Stem stability drives treatment: ORIF for a well-fixed stem, revision for a loose one · trauma · advanced
- The Vancouver classification is the framework for fractures around a hip stem and it directly drives treatment. Type A = trochanteric (AG greater trochanter, AL lesser trochanter); Type B = around or just below the stem tip; Type C = well distal to the stem tip. The single most important variable within Type B is STEM STABILITY.
- B1 = stem WELL-FIXED, treat with ORIF (locking plate spanning the femur, combination of locking/cortical screws and cerclage cables around the stem, +/- cortical strut allograft). B2 = stem LOOSE with adequate bone, treat with REVISION to a long uncemented tapered fluted stem bypassing the fracture +/- ORIF. B3 = stem loose with DEFICIENT bone stock, treat with revision + bone graft/allograft-prosthetic composite, or proximal femoral replacement in the frail elderly.
- The exam-defining trap is misclassifying a LOOSE stem as B1 and plating it. Assess stability with the history (pre-injury thigh/start-up pain), serial radiographs (subsidence, radiolucent lines, cement-mantle fracture, debonding), and if any doubt TEST the stem intra-operatively. A plated loose stem fails.
- Type C fractures are treated as a fracture in their own right with a locking plate, but the plate MUST overlap the stem proximally so there is no unsupported segment of bone between the plate and the stem tip — an inter-implant stress riser is a classic cause of refracture.
- “Always state your reasoning out loud: 'I classify by fracture location AND stem stability — the two together define the Vancouver type and the operation.' Examiners want B1 vs B2 distinguished before any mention of implants.
- “Pre-injury thigh pain or start-up pain is a red flag for a loose stem — it reclassifies an apparent B1 to a B2 and changes the operation from plate to revision.
- “Span the WHOLE femur and overlap implants. Whether plating a B1 or a Type C, avoid leaving a short rigid segment or an open span between implants — both create stress risers and refracture.
- “Periprosthetic fracture mortality approaches that of a native hip fracture (about 10% at 1 year, higher in the frail). Treat these as fragility-fracture-equivalent: orthogeriatric co-care, early surgery, early weight-bearing.
When & Why
The problem. A periprosthetic femoral fracture around a hip stem is a fracture in bone that already carries an implant, so the operation must respect BOTH the broken bone AND the stem that sits in it. The Vancouver classification (Duncan and Masri) is the universally adopted framework precisely because it is treatment-directing: it combines three factors — the site of the fracture, the stability of the stem, and the quality of the bone stock — and each combination maps to a defined operation. The whole game is one question. Once a fracture is localised to the stem-tip region (Type B), the only thing that matters is whether the stem is well-fixed (B1) or loose (B2/B3) — because that single distinction decides whether you plate the bone and leave the stem, or revise the stem. Everything below serves that decision. Assessing stem stability — the crux. Interrogate stability BEFORE you choose an implant: - History: pre-injury thigh pain or start-up pain is the classic clue to a pre-existing loose stem — it can reclassify an apparent B1 to a B2.
- Radiographs: full-length femur films (AP and lateral) including the joint above (hip) and below (knee). Signs of loosening are subsidence/migration, complete radiolucent lines at the bone-cement or bone-implant interface, cement-mantle fracture, debonding, pedestal formation and varus tilt. Compare with the immediate post-operative film for migration.
- Intra-operative test: when stability is still uncertain after history and imaging, expose and test the stem directly. If it is loose, convert to a revision (B2/B3). Plating a stem that is in fact loose is the principal avoidable error.
- Stem
- Well-fixed
- Bone
- Often lytic
- Operation
- Usually non-operative; fix if abductors threatened
- Key Principle
- Investigate underlying osteolysis
- Stem
- Well-fixed
- Bone
- Adequate
- Operation
- ORIF — locking plate + cables +/- strut
- Key Principle
- Fix the fracture, keep the stem; span the femur
- Stem
- Loose
- Bone
- Adequate
- Operation
- Revision to long uncemented tapered fluted stem (+/- ORIF)
- Key Principle
- Bypass fracture by 2 cortical diameters; gain distal fixation
- Stem
- Loose
- Bone
- Deficient
- Operation
- Long stem + graft / APC, or proximal femoral replacement
- Key Principle
- Restore stock (young) or replace (frail elderly)
- Stem
- Irrelevant to fracture
- Bone
- Variable
- Operation
- ORIF — locking plate
- Key Principle
- Overlap the stem; no inter-implant stress riser
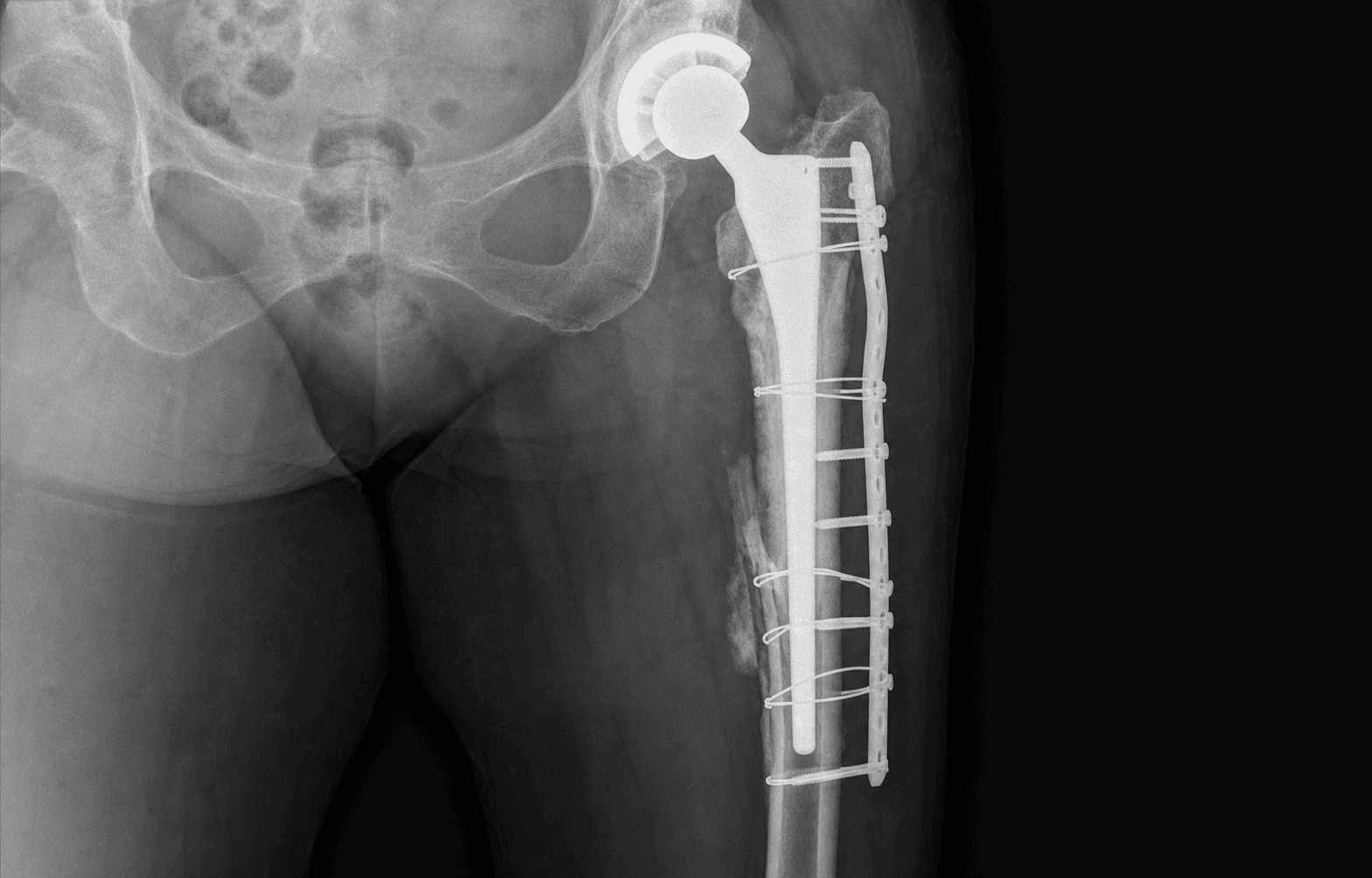
Well-fixed stem, adequate bone. A long locking plate spanning the femur, cerclage cables and unicortical locking screws proximally around the stem and bicortical screws distally, +/- a cortical strut. Fix the fracture and leave the stem undisturbed.
Loose stem, adequate bone. A long uncemented tapered fluted stem bypasses the fracture and gains distal diaphyseal fixation, +/- ORIF, often through an extended trochanteric osteotomy. The revision stem both solves the loosening and internally splints the fracture.
Loose stem, deficient bone. Younger patient: long stem + bone graft / impaction grafting / allograft-prosthetic composite to restore stock. Frail elderly: proximal femoral replacement (megaprosthesis) to allow immediate weight-bearing.
Pre-operative preparation (all types). - Work-up: full-length femur radiographs (hip and knee included); CT if intra-articular extension, bone-loss assessment or stem-tip detail is needed. Identify the implant (stem make and taper, cemented vs uncemented, head size) and obtain the previous operation note if revision is possible.
- Exclude infection: a periprosthetic fracture can be the presentation of an infected loose stem — check CRP/ESR and aspirate if indicated before any reconstruction.
- Medical optimisation: orthogeriatric review, anticoagulation management, group-and-save/crossmatch (revision can be high-blood-loss), anaesthetic assessment. Aim for early surgery on a planned list with the right implants and revision trays available. The frailty lens. Because mortality approaches that of a native hip fracture, the construct should ideally permit early weight-bearing. A megaprosthesis or a stable long-stem revision allows this; a tenuous plate fixation in poor bone that demands prolonged restricted weight-bearing is often the wrong answer in a frail patient even when it is technically possible.
Location tells me A, B or C. For a B fracture, stem stability splits B1 from B2/B3, and bone stock splits B2 from B3. Only then do I choose an implant. In the elderly I also weight the decision toward whatever lets the patient stand the next day. I would rather open and check the stem than commit to a plate on an uncertain stem.
- Calling a fracture B1 without rigorously excluding a loose stem — this is the highest-yield error.
- Ignoring pre-injury thigh/start-up pain in the history.
- Not obtaining full-length femur films — missing a second fracture, the stem tip, or a distal implant.
- Forgetting bone stock — a loose stem in deficient bone is B3, not B2, and needs a different reconstruction.
The Operation
The goal: classify the fracture, expose the femur through an approach that gives controlled access to the canal, confirm stem stability on the table, then execute the operation dictated by the Vancouver type — ORIF around a well-fixed stem, or revision with a stem that bypasses the fracture. The exposure is the heart of the case and is laid out as the first operative steps below.
Operative sequence
- Lateral position for a hip/posterior-femoral approach (or supine for an isolated Type C distal femur), on a radiolucent table that allows full-length imaging.
- Confirm the implant and have revision trays, cement-removal instruments, cerclage cables, locking plates and cortical struts available before you cut — running out mid-case is how an ETO or a loose stem becomes a crisis.
- Wide prep and drape for possible proximal femoral replacement if bone stock is poor.
- For a B fracture around the stem, use a posterior (Moore/Southern) or lateral approach to the hip and proximal femur over the fracture (see posterior approach to the hip and posterolateral approach to the femur).
- For a B2 revision, plan an extended trochanteric osteotomy (ETO) — a longitudinal osteotomy of the lateral femoral cortex including the greater trochanter — to gain controlled access to the canal and cement while preserving abductor continuity for later cable repair. The ETO is the workhorse exposure for removing a well-cemented or distally fixed stem.
- Preserve the soft-tissue envelope and blood supply: use indirect/biological reduction and avoid stripping the fracture fragments, which devascularises bone and causes nonunion.
- With the fracture exposed, test the stem directly. This is the branch point of the whole operation.
- If the stem is well-fixed, proceed to ORIF (B1 pathway).
- If the stem is loose, abandon ORIF and proceed to revision (B2/B3 pathway).
- Plating a stem that is in fact loose is the archetypal avoidable error — this step exists to prevent it.
- Reduce the fracture with cables and clamps using biological technique; restore length, alignment and rotation. Bridging fixation is appropriate for comminuted patterns.
- Apply a long lateral locking plate spanning the whole femur, from the trochanteric region to the distal metaphysis, so you do not swap one stress riser for another at a plate end.
- Use a combination construct: proximally, where the stem fills the canal, use cerclage cables and unicortical locking screws (plus screws angled around the stem); distally use bicortical screws.
- Consider an anterior cortical strut allograft as an onlay to augment fixation in poor bone or to add a second plane of fixation.
- Complete the ETO if needed, and extract the loose stem; remove all cement and the cement restrictor if cemented, and debride and prepare the canal.
- Insert a long uncemented tapered fluted titanium stem that bypasses the fracture by at least about two cortical diameters and gains rotational and axial fixation in the diaphysis distal to the fracture. Modular designs let you set length, version and offset independently.
- Reduce the fracture around the stem with cerclage cables; add a plate or strut only if the fracture pattern still demands it (B2 +/- ORIF).
- The revision stem is the key implant — it bypasses the fracture AND solves the loosening.
- Younger, higher-demand patient with restorable stock: long revision stem with bone graft / impaction grafting / allograft-prosthetic composite (APC) to rebuild proximal bone.
- Frail elderly patient: proximal femoral replacement (megaprosthesis) — it sacrifices stock but allows immediate weight-bearing, prioritising rapid mobilisation and survival over bone preservation.
- Address instability risk after major proximal reconstruction — consider a dual-mobility or constrained articulation given the soft-tissue compromise.
- Treat as an ordinary distal/diaphyseal femoral fracture with a distal femoral locking plate (or a retrograde nail where geometry allows and no knee implant interferes).
- Crucially, overlap the plate with the stem proximally — cables and unicortical or locking screws around the stem — so there is no unsupported segment between the plate and the stem tip. An open inter-implant span is a classic stress riser and a cause of refracture.
- Reattach the ETO / greater trochanter with cables or a claw to restore the abductor lever arm; secure trochanteric fixation protects abductor function.
- Layered closure over drains as needed; confirm stability and perfusion.
- Obtain intra-operative imaging to confirm reduction, stem position, plate length and implant overlap before leaving theatre.
Proximally I cannot get bicortical purchase past the stem, so I use a mix of cerclage cables and unicortical locking screws, plus screws that pass around the stem. Distally I get good bicortical fixation. The plate spans the whole femur so I am not creating a new stress riser at a plate end.
The revision stem is the key implant — it bypasses the fracture and obtains distal diaphyseal fixation, which both fixes the loosening and internally splints the fracture. Cerclage cables reduce the proximal fragments around it; I add a plate or strut only if the fracture still needs it.
- Plating a stem that is actually loose (missed B2) — the commonest cause of failure.
- A short plate that creates a new stress riser at its end.
- Over-stripping fracture fragments and devascularising the bone (nonunion).
- Inadequate proximal fixation around the stem — balance cables, unicortical locking screws and strut.
- Inadequate distal fixation — the tapered stem must engage sound diaphyseal bone past the fracture.
- Iatrogenic perforation or further fracture during stem/cement removal — a controlled ETO helps avoid this.
- Failure to reattach the abductor/trochanter securely.
- Under-recognised B3 — if proximal bone is deficient, switch to a graft/APC or replacement plan.
Aftercare & Complications
Rehabilitation — the goal is early, safe weight-bearing. Prolonged non-weight-bearing is poorly tolerated and dangerous in the elderly, so the construct should ideally allow it: - Revision to a stable long stem and a proximal/distal femoral replacement generally permit early or immediate weight-bearing.
- ORIF weight-bearing depends on fracture pattern, bone quality and construct strength — progress under radiographic guidance. A tenuous fixation in poor bone is a reason to reconsider the strategy, not to impose long restriction. Multidisciplinary pathway. - Orthogeriatric co-management throughout admission; VTE prophylaxis; delirium prevention; nutrition and bone-health optimisation (treat the underlying osteoporosis).
- Physiotherapy from day 1; occupational therapy and discharge planning early.
- Follow-up: serial radiographs to confirm union/stability and exclude implant migration or inter-implant refracture; monitor for late infection and instability after revision. A periprosthetic fragility fracture is a sentinel event — refer to a bone-health clinic and address falls prevention, because many of these patients fall again.
- Context
- Plated B2 (loose stem treated as B1)
- Recognition
- Early loss of fixation, persistent pain, stem migration on serial films
- Prevention and Management
- Prevention: rigorously assess stem stability (history, radiographs, intra-operative test) before plating. Management: revision to a long-stem reconstruction (the operation that should have been done)
- Context
- ORIF, especially with devascularised fragments or poor bone
- Recognition
- Persistent pain and absence of bridging callus beyond expected time; hardware loosening
- Prevention and Management
- Prevention: biological reduction, span the femur, augment with strut/graft. Management: revision fixation +/- bone graft; consider revision to a long stem if implant-related
- Context
- Frail comorbid host; long operations
- Recognition
- Wound issues, raised CRP/ESR, pain; aspiration positive
- Prevention and Management
- Prevention: optimise host, prophylactic antibiotics, exclude pre-existing infection (the fracture may be the presentation of an infected loose stem). Management: DAIR vs staged revision per duration/organism
- Context
- Short plate, gap between plate and stem, or between hip and knee implants
- Recognition
- New fracture between or at the end of implants after a further fall
- Prevention and Management
- Prevention: span the whole femur and OVERLAP implants — never leave an unsupported segment. Management: revision with a spanning construct that bridges both implants
- Context
- ORIF under high cyclical load, delayed union
- Recognition
- Hardware breakage on radiographs, recurrence of pain/deformity
- Prevention and Management
- Prevention: adequate-length locking construct, combination fixation around the stem, biological technique. Management: revision fixation +/- graft, or revision arthroplasty
- Context
- Major proximal reconstruction / proximal femoral replacement
- Recognition
- Recurrent dislocation; abductor insufficiency
- Prevention and Management
- Prevention: dual-mobility or constrained liner where soft tissues are compromised; secure abductor/trochanter reattachment. Management: closed reduction; revise to constrained/dual-mobility if recurrent
- Context
- Elderly, comorbid, anticoagulated host
- Recognition
- VTE, chest infection, delirium, decompensation of comorbidity
- Prevention and Management
- Prevention: orthogeriatric co-care, early surgery, VTE prophylaxis, early mobilisation. Management: multidisciplinary medical management; 1-year mortality approaches that of native hip fracture
- Context
- After ETO or trochanteric fixation
- Recognition
- Lurch, abductor weakness, proximal cable/wire migration
- Prevention and Management
- Prevention: secure cable/claw reattachment, protect abductor pull early. Management: revision trochanteric fixation if symptomatic
Viva & Exam Focus
VANCOUVERVANCOUVER — classifying the hip-stem fracture
STABLESTABLE — is the stem loose?
Systematic assessment of stem stability before choosing ORIF versus revision
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“An 82-year-old woman falls and sustains a femoral fracture around the tip of a 9-year-old cemented total hip stem. The radiograph shows a spiral fracture at the stem tip. How do you classify and manage this?”
“What is the single most important determinant of treatment in a Vancouver B fracture, and why does getting it wrong matter so much?”
“A 70-year-old man with a long-standing total knee replacement falls and sustains a fracture of the distal femur just above the femoral component. He also has a hip replacement on the same side. Talk me through your assessment and management.”
The Vancouver Classification
- Type A = trochanteric: AG greater trochanter, AL lesser trochanter — usually non-operative, often lytic
- Type B = around / just distal to the stem tip — the decisive zone; sub-typed by stem stability and bone
- B1 = stem well-fixed; B2 = stem loose, good bone; B3 = stem loose, deficient bone
- Type C = well distal to the stem tip — treat as an ordinary fracture but overlap the stem
- Combines fracture site + stem stability + bone stock = treatment-directing classification
Assessing Stem Stability (the crux)
- History: pre-injury thigh pain or start-up pain = red flag for a loose stem
- Radiographs: subsidence/migration, complete radiolucent lines, cement-mantle fracture, debonding
- Full-length femur films (hip + knee); compare with the original post-operative radiograph
- If any doubt remains: TEST the stem intra-operatively and decide on the table
- Plating a loose stem (missed B2) is the archetypal, avoidable failure
Treatment by Type
- A: usually non-operative; fix a displaced AG fragment if the abductors are threatened; investigate osteolysis
- B1 (well-fixed): ORIF — long locking plate spanning the femur, cables + unicortical locking screws proximally, bicortical distally, +/- cortical strut
- B2 (loose, good bone): revision to a long uncemented tapered fluted stem bypassing the fracture (+/- ORIF, often via ETO)
- B3 (loose, poor bone): long stem + graft/APC (young), or proximal femoral replacement (frail elderly, immediate weight-bearing)
- C: distal femoral locking plate — OVERLAP the stem, no inter-implant stress riser
Fixation Principles
- Span the WHOLE femur — avoid creating a new stress riser at a plate end
- Combination fixation around the stem: cerclage cables + unicortical locking screws + screws around the stem
- Cortical strut allograft augments fixation in poor bone and adds a second fixation plane
- Revision stem must gain distal diaphyseal fixation and bypass the fracture (about 2 cortical diameters)
- Overlap implants whenever two are present (hip + knee, or plate + stem)
Distal Femur Around a TKA
- Classification: Su (level vs component) and Lewis-Rorabeck (displacement + component fixation)
- Retrograde nail: open-box, well-fixed femoral component — load-sharing
- Distal femoral locking plate: versatile, very distal fractures or closed-box component
- Distal femoral replacement: loose component, unreconstructable comminution, frail elderly
- Mind the inter-implant zone if an ipsilateral hip stem is present
The Patient and Outcomes
- Rising incidence with arthroplasty volume and an ageing population (registry-documented)
- Mortality approaches that of a native hip fracture (about 10% at 1 year) — treat as a fragility fracture
- Orthogeriatric co-care, medical optimisation, early surgery
- Choose a construct allowing EARLY weight-bearing where possible
- Bone-health/osteoporosis treatment and falls prevention — it is a sentinel fragility event
Danger Zones / Classic Errors
- Plating a loose stem (B2 treated as B1) — addresses the fracture, not the cause; fails
- Inter-implant stress riser — short plate, or a gap between two implants — causes refracture
- Missing B3 (deficient bone) — a loose stem in poor bone needs graft or replacement, not a standard revision
- Imposing prolonged non-weight-bearing in a frail elderly patient — poorly tolerated, increases mortality
- Missing an infected loose stem presenting as a fracture — exclude infection before reconstruction
Background & Evidence
Epidemiology. Periprosthetic femoral fracture is a recognised and growing problem, driven by increasing arthroplasty volume and an ageing population (Lindahl, Swedish registry-based epidemiology). National joint registries (NJR UK, AOANJRR Australia, AJRR US, Swedish/Nordic registries) document a rising absolute number of these fractures, and periprosthetic fracture is now a recognised and growing indication for revision. Registry data also informs implant- and fixation-related fracture risk — for example, some collarless polished tapered cemented stems are associated with a recognised periprosthetic fracture pattern. The Vancouver classification in full (Duncan and Masri). Its strength is that it is comprehensive yet treatment-directing, with good inter- and intra-observer reliability and validity.
- Location
- Trochanteric region
- Stem
- Well-fixed
- Bone Stock
- Variable (often lytic)
- Typical Treatment
- Mostly non-operative; fix if abductor mechanism at risk
- Location
- Around / just distal to stem tip
- Stem
- Well-fixed
- Bone Stock
- Adequate
- Typical Treatment
- ORIF — locking plate, cables, +/- strut
- Location
- Around / just distal to stem tip
- Stem
- Loose
- Bone Stock
- Adequate
- Typical Treatment
- Revision to long stem (+/- ORIF)
- Location
- Around / just distal to stem tip
- Stem
- Loose
- Bone Stock
- Deficient
- Typical Treatment
- Long stem + graft, or proximal femoral replacement
- Location
- Well distal to stem tip
- Stem
- Well-fixed (irrelevant)
- Bone Stock
- Variable
- Typical Treatment
- ORIF as a fracture — plate must overlap the stem
Type A — trochanteric. AG = greater trochanter, AL = lesser trochanter. Usually low-energy, frequently associated with osteolysis from polyethylene wear particles that weakens the bone. Most are stable and managed non-operatively with protected weight-bearing. Fix a displaced AG fragment that destabilises the abductor mechanism (tension-band wiring, claw/hook plate, cables); a significant AL avulsion may be a marker of underlying osteolysis and impending stem compromise — investigate the stem. Type B — the decisive zone (around or just distal to the stem tip). Once a fracture is localised here, the only question that matters is whether the stem is well-fixed. B1 = well-fixed (fracture problem, fix it and keep the stem). B2 = loose with good bone (implant failure, revise). B3 = loose with deficient bone (reconstruct or replace). Type C — well distal to the stem tip. Treated as an ordinary distal/diaphyseal femoral fracture; the stem's fixation status is irrelevant to the fracture itself, but the construct must overlap the plate proximally with the stem to avoid an unsupported inter-implant segment. Outcomes. Well-classified and well-executed B1 ORIF and B2/B3 revisions achieve high union and stability rates; the major determinant of failure is misclassification (plating a loose stem) and inadequate constructs (short plates, inter-implant gaps). Cortical strut allografts incorporate over time and can augment fixation in poor bone. Periprosthetic distal femur (around a TKA) — brief account. - Classification: Su (based on level relative to the femoral component) and Lewis-Rorabeck (incorporates displacement and component fixation).
- Retrograde intramedullary nail: suitable when the femoral component has an open box that admits the nail and the component is well-fixed; gives load-sharing fixation.
- Distal femoral locking plate: versatile, especially for very distal fractures or a closed-box component; biological/bridging application.
- Distal femoral replacement: for a loose femoral component, very distal/comminuted unreconstructable fractures, or the frail elderly needing immediate weight-bearing.
- Beware the inter-implant zone: if a hip stem is also present (or a long plate is used), avoid leaving an unsupported segment between the two implants.
References
Fractures of the femur after hip replacement — the Vancouver classification
Original description of the Vancouver classification, combining fracture site, stem stability and bone stock into a single treatment-directing framework.
The reliability and validity of the Vancouver classification of femoral fractures after hip replacement
Demonstrates good inter- and intra-observer reliability and validity of the Vancouver system for guiding management.
Epidemiology of periprosthetic femur fracture around a total hip arthroplasty
Swedish registry-based epidemiology documenting the rising incidence of periprosthetic femoral fractures and their risk factors.
Periprosthetic femoral fractures above total knee replacements
The Su classification and management algorithm for periprosthetic distal femoral fractures around a total knee replacement.
Classification of periprosthetic fractures complicating total knee arthroplasty
The Lewis-Rorabeck classification, incorporating fracture displacement and component fixation status.