Anatomic reconstruction of the LCL, popliteus tendon and popliteofibular ligament | advanced
- Three primary static stabilisers: lateral collateral ligament (LCL), popliteus tendon and popliteofibular ligament (PFL). Missed grade III PLC injury is the most common cause of cruciate graft failure and persistent varus thrust.
- Dial test at 30 degrees isolates PLC; increased external rotation at both 30 and 90 degrees indicates combined PLC plus PCL injury. Side-to-side difference greater than 10 degrees is diagnostic of grade III injury.
- Common peroneal nerve must be identified, decompressed and protected throughout — nerve palsy occurs in up to 20 percent of acute PLC injuries and remains the most feared complication of reconstruction.
- LaPrade anatomic technique uses two femoral tunnels (LCL and popliteus) plus fibular and tibial tunnels to restore all three static restraints; non-anatomic fibular-based (Larson) techniques are simpler but less effective in combined injuries.
- “The dial test is performed prone with the knee at 30 and 90 degrees of flexion — thigh-foot angle difference greater than 10 degrees at 30 degrees alone confirms isolated PLC injury; difference at both angles indicates PCL involvement.
- “Varus stress radiograph at 20 degrees flexion with greater than 2.5 mm side-to-side difference or greater than 4 mm absolute opening confirms grade III LCL/PLC injury and predicts need for reconstruction.
- “Chronic varus alignment greater than 5 degrees must be corrected with biplanar osteotomy before or at the time of ligament reconstruction — failure to address bony alignment is the leading cause of recurrent laxity.
- “Tunnel convergence between femoral ACL and PLC tunnels is avoided by aiming the PLC femoral tunnels 35-40 degrees anterior and proximal relative to the lateral epicondyle axis.
When & Why
The posterolateral corner is reconstructed when its three static stabilisers are disrupted and the knee is symptomatic. Anatomic reconstruction restores the lateral collateral ligament (LCL), popliteus tendon and popliteofibular ligament (PFL) — the structures that resist varus and external rotation. Missed grade III PLC injury is the most common cause of cruciate graft failure, so identifying and reconstructing it is as important as the cruciate itself. Absolute indications
- Grade III PLC injury with symptomatic varus instability or thrust gait
- Combined cruciate and PLC injury requiring multi-ligament reconstruction
- Failed cruciate reconstruction secondary to untreated PLC insufficiency
- Chronic PLC injury with greater than 10 degrees side-to-side external rotation difference on the dial test Relative indications
- Grade II PLC injury with persistent functional instability after 3-6 months of rehabilitation
- Varus alignment greater than 5 degrees with medial compartment overload symptoms
- High-demand pivoting or cutting athlete with documented grade III laxity Contraindications
- Absolute: active knee infection or septic arthritis; uncontrolled medical comorbidities precluding major surgery; non-ambulatory patient with minimal functional demand
- Relative: acute grade I-II PLC injury (trial of non-operative management first); isolated grade II injury without thrust or giving-way; severe arthrofibrosis or range of motion less than 90 degrees flexion Confirm the injury before you cut. The decision rests on three tests. The dial test is performed prone at 30 and 90 degrees of flexion — a side-to-side external rotation difference greater than 10 degrees at 30 degrees alone confirms isolated grade III PLC injury, while a difference at both 30 and 90 degrees indicates combined PLC plus PCL injury. Varus stress radiographs at 20 degrees flexion with greater than 2.5 mm side-to-side difference or greater than 4 mm absolute opening confirm grade III LCL/PLC injury. The external rotation recurvatum test with a heel-height difference greater than 2 cm indicates significant PLC laxity. Obtain full-length standing hip-knee-ankle radiographs in every chronic case to assess alignment. Anatomic versus non-anatomic — the technique choice. Every reconstruction must decide between a true anatomic restoration and a simpler non-anatomic sling.
Restores all three static stabilisers with separate femoral tunnels for LCL and popliteus plus fibular and tibial tunnels. Near-native varus and rotational stability in biomechanical studies, and it reduces ACL graft forces by 30-40 percent in combined injuries. The evidence-based default.
A figure-of-eight graft around the fibular head. Simpler, but restores only two of the three stabilisers and does not control external rotation at 60-90 degrees as well — less effective in combined injuries.
Two tibial tunnels carry the limbs when the fibular head is fractured or bone stock is poor. The fallback when a fibular tunnel is not safe to create.
Correct chronic varus first. Chronic varus greater than 5 degrees produces medial compartment overload and accelerates graft failure. Opening-wedge or closing-wedge biplanar osteotomy normalises the mechanical axis and improves ligament reconstruction survival — it is mandatory when the mechanical axis falls medial to the medial tibial spine, performed before or concurrent with the ligament reconstruction. Consent. Counsel regarding common peroneal nerve injury (1-3 percent permanent palsy), recurrent instability (5-10 percent), stiffness requiring manipulation (10-15 percent), infection (less than 1 percent), and the possible need for osteotomy in chronic varus. Setup. General or spinal anaesthesia with a regional block for postoperative analgesia; a popliteal fossa catheter for 48-hour infusion is useful in complex multi-ligament cases. Graft is Achilles tendon allograft (preferred for size and strength) or ipsilateral/contralateral semitendinosus autograft, 7-9 mm in diameter for each limb — two grafts or a single bifurcated graft may be used.
The Operation
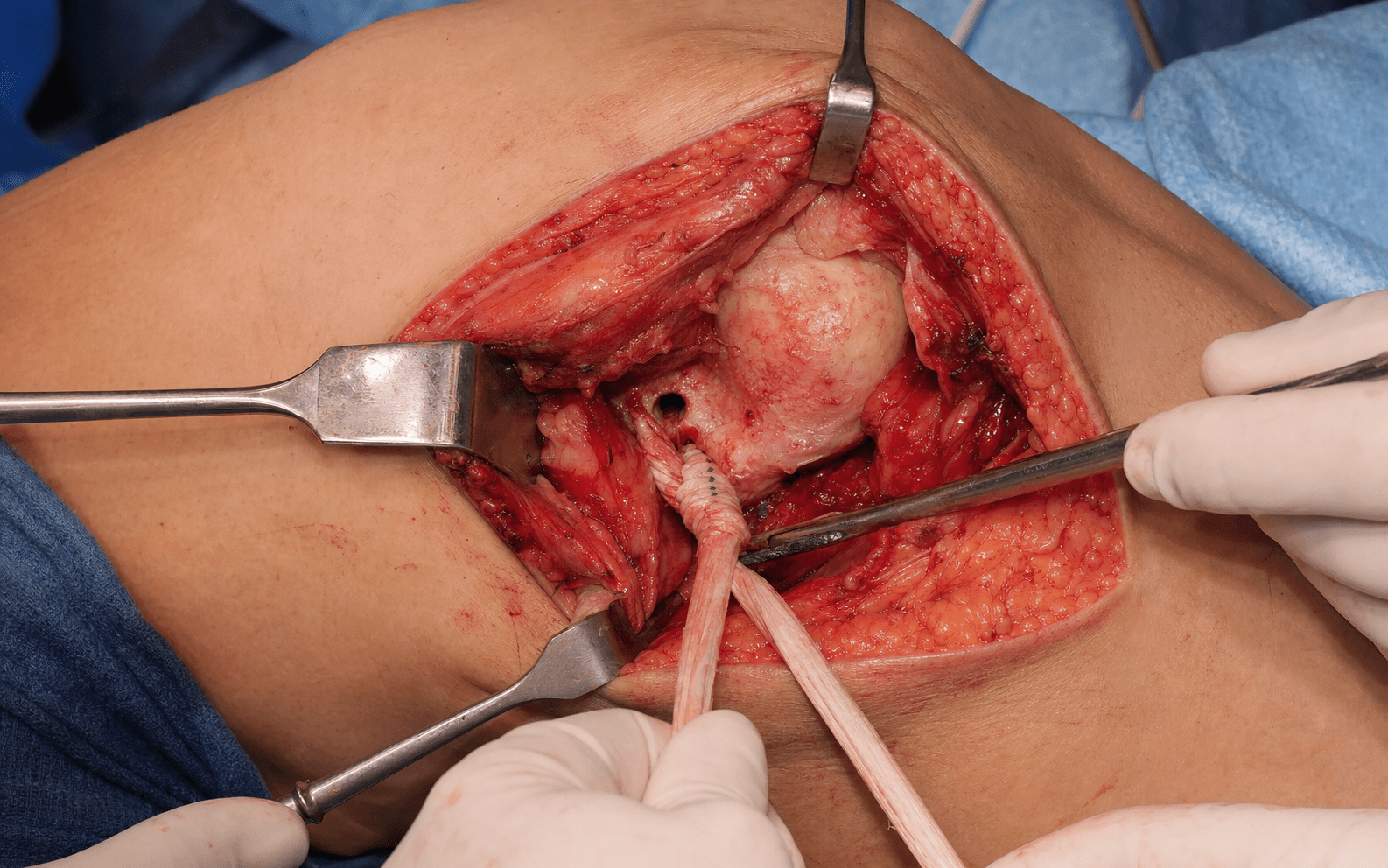
The goal: through the posterolateral exposure, identify and protect the common peroneal nerve, expose the fibular head and lateral femoral condyle, create fibular, tibial and two femoral tunnels, pass and tension graft limbs to restore all three static restraints, then fix the cruciates last. The exposure and nerve protection are laid out in full as the first steps below — this is the heart of the operation.
Operative sequence
- Supine with a leg holder allowing full flexion and extension (or lateral decubitus, hip flexed 45 degrees and knee flexed 90 degrees for an isolated PLC case). Thigh tourniquet, inflated only if bleeding obscures the deep dissection. The foot is prepped free so the dial test can be repeated intraoperatively.
- Palpate and mark the lateral femoral epicondyle, the posterior border of the iliotibial band, the fibular head and the biceps femoris tendon — these landmarks frame the incision.
- A curvilinear incision runs from the lateral femoral epicondyle distally along the posterior border of the iliotibial band to the fibular head, then distally along the posterior border of the biceps femoris.
- Split the iliotibial band in line with its fibres about 2 cm anterior to the lateral intermuscular septum. Retract the biceps femoris posteriorly to expose the common peroneal nerve.
- Identify the nerve at the posterior border of the biceps femoris, about 2 cm proximal to the fibular head. It winds around the fibular neck and divides into deep and superficial branches within the peroneal compartment.
- Decompress it from the fibular neck to the entrance of the peroneal tunnel and protect it with a vessel loop for the entire case. In chronic cases the nerve is often encased in dense scar — perform a formal neurolysis under loupes.
- Confirm continuity with intraoperative nerve stimulation before and after tunnel drilling.
- Expose the fibular head by elevating the peroneal muscles from its anterior surface and the soleus from its posterior surface, protecting the nerve throughout.
- Identify the LCL and PFL insertions on the fibular head — these mark the target for the fibular tunnel.
- Palpate the lateral epicondyle. The LCL origin lies 3-4 mm proximal and posterior to it; the popliteus tendon origin lies 11 mm anterior and distal to the LCL origin.
- Mark these two femoral footprints — they will receive the two femoral tunnels.
- Perform arthroscopy to confirm the combined injury, address meniscal pathology, and create the ACL or PCL femoral and tibial tunnels.
- The cruciate grafts are passed but fixed LAST, after the PLC, to avoid overconstraint.
- Place a 2.5 mm guide pin from anterolateral to posteromedial through the centre of the fibular head, exiting about 1 cm distal to the styloid tip.
- Confirm position with anteroposterior and lateral fluoroscopy, then over-ream to 6-7 mm and pass a passing suture.
- Identify Gerdy's tubercle. Start the pin 1 cm distal and medial to the tubercle, aimed 60 degrees distal and 20 degrees medial, exiting the posteromedial tibia about 1 cm distal to the joint line.
- Confirm on the lateral fluoroscopic view to keep clear of the popliteal vessels, then over-ream to 7 mm.
- At the LCL origin, place a 2.5 mm pin aimed 35-40 degrees anterior and proximal. At the popliteus origin (11 mm anterior and distal to the LCL origin) place a second pin on the same trajectory.
- Over-ream each to 7-8 mm to a depth of 25 mm. Confirm divergence from any ACL tunnel with fluoroscopy.
- Pass the LCL graft limb through the fibular tunnel from anterior to posterior and fix to the femoral LCL tunnel with a 7 mm interference screw at 20 degrees flexion in neutral rotation under slight valgus tension.
- Pass the popliteus/PFL limb through the tibial tunnel and fix to the popliteus femoral tunnel at 60 degrees flexion with slight internal rotation tension. Use a cortical button or interference screw fixation on the tibia.
- Reduce the knee in neutral rotation and slight valgus. Tension and fix the cruciate grafts last, after both PLC limbs are secured.
- Repeat the dial test to confirm that varus and external rotational stability have been restored.
- Irrigate, achieve haemostasis, and close in layers over a drain.
Identify the nerve first at the posterior biceps border, before any deep dissection. Decompress it fully around the fibular neck and keep a vessel loop on it for the whole case — in chronic injury perform a formal neurolysis under loupes. Stimulate before and after tunnel drilling to confirm you have not caused iatrogenic injury. Avoid excessive retraction during fibular exposure: use gentle technique with frequent relaxation, and confirm every guide pin in two planes before reaming so the nerve is not transected.
Three structures are at risk during tunnel creation. The common peroneal nerve — confirm pin position in two planes before fibular reaming to avoid transection. The fibular head — use a maximum 7 mm tunnel centred in the head to avoid fracture or cortical blow-out. The popliteal vessels — confirm the tibial guide pin on the lateral view and stay 1 cm distal to the joint line. In combined cases, aim the PLC femoral tunnels 35-40 degrees anterior and proximal and drill the ACL tunnel last to avoid femoral tunnel convergence.
Identify the common peroneal nerve at the posterior border of the biceps femoris before any deep dissection, decompress it around the fibular neck, and keep a vessel loop on it for the entire case. In chronic cases perform a formal neurolysis under loupes. Nerve stimulation before and after tunnel drilling confirms continuity and gives confidence that no iatrogenic injury has occurred.
Fix the LCL limb first at 20 degrees flexion under valgus load, then the popliteus limb at 60 degrees with slight internal rotation. Only once both PLC limbs are secured do you tension and fix the cruciate grafts. This order prevents the PLC from being over-tensioned by the cruciate and reduces tunnel-convergence problems.
Aftercare & Complications
Rehabilitation | Phase | Timing | Weight bearing & brace | Motion & strengthening | |---|---|---|---| | 1 — Protection | 0-6 weeks | Touch-down weight bearing with crutches (longer if osteotomy performed); hinged brace locked in extension for 2 weeks then unlocked, worn at all times except therapy | Passive and active-assisted flexion to 90 degrees by week 4; full extension maintained; quad sets, straight-leg raises, ankle pumps; no active hamstring contraction for 6 weeks | | 2 — Motion & strength | 6-12 weeks | Progress to full weight bearing at 6-8 weeks if radiographic healing confirmed; wean daytime brace 8-10 weeks, continue night brace to 12 weeks | Advance to full flexion by 8-10 weeks; closed-chain exercises, stationary bike, leg press; avoid open-chain hamstring work until 4 months | | 3 — Functional | 3-6 months | Full weight bearing | Progressive resistance, single-leg squats, proprioceptive training; initiate straight-line jogging at 4-5 months if strength and stability allow | | 4 — Return to sport | 6-9 months | Full | Cutting, pivoting and contact drills from 6-9 months; full return 9-12 months for contact or pivoting sports when strength symmetry is greater than 90 percent and the dial test is negative | Rehabilitation pearls
- Early quadriceps activation prevents patellar tendon shortening and anterior knee pain.
- Avoid active hamstring contraction for 6 weeks to protect the popliteus and PFL grafts.
- Serial dial testing at each phase confirms maintenance of stability.
- In combined osteotomy cases, delay weight bearing until radiographic union (typically 8-12 weeks). Complications
- Incidence
- 1-3 percent permanent; up to 20 percent transient
- Recognition
- Foot drop, sensory loss in the first web space, positive Tinel sign at the fibular neck
- Prevention and management
- Prevention: identify, decompress and protect the nerve throughout; use intraoperative stimulation. Management: ankle-foot orthosis for foot drop; exploration and neurolysis or repair if no recovery by 3-6 months; tendon transfers (posterior tibial to the dorsum of the foot) for permanent palsy
- Incidence
- 5-15 percent at 2 years
- Recognition
- Return of thrust gait, positive dial test greater than 10 degrees, varus stress opening greater than 3 mm
- Prevention and management
- Prevention: anatomic technique, correct chronic varus with osteotomy, avoid tunnel convergence, protect grafts during rehab. Management: revision reconstruction with allograft; consider osteotomy if alignment was not addressed initially
- Incidence
- 2-4 percent
- Recognition
- Intraoperative loss of fixation, postoperative varus instability, radiographic fracture line
- Prevention and management
- Prevention: 6-7 mm tunnel only, confirm two-plane fluoroscopy, avoid anterior or distal placement. Management: convert to tibial-based reconstruction or staged bone grafting and revision
- Incidence
- 3-8 percent in combined ACL-PLC
- Recognition
- Intraoperative loss of pin purchase, postoperative instability, CT confirmation of intersection
- Prevention and management
- Prevention: aim PLC tunnels 35-40 degrees anterior and proximal; drill the ACL tunnel last; use navigation if available. Management: redirect tunnel or use alternative fixation (cortical button); consider staged revision
- Incidence
- 10-20 percent requiring manipulation
- Recognition
- Loss of flexion greater than 10 degrees or extension deficit greater than 5 degrees at 6-8 weeks
- Prevention and management
- Prevention: early ROM from day 1, avoid over-tensioning in extension, use a popliteal catheter for analgesia. Management: aggressive physiotherapy; manipulation under anaesthesia at 6-8 weeks if flexion is less than 90 degrees; arthroscopic lysis if refractory
- Incidence
- Less than 1 percent
- Recognition
- Intraoperative bleeding, expanding haematoma, loss of distal pulses
- Prevention and management
- Prevention: confirm tibial guide-pin position on lateral fluoroscopy; stay 1 cm distal to the joint line. Management: immediate vascular exploration and repair; endovascular stent for a contained injury
- Incidence
- 5-10 percent at 5 years
- Recognition
- Progressive return of laxity, positive stress radiographs, MRI evidence of graft attenuation
- Prevention and management
- Prevention: address alignment, use a strong graft (Achilles allograft), protect during rehab, avoid early pivoting. Management: revision reconstruction with fresh allograft; consider osteotomy or arthroplasty in older patients
Viva & Exam Focus
L.P.P.The three static stabilisers and their functions
D.I.A.L.Diagnostic work-up of a PLC injury
- Location
- Posterior to the biceps femoris tendon, about 2 cm proximal to the fibular head, then around the fibular neck
- Risk
- Palsy in 15-25 percent of acute PLC injuries; the most feared complication; encased in scar in chronic cases
- How to avoid or manage
- Identify at the posterior biceps border, decompress from the fibular neck to the peroneal tunnel, protect with a vessel loop, confirm with stimulation
- Location
- The fibular head is small (average width 18-22 mm)
- Risk
- A tunnel too anterior, distal or large risks fracture or cortical blow-out
- How to avoid or manage
- Use a 6-7 mm tunnel centred in the head, directed anterolateral to posteromedial, exiting 1 cm distal to the styloid tip; confirm two-plane fluoroscopy before reaming
- Location
- LCL origin 3-4 mm proximal and posterior to the epicondyle; popliteus 11 mm anterior and distal; ACL femoral tunnel typically 6-7 mm from the lateral wall
- Risk
- Divergent angles let the ACL and PLC tunnels intersect within the lateral femoral condyle, weakening both reconstructions
- How to avoid or manage
- Aim PLC tunnels 35-40 degrees anterior and proximal; confirm divergence with fluoroscopy or navigation; in combined cases drill the ACL tunnel last
- Location
- Long-standing PLC insufficiency produces lateral joint opening and medial compartment overload, giving varus greater than 5 degrees on the standing hip-knee-ankle radiograph
- Risk
- Reconstruction alone in uncorrected varus leads to rapid graft stretch-out and recurrent instability
- How to avoid or manage
- Obtain full-length standing films in all chronic cases; correct varus greater than 5 degrees with biplanar osteotomy before or concurrent with reconstruction
- Location
- Immediately medial to the popliteus tendon insertion on the posterior tibia
- Risk
- Posterior tibial tunnel penetration can cause life-threatening haemorrhage or arteriovenous fistula
- How to avoid or manage
- Use a posteromedial tibial tunnel starting 1 cm distal and medial to Gerdy's tubercle, aimed 60 degrees distal and 20 degrees medial; confirm the guide pin on lateral fluoroscopy; have vascular instruments available
- Location
- In combined ACL-PLC or PCL-PLC injury the sequence of graft tensioning determines final stability
- Risk
- Tensioning the cruciate first in varus overconstrains or underconstrains the knee, leaving residual laxity and accelerating graft failure
- How to avoid or manage
- Reduce in neutral rotation and slight valgus; fix the PLC first, then the cruciate; in PCL-PLC fix the PCL at 90 degrees first, then the PLC at 20-30 degrees
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old rugby player sustains a combined ACL and grade III PLC injury during a tackle. Standing radiographs show 6 degrees of varus alignment. Describe your surgical plan, including the sequence of procedures and the rationale for any osteotomy.”
“During a LaPrade PLC reconstruction, after drilling the fibular tunnel you notice loss of pin purchase and a small cortical breach on the anterior fibular head. What is your intraoperative decision-making process and how do you salvage the reconstruction?”
“A 35-year-old patient with a chronic combined PCL and PLC injury undergoes reconstruction. At 6 months postoperatively the dial test shows a persistent 12-degree side-to-side difference at 30 degrees. What are the possible causes and your diagnostic work-up?”
Key diagnostic thresholds
- Dial test greater than 10 degrees side-to-side at 30 degrees = grade III isolated PLC
- Dial test greater than 10 degrees at both 30 and 90 degrees = combined PLC plus PCL
- Varus stress radiograph greater than 2.5 mm side-to-side or greater than 4 mm absolute = grade III LCL/PLC
- Heel-height difference greater than 2 cm on external rotation recurvatum test = significant PLC laxity
- Standing varus greater than 5 degrees = requires corrective osteotomy before ligament reconstruction
Tunnel parameters
- Fibular tunnel: 6-7 mm diameter, centre of the head, exit 1 cm distal to the styloid tip
- Tibial tunnel: start 1 cm distal and medial to Gerdy's tubercle, aim 60 degrees distal and 20 degrees medial
- Femoral LCL tunnel: 3-4 mm proximal and posterior to the lateral epicondyle, 35-40 degrees anterior and proximal trajectory
- Femoral popliteus tunnel: 11 mm anterior and distal to the LCL origin, same trajectory
- Maximum tunnel diameter to avoid fibular fracture = 7 mm
Tensioning sequence and angles
- LCL limb fixed at 20 degrees flexion under slight valgus load
- Popliteus/PFL limb fixed at 60 degrees flexion with slight internal rotation
- Cruciate grafts fixed last, after PLC fixation
- In combined PCL-PLC: fix the PCL at 90 degrees first, then the PLC at 20-30 degrees
- Final check: neutral rotation and slight valgus before cruciate fixation
Rehabilitation milestones
- Weeks 0-6: touch-down weight bearing, brace locked in extension initially, passive flexion to 90 degrees by week 4
- Weeks 6-12: progress to full weight bearing, full ROM, begin closed-chain strengthening
- Months 3-6: proprioception, straight-line jogging at 4-5 months
- Months 6-9: sport-specific drills, return to play when strength symmetry is greater than 90 percent and the dial test is negative
- No active hamstring contraction for the first 6 weeks to protect the popliteus and PFL grafts
Background & Evidence
The three static stabilisers. Modern anatomic reconstruction is built on the quantitative anatomy of the posterolateral corner. The three primary static restraints and their attachments are:
- Attachments
- Origin 3-4 mm proximal and posterior to the lateral epicondyle; insertion on the fibular head 8 mm posterior to the anterior margin and 14 mm distal to the tip; average length 70 mm
- Primary restraint
- Primary varus restraint at 0-30 degrees flexion
- Attachments
- Origin 11 mm anterior and distal to the LCL femoral origin on the lateral femoral condyle; courses posteromedially through the popliteal hiatus to insert on the posterior tibia
- Primary restraint
- Primary external rotation restraint at 30-90 degrees flexion
- Attachments
- Origin at the musculotendinous junction of popliteus; inserts on the posteromedial aspect of the fibular styloid about 1 cm distal to the tip
- Primary restraint
- Primary restraint to posterolateral rotation and varus at 60-90 degrees flexion
Dynamic stabilisers. The popliteus muscle, biceps femoris, lateral gastrocnemius head and iliotibial band provide dynamic posterolateral stability and must be protected during exposure. Common peroneal nerve course. The nerve emerges from posterior to the biceps femoris tendon about 2 cm proximal to the fibular head, winds around the fibular neck, and divides into deep and superficial peroneal nerves within the peroneal compartment. In acute injuries it may be stretched or contused; in chronic cases it is often encased in dense scar requiring neurolysis — which is why identification and decompression are mandatory steps of the operation. Why anatomic reconstruction matters. Non-anatomic fibular-based techniques (Larson figure-of-eight) restore only two of the three static stabilisers and do not address the popliteofibular ligament's contribution to external rotation control at 60-90 degrees. The LaPrade anatomic technique, with separate femoral tunnels for the LCL and popliteus plus fibular and tibial tunnels, restores near-native varus and rotational stability in biomechanical studies, and in combined ACL-PLC injuries it reduces ACL graft forces by 30-40 percent compared with non-anatomic techniques. Combined osteotomy evidence. Chronic varus greater than 5 degrees produces medial compartment overload and accelerates graft failure. Opening-wedge or closing-wedge biplanar osteotomy normalises the mechanical axis and improves ligament reconstruction survival. In series of combined osteotomy plus ligament reconstruction, 85-90 percent of patients achieve good or excellent outcomes at 5 years with low revision rates.
References
The posterolateral attachments of the knee: a qualitative and quantitative morphologic analysis of the fibular collateral ligament, popliteus tendon, popliteofibular ligament, and lateral gastrocnemius tendon
- Cadaveric sectioning study defining the three primary static stabilisers of the posterolateral corner
- Quantified the contribution of LCL, popliteus tendon and PFL to varus and external rotation restraint at multiple flexion angles
- Established the anatomic landmarks used in modern anatomic reconstruction techniques
An analysis of an anatomical posterolateral knee reconstruction: an in vitro biomechanical study and development of a surgical technique
- Biomechanical validation of the LaPrade fibular-and-tibial-based anatomic reconstruction
- Demonstrated restoration of near-native varus and rotational stability compared with non-anatomic techniques
- Highlighted the importance of separate femoral tunnels for the LCL and popliteus tendon
Proximal tibial opening wedge osteotomy as the initial treatment for chronic posterolateral corner deficiency in the varus knee: a prospective clinical study
- Prospective clinical study demonstrating that proximal tibial osteotomy improves posterolateral stability in chronic varus knees with PLC deficiency
Posterolateral corner injuries of the knee: anatomy, diagnosis, and treatment
- Comprehensive review outlining the anatomic basis and surgical principles for anatomic PLC reconstruction
Current concepts in the recognition and treatment of posterolateral corner injuries of the knee
- Evidence-based review of diagnostic tests and treatment algorithms supporting anatomic reconstruction for grade III PLC injuries