every paediatric femur case planned for nailing.
Viva & Exam Focus
NAILSNAILS — nail selection and pre-bending principles
FEMURFEMUR — pattern, fixation choice and removal
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 7-year-old boy weighing 28 kg sustains a closed transverse midshaft femoral fracture after a fall from a climbing frame. The fracture is length-stable with 1.5 cm shortening and 15 degrees varus. How do you decide between flexible intramedullary nailing and spica casting?”
“You are planning flexible nailing on a 9-year-old girl with a short-oblique femoral shaft fracture. Intra-operatively you discover the fracture is actually long-oblique with a small butterfly fragment, making it length-unstable. What do you do?”
“A 10-year-old boy (48 kg) with a transverse femoral shaft fracture undergoes flexible nailing. At 4 months the fracture has united but he has persistent pain over the medial femoral condyle with a prominent nail end. How do you manage this, and when do you remove the nails?”
Indications — strict criteria
- Age 5 to 11 years, weight less than 50 kg
- Length-stable transverse or short-oblique midshaft fractures only
- Length-unstable (spiral, comminuted, long-oblique greater than twice the diameter) means submuscular plating or a rigid nail
- Greater than 10 degrees varus/valgus, greater than 15 degrees AP angulation, or greater than 1.5 cm shortening after closed reduction is a surgical indication
Surgical anatomy — entry points and physis
- Distal femoral physis at the adductor tubercle medially and 1 cm proximal to the patella laterally
- Entry points 1.5 to 2 cm proximal to the physis in the metaphyseal flare
- Medial and lateral entries must be at the same level on true AP fluoroscopy
- Canal diameter at the isthmus typically 8 to 12 mm; each nail 30 to 40 percent of the diameter
Implant principles — three-point fixation
- Two equal-diameter titanium elastic nails pre-bent to three times the canal diameter
- Apex of the bend at the fracture level when fully seated
- Balanced medial and lateral nails create opposing three-point fixation
- End caps are mandatory for length-unstable patterns or early weight bearing
Operative sequence
- 1. Closed reduction confirmed anatomic on AP and lateral
- 2. Mark entry points 1.5 to 2 cm proximal to the physis under fluoroscopy
- 3. Create metaphyseal entry holes directed 30 to 40 degrees proximally
- 4. Pre-bend symmetrically; insert the medial nail first
- 5. Advance each nail to the proximal metaphysis (greater-trochanter level)
- 6. Apply end caps if indicated; trim ends flush or slightly proud
- 7. Final full-length radiographs before closure
Complications — anticipate and prevent
- Nail-end irritation or bursitis: 15 to 25 percent — trim or remove early
- Malunion greater than 10 degrees: 5 to 10 percent — strict length-stable selection
- Leg-length discrepancy greater than 1 cm: less than 5 percent — equal nails and symmetric bend
- Loss of reduction in unstable fractures: 20 to 30 percent without end caps — convert to a plate or add end caps plus immobilisation
Post-operative care
- Touch-down weight bearing progressing to full by 6 to 8 weeks in stable fractures
- Knee immobiliser or cast for comfort in younger children
- Nail removal elective at 6 to 12 months once remodelling is evident
- Earlier removal if symptomatic; trimming is a valid interim option
Borderline patients (10 to 12 years or 45 to 55 kg)
- Higher complication rates with flexible nailing
- Consider submuscular plating for any unstable pattern or heavier child
- Lateral-entry rigid nail is an alternative above 11 years and 50 kg
- Document the decision and counsel the family about increased risk
Evidence thresholds
- Union greater than 95 percent in length-stable fractures with correct technique
- Malunion risk rises sharply above 11 years or 50 kg
- End caps reduce shortening in unstable patterns (Luhmann 2005)
- Submuscular plating has lower malunion and irritation rates in unstable fractures (Sink 2012)
Background & Evidence
How the implant works. Each pre-bent nail contacts the cortex at three points — the entry cortex, the opposite cortex at the apex of the bend (fracture level), and the far cortex proximal or distal to the fracture. The elastic recoil of the pre-bent titanium creates continuous compression across the fracture, and balanced medial and lateral nails counteract varus/valgus and flexion/extension forces. The femoral isthmus (the narrowest point, at the junction of the proximal and middle thirds) governs nail diameter: at 8 to 12 mm in the target age group, a nail of 30 to 40 percent of that diameter is chosen. The canal widens distally into the metaphysis, which is what allows two divergent nails to be inserted without cortical perforation. Selection thresholds. The age and weight criteria are evidence-based, not arbitrary: the multicentre series of Moroz and colleagues identified 11 years and 50 kg as the inflection points, with children above these having 4.3 times higher odds of a poor outcome. Length-stable fractures are the key eligibility test — long-oblique and comminuted patterns shorten under elastic nails, and end caps only partly mitigate this.
- Flexible IM nailing
- 5 to 11 years, less than 50 kg
- Submuscular plating
- Any age or weight
- Rigid IM nailing
- Greater than 11 years, greater than 50 kg
- Spica casting
- Less than 5 years or stable patterns
- Flexible IM nailing
- Length-stable only
- Submuscular plating
- Any pattern
- Rigid IM nailing
- Any pattern
- Spica casting
- Length-stable, acceptable reduction
- Flexible IM nailing
- Greater than 95 percent
- Submuscular plating
- Greater than 98 percent
- Rigid IM nailing
- Greater than 95 percent
- Spica casting
- Greater than 90 percent (selected)
- Flexible IM nailing
- 5 to 10 percent (angulation)
- Submuscular plating
- Less than 3 percent
- Rigid IM nailing
- Less than 5 percent
- Spica casting
- 10 to 20 percent (shortening or angulation)
- Flexible IM nailing
- Less than 5 percent greater than 1 cm
- Submuscular plating
- Less than 3 percent
- Rigid IM nailing
- Less than 3 percent
- Spica casting
- 5 to 15 percent
- Flexible IM nailing
- Elective 6 to 12 months
- Submuscular plating
- Optional 12 months
- Rigid IM nailing
- Optional after maturity
- Spica casting
- Not applicable
- Flexible IM nailing
- Yes (protected)
- Submuscular plating
- Yes (immediate)
- Rigid IM nailing
- Yes (immediate)
- Spica casting
- No (6 to 12 weeks cast)
Outcomes. In properly selected length-stable fractures, union exceeds 95 percent, with radiographic union at 6 to 10 weeks in children under 10 and return to protected full weight bearing by 4 to 8 weeks. Leg-length discrepancy greater than 1 cm occurs in less than 5 percent when the nails are of equal diameter and symmetrically pre-bent. The dominant complication is nail-end irritation (15 to 25 percent), reflecting the prominence of the nail tips at the knee rather than a failure of fixation.
References
Titanium elastic nailing of femoral shaft fractures in children
- Retrospective review of 58 children treated with titanium elastic nails
- 97 percent excellent or good results using Flynn criteria when length-stable fractures were selected
- Complication rate 21 percent, predominantly nail-end irritation requiring trimming or removal
Comparison of flexible intramedullary nailing versus submuscular plating for paediatric femoral shaft fractures
- Prospective comparison of 43 flexible-nail and 38 submuscular-plate patients
- Flexible nails had a higher rate of malunion (12 percent versus 3 percent) and nail irritation (19 percent)
- Submuscular plating allowed immediate full weight bearing and an earlier return to activity
Complications of titanium elastic nailing in paediatric femoral fractures
- Review of 78 children; overall complication rate 26 percent
- Nail-end irritation or bursitis occurred in 18 percent and was the most common reason for reoperation
- Malunion greater than 10 degrees occurred in 8 percent, predominantly in length-unstable fractures treated without end caps
End caps improve stability in length-unstable paediatric femoral fractures treated with flexible nails
- Retrospective series comparing nails with and without end caps in unstable fracture patterns
- End-cap group had significantly less shortening (mean 3 mm versus 12 mm) and a lower reoperation rate
- End caps add 5 to 7 minutes of operative time but reduce loss-of-reduction complications
Age and weight as predictors of outcome after flexible nailing of femoral shaft fractures
- Multicentre review of 234 children; 11 years and 50 kg identified as inflection points
- Children older than 11 years or heavier than 50 kg had 4.3 times higher odds of a poor outcome
- The authors recommend submuscular plating or rigid nailing for patients above these thresholds