Medial opening-wedge or lateral closing-wedge osteotomy of the distal tibia for asymmetric ankle OA | advanced
- The supramalleolar osteotomy corrects the distal tibial joint surface by creating a controlled cut 4 to 6 cm proximal to the ankle joint. In varus ankle OA the medial compartment is overloaded; a medial opening-wedge corrects the TAS angle (tibial anterior surface angle, normal 93 degrees plus or minus 4) and redistributes load onto the preserved lateral compartment.
- A concurrent fibular osteotomy is almost always required. In a medial opening-wedge the fibula must be shortened (oblique osteotomy at the same level, often with a 5 to 10 mm segment resected) so the tibia can open laterally; failure to release the fibula adequately is the commonest cause of under-correction.
- Pre-operative assessment must confirm a mobile subtalar joint, salvageable cartilage in the underloaded compartment (MRI), a correctable deformity on stress views, and that the CORA sits at the ankle (supramalleolar) rather than more proximally. Full-thickness cartilage loss in the compartment you intend to offload onto is a contra-indication.
- The goal is neutral alignment with a congruent talus under the plafond. Over-correction (valgus from an intended varus correction) rapidly degenerates the opposite compartment; under-correction leaves the original overload unchanged. Aim for a TAS of approximately 93 degrees — do NOT over-correct at the ankle as you might at the knee.
When & Why
Indication. Symptomatic asymmetric (eccentric) ankle osteoarthritis with a correctable deformity — varus OA with medial compartment overload and preserved lateral cartilage, or valgus OA with lateral overload and preserved medial cartilage — that has failed non-operative treatment (activity modification, a rocker-bottom shoe or AFO, lateral/medial wedge insole, NSAIDs and an intra-articular corticosteroid injection). The patient is typically young and active (under 55 to 60), wishes to delay or avoid ankle arthrodesis or replacement, has a mobile subtalar joint, and at least 30 degrees of sagittal ankle motion. Absolute indications - Asymmetric ankle OA (Takakura stage II or III) with a correctable deformity and a preserved opposing compartment
- Varus ankle with a TAS angle less than 90 degrees (or valgus with TAS greater than 96 degrees) that remains symptomatic despite non-operative care
- Young, active patient (typically under 55 to 60) wishing to delay arthrodesis or total ankle replacement
- Mobile subtalar joint with at least 30 degrees of sagittal ankle motion Relative indications - Post-traumatic malunion of the distal tibia or plafond contributing to asymmetric loading
- Ankle OA secondary to distal tibial physeal arrest (growth disturbance)
- Periarticular deformity with correctable ankle subluxation
- Patient unsuitable for arthrodesis (bilateral disease, contralateral hindfoot fusion) or TAR (young age, high activity demands) Contra-indications Absolute: - End-stage (stage 4) concentric ankle OA with complete loss of joint space bilaterally — there is no compartment to offload onto
- Rigid subtalar arthritis (the STJ cannot compensate for residual malalignment)
- Active infection (osteomyelitis, septic arthritis) at or near the ankle
- Severe osteoporosis with insufficient bone stock for plate fixation
- Charcot neuroarthropathy or significant peripheral neuropathy with loss of protective sensation Relative: - Rheumatoid arthritis with active inflammatory disease (optimise medically first)
- Active smoking (significantly elevated nonunion risk — insist on cessation)
- BMI greater than 35 (increased wound complication and nonunion rates)
- Previous ankle trauma with extensive scarring compromising the approach
- Diabetes mellitus with peripheral vascular disease The three things you must confirm before listing for SMO. These are the selection gatekeepers — miss one and the operation fails.
A stiff or arthritic STJ cannot compensate for any residual tibiotalar malalignment, and the patient will have persistent pain regardless of how well the osteotomy is performed. Assess clinically and on Broden views or CT.
The compartment you are offloading onto must have intact cartilage. Confirm on MRI (or arthroscopy) — full-thickness loss in the underloaded compartment is a contra-indication, because there is nothing left to load.
On a full-length standing hip-knee-ankle film, the centre of rotation of angulation must sit at or near the ankle joint. A proximal deformity (e.g. tibial plateau malunion) will NOT be corrected by a supramalleolar osteotomy alone.
Opening-wedge or closing-wedge? Both correct the TAS angle back toward neutral; the choice is biomechanical and surgeon-dependent. Medial opening-wedge is the predominant current technique for varus OA.
- Medial opening-wedge
- Anteromedial (along the medial border)
- Lateral closing-wedge
- Anterolateral (over distal fibula and lateral tibia)
- Medial opening-wedge
- Required (tricortical autograft or allograft)
- Lateral closing-wedge
- Not required (inherent bone contact)
- Medial opening-wedge
- 90 to 95 percent (slightly slower)
- Lateral closing-wedge
- 95 to 98 percent (inherent stability)
- Medial opening-wedge
- High — adjustable wedge under fluoroscopy
- Lateral closing-wedge
- Pre-calculated wedge — less adjustable intra-operatively
- Medial opening-wedge
- Yes — shortening / oblique with segment resection
- Lateral closing-wedge
- Yes — at the same level
- Medial opening-wedge
- Low
- Lateral closing-wedge
- Higher (anterior compartment dissection; 1 to 5 percent transient palsy)
- Medial opening-wedge
- Preserved (opens, does not remove bone)
- Lateral closing-wedge
- Reduced (wedge of bone resected)
- Medial opening-wedge
- Predominant technique in most centres
- Lateral closing-wedge
- Historical; used when a lateral approach is preferred
Consent specifically for nonunion (2 to 8 percent), under- or over-correction (5 to 15 percent), infection (1 to 3 percent), neurovascular injury including transient peroneal nerve palsy (1 to 3 percent), hardware irritation requiring removal (10 to 25 percent), and the possibility of eventual conversion to ankle arthrodesis or replacement if arthritis progresses. Setup. Supine on a radiolucent table; a sandbag under the ipsilateral buttock can help present the medial ankle. Prep the ipsilateral iliac crest into the field if autograft is planned. Thigh tourniquet to 250 mmHg. Position the image intensifier for true AP, lateral and mortise views before draping — fluoroscopy is used repeatedly throughout. Single-dose IV cefazolin 2 g at induction.
The Operation
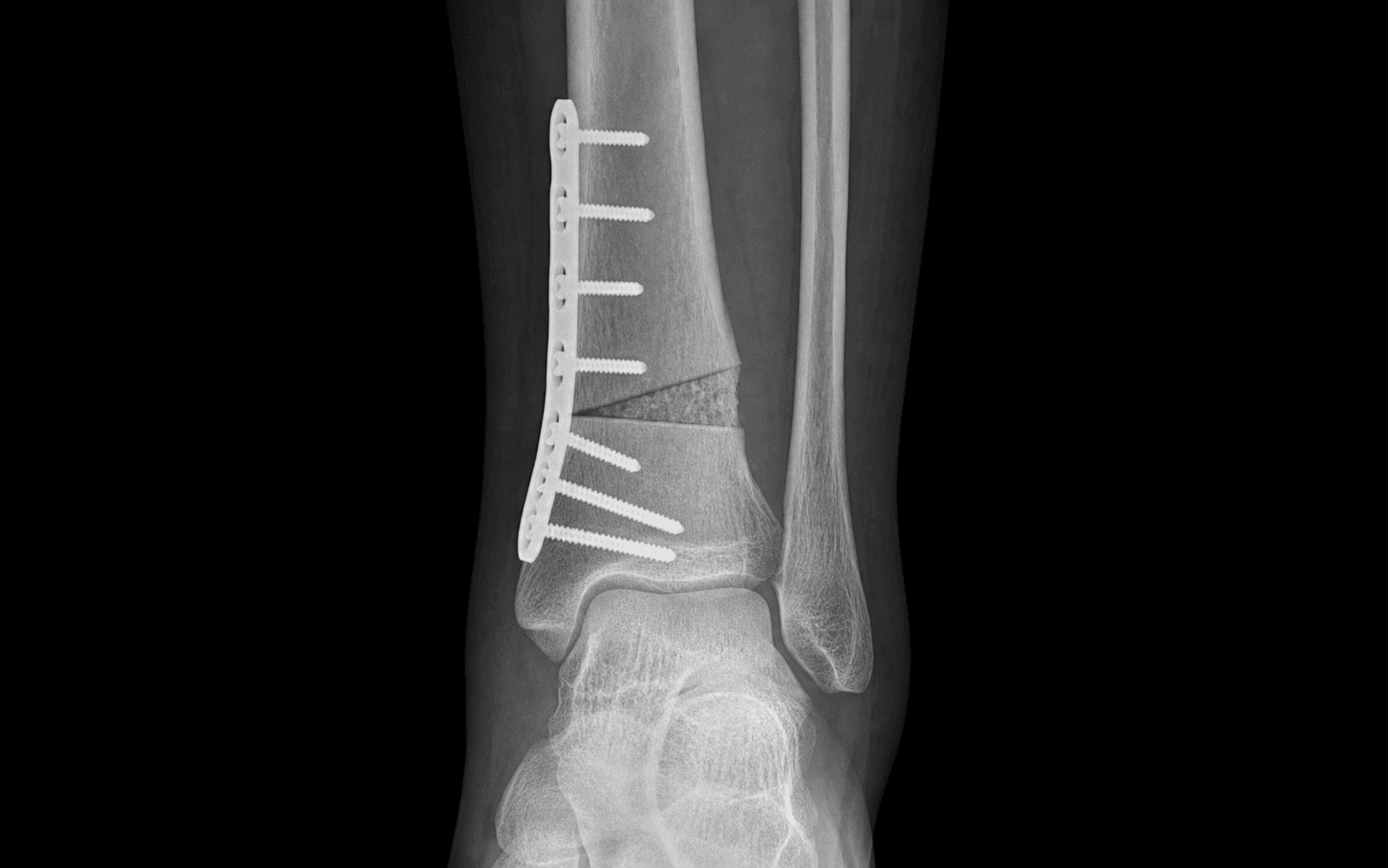
The goal: through an anteromedial approach, expose the distal tibial metaphysis 4 to 6 cm above the plafond, perform a controlled incomplete osteotomy with the lateral cortex as a greenstick hinge, shorten the fibula at the same level so the tibia is free to open, correct the TAS angle to neutral, fill the defect with structural graft, and lock a contoured plate across it — restoring a congruent talus under a neutral plafond.
Operative sequence — medial opening-wedge osteotomy
- Supine on a radiolucent table, sandbag under the ipsilateral buttock to present the medial ankle; iliac crest prepped if autograft is planned.
- Thigh tourniquet to 250 mmHg, exsanguinate and inflate before preparation. Image intensifier positioned for true AP, lateral and mortise views — confirm a true mortise view is achievable before draping.
- Longitudinal incision along the anteromedial border of the distal tibia, centred over the planned osteotomy 4 to 6 cm proximal to the medial malleolus, about 8 to 10 cm long.
- In the subcutaneous plane, identify and protect the saphenous vein and nerve running along the medial subcutaneous border of the tibia.
- Deepen to the fascia over tibialis anterior; incise it longitudinally and retract the tibialis anterior tendon and muscle belly anteriorly.
- The anterior tibial neurovascular bundle and deep peroneal nerve lie beneath tibialis anterior — identify them and protect with a Hohmann retractor placed on the lateral subperiosteal surface.
- Expose the medial distal tibia subperiosteally, elevating only enough periosteum to seat the plate; avoid excessive stripping, which compromises osteotomy blood supply.
- Under fluoroscopy, score the osteotomy line on the medial cortex 4 to 6 cm proximal to the joint and parallel to the tibial plafond.
- Insert two K-wires parallel to the planned line, perpendicular to the shaft, as direction guides — confirm on AP and lateral that they are parallel to the joint and not heading into it.
- Separate longitudinal incision over the lateral fibula at the level of the tibial osteotomy; protect the superficial peroneal nerve branches.
- Oblique osteotomy of the fibula at the same level with an oscillating saw; resect a 5 to 10 mm segment so the tibia is free to open laterally without the fibula acting as a tension band.
- Confirm under fluoroscopy that the fibula is completely divided and is not blocking correction.
- With an oscillating saw, cut from the medial cortex and advance laterally toward — but not through — the lateral cortex, leaving it intact as a hinge.
- Advance to within 2 to 3 mm of the lateral cortex, then complete it with multiple 2.5 mm drill holes and gentle osteotome taps so the lateral cortex fractures in a controlled greenstick fashion (not a complete division).
- Confirm the cut is complete by inserting a thin osteotome and gently levering — the medial side should open. If resistance is met, the lateral cortex is still intact and must be perforated further. Keep the osteotomy at least 4 cm proximal to the joint.
- Open gradually with laminar spreaders under fluoroscopy until the corrected TAS angle is reached (approximately 93 degrees) and the talus sits congruently under the plafond.
- Measure the medial defect. Prepare a tricortical iliac crest autograft (or fresh-frozen structural allograft) to match; for defects less than 5 mm, cancellous chips or synthetic substitute may supplement, but a structural graft is preferred for defects greater than 5 mm.
- Insert the graft with its cortical surface oriented to resist compression; confirm position fluoroscopically. Keep the spreader in place until the plate is applied.
- Apply an anatomically contoured anteromedial locking plate across the osteotomy — typically 3 to 4 screw holes proximal and 2 to 3 distal.
- Insert locking screws under fluoroscopy, proximal first then distal, checking each screw length on lateral fluoroscopy so that no distal screw penetrates the ankle joint.
- Remove the spreader and confirm the correction holds: TAS on AP, TLS on lateral, talar congruency on the mortise view. Check ankle dorsiflexion and plantarflexion are preserved and the fibular osteotomy site is stable.
- Irrigate thoroughly. Close periosteum and deep fascia over the plate with absorbable sutures, then subcutaneous layer and skin in layers.
- Apply a sterile, well-padded below-knee posterior splint with the ankle in neutral.
Lateral closing-wedge — the alternative, in brief. Through an anterolateral incision over the distal tibial metaphysis: osteotomise the fibula at the same level (essential, so the lateral tibial cortices can close and the distal fragment can translate), mark the wedge with K-wires under fluoroscopy, resect a calculated lateral wedge with the saw, close and compress the fragments, and fix with an anterolateral locking plate — no graft is needed because of inherent bone contact. Its specific risks are a higher deep peroneal nerve palsy rate (1 to 5 percent, usually transient) from anterior compartment dissection, and a slightly higher lateral wound breakdown rate on the thin distal tibial skin.
- Incomplete fibular osteotomy — the intact fibula acts as a tension band and blocks correction; it is the single commonest cause of under-correction in opening-wedge SMO. Resect a 5 to 10 mm segment and confirm the fibula is freely mobile before plating.
- Over-penetration of the saw through the lateral cortex — risks the deep peroneal nerve, anterior tibial vessels and the posterior tibial neurovascular bundle. Stop 2 to 3 mm short and complete the cortex with drill holes.
- Distal screws entering the ankle joint — entirely preventable: check every screw on AP and lateral fluoroscopy before closing.
Open the osteotomy incrementally and read the TAS angle on each opening. Stop at approximately 93 degrees on the AP mortise view with the talus congruent under the plafond. Cut the tricortical graft to a press-fit so it holds the correction without relying on the plate alone, and confirm the final TAS, TLS and talar congruence on AP, lateral and mortise views before closing.
Unlike a high tibial osteotomy, where a few degrees of valgus is accepted, the ankle demands neutral alignment. Over-correcting a varus ankle into valgus simply shifts overload to the lateral compartment and accelerates its degeneration — one of the commonest reasons for early revision to arthrodesis. Aim for a TAS of about 93 degrees, with a tolerance of plus or minus 2 degrees.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy and weight-bearing | |-------|--------|-----------------|----------------------------| | 1 | 0 to 2 weeks | Below-knee posterior splint or cast, ankle neutral, non-weight-bearing | Elevation, toe active range of motion only; wound check at 10 to 14 days | | 2 | 2 to 6 weeks | Removable CAM boot | Touch weight-bearing (10 to 15 kg); gentle active dorsiflexion/plantarflexion in the boot; stationary cycling without resistance | | 3 | 6 to 12 weeks | CAM boot, weaning | Partial to full weight-bearing as callus appears on the 6-week film; progressive active and active-assisted ROM, subtalar mobilisation | | 4 | 3 to 9 months | None (night splint if needed) | Calf raises, resistance bands, proprioception; impact sport only once union is confirmed and strength recovered | Return to function. Office or sedentary work by 4 to 6 weeks; light or standing duties by 8 to 12 weeks; heavy manual work by 12 to 16 weeks or longer. Driving once an emergency stop is safe — typically 8 to 12 weeks for the right (driving) ankle. Low-impact sport (swimming, cycling) from 12 to 16 weeks; running and impact sport from 6 to 9 months once union is confirmed. Radiographs at 6 weeks (early callus), 3 months (confirm union), 6 and 12 months, then annually. Offer hardware removal at 12 to 18 months once union is solid — hardware irritation is the commonest reason for a planned return to theatre. Complications
- Incidence
- 2 to 8 percent
- Recognition
- Pain at the osteotomy site beyond 4 to 6 months; no trabecular bridging on serial films; hardware loosening or breakage
- Prevention and management
- Stable locking-plate fixation, adequate graft, protected weight-bearing for 6 to 8 weeks, smoking cessation, optimise vitamin D. Established nonunion at 6 to 9 months: revision fixation with iliac-crest autograft; bone stimulant as adjunct
- Incidence
- 5 to 15 percent
- Recognition
- Residual varus or valgus tilt on post-operative films (TAS still abnormal); persistent pain in the originally overloaded compartment
- Prevention and management
- Accurate templating; intra-operative fluoroscopic TAS check before final fixation; ensure the fibular osteotomy is adequate. Mild (2 to 3 degrees): observe. Significant: revision osteotomy or conversion to arthrodesis
- Incidence
- 3 to 10 percent
- Recognition
- Excessive valgus after correcting varus (or vice versa); new pain in the opposite compartment
- Prevention and management
- Fluoroscopic confirmation of TAS near 93 degrees; do not over-correct at the ankle. Early revision osteotomy; if the newly overloaded compartment has degenerated, conversion to arthrodesis
- Incidence
- 10 to 25 percent
- Recognition
- Palpable plate or screw heads; pain with direct pressure or shoe wear
- Prevention and management
- Low-profile plates on the flat medial surface; avoid long screw heads. Remove plate and screws once union is confirmed (12 to 18 months)
- Incidence
- 1 to 5 percent (lateral approach)
- Recognition
- Foot drop or weak dorsiflexion; numbness in the first web space; weak EHL
- Prevention and management
- Identify and protect the nerve during the lateral approach; subperiosteal Hohmann retractors. Transient: AFO, expect recovery in 3 to 6 months; nerve conduction at 6 weeks. Persistent at 4 to 6 months: explore and neurolyse
- Incidence
- 1 to 3 percent
- Recognition
- Superficial: erythema, warmth, discharge. Deep: fever, raised CRP, dehiscence, draining sinus, hardware exposure
- Prevention and management
- Single-dose IV antibiotics at induction; meticulous handling; secure layered closure. Superficial: oral antibiotics and wound care. Deep: washout, IV antibiotics, culture-directed therapy; hardware removal if infection persists
- Incidence
- Variable
- Recognition
- New or worsening joint-space narrowing on serial films; increasing weight-bearing pain
- Prevention and management
- Accurate correction to neutral; select stage II to III patients with a mobile STJ; address concomitant hindfoot deformity. Convert to arthrodesis or TAR when conservative measures fail
- Incidence
- 2 to 5 percent
- Recognition
- Pain at the fibular osteotomy site; lateral ankle discomfort
- Prevention and management
- Ensure good bone contact; consider fibular plating in high-risk patients. Most fibular nonunions are asymptomatic; symptomatic cases: revision with bone grafting
Viva & Exam Focus
ALIGNEDALIGNED — SMO planning
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 48-year-old man has a 3-year history of progressive right ankle pain worsened by walking. He has a varus hindfoot, a TAS angle of 83 degrees, an 8-degree talar tilt, medial compartment narrowing with a preserved lateral compartment, 35 degrees of sagittal motion and a mobile subtalar joint. How do you manage him?”
“During a medial opening-wedge SMO, after grafting and plating, fluoroscopy shows a TAS of only 88 degrees — your target was 93. The fibula has been osteotomised. What has likely happened and what do you do?”
“A 55-year-old woman with valgus ankle OA has a TAS of 98 degrees, lateral compartment narrowing with medial preservation, a BMI of 38, a 20 pack-year smoking history and well-controlled type 2 diabetes. How do you counsel her regarding SMO?”
Selection
- Asymmetric ankle OA: varus (medial narrowing, lateral preservation) or valgus (lateral narrowing, medial preservation)
- Ideal: young (under 55 to 60), active, Takakura stage II to III, mobile STJ, at least 30 degrees sagittal motion, correctable deformity
- Contra-indicated: end-stage concentric OA, rigid STJ arthritis, active infection, Charcot neuropathy, full-thickness loss in the opposite compartment
The angles
- TAS (AP): normal 93 degrees (range 89 to 97); less than 90 is varus, greater than 96 is valgus — the angle SMO corrects
- TLS (lateral): normal 80 degrees (range 76 to 84) — assesses sagittal deformity
- Takakura: I narrowing no malleolar contact; II talus contacts malleolus no cyst; III contact with cyst; IV complete medial joint-space obliteration
Planning
- Weight-bearing AP and lateral for TAS and TLS; full-length hip-knee-ankle film to find the CORA
- MRI to confirm the opposite compartment is salvageable; stress views for ligamentous contribution and correctability
- Correction wedge: target TAS 93 degrees; wedge base equals osteotomy height times the tangent of the correction angle
Operation (opening-wedge)
- Anteromedial approach; osteotomy 4 to 6 cm proximal, parallel to the plafond
- Saw to within 2 to 3 mm of the lateral cortex, then 2.5 mm drill holes for a controlled greenstick hinge
- Fibular osteotomy at the same level with a 5 to 10 mm segment resection
- Open to a TAS of about 93 degrees; tricortical graft; anteromedial locking plate; check every screw on AP and lateral
Danger zones
- Incomplete fibular osteotomy = under-correction — the intact fibula blocks correction in both techniques
- Over-penetration of the saw risks the deep peroneal nerve, anterior tibial vessels and posterior tibial bundle
- Over-correction past 93 degrees overloads the opposite compartment — aim neutral, NOT slight valgus
- Distal screws entering the joint — check every screw on fluoroscopy before closing
Complications
- Nonunion 2 to 8 percent (higher in smokers, diabetics, opening-wedge)
- Under-correction 5 to 15 percent; over-correction 3 to 10 percent
- Hardware irritation 10 to 25 percent (commonest reason for planned re-operation)
- Deep peroneal nerve palsy 1 to 5 percent with the lateral approach (usually transient)
Rehabilitation
- 0 to 2 weeks: non-weight-bearing in a splint, ankle neutral
- 2 to 6 weeks: CAM boot, touch weight-bearing, active ROM
- 6 to 12 weeks: progress to full weight-bearing, wean boot, formal physiotherapy
- Impact sport from 6 to 9 months once union is confirmed
SMO vs arthrodesis vs TAR
- SMO: joint-preserving for eccentric OA in young active patients; delays fusion or replacement
- Arthrodesis: definitive pain relief, sacrifices motion, alters gait; gold standard for end-stage OA
- TAR: preserves motion, good for moderate activity; prosthetic longevity concerns in younger patients
- SMO is a time-buying procedure — it does not preclude later arthrodesis or TAR
Background & Evidence
Rationale and biomechanics. The supramalleolar osteotomy redistributes joint contact pressures by realigning the distal tibial articular surface relative to the talus. In varus ankle OA the medial compartment bears disproportionate load; after a medial opening-wedge correction, contact pressure shifts laterally toward the preserved cartilage. Biomechanical studies show that a 10-degree correction of the TAS angle can shift the centre of contact pressure by 10 to 20 percent of the tibiotalar surface area. Non-operative measures manage symptoms in early asymmetric OA but do not halt progression, because the eccentric mechanical abnormality persists and keeps driving degeneration of the overloaded compartment — SMO addresses that mechanical cause rather than the symptom alone. The radiographic angles. - Tibial anterior surface (TAS) angle — on the weight-bearing AP ankle radiograph, the angle between the anatomical axis of the tibia and the distal tibial joint surface. Normal is about 93 degrees (range 89 to 97). Less than 90 indicates varus tilt; greater than 96 indicates valgus tilt. This is the primary angle SMO corrects. (Do not confuse it with the tibial plateau angle / MPTA, which is proximal and relevant to high tibial osteotomy, not SMO.)
- Tibial lateral surface (TLS) angle — on the weight-bearing lateral film, the angle between the tibial axis and the distal articular surface. Normal is about 80 degrees (range 76 to 84). An abnormal TLS indicates sagittal plane deformity (recurvatum or procurvatum) that may need additional correction.
- Talar tilt — between the plafond and the talar dome on the AP view. In varus OA the talus tilts into the medial compartment; after SMO it should sit congruently under the corrected plafond. Takakura staging of varus ankle OA.
- Radiographic features
- Narrowing of the medial joint space but no contact of the talus with the medial malleolus
- Typical management
- Conservative; activity modification, orthotic, injection
- Radiographic features
- Talus contacts the medial malleolus without subchondral cyst formation
- Typical management
- Conservative first; SMO if it fails
- Radiographic features
- Contact with the medial malleolus and subchondral cyst formation (IIIa early, IIIb advanced)
- Typical management
- Supramalleolar osteotomy — the prime indication
- Radiographic features
- Complete obliteration of the medial joint space (concentric end-stage disease)
- Typical management
- Arthrodesis or total ankle replacement — SMO is not appropriate
The fibula and its role. The fibula is the lateral strut of the mortise and a key mechanical constraint. In a medial opening-wedge, the intact fibula acts as a tension band resisting lateral opening — so an oblique osteotomy at the same level (often with a 5 to 10 mm segment resected) releases this constraint. In a lateral closing-wedge, the fibula must be osteotomised at the same level so the lateral tibial cortices can appose and the distal fragment can translate medially. A Z-osteotomy or step-cut controls shortening precisely. Inadequate fibular release is the commonest technical cause of under-correction. Outcomes and survivorship. In well-selected patients, approximately 70 to 85 percent report good to excellent results at 5 to 7 years. Krähenbühl's series reported 71 percent good or excellent outcomes with survivorship (free of arthrodesis) of 79 percent at 10 years and 67 percent at 15 years; Takakura stage IV disease and subtalar arthritis were the strongest predictors of failure. Tanaka's varus-OA series showed 73 percent excellent or good results at a mean 8.3 years, better in stage II disease. A 2023 systematic review (547 patients) found a mean AOFAS improvement of 33.2 points, a mean TAS correction of 9.4 degrees and a complication rate of 12.1 percent (nonunion 3.2 percent). Special situations. Where the hindfoot deformity is multiplanar — a varus plafond tilt plus a varus heel — an isolated SMO under-corrects, and a concurrent medial-displacement (Dwyer) calcaneal osteotomy is added through a separate lateral incision; combined correction gives better multiplanar alignment, with survivorship around 80 percent at 7 years in stage II disease. After plafond malunion, pre-operative CT is essential — SMO corrects the coronal deformity but does not address intra-articular step-off. In chronic lateral ligament insufficiency with progressive valgus OA, SMO may be combined or staged with ligament reconstruction. Revision SMO is demanding (hardware removal, scarred biology) and the goals are unchanged: a neutral TAS with a congruent talus.
References
Mid- to Long-term Results of Supramalleolar Osteotomy
- Retrospective review of 46 supramalleolar osteotomies with minimum 5-year follow-up (mean 9.5 years)
- 71% of patients had a good or excellent clinical outcome; survivorship was 79% at 10 years and 67% at 15 years
- Takakura stage IV disease and subtalar joint arthritis were significant predictors of progression to arthrodesis
Realignment surgery as alternative treatment of varus and valgus ankle osteoarthritis
- Prospective series of 35 consecutive patients with post-traumatic asymmetric ankle OA treated with lower leg and hindfoot realignment surgery
- Significant improvement in AOFAS hindfoot score at mean 5.6-year follow-up; outcome correlated with preoperative Takakura stage
- No patient with stage IV disease achieved a good result, confirming that realignment surgery is not appropriate for end-stage OA
Supramalleolar osteotomy for the treatment of ankle osteoarthritis leads to favourable outcomes and low complication rates at mid-term follow-up: a systematic review
- Systematic review of 18 studies (547 patients) reporting clinical and radiographic outcomes after supramalleolar osteotomy for ankle OA
- Mean AOFAS score improved by 33.2 points post-operatively; mean TAS angle correction of 9.4 degrees achieved
- Overall complication rate was 12.1%; nonunion rate 3.2%; most studies were Level IV evidence highlighting the need for higher-quality prospective data
Supramalleolar osteotomy for the treatment of distal tibial angular deformities and arthritis of the ankle joint
- Series of 42 patients with distal tibial angular deformities and secondary ankle arthritis treated with supramalleolar osteotomy
- All patients had significant improvement in pain scores and tibiotalar alignment at mean 4.5-year follow-up
- Two patients developed delayed union requiring revision bone grafting; no nonunions in the final cohort
Low tibial osteotomy for varus-type osteoarthritis of the ankle
- Retrospective series of 26 ankles in 25 patients with varus-type ankle OA treated with low tibial valgus opening-wedge osteotomy
- Mean follow-up 8.3 years; 73% of ankles achieved excellent or good clinical results with significant pain and function score improvement
- Superior outcomes in ankles with preoperative Takakura stage II disease; 11 ankles with progressive arthritis at long-term follow-up