Prone Position | Two Intervals | Posterior Malleolus Buttress
- Prone positioning is essential for direct posterior visualisation and buttress plating — supine positioning does not allow it.
- The posterolateral interval between the peroneal tendons and flexor hallucis longus is the workhorse for most posterior malleolar fragments because it avoids direct dissection around the posterior tibial neurovascular bundle.
- The posterior tibial neurovascular bundle (artery, veins, tibial nerve) lies between flexor digitorum longus and tibialis posterior in the deep posterior compartment — identify and protect it before any deep medial work.
- A buttress (antiglide) plate on the posterior tibial cortex resists posterior and proximal displacement of the fragment under Achilles and plantarflexion load.
- Fragments involving greater than 25 percent of the articular surface or with greater than 2 mm step-off or gap generally warrant direct reduction and buttress fixation.
When & Why
What it exposes. The posterior approach gives direct access to the posterior malleolus and the posterior distal tibial plafond for fractures that cannot be adequately reduced or stabilised through standard lateral or anteromedial approaches. Approximately 7 to 44 percent of ankle fractures involve the posterior malleolus, with higher rates in pilon fractures. Two intervals, one position. Two primary intervals are used, both performed in the prone position so that gravity assists retraction of the posterior compartment and the posterior tibial surface is exposed for buttress plating. The posterolateral interval (peroneals and FHL) is the workhorse for posterolateral fragments and the fibula; the posteromedial interval (behind the medial malleolus, between TP/FDL and the neurovascular bundle) is reserved for isolated posteromedial fragments or medial extension.
- Interval and position
- Between peroneals and FHL; prone
- Best for
- Most posterior malleolar and posterolateral pilon fragments
- Interval and position
- Behind the medial malleolus, between TP/FDL and the NV bundle; prone
- Best for
- Isolated posteromedial fragments or medial extension
- Interval and position
- Both intervals through separate incisions in one prone position
- Best for
- Complex pilon with both posterior columns
When to operate. Fragments involving greater than 25 percent of the articular surface or with greater than 2 mm step-off or gap generally require direct reduction and buttress fixation. Smaller fragments may be treated with percutaneous anterior-to-posterior screws, but these carry a higher risk of malreduction and lack the buttress effect. Position and landmarks. Prone on a radiolucent table with the affected knee flexed 20 to 30 degrees over a bolster (this relaxes the gastrocnemius-Achilles complex), the foot overhanging the table end or supported on a padded rest, and all pressure points padded (face, chest rolls, pelvis, patellae and ankles). Arms are abducted less than 90 degrees with padding, and a tourniquet sits high on the thigh if used. Surface landmarks are the medial and lateral malleoli, the Achilles tendon midline, the fibular tip and posterior border of the fibula (posterolateral interval), the posteromedial border of the distal tibia (posteromedial interval), and the posterior tibial artery palpable behind the medial malleolus. Ensure the C-arm can rotate freely from the lateral side. If the patient cannot tolerate prone positioning, a lateral decubitus position with the affected side up is an alternative, although visualisation is slightly compromised.
The Exposure
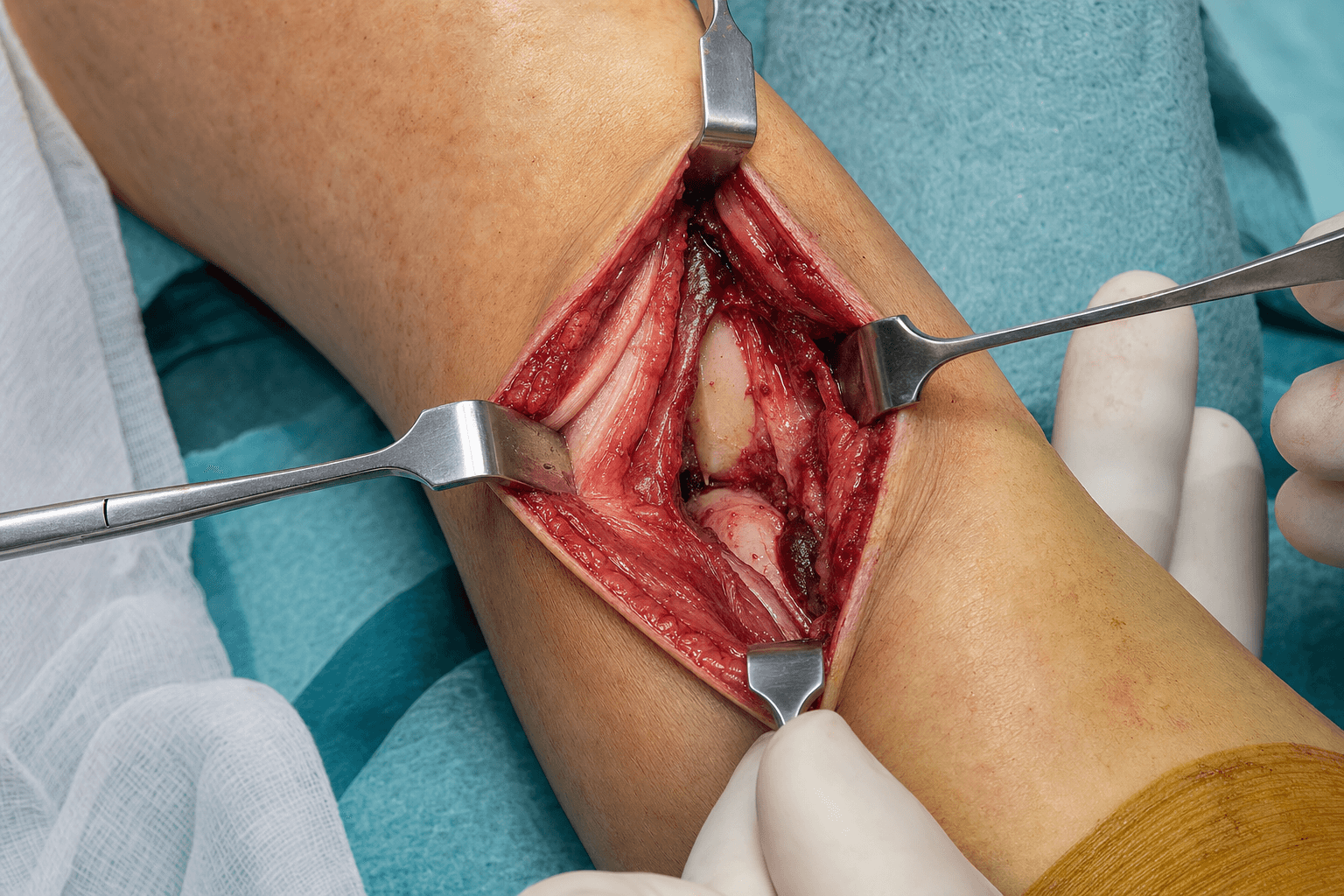
Work down through the layers along the posterior border of the fibula, protecting the sural nerve and short saphenous vein superficially, then develop the peroneals-FHL interval down to the posterior tibia and the medial neurovascular bundle. The posterolateral exposure is shown below; the posteromedial variant follows the second timeline.
Posterolateral exposure — the workhorse
- A longitudinal or slightly oblique incision 8 to 12 cm long, centred over the posterior border of the fibula and extending distally toward the tip of the fibula.
- The line allows proximal extension along the fibula and distal extension around the lateral malleolus for combined fibular fixation.
- Incise skin and subcutaneous tissue, identifying and protecting the sural nerve and short saphenous vein, which usually lie medial to the incision.
- Use blunt dissection in the subcutaneous plane and gentle retraction.
- Incise the fascia over the peroneal compartment, exposing the peroneal muscle group.
- Develop the interval between the peroneal tendons (retracted anteriorly, carrying the superficial peroneal nerve with them) and the fascia over flexor hallucis longus (retracted posteriorly and medially).
- This is an inter-compartmental plane between the superficial peroneal nerve laterally and the tibial nerve medially, so it avoids denervating either group.
- Identify the peroneal artery and its branches; ligate small perforators as needed while preserving the main vessel.
- Elevate the FHL origin subperiosteally from the posterior fibula and distal tibia using a Cobb elevator, staying on bone.
- This exposes the posterolateral distal tibia and the posterior malleolus.
- The posterior tibial neurovascular bundle is encountered medially in the deep compartment — identify and protect it with a vessel loop before proceeding medially.
- Reduce the fragment under direct vision and apply a buttress (antiglide) plate to the posterior tibial surface, with screws directed anteriorly.
Posteromedial exposure — for posteromedial fragments
- A longitudinal incision 6 to 10 cm long, posterior to the medial malleolus, along the posteromedial border of the distal tibia.
- Protect the saphenous nerve and great saphenous vein anteriorly in the subcutaneous plane.
- Incise the deep fascia and identify the interval between the Achilles tendon and the posteromedial structures.
- Identify the posterior tibial neurovascular bundle early (it lies posterior to flexor digitorum longus) and loop it for protection before any deep work.
- Develop the plane between tibialis posterior and flexor digitorum longus (retracted anteriorly) and the neurovascular bundle (retracted posteriorly).
- Expose the posterior distal tibia and posterior malleolus subperiosteally.
Injury to the posterior tibial neurovascular bundle causes ischaemic contracture, plantar numbness and intrinsic muscle paralysis. With careful identification and protection the incidence in posterior approaches is reported between 1 and 4 percent. Identify and loop the bundle, never place metal retractors directly on it, document neurovascular status pre- and intra-operatively, and if it is injured proceed to immediate vascular repair and nerve exploration.
Always perform blunt dissection in the deep plane and use a headlight or lighted retractor. The FHL muscle belly is the landmark for the correct interval — the neurovascular bundle lies just medial to FHL at the level of the ankle, so maintain constant awareness of its position during retraction.
Dangers & Extensions
Structures at risk, by layer and interval
- Structure at risk
- Sural nerve and short saphenous vein
- How to protect it
- Identify and retract gently; blunt dissection in the subcutaneous plane
- Structure at risk
- Saphenous nerve and great saphenous vein
- How to protect it
- Protect anteriorly in the subcutaneous plane
- Structure at risk
- Peroneal artery and venae comitantes
- How to protect it
- Ligate small perforators only; preserve the main vessel
- Structure at risk
- Posterior tibial neurovascular bundle
- How to protect it
- Identify and loop with a vessel loop before medial retraction
- Structure at risk
- Posterior tibial artery, veins and tibial nerve
- How to protect it
- Identify before any deep retraction; vessel loop; no metal retractors on the bundle
- Structure at risk
- FHL tendon (lateral to medial distally); FDL and TP tendons
- How to protect it
- Retract gently and protect during plate application
Extensile options. Extend the posterolateral incision proximally along the posterior border of the fibula (the interval remains between peroneals and FHL/soleus origin) to reach more proximal tibial shaft or plateau fragments, or distally to the tip of the fibula and around the lateral malleolus for combined fibular fixation. The posteromedial incision extends distally behind the medial malleolus when medial malleolar fixation is also needed. Closure and postoperative protocol. Close in layers over a drain if dissection was extensive or bleeding significant; close the deep fascia loosely to avoid a compartment syndrome, then subcutaneous tissue and skin in standard fashion. Apply a posterior splint or boot with the ankle in neutral to slight dorsiflexion, and keep the patient non-weight-bearing for 6 to 12 weeks depending on fracture stability and fixation. Early ankle range of motion begins at 2 weeks if fixation is stable, progressive weight bearing at 6 weeks with radiographic healing, and full weight bearing is typically achieved by 12 weeks. Obtain a CT at 12 weeks if there is clinical concern about articular congruity.
Procedures Through This Approach
- Pilon ORIF — posterior column fixation in pilon fractures (AO 43-B3, 43-C), usually performed first in the prone position.
- Trimalleolar ankle ORIF — direct reduction and buttress plating of large posterior malleolar fragments.
- Buttress (antiglide) plating for fragments greater than 25 percent of the articular surface or greater than 2 mm step-off.
- Combined fibular fixation and lateral malleolar ORIF through the same or extended posterolateral incision.
- FHL tendon decompression or repair if entrapped, and peroneal tendon access and repair (posterolateral interval).
- Bone grafting of metaphyseal voids after articular reduction.
Viva & Exam Focus
POSTLATPOSTLAT — the posterolateral exposure
Viva scenarios — posterior distal tibia approach
Practise clinical reasoning and management decisions out loud
“A 35-year-old male sustains a trimalleolar ankle fracture after a fall from height. CT shows a posterior malleolar fragment involving 35 percent of the articular surface with 3 mm of step-off. What approach would you use and why?”
“A 42-year-old female has an AO 43-C3 pilon fracture with a large posterolateral and posteromedial fragment after a motor vehicle collision. CT confirms both posterior columns are involved. How do you plan the surgical approach and positioning?”
“During a posteromedial approach for a posteromedial pilon fragment, you encounter brisk bleeding and loss of palpable posterior tibial pulse after placing a retractor. What is your immediate management?”
Positioning
- Prone position essential for direct posterior access
- Knee flexed 20 to 30 degrees over bolster relaxes Achilles
- All pressure points padded (face, chest, pelvis, knees)
- Radiolucent table mandatory for fluoroscopy
- Tourniquet high on thigh if used
Posterolateral Interval
- Primary workhorse for most posterior malleolar fragments
- Between peroneal tendons (superficial peroneal nerve) and FHL (tibial nerve)
- Sural nerve and short saphenous vein in the subcutaneous plane
- Peroneal artery branches may require ligation
- Posterior tibial NV bundle encountered medially - protect early
Posteromedial Interval
- Reserved for posteromedial fragments or medial extension
- Incision posterior to the medial malleolus
- Saphenous nerve protected anteriorly
- Posterior tibial artery, veins and tibial nerve are the critical dangers
- Develop plane between TP/FDL and the NV bundle
Danger Structures
- Posterior tibial neurovascular bundle - most critical deep structure
- Sural nerve (posterolateral) and saphenous nerve (posteromedial)
- Peroneal artery in the posterolateral interval
- Flexor hallucis longus tendon crosses the field distally
- No metal retractors directly on NV structures
Buttress Fixation
- Buttress plate on the posterior cortex resists posterior displacement
- Under-contour the plate for a compression effect
- Screws directed anteriorly from the posterior plate
- 3.5 mm reconstruction or anatomic posterior plates
- Confirm no intra-articular screw penetration on fluoroscopy
Procedures and Closure
- Direct reduction of the posterior malleolus and pilon posterior column
- Buttress plating for fragments greater than 25 percent or 2 mm step-off
- FHL and peroneal tendon access
- Layered closure with a drain if extensive
- Non-weight-bearing 6 to 12 weeks, posterior splint initially
References
The posterolateral approach to the tibia for displaced posterior malleolar injuries
- Posterolateral approach provides direct visualization and safe interval for buttress plating of displaced posterior malleolar fragments
A staged protocol for soft tissue management in the treatment of complex pilon fractures
- Staged protocol with spanning external fixation reduced deep infection rate from 23 percent to 4 percent in high-energy pilon fractures
- Definitive fixation delayed until wrinkle test positive (average 10 to 14 days)
- Posterior approaches performed safely in the staged protocol when posterior skin condition allowed
Comparison between anterior-to-posterior screw fixation versus posterolateral approach plate fixation for posterior malleolar fracture: a systematic review and meta-analysis
- Posterolateral approach plate fixation demonstrated superior reduction quality and outcomes versus indirect anterior-to-posterior screws
Safety of the modified posteromedial approach in complex ankle fractures: comparative analysis versus posterolateral access
- Modified posteromedial approach is safe with low complication rates and comparable access to posterolateral for complex posterior malleolar involvement