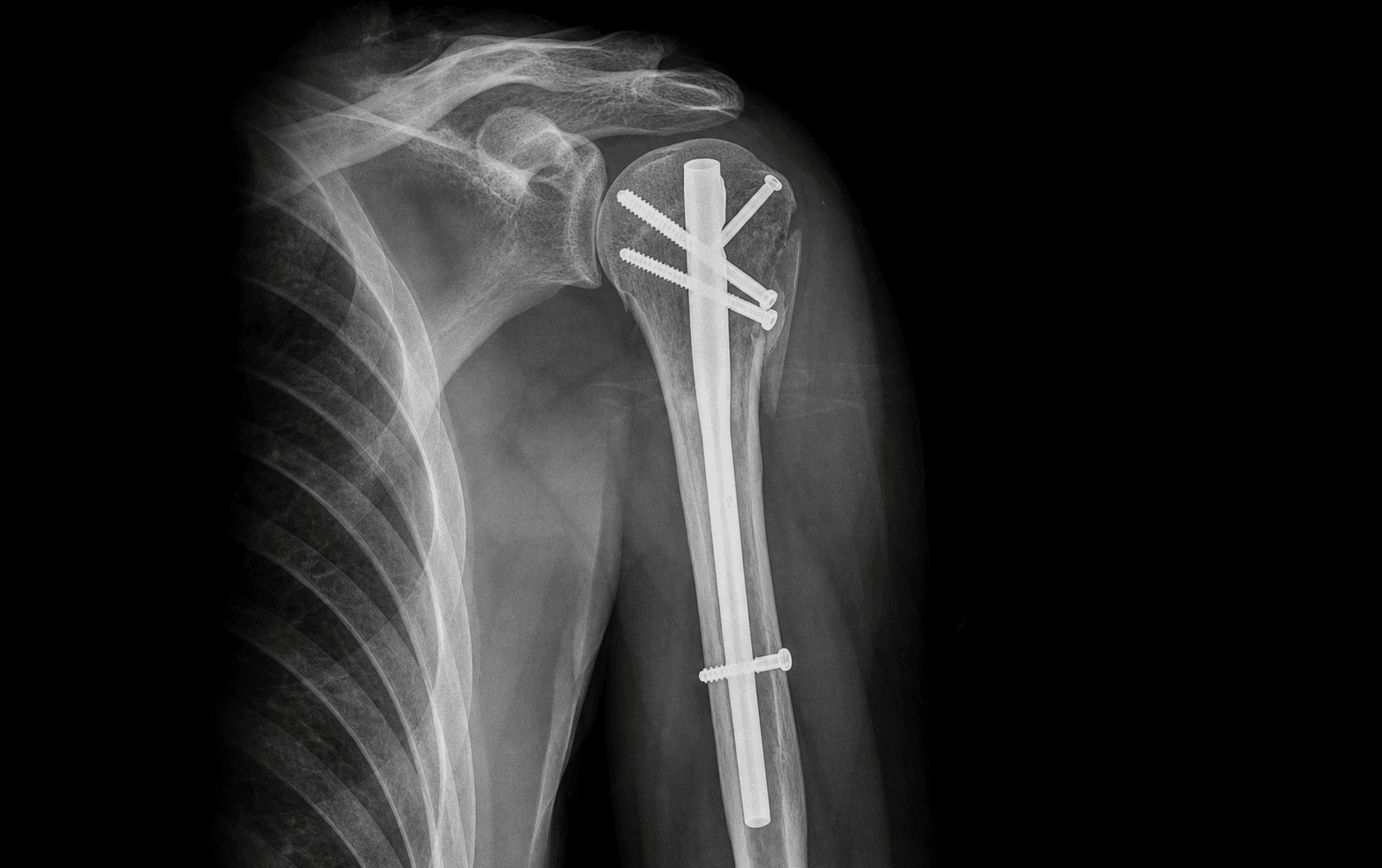
Antegrade intramedullary nailing via the anterosuperior deltoid-split approach for surgical neck and proximal humeral fractures
- The entry point is the operation: a straight medial entry at the apex of the humeral head articular surface spares the rotator cuff footprint and prevents varus malreduction. Older bent nails required a more lateral entry through the greater tuberosity and supraspinatus tendon, causing iatrogenic cuff injury in up to 25% of cases.
- The anterosuperior deltoid-split approach places the axillary nerve at risk approximately 5-7 cm distal to the acromion. The safe zone is proximal to this; identify and protect the nerve with a vessel loop before any distal extension of the split.
- Proximal locking must achieve multiplanar fixation (typically two or three proximal screws in different planes) plus separate tuberosity fixation when the greater or lesser tuberosity is displaced. Varus malunion greater than 20 degrees is the most common technical error and strongly predicts poor outcome.
- Distal interlocking is performed with the arm in slight abduction and external rotation to avoid the radial nerve in the spiral groove. Use a minimum of two distal screws; one static and one dynamic slot if available on the implant system.
When & Why
Indication. Antegrade intramedullary nailing for a displaced 2-part surgical neck fracture of the proximal humerus that has failed non-operative care, or for fracture patterns where a load-sharing implant is biomechanically preferable to a locking plate. The decision to nail — and the choice of nailing over plating — rests on fracture pattern, bone quality and the soft-tissue envelope, not on any proven functional superiority. Absolute indications
- Displaced 2-part surgical neck fracture with greater than 50% translation or greater than 30 degrees angulation in a physiologically young or active patient
- Segmental proximal humerus fractures extending into the diaphysis where a load-sharing implant is biomechanically advantageous
- Pathological fractures through metastatic lesions in the proximal humerus where immediate stability is required for palliation
- Failed non-operative treatment of a surgical neck fracture with ongoing pain and loss of function at 6-8 weeks Relative indications
- Osteoporotic 2-part or 3-part fractures in elderly patients where locking-plate fixation carries a high risk of screw cut-out
- Bilateral proximal humerus fractures where a single implant allows earlier mobilisation
- Patients with a poor soft-tissue envelope or comorbidities precluding extensive open reduction and plate fixation Contraindications
- Absolute: active infection at the surgical site or systemic sepsis; severe pre-existing rotator cuff arthropathy or an irreparable cuff tear that would render nailing ineffective; an open proximal humerus fracture with extensive soft-tissue loss requiring flap coverage.
- Relative: greater tuberosity displacement greater than 1 cm that cannot be adequately reduced and fixed through the nail (consider a plate or combined approach); severe varus deformity with medial comminution where anatomic reduction cannot be achieved closed (consider open reduction or plate); patient non-compliance with protected weight-bearing in the early post-operative period. Nail or plate? Modern straight intramedullary nails provide a load-sharing construct that is particularly advantageous in osteoporotic bone and segmental fracture patterns. The medial entry point completely spares the rotator cuff footprint, eliminating the iatrogenic cuff injury inherent in older bent-nail designs. A systematic review of randomised trials comparing nailing with locking-plate fixation found no significant difference in functional scores or complication rates at one year, but nailing was associated with shorter operative time and lower blood loss. Nonunion rates are low (less than 5%) with both techniques when reduction is anatomic; varus malunion remains the most common technical error with nailing and strongly predicts poorer outcome. (The full side-by-side comparison is in Background and Evidence.) Consent. Counsel specifically regarding axillary nerve injury (2-3%), rotator cuff injury (less than 5% with straight nails), varus malunion (10-20%), screw back-out (5-10%), nonunion (less than 5%), avascular necrosis (3-8%), and the need for protected weight-bearing for six weeks. Setup. Beach-chair position with the head secured in a Mayfield headrest; the arm is draped free and placed on a radiolucent hand table or supported by an assistant. Position the C-arm to allow true AP, scapular-Y and axillary views without moving the patient. General anaesthesia with an interscalene block for post-operative analgesia; muscle relaxation is essential for closed reduction manoeuvres.
The Operation
The goal is to stabilise the surgical neck fracture with a load-sharing intramedullary construct through the anterosuperior deltoid-split approach, using a rotator-cuff-sparing medial entry point, while protecting the axillary nerve proximally and the radial nerve distally. The exposure is laid out in full as the first steps below — it is the heart of the operation.
Operative sequence
- Make a 4-6 cm longitudinal incision from the anterolateral corner of the acromion distally along the deltoid raphe. The raphe is identified by the orientation of the deltoid fibres and the relative paucity of vessels.
- Deepen through subcutaneous fat to the deltoid fascia, then split the deltoid fibres in line with the raphe using blunt dissection with scissors or a finger.
- Keep the initial split to 4 cm; do not extend distally until the axillary nerve has been identified (Step 2).
- Insert a finger or blunt instrument along the deep surface of the deltoid and palpate the axillary nerve as a transverse cord 5-7 cm distal to the acromion.
- Pass a vessel loop around the nerve and gently retract it distally.
- The safe zone for the deltoid split is proximal to the nerve; any distal extension must be performed under direct vision with the nerve protected.
- Incise the subdeltoid bursa and retract the deltoid laterally.
- Identify the long head of biceps tendon in the bicipital groove as the key rotational landmark.
- Visualise the greater and lesser tuberosities and the humeral head articular surface.
- Perform closed reduction manoeuvres: longitudinal traction, abduction and external rotation to correct varus and restore the head-shaft angle. Confirm reduction on AP and scapular-Y views with the image intensifier.
- The entry point is at the apex of the humeral head articular surface, just medial to the rotator cuff footprint and in line with the medullary canal.
- Confirm the entry point on the AP view (medial to the greater tuberosity) and the axillary view (centred on the head) before reaming.
- Select the appropriate nail length and diameter (typically 9-11 mm diameter for most adults). Insert the nail over the guide wire with the arm in slight abduction to avoid varus.
- Seat the proximal nail end 2-3 mm below the articular surface to prevent subacromial impingement; confirm on the AP view.
- Lock proximally using the targeting guide with multiplanar fixation — typically two or three proximal screws in different planes (one anterior, one posterior, one superior). When the greater tuberosity is displaced, use the nail's tuberosity-specific locking options or pass heavy non-absorbable sutures through the cuff and secure them to the nail or a separate screw.
- Position the arm in slight abduction and external rotation to move the radial nerve away from the lateral cortex.
- Place two distal interlocking screws using the free-hand technique or the distal targeting guide (one static, one dynamic slot if available).
- Confirm screw position and length on the AP and lateral views.
- Obtain final AP, scapular-Y and axillary views to confirm anatomic reduction, correct nail position and secure tuberosity fixation.
- Irrigate the wound. Close the deltoid fascia with absorbable sutures and the skin with non-absorbable interrupted sutures.
- Apply a sling.
The axillary nerve exits the quadrilateral space and courses transversely across the deep surface of the deltoid approximately 5-7 cm distal to the acromion, where it can be palpated as a cord-like structure within the subdeltoid bursa. Identify it and protect it with a vessel loop before extending the deltoid split beyond 5 cm — the anterior branch supplies the anterior and middle deltoid and is the structure most at risk. Excessive medial retraction can also injure the cephalic vein or the anterior circumflex humeral vessels, and in obese patients the nerve may lie more distal than expected, so always confirm its position by palpation.
The entry point must sit at the apex of the articular surface, collinear with the medullary canal. A starting point that is too lateral — through the greater tuberosity — damages the supraspinatus insertion and forces the nail into varus. Achieve anatomic reduction before reaming: failure to do so locks in a permanent varus deformity. In osteoporotic bone, avoid over-reaming, which risks iatrogenic fracture propagation.
Place the guide wire under direct vision at the apex of the articular cartilage. Confirm on the AP view that the wire is collinear with the humeral shaft and on the axillary view that it is centred — any lateral starting point will force varus when the nail is inserted. After nail insertion, obtain a true AP view and measure the head-shaft angle; if it is less than 130 degrees, remove the nail, re-reduce the fracture in valgus and re-insert. Never accept varus greater than 20 degrees. Lock proximally with at least two screws in different planes and add tuberosity sutures if needed.
The single most important technical advance over first-generation bent nails is the true rotator-cuff-sparing medial entry at the apex of the articular cartilage. Bent nails entered laterally through the supraspinatus footprint and caused iatrogenic cuff injury in up to 25% of cases; the straight medial entry, combined with multiplanar proximal locking, is the reason modern nails preserve cuff integrity while improving varus stability.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation and activity | Therapy | |-------|--------|------------------------------|---------| | Early | 0-2 weeks | Sling for comfort; non-weight-bearing; wound review at 10-14 days | Pendulum and passive range from day 1; active-assisted abduction limited to 60 degrees | | Intermediate | 3-6 weeks | Sling for comfort when not exercising | Progressive active forward elevation and external rotation; isometric deltoid and cuff work from 4 weeks | | Late | 7-12 weeks | Progressive weight-bearing from 6 weeks to full by 12 weeks | Active strengthening (Theraband, light dumbbell); functional training; driving when safe | | Return to function | — | Light work 6-8 weeks; manual labour 3-4 months; contact sports or heavy lifting 4-6 months after radiographic union | Graded return to sport and heavy activity | Rehabilitation pearls
- Early passive motion prevents stiffness but must not compromise reduction.
- In osteoporotic bone, extend protected weight-bearing to 8-10 weeks and delay active abduction.
- Formal physiotherapy input is essential; patient-directed home exercises alone are insufficient. Special considerations Osteoporotic bone. Consider polymethylmethacrylate (PMMA) augmentation of the proximal locking screws, use the largest diameter proximal screws available in the implant system, extend protected weight-bearing and delay active abduction, and obtain serial radiographs every two weeks for the first six weeks to detect early collapse. Tuberosity fixation. When the greater tuberosity is displaced greater than 5 mm, pass heavy non-absorbable sutures through the cuff and secure them to the nail or a separate screw. Confirm tuberosity position on the axillary view before final locking, and limit post-operative abduction to 60 degrees for four weeks to protect the repair. Complications
- Incidence
- 2-3% (higher if the split is extended without identification)
- Recognition
- Deltoid weakness, sensory loss over the lateral shoulder, positive deltoid extension lag sign
- Prevention and management
- Identify and protect the nerve with a vessel loop before extending the split beyond 5 cm. Most are neurapraxias resolving by 6 months; a persistent deficit at 3 months warrants EMG and exploration
- Incidence
- 10-20%
- Recognition
- Head-shaft angle less than 120 degrees on AP, loss of forward elevation, impingement pain
- Prevention and management
- Anatomic reduction before nailing, medial entry point, provisional K-wire stabilisation in valgus. Corrective osteotomy if symptomatic and young; accept in the elderly if function is acceptable
- Incidence
- 5-10% (higher in osteoporosis)
- Recognition
- Progressive varus collapse on serial radiographs, screw prominence, loss of fixation
- Prevention and management
- PMMA augmentation of proximal screws in severe osteoporosis, protected weight-bearing for 6 weeks. Revision to locking plate or hemiarthroplasty if collapse is symptomatic
- Incidence
- 5-15% (markedly lower with straight nails)
- Recognition
- Persistent lateral shoulder pain, abduction weakness, positive drop-arm test
- Prevention and management
- Medial straight-nail entry completely spares the cuff footprint. MRI if symptomatic; repair if a full-thickness tear is confirmed
- Incidence
- less than 5%
- Recognition
- Persistent pain at the fracture site at 6 months, lack of radiographic healing, hardware failure
- Prevention and management
- Anatomic reduction, stable fixation, avoid smoking and NSAIDs. Revision open reduction with bone grafting and conversion to locking plate or nail exchange
- Incidence
- 3-8% (higher with 3-part and 4-part fractures)
- Recognition
- Progressive collapse of the humeral head on radiographs, increasing pain and stiffness at 6-18 months
- Prevention and management
- Anatomic reduction, preservation of the medial periosteal hinge, avoid excessive stripping. Observe for early collapse; hemiarthroplasty or reverse shoulder arthroplasty for symptomatic late collapse
- Incidence
- less than 1%
- Recognition
- Wrist drop, loss of finger extension, sensory loss in the first dorsal web space
- Prevention and management
- Arm in abduction and external rotation during distal interlocking; confirm drill trajectory on the image intensifier. Observe for 3 months (most neurapraxias resolve); explore if no recovery
- Incidence
- 5-10%
- Recognition
- Pain with abduction greater than 90 degrees, positive Neer impingement sign, nail prominence on radiographs
- Prevention and management
- Seat the proximal nail 2-3 mm below the articular surface. Nail removal after union if symptomatic; arthroscopic acromioplasty if nail position is correct
Viva & Exam Focus
ENTRYENTRY — Straight nail entry biomechanics
NAILNAIL — Pre-locking checklist
The trap. Using an older bent-nail entry point through the greater tuberosity and supraspinatus tendon footprint causes iatrogenic rotator cuff injury and persistent shoulder pain. The fix. Modern straight nails permit a medial entry at the apex of the humeral head articular cartilage, completely sparing the rotator cuff insertion. Confirm the entry point on the AP and axillary views before reaming.
Location. The axillary nerve exits the quadrilateral space and courses transversely 5-7 cm distal to the acromion on the deep surface of the deltoid. Risk. Extending the deltoid split beyond 5 cm without identifying the nerve risks transection or stretch injury. Always identify the nerve with a vessel loop before distal extension.
The trap. Accepting a varus reduction (head-shaft angle less than 120 degrees) leads to poor functional outcome, screw cut-out and nonunion. The fix. Achieve anatomic reduction before guide-wire placement. The medial entry point plus provisional K-wire stabilisation in valgus prevents varus collapse. Confirm 130-140 degrees on the true AP view before locking.
Location. The radial nerve lies in the spiral groove on the posterior humerus, approximately 10-12 cm proximal to the lateral epicondyle. Risk. A laterally directed distal interlocking screw or drill bit can injure the nerve when the arm is in neutral rotation. Place the arm in slight abduction and external rotation and confirm the drill trajectory on the image intensifier.
The trap. Treating a 2-part surgical neck fracture as isolated when the greater tuberosity is displaced greater than 5 mm leads to rotator cuff dysfunction and impingement. The fix. Always assess tuberosity position on the AP, scapular-Y and axillary views. Displaced tuberosities require separate fixation (suture or screw) through the proximal nail locking options or an additional mini-open approach.
Why it is different. Severe osteoporosis reduces proximal screw purchase and increases the risk of screw back-out and secondary varus collapse. Implications. Consider PMMA augmentation of the proximal locking screws or a nail with larger diameter proximal screws. Extend protected weight-bearing and delay active abduction to reduce early failure.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman with osteoporosis (T-score -3.2) sustains a displaced 2-part surgical neck fracture of the proximal humerus after a fall from standing height. The head-shaft angle measures 95 degrees on the AP radiograph. Discuss your operative plan and the specific technical modifications required for osteoporotic bone.”
“You are planning antegrade nailing for a 45-year-old man with a segmental proximal humerus fracture extending into the diaphysis. The greater tuberosity is displaced 8 mm laterally. Walk me through the critical technical steps to address the tuberosity and ensure stable fixation.”
“A 72-year-old woman underwent antegrade nailing of a 2-part surgical neck fracture 8 weeks ago. She presents with increasing shoulder pain and radiographs show 15 degrees of varus collapse with one proximal screw backing out. Discuss your assessment and management options.”
Key indications
- Displaced 2-part surgical neck fracture with greater than 50% translation or greater than 30 degrees angulation
- Segmental fractures extending into the diaphysis — load-sharing advantage of the nail
- Osteoporotic bone where locking-plate screw cut-out risk is high
- Failed non-operative treatment at 6-8 weeks with ongoing pain and dysfunction
Critical anatomy
- Straight-nail entry: apex of the humeral head articular surface, medial to the rotator cuff footprint
- Axillary nerve: 5-7 cm distal to the acromion on the deep surface of the deltoid — identify before extending the split
- Radial nerve: spiral groove, 10-12 cm proximal to the lateral epicondyle — protect during distal interlocking
- Head-shaft angle: normal 130-140 degrees; varus less than 120 degrees predicts poor outcome
Surgical approach pearls
- Anterosuperior deltoid-split: 4-6 cm incision along the deltoid raphe from the anterolateral acromion
- Identify the axillary nerve with a vessel loop before extending the split beyond 5 cm
- The long head of biceps in the bicipital groove is the key rotational landmark
- The medial entry point completely spares the rotator cuff footprint
Reduction and fixation principles
- Anatomic reduction before nail insertion — varus is the most common technical error
- Provisional K-wire stabilisation in valgus prevents collapse during nail passage
- Proximal locking: minimum two screws in different planes plus tuberosity fixation when displaced greater than 5 mm
- Distal interlocking: arm in abduction and external rotation; two screws minimum (one static, one dynamic)
Osteoporosis modifications
- PMMA augmentation of proximal locking screws increases load to failure by approximately 68%
- Use the largest diameter proximal screws available in the system
- Extend protected weight-bearing to 8 weeks and delay active abduction
- Serial radiographs every 2 weeks for the first 6 weeks to detect early collapse
Common complications
- Varus malunion (10-20%): head-shaft angle less than 120 degrees — preventable with anatomic reduction
- Screw back-out (5-10%): higher in osteoporosis without augmentation
- Axillary nerve injury (2-3%): eliminated by routine nerve identification
- Avascular necrosis (3-8%): higher with varus malreduction or excessive stripping
- Rotator cuff injury (5-15%): markedly lower with the straight medial entry versus older bent nails
Post-operative protocol
- Sling for comfort; pendulum exercises from day 1; active-assisted abduction limited to 60 degrees for 2 weeks
- Non-weight-bearing for 6 weeks (8 weeks in osteoporosis)
- Active strengthening from week 7; return to manual work at 3-4 months
- Tuberosity repair: limit abduction to 60 degrees for 4 weeks post-operatively
Background & Evidence
Surgical anatomy of antegrade nailing Humeral head and neck geometry. The humeral head articular surface is retroverted approximately 20-30 degrees relative to the transepicondylar axis and inclined 130-140 degrees to the shaft. The anatomic neck is the oblique groove separating the articular surface from the tuberosities; the surgical neck lies distal to the tuberosities at the metaphyseal-diaphyseal junction. The bicipital groove lies between the greater and lesser tuberosities and is the key landmark for rotational reduction. Rotator cuff footprint and entry point. The supraspinatus inserts on the superior facet of the greater tuberosity; the infraspinatus on the middle and inferior facets; the teres minor on the inferior facet. Older bent-nail designs required a lateral entry through the supraspinatus tendon footprint, producing iatrogenic cuff injury in up to 25% of cases. Modern straight nails allow a true medial entry at the apex of the articular cartilage, completely sparing the cuff footprint. Axillary nerve course. The axillary nerve exits the quadrilateral space posteriorly and courses transversely across the deep surface of the deltoid approximately 5-7 cm distal to the acromion. It lies within the subdeltoid bursa and can be palpated as a cord-like structure before visual identification. It divides into anterior and posterior branches; the anterior branch supplies the anterior and middle deltoid and is at greatest risk during the split. Radial nerve and distal interlocking. The radial nerve descends in the spiral groove on the posterior humerus, approximately 10-12 cm proximal to the lateral epicondyle, then pierces the lateral intermuscular septum to become superficial in the distal third of the arm. During distal interlocking the arm is positioned in slight abduction and external rotation to move the nerve away from the lateral cortex trajectory. Vascular supply and avascular necrosis risk. The ascending branch of the anterior circumflex humeral artery (the arcuate artery) enters the humeral head at the superomedial aspect of the bicipital groove and supplies the majority of the head. Anatomic reduction and preservation of the medial periosteal hinge are critical to maintaining head perfusion. Avascular necrosis occurs in 3-10% of 3-part and 4-part fractures and is higher with varus malreduction or excessive soft-tissue stripping.
- Intramedullary nail
- 60-90 minutes
- Locking plate
- 90-120 minutes
- Intramedullary nail
- 50-150 mL
- Locking plate
- 200-400 mL
- Intramedullary nail
- Preserved (medial entry)
- Locking plate
- At risk (deltopectoral approach)
- Intramedullary nail
- 10-20% (technical)
- Locking plate
- 5-15%
- Intramedullary nail
- 15-25% (cuff-related)
- Locking plate
- 10-20% (implant-related)
- Intramedullary nail
- 8-12%
- Locking plate
- 10-15%
References
Effect of intramedullary nail and locking plate in the treatment of proximal humerus fracture: an update systematic review and meta-analysis
- Systematic review and meta-analysis including randomised and observational studies comparing intramedullary nailing versus locking plate for proximal humerus fractures
- No significant difference in functional outcome scores (Constant, DASH) or overall complication rates between nailing and plating
- Intramedullary nailing associated with significantly shorter operative time and reduced blood loss in pooled analyses
The female geriatric proximal humeral fracture: protagonist for straight antegrade nailing?
- Prospective evaluation of straight antegrade nailing in elderly female patients with proximal humeral fractures and low bone mineral density
- High union rates and acceptable functional scores with low rates of varus collapse when modern straight-nail designs and medial entry were employed
- Straight nails performed particularly well in osteoporotic bone compared with historical bent-nail data
Biomechanical evaluation of straight antegrade nailing in proximal humeral fractures: the rationale of the proximal anchoring point
- Cadaveric biomechanical study demonstrating that a medial straight-nail entry at the apex of the humeral head articular surface optimises load-sharing and reduces the varus moment arm
- The proximal anchoring point concept explains the superior stability of modern straight nails versus older bent-nail designs that entered through the greater tuberosity
- Multiplanar proximal locking screws significantly increased construct stiffness under varus and rotational loading
Different treatments for 3- or 4-part proximal humeral fractures in elderly patients: a Bayesian network meta-analysis of randomised controlled trials
- Bayesian network meta-analysis of randomised controlled trials in elderly patients with 3- and 4-part proximal humeral fractures
- Intramedullary nailing ranked highly for functional recovery and lower reoperation rates in selected osteoporotic fracture patterns
- Locking plates and nailing both outperformed non-operative treatment; nailing showed advantages in operative time and blood loss