Anatomic subcapital realignment via Ganz surgical hip dislocation with retinacular-flap protection of the MFCA · advanced
- The modified Dunn procedure is indicated for moderate-to-severe slips (Southwick angle greater than 30 to 40 degrees) and selected unstable slips where in-situ pinning would leave an unacceptable residual cam deformity and femoroacetabular impingement. The goal is anatomic subcapital realignment while preserving the epiphyseal blood supply via the retinacular soft-tissue flap.
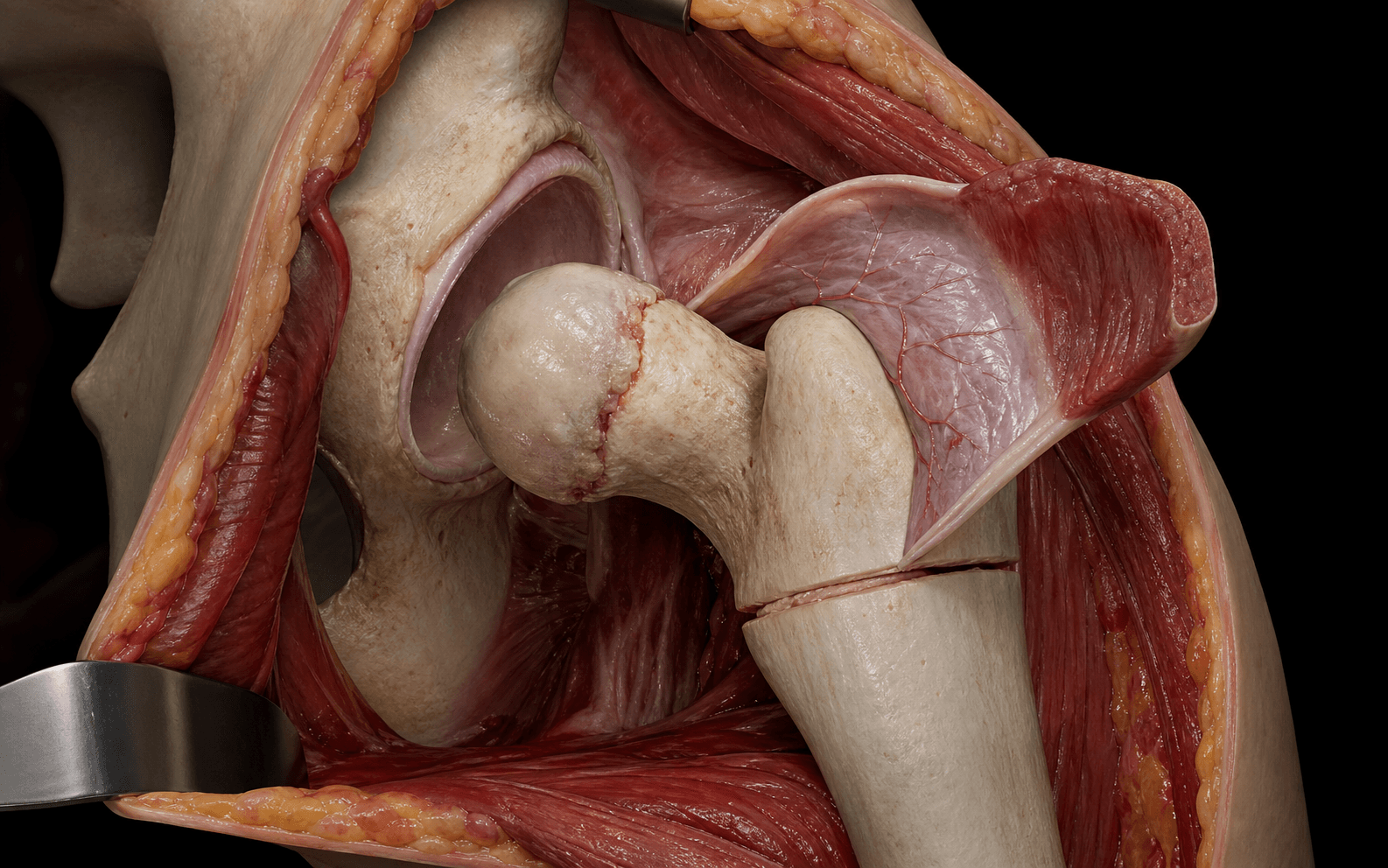
- The Ganz surgical hip dislocation uses a trochanteric flip osteotomy to expose the hip without disrupting the deep branch of the medial femoral circumflex artery (MFCA). The retinacular flap is developed by subperiosteal elevation along the femoral neck, protecting the terminal branches to the epiphysis. Controlled shortening of the femoral neck allows tension-free reduction of the epiphysis.
- Avascular necrosis is the central complication (reported 10 to 25 percent in series) and is directly related to injury to the MFCA terminal branches during flap development or excessive tension during reduction. The learning curve is steep — the procedure should be performed in high-volume centres by surgeons with specific training.
- Post-operative fixation uses 2 to 3 cannulated screws across the physis into the epiphysis, and trochanteric fixation with 2 to 3 cortical screws. Protected weight-bearing continues for 6 to 12 weeks with serial radiographs to monitor physeal healing and AVN.
When & Why
Indication. Symptomatic moderate-to-severe stable SCFE with a Southwick lateral slip angle greater than 30 to 40 degrees, where in-situ pinning would leave a clinically unacceptable cam deformity and femoroacetabular impingement. It is also used in selected acute unstable slips (the patient unable to bear weight) with severe displacement, when anatomic reduction under direct vision is judged feasible and the surgeon has specific training in the technique, and for a symptomatic residual cam after previous in-situ pinning with documented impingement on CT or MR arthrogram. Contraindications. Absolute: a closed physis (consider an intertrochanteric or periacetabular osteotomy instead), active infection, or a surgeon without the specific training and institutional volume to manage the learning curve. Relative: mild slips less than 30 degrees (in-situ pinning remains the standard), unstable slips presenting after 72 hours with established AVN on MRI, and severe medical comorbidities precluding prolonged surgery. The one decision that matters. For a given slip, three broad strategies exist — and the choice turns on the slip severity, the physes, and the surgeon's training:
The standard for mild and many moderate slips — a single central screw across the physis. Safe and reproducible, but a moderate-to-severe slip pinned in situ leaves a large anterolateral cam that drives femoroacetabular impingement and early osteoarthritis.
Anatomic subcapital realignment via a Ganz surgical hip dislocation with a retinacular flap. Restores the head-neck offset while the physis is still open, at the cost of a 10 to 25 percent AVN risk and a steep, volume-dependent learning curve.
Pin now, then arthroscopic or open cam resection once symptomatic impingement develops. Avoids the realignment learning curve but addresses the deformity late and as a second operation.
Why realign. In-situ pinning of a moderate-to-severe slip leaves a large anterolateral cam deformity that causes cam-type femoroacetabular impingement, labral damage and early osteoarthritis. Long-term studies show that slips greater than 30 to 40 degrees carry a high rate of symptomatic impingement within 10 to 15 years. The modified Dunn procedure restores the head-neck offset and eliminates the cam while the physis is still open.
A Southwick slip angle greater than 30 degrees on the lateral radiograph is the common threshold for considering realignment over in-situ pinning; greater than 50 to 60 degrees almost always leaves a clinically significant cam deformity if pinned in situ.
An unstable slip (the patient unable to bear weight even with crutches) already carries a 20 to 40 percent AVN risk with any treatment, including in-situ pinning. The modified Dunn is considered when the slip is severe and anatomic reduction is judged feasible under direct vision — it does not abolish that baseline risk.
Special situations. For an unstable SCFE, operate within 24 to 48 hours once physiologically stable; consider pre-operative traction or a gentle closed reduction under anaesthesia before open realignment, and counsel the family extensively about the elevated AVN risk. Bilateral severe slips are managed as staged procedures 6 to 12 weeks apart (single-stage bilateral surgery only in highly selected, medically stable patients with experienced teams). After failed in-situ pinning with a symptomatic cam, prefer arthroscopic or open osteochondroplasty over revision realignment if the physis has closed. Consent specifically for AVN (10 to 25 percent, higher in unstable slips), trochantric nonunion (3 to 8 percent), chondrolysis (5 to 10 percent), an expected leg-length discrepancy of 1 to 2 cm, infection, nerve injury, and the possibility of future reconstructive surgery. Emphasise that results are volume-dependent and that in-situ pinning with later osteochondroplasty is a valid alternative. Setup. Lateral decubitus on a radiolucent table with the operative hip uppermost; the entire leg is prepped free and a perineal post is used for traction. Position the image intensifier to obtain AP and true lateral (frog-leg equivalent) views intraoperatively. General anaesthesia with muscle relaxation, a regional block (lumbar plexus or femoral) for post-operative analgesia, an arterial line, and a cell saver available.
The Operation
The goal is to anatomically realign the slipped epiphysis at the capital-neck junction while preserving the epiphyseal blood supply, then fix it in the corrected position. The whole operation is built around protecting the deep branch of the medial femoral circumflex artery (MFCA) — the sole supply to the epiphysis — which originates from the profunda femoris (or directly from the femoral artery), runs posteriorly along the intertrochanteric crest and then along the posterolateral femoral neck about 1.5 cm distal to the intertrochanteric line, before giving off 2 to 4 terminal retinacular branches that enter the epiphysis at its posterosuperior and posteroinferior margins. The Ganz surgical hip dislocation exposes the hip without disturbing that vessel, and a subperiosteal retinacular flap carries the terminal branches safely with the epiphysis during realignment.
Operative sequence
- Confirm the lateral position and that the image intensifier gives clear AP and true lateral views.
- Make a straight lateral incision from the iliac crest to the mid-thigh, centred over the greater trochanter, and split the iliotibial band in line.
- Identify the posterior border of the greater trochanter. With an oscillating saw, perform the osteotomy starting just anterior to the posterior edge and exiting distal to the vastus lateralis ridge, taking a 1.5 cm thick wafer of trochanter.
- Reflect the trochanteric wafer anteriorly with the attached vastus lateralis and gluteus medius, preserving the posterior abductor attachment and the MFCA course. Tag the gluteus minimus insertion.
- Expose the capsule. Incise it in a Z-shaped fashion: the superior limb runs along the acetabular rim, the anterior limb along the femoral neck, and the inferior limb is preserved to protect the MFCA.
- Dislocate the hip by flexing, adducting and externally rotating the leg while applying traction.
- Divide the ligamentum teres with curved scissors. The femoral head is now fully exposed.
- With the head dislocated, identify the posterior neck. Using a periosteal elevator, begin subperiosteal elevation at the distal neck just proximal to the intertrochanteric line.
- Develop the flap proximally along the posterolateral neck, staying strictly subperiosteal, until the epiphyseal margin is reached.
- The deep branch of the MFCA and its 2 to 4 terminal retinacular vessels are visualised and protected within the flap. The flap — a fibrous sleeve of terminal MFCA branches, periosteum and reflected capsule — must remain in continuity with the epiphysis.
- With the flap protected, perform a subcapital osteotomy at the physis using a thin oscillating saw or osteotome. Remove a 5 to 10 mm wafer of metaphyseal bone to allow shortening.
- Reduce the epiphysis onto the shortened neck under direct vision. The head should sit flush without step-off and without tension on the flap.
- Confirm reduction with fluoroscopy in AP and lateral projections.
- Fix the epiphysis with 2 to 3 cannulated 6.5 to 7.3 mm screws inserted from the lateral cortex across the physis into the epiphysis, perpendicular to the physis and engaging at least 5 threads in the epiphysis.
- Fix the trochanteric osteotomy with 2 to 3 cortical screws (3.5 or 4.5 mm) with washers, aiming for compression and at least 3 cortices of distal purchase. Add a tension-band cable if bone quality is poor.
- Before final closure, confirm epiphyseal perfusion with laser Doppler or drill-hole bleeding. If flow is lost, release the reduction, add more shortening, or accept slight under-correction.
- Irrigate the joint, close the capsule loosely, reattach the trochanter, and close the iliotibial band and skin over drains.
Mark the osteotomy line with electrocautery before cutting. The posterior starting point is critical — too posterior risks the MFCA and sciatic nerve, too anterior leaves a thin wafer with poor screw purchase. Confirm the exit point is distal to the vastus ridge so the vastus lateralis stays attached.
An osteotomy exiting too posteriorly risks the MFCA and sciatic nerve; a thin trochanteric wafer gives poor screw purchase and trochanteric escape; and excessive proximal extension risks the superior gluteal neurovascular bundle.
Use only blunt elevators and never electrocautery near the posterolateral neck. Develop the flap from distal to proximal in one continuous plane — visible vessel pulsation or bleeding from the flap edge confirms perfusion is intact, and any resistance means you are in the wrong plane, so stop and re-enter subperiosteally.
Thermal injury from electrocautery causes immediate vessel thrombosis and AVN; leaving the periosteum on the bone instead of elevating it with the flap transects the vessels; and over-dissection into the substance of the flap destroys the terminal branches.
If the epiphysis will not reduce without tension on the flap, do not force it — tension on the retinacular vessels is the commonest cause of iatrogenic AVN. Add further controlled shortening (another 3 to 5 mm), or accept a slight under-correction of 5 to 10 degrees; perfusion is more important than perfect anatomy.
Check screw position with an intraoperative arthrogram before closing. One screw in the posterosuperior quadrant and one in the posteroinferior quadrant give the best epiphyseal purchase, and a screw tip within 2 mm of subchondral bone should be backed out and re-angled.
Intraoperative assessment of epiphyseal perfusion — laser Doppler, or direct observation of bleeding from drill holes — confirms retinacular-flap integrity before final fixation. This is the last opportunity to correct a technical error that would otherwise cause AVN.
The whole operation protects the deep branch of the medial femoral circumflex artery, which runs along the posterolateral neck about 1.5 cm distal to the intertrochanteric line and is the sole supply to the epiphysis. Develop the retinacular flap strictly subperiosteally with blunt instruments, never use electrocautery near the posterolateral neck, shorten the neck enough to avoid tension on reduction, and confirm perfusion before fixation. Injury to this vessel is the direct cause of avascular necrosis.
Aftercare & Complications
Rehabilitation | Phase | Timing | Weight-bearing and precautions | Therapy focus | |-------|--------|--------------------------------|---------------| | 1 | 0 to 6 weeks | Touch-down weight-bearing (10 to 20 kg) with crutches; no active abduction, avoid flexion greater than 90 degrees | Isometric quadriceps, gluteal and core activation; passive and active-assisted hip ROM within safe limits | | 2 | 6 to 12 weeks | Progressive to partial then full weight-bearing once trochanteric healing is confirmed | Active abduction and strengthening; stationary bike, pool therapy | | 3 | 3 to 6 months | Full weight-bearing | Progressive resistance and proprioception; return to low-impact sports when strength and ROM are symmetric | | 4 | 6 to 12 months | Full activity | Sport-specific training; contact sports only after radiographic physeal closure and normal strength | Post-operative protocol - DVT prophylaxis: mechanical compression plus LMWH or aspirin for 4 to 6 weeks.
- Analgesia: multimodal — paracetamol, NSAIDs if renal function allows, gabapentinoids, opioid as needed; a regional catheter for 48 to 72 hours in some centres.
- Wound care: drains removed at 24 to 48 hours; sutures or staples out at 14 to 21 days.
- Monitoring: serial AP and frog-lateral radiographs at 2, 6, 12 and 24 weeks, then 6-monthly until physeal closure; MRI at 3 to 6 months if pain or restricted motion persists; clinical leg-length and abductor strength at each visit. An expected shortening of 1 to 2 cm is common and usually well tolerated. Long-term outcome is dominated by AVN — when it is avoided, the procedure gives high survivorship and little osteoarthritis at 10 years. Complications
- Incidence
- 10 to 25 percent overall; higher in unstable slips and inexperienced hands
- Recognition
- Groin or buttock pain 3 to 12 months post-operatively; restricted internal rotation; radiographic sclerosis and collapse of the femoral head
- Prevention and management
- Prevention: strict subperiosteal flap technique, controlled neck shortening, perfusion monitoring, avoid thermal injury. Management: early detection with serial radiographs and MRI; core decompression or vascularised fibular graft in early collapse; salvage arthroplasty or arthrodesis in advanced collapse
- Incidence
- 3 to 8 percent
- Recognition
- Lateral hip pain, Trendelenburg gait, palpable gap or migration on radiographs at 6 to 12 weeks
- Prevention and management
- Prevention: adequate screw purchase (minimum 3 cortices), compression technique, protected weight-bearing until union. Management: revision fixation with cable augmentation or trochanteric advancement; bone grafting for atrophic nonunion
- Incidence
- 5 to 10 percent
- Recognition
- Rapid joint-space narrowing on radiographs within 3 to 6 months; stiffness and pain out of proportion to radiographic changes
- Prevention and management
- Prevention: avoid hardware penetration, minimise joint exposure time, prophylactic antibiotics, gentle retraction. Management: early arthroscopic lavage and synovectomy; intra-articular steroid or viscosupplementation; ultimately arthrodesis or arthroplasty if progressive
- Incidence
- 2 to 5 percent
- Recognition
- Loss of reduction on serial radiographs; increased slip angle; hardware breakage or backing out
- Prevention and management
- Prevention: adequate screw length and thread engagement in the epiphysis; avoid single-screw constructs in severe slips. Management: revision to additional screws or conversion to intertrochanteric osteotomy
- Incidence
- Expected 1 to 2 cm shortening; symptomatic greater than 3 cm in 5 to 10 percent
- Recognition
- Trendelenburg gait, leg-length inequality on block testing, abductor weakness on resisted abduction
- Prevention and management
- Prevention: limit neck resection to 5 to 10 mm; advance the trochanter distally to restore tension. Management: shoe lift for mild discrepancy; trochanteric advancement or distal femoral lengthening for symptomatic cases
- Incidence
- Less than 2 percent
- Recognition
- Wound erythema, drainage, fever, elevated CRP or ESR; deep collection on MRI or ultrasound
- Prevention and management
- Prevention: prophylactic antibiotics, meticulous haemostasis, layered closure. Management: superficial — oral antibiotics and wound care; deep — irrigation and debridement, IV antibiotics, possible hardware retention until union
Viva & Exam Focus
DUNNDUNN — Modified Dunn Procedure principles
GANZGANZ — Surgical hip dislocation steps
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 12-year-old boy presents with an acute unstable SCFE of the left hip. He is unable to bear weight. The lateral slip angle measures 55 degrees. You are considering a modified Dunn procedure. What are the key decision points and how do you counsel the family?”
“During a modified Dunn procedure you have developed the retinacular flap and performed neck shortening. On attempting reduction you notice the epiphysis will not reduce without significant tension on the flap. What do you do?”
“A 13-year-old girl underwent a modified Dunn procedure for a 48-degree stable SCFE six months ago. She now presents with increasing groin pain and a limp. Radiographs show sclerosis and early collapse of the femoral head. What is the diagnosis and how do you manage her?”
Indications
- Moderate-to-severe stable SCFE (Southwick greater than 30 to 40 degrees) where in-situ pinning leaves an unacceptable cam
- Selected severe unstable slips when anatomic reduction is feasible under direct vision
- Symptomatic residual cam after previous in-situ pinning with documented impingement
- Contraindicated with a closed physis, active infection, or an untrained surgeon
Surgical anatomy
- Deep branch of MFCA runs posterolateral on the neck 1.5 cm distal to the intertrochanteric line — protect it
- Retinacular flap carries the terminal MFCA branches — developed strictly subperiosteally
- Trochanteric flip: 1.5 cm wafer, anterior to the posterior edge, exiting distal to the vastus ridge
- Z-shaped capsulotomy preserves the inferior flap containing the MFCA
Critical steps
- Trochanteric flip with vastus lateralis and gluteus medius attached
- Subperiosteal retinacular flap from distal neck proximally — no cautery near the posterolateral neck
- Controlled neck shortening (5 to 10 mm) for tension-free reduction
- Anatomic reduction under direct vision — slight under-correction beats vessel stretch
- 2 to 3 cannulated screws across the physis; confirm with an arthrogram
- Trochanteric fixation with 2 to 3 cortical screws; protected weight-bearing until union
Complications
- AVN: 10 to 25 percent overall; higher in unstable slips and low-volume surgeons
- Trochanteric nonunion: 3 to 8 percent
- Chondrolysis: 5 to 10 percent; avoid hardware penetration
- Leg-length discrepancy: expected 1 to 2 cm shortening
- Fixation failure: 2 to 5 percent
Post-operative
- Touch-down weight-bearing for 6 weeks; progress at 6 to 12 weeks once healing is confirmed
- No active abduction or flexion greater than 90 degrees for 6 weeks
- Radiographs at 2, 6, 12 and 24 weeks; MRI at 3 to 6 months if symptomatic
- Return to sport at 6 to 12 months after physeal closure
Viva pearls
- Unstable severe slip: surgery within 24 to 48 hours; controlled shortening is mandatory
- Tension on the flap: add shortening or accept under-correction — never force reduction
- Confirm perfusion before fixation — the last chance to correct a technical error
- AVN at 3 to 6 months: early MRI, stage, and refer to a hip preservation centre
- Counselling: outcomes are volume-dependent; discuss in-situ pinning as an alternative
Background & Evidence
Pathoanatomy. In a slipped capital femoral epiphysis the epiphysis displaces relative to the metaphysis through the open physis, and when a moderate-to-severe slip is pinned in situ the residual morphology leaves a large anterolateral head-neck offset — the cam lesion. This cam produces cam-type femoroacetabular impingement, labral damage and early osteoarthritis; long-term data show that slips greater than 30 to 40 degrees carry a high rate of symptomatic impingement within 10 to 15 years. The modified Dunn procedure restores the head-neck offset and removes the cam while the physis is still open. Blood supply recap. The epiphysis is supplied almost exclusively by the deep branch of the MFCA; once the physis closes the metaphyseal contribution is lost and the terminal retinacular vessels become the sole supply. This is why any injury to the deep branch or its terminals during flap development or reduction causes AVN — and why the operation is designed around protecting them.
- Southwick lateral slip angle
- Less than 30 degrees
- Typical management
- In-situ pinning is the standard
- Southwick lateral slip angle
- About 30 to 40 degrees
- Typical management
- In-situ pinning; consider realignment if an unacceptable cam or impingement is likely
- Southwick lateral slip angle
- Greater than 40 degrees
- Typical management
- Modified Dunn favoured for anatomic realignment
- Southwick lateral slip angle
- Greater than 50 to 60 degrees
- Typical management
- Modified Dunn; in-situ pinning almost always leaves a clinically significant cam
Key evidence. The Ganz surgical hip dislocation (Ganz, 2001) established that the hip can be fully exposed without avascular necrosis when the MFCA is protected by the retinacular flap — the anatomic foundation of the modified Dunn procedure. Slongo (2010) reported anatomic correction of severe slips with an AVN rate under 10 percent in experienced hands, and Huber (2011) confirmed AVN rates of 10 to 25 percent driven by unstable slips, delayed surgery and excessive tension during reduction. At 10 years, Ziebarth (2017) showed high survivorship and little osteoarthritis when AVN was avoided — confirming that AVN, not the original slip, determines the long-term outcome.
References
Surgical dislocation of the adult hip: a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis
- Original description of the surgical hip dislocation technique using trochanteric flip osteotomy
- Zero AVN in the initial series when the MFCA was protected by the retinacular flap
- Established the anatomic basis for safe dislocation and subcapital realignment
Treatment of slipped capital femoral epiphysis with a modified Dunn procedure
- The modified Dunn procedure achieved anatomic correction in severe SCFE with an AVN rate under 10 percent in experienced hands
Adolescent slipped capital femoral epiphysis treated by a modified Dunn osteotomy with surgical hip dislocation
- AVN rate 10 to 25 percent; risk factors include unstable slips, delayed surgery, and excessive tension during reduction
High survivorship and little osteoarthritis at 10-year follow-up in SCFE patients treated with a modified Dunn procedure
- Ten-year follow-up showed high survivorship and little osteoarthritis when AVN was avoided