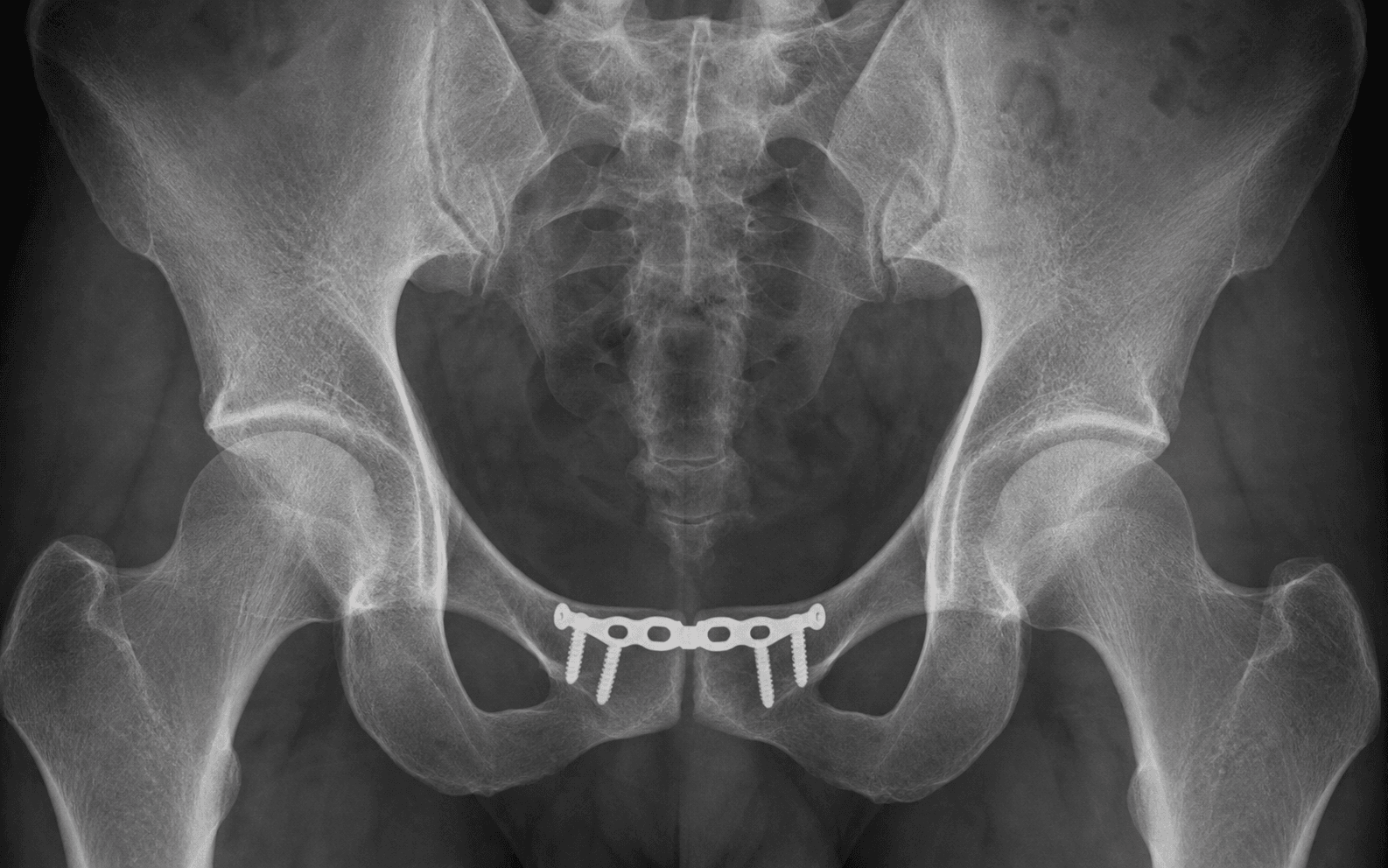
Anterior pelvic ring ORIF · open-book (APC-II/III) injuries
- Symphyseal diastasis greater than 2.5 cm on an AP pelvis with external rotation of the hemipelves indicates an open-book (APC) injury that requires anterior stabilisation once posterior ring stability is confirmed or addressed.
- The corona mortis is an anomalous anastomosis between the external iliac (or inferior epigastric) and obturator vessels that crosses the superior pubic ramus 5–7 cm lateral to the symphysis in up to 30 percent of patients — it must be identified and ligated before retraction or drilling, or its unseen division causes catastrophic bleeding.
- Posterior ring instability is present in the majority of patients with symphyseal diastasis greater than 2.5 cm; anterior plating alone fails in up to 30 percent of cases if the posterior ring is not reduced and stabilised (SI screws or posterior plating).
- The Pfannenstiel approach elevates the rectus abdominis insertions off the pubic tubercles; the bladder must be decompressed with a Foley catheter and protected with a malleable retractor throughout reduction and plating.
- A single superior 3.5 mm or 4.5 mm reconstruction plate (6- or 8-hole) with three screws on each side suffices when the posterior ring is stable; double plating (superior plus anterior) is reserved for highly comminuted or osteoporotic bone.
- Bladder or urethral injury coexists in up to 15 percent of open-book injuries, so a preoperative CT cystogram and urology review are mandatory before symphyseal plating.
When & Why
Indication. Open reduction and anterior plating of the pubic symphysis is performed for a disrupted symphyseal joint that is part of an unstable pelvic ring — the classic open-book (anteroposterior compression, APC) injury. The operation restores the anterior pelvic ring, but only as one half of a ring that must be stable at the back as well. Absolute indications
- Symphyseal diastasis greater than 2.5 cm on the AP pelvis with clinical or radiographic pelvic ring instability (open-book / APC-II or APC-III pattern).
- Combined anterior and posterior pelvic ring injury requiring anterior stabilisation to restore ring continuity.
- Open pelvic injury with symphyseal disruption needing debridement and stabilisation.
- Associated bladder or urethral injury requiring simultaneous repair and symphyseal stabilisation. Relative indications
- Diastasis of 1.5–2.5 cm with persistent pain or instability after non-operative management with a pelvic binder.
- A young patient with high functional demand and residual symphyseal pain after conservative treatment.
- A polytrauma patient in whom early mobilisation is critical and anterior plating facilitates nursing and respiratory care. Contraindications. Absolute: haemodynamic instability requiring damage-control external fixation only (convert later); active pelvic or abdominal infection; severe osteoporosis or bone loss precluding stable screw purchase. Relative: a patient too unstable for prolonged positioning; pregnancy in the second or third trimester (consider external fixation until delivery); a pre-existing severe abdominal wall hernia or a heavily scarred prior Pfannenstiel incision. The one principle that governs everything. Whatever you do at the front of the ring, isolated anterior plating fails when the back of the ring is unstable. Implant failure runs 5–15 percent when posterior ring instability is not addressed and drops below 5 percent with concurrent posterior stabilisation. So confirm and plan the posterior ring (percutaneous SI screws preferred) before or during the same sitting as the anterior plate. Consent specifically for bleeding from the corona mortis or obturator vessels, bladder or urethral injury, infection (3–8 percent), heterotopic ossification (10–25 percent), chronic symphyseal pain or non-union (5–10 percent), and the possibility of staged posterior fixation and a second anaesthetic. Setup. Supine on a radiolucent table, both arms abducted or tucked, with a small sacral bump to improve access to the symphysis; the table must allow full inlet, outlet and Judet views from both sides. General endotracheal anaesthesia with muscle relaxation. Wide skin prep from xiphisternum to mid-thigh including the perineum. Insert a Foley catheter before incision and confirm bladder decompression; have a vascular set, blood products and cell salvage available.
The Operation
The goal is to expose the symphysis through a Pfannenstiel approach, protect the bladder and the corona mortis, reduce the diastasis anatomically, and stabilise the anterior ring with a contoured reconstruction plate — always in the context of a posterior ring that is stable or simultaneously fixed. The exposure (Steps 2–4) is the heart of the operation.
Operative sequence
- Supine on a radiolucent table, both arms abducted or tucked, small sacral bump; the table must allow full inlet, outlet and Judet views.
- General anaesthesia with muscle relaxation; consider an epidural for postoperative analgesia in isolated injuries.
- Wide skin prep from xiphisternum to mid-thigh including the perineum.
- Insert a Foley catheter before incision and confirm the bladder is decompressed; have a vascular set, blood products and cell salvage available.
- Confirm AP, inlet and outlet fluoroscopy from both sides before draping.
- Make a transverse Pfannenstiel incision 2 cm above the pubic symphysis, extending 8–12 cm laterally.
- Divide the subcutaneous fat, identify the linea alba, and incise it in the midline.
- Develop the space of Retzius (the extraperitoneal plane between rectus abdominis and transversalis fascia, with the bladder lying immediately posterior) bluntly.
- Place a self-retaining retractor (Bookwalter or Omni-Tract) with blades on the rectus edges; keep a malleable retractor on the bladder throughout the case.
- Elevate the rectus abdominis insertions sharply from the superior aspect of the pubic tubercles with electrocautery or a periosteal elevator; tag each insertion with heavy non-absorbable suture for later repair.
- Continue subperiosteal elevation laterally along the superior pubic ramus for 6–8 cm on each side, staying on bone to protect the obturator neurovascular bundle.
- Identify and protect the spermatic cord (male) or round ligament (female) crossing just lateral to the pubic tubercle — retract it laterally.
- Deliberately look for the corona mortis 5–7 cm lateral to the symphysis on the superior ramus — an anomalous anastomosis between the external iliac/inferior epigastric and obturator vessels present in 20–30 percent of patients.
- If a vessel crosses the ramus, ligate it proximally and distally with clips or ties before any retraction or drilling.
- Continue subperiosteal elevation under direct vision, protecting the obturator bundle as it exits the obturator canal 2–3 cm lateral to the symphysis.
- Apply pointed reduction clamps (or a Weber clamp) to the pubic tubercles and reduce the diastasis under direct vision.
- Confirm anatomic reduction on AP, inlet and outlet views before placing any screw.
- In chronic or severely displaced injuries, use a Schanz pin in each iliac crest as a joystick to control rotation; hold the reduction with a pointed clamp or provisional K-wire.
- If the posterior ring is unstable, reduce and provisionally stabilise it first (percutaneous SI screws) before finalising the anterior plate.
- Select a 6- or 8-hole 3.5 mm or 4.5 mm reconstruction plate and contour it to the superior surface of the symphysis, placed slightly anterior to the midline to avoid the symphyseal disc.
- Insert three bicortical screws on each side; measure length carefully and confirm with fluoroscopy to avoid bladder or urethral penetration.
- In osteoporotic bone or highly comminuted injuries, add a second anterior 3.5 mm plate (double plating) for added stability.
- Irrigate the wound; reattach the rectus insertions to the plate or bone with heavy non-absorbable sutures — this prevents abdominal wall hernia and maintains core stability.
- Close the linea alba in two layers, then subcutaneous tissue and skin; apply a sterile dressing.
- If posterior ring instability was identified, perform percutaneous SI screw fixation (or posterior plating) in the same sitting, or as a staged procedure once the patient is physiologically stable.
- Anterior plating alone fails in up to 30 percent of cases when the posterior ring is left unstabilised.
Before any lateral ramus retraction or drilling, identify the corona mortis 5–7 cm lateral to the symphysis. This anomalous anastomosis between the external iliac/inferior epigastric and obturator vessels is present in 20–30 percent of patients; dividing it unseen causes rapid, difficult-to-control retroperitoneal bleeding that can exceed 1 L within minutes. Ligate it under direct vision, dissect the superior ramus only under direct vision, and keep a low threshold for vascular surgery assistance.
Decompress the bladder with a Foley catheter before the incision. Once in the space of Retzius, place a malleable retractor directly on the bladder and have the assistant hold it gently posteriorly for the entire case — this protects the bladder during reduction manoeuvres and screw placement. Re-confirm bladder position by direct vision before each clamp and screw.
Symphyseal diastasis greater than 2.5 cm almost always means an APC-III or combined injury with posterior ring disruption. Stabilise the posterior ring (percutaneous SI screws or posterior plating) before or during the same procedure as the anterior plate — isolated anterior plating fails by fatigue at 3–6 months when the posterior ring is left unstable.
The six structures that can hurt you during this approach, and how to protect each:
An anomalous vessel crossing the superior pubic ramus 5–7 cm lateral to the symphysis in 20–30 percent of patients, linking the external iliac or inferior epigastric system to the obturator vessels. Division unseen causes rapid blood loss that can exceed 1 L within minutes. Identify it under direct vision before retractors or drilling and ligate with clips or ties; keep vascular surgery on standby.
Up to 15 percent of APC injuries have an associated bladder rupture or urethral injury. Watch for blood at the meatus, a high-riding prostate, perineal haematoma or inability to pass a Foley — a CT cystogram is mandatory. Decompress the bladder before incision and protect it with a malleable retractor; obtain urology input for any suspected injury before plating.
Diastasis greater than 2.5 cm almost always indicates an APC-III or combined injury with sacral fracture or SI joint disruption. Anterior plating alone then fails with recurrent diastasis and chronic pain. Assess posterior stability with inlet/outlet views, CT and stress examination under anaesthesia, and stabilise the posterior ring before or with the anterior plate.
The rectus insertions must be elevated sharply from the pubic tubercles to expose the symphysis; overzealous stripping causes avulsion or abdominal wall hernia. Tag the insertions with heavy suture before elevation and reattach them securely to the plate or bone at closure with a two-layer linea alba repair.
The spermatic cord in males and the round ligament in females cross the inguinal canal just lateral to the pubic tubercle and must be identified and protected during the Pfannenstiel approach. Injury risks testicular ischaemia, hernia or chronic pain; in females round ligament division is acceptable but should be documented.
Continued micromotion from an unstabilised posterior ring causes fatigue failure of the anterior plate at the symphysis, usually within 3–6 months. Confirm posterior stability intraoperatively with stress views, use at least a 6-hole plate with three screws on each side when posterior fixation is performed, and consider double plating in osteoporotic or comminuted bone.
Aftercare & Complications
Rehabilitation. Weight-bearing is dictated by posterior ring stability, not the anterior plate alone. | Phase | Timing | Weight-bearing & immobilisation | Therapy & milestones | |-------|--------|---------------------------------|----------------------| | Immediate | Day 0–7 | Bed to chair on day 1; touch-down weight-bearing on the affected side if a unilateral injury, or weight-bearing as tolerated if the posterior ring is stable | LMWH for DVT prophylaxis from day 1; Foley for 48–72 h; drains out at 48 h; multimodal analgesia | | Early | Week 1–6 | Touch-down or partial weight-bearing (20 kg) for 6 weeks if the posterior ring was unstable; avoid hip flexion beyond 90 degrees and adduction | Isometric quads and gluteals from day 1; gentle hip ROM from week 2; core and pelvic floor from week 4 | | Late | Week 6–12+ | Progress to full weight-bearing at 6–12 weeks once radiographs confirm stability | Low-impact activity at 3 months; running and sport at 6 months if united and pain-free | Most patients return to desk work by about 6 weeks and to heavy manual work by 12–16 weeks. Review AP, inlet and outlet radiographs at 2, 6 and 12 weeks. Hardware is removed only at 12–18 months if symptomatic (plate prominence or pain) — it is not routine. Complications
- Incidence
- 5–15 percent if unidentified
- Recognition
- Sudden brisk bleeding during lateral ramus exposure or drilling; hypotension; expanding retroperitoneal haematoma
- Prevention and management
- Identify and ligate under direct vision before retraction or drilling; if injured — immediate vascular control with clips or ties, pack the space of Retzius, vascular surgery review and consider angiographic embolisation
- Incidence
- Up to 15 percent of open-book injuries
- Recognition
- Blood at the meatus, high-riding prostate, inability to pass a Foley, CT cystogram extravasation
- Prevention and management
- Preoperative CT cystogram and urology review; decompress and protect the bladder; urologic repair, suprapubic catheter if the urethra is repaired, delay plating if infection is present
- Incidence
- 5–15 percent without posterior stabilisation; less than 5 percent with posterior fixation
- Recognition
- Recurrent symphyseal diastasis on follow-up radiographs; pain; hardware prominence
- Prevention and management
- Stabilise the posterior ring (SI screws or posterior plating); at least three screws on each side of a 6-hole plate; revision anterior plating with posterior stabilisation, consider double plating
- Incidence
- 3–8 percent
- Recognition
- Wound erythema, drainage, fever, raised CRP and white cell count; deep infection may involve the plate or bone
- Prevention and management
- Perioperative cefazolin, meticulous haemostasis, layered closure; superficial — oral antibiotics and wound care; deep — surgical debridement, IV antibiotics, hardware removal after union if loose
- Incidence
- 10–25 percent
- Recognition
- Progressive limitation of hip motion; radiographic calcification around the symphysis and rami
- Prevention and management
- Minimise soft-tissue stripping; consider indomethacin prophylaxis in high-risk patients; observe if asymptomatic, excise after maturation (greater than 6 months) if symptomatic
- Incidence
- 5–10 percent
- Recognition
- Persistent pain on single-leg stance; radiographic non-union or hardware failure
- Prevention and management
- Anatomic reduction and stable fixation with posterior stabilisation; activity modification and injections; revision with bone grafting and double plating for symptomatic non-union
Viva & Exam Focus
CORONACORONA — corona mortis and anterior ring dangers
PLATEPLATE — symphyseal plating principles
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old man is brought to the emergency department after a high-speed motor vehicle collision. The AP pelvis shows a 3.5 cm symphyseal diastasis with external rotation of both hemipelves, and CT confirms a sacral fracture displaced more than 1 cm. How do you plan definitive stabilisation?”
“During a Pfannenstiel approach for symphyseal plating you identify a large vessel crossing the superior pubic ramus 6 cm lateral to the symphysis. How do you manage this finding, and what complication are you preventing?”
“A 28-year-old woman undergoes symphyseal plating for an APC-II injury. At 6-month follow-up she has persistent anterior pelvic pain on single-leg stance, and radiographs show 4 mm of recurrent diastasis with one loose screw. What is the likely cause and how do you manage it?”
Diagnosis & indications
- Diastasis greater than 2.5 cm on AP pelvis indicates an open-book (APC) injury needing stabilisation
- Posterior ring instability coexists in most APC-II and all APC-III injuries — assess with CT and stress views
- Corona mortis present in 20–30 percent — crosses the superior ramus 5–7 cm lateral to the symphysis
- Bladder or urethral injury in up to 15 percent — mandatory preoperative CT cystogram
- Tile B1 / Young-Burgess APC-II and APC-III are the classic patterns requiring anterior plating
When & why
- Absolute: diastasis greater than 2.5 cm with instability (APC-II/III), combined ring injury, open injury, simultaneous bladder repair
- Relative: 1.5–2.5 cm diastasis with persistent pain after binder treatment, young high-demand patient, polytrauma for early mobilisation
- Contraindication: haemodynamic instability — use damage-control external fixation first
- Always stabilise the posterior ring with or before the anterior plate
Surgical anatomy & danger zones
- Pfannenstiel incision 2 cm above the symphysis; develop the space of Retzius and protect the bladder with a malleable retractor
- Elevate the rectus insertions from the pubic tubercles and tag for reattachment — prevents abdominal wall hernia
- Corona mortis: ligate before lateral ramus retraction or drilling
- Obturator nerve exits 2–3 cm lateral to the symphysis — stay subperiosteal during ramus exposure
- Spermatic cord / round ligament cross lateral to the pubic tubercle — identify and protect
Operative steps
- 1. Supine on a radiolucent table, Foley-decompressed bladder
- 2. Pfannenstiel incision, develop the space of Retzius, malleable retractor on the bladder
- 3. Elevate the rectus insertions, ligate the corona mortis, expose the superior rami 6–8 cm laterally
- 4. Reduce the symphysis with pointed clamps; confirm on AP, inlet and outlet views
- 5. Apply a 6- or 8-hole 3.5 mm reconstruction plate superiorly with three bicortical screws each side
- 6. Consider a second anterior plate in osteoporotic or comminuted bone
- 7. Reattach the rectus insertions, close the linea alba in layers
- 8. Stabilise the posterior ring (percutaneous SI screws) in the same sitting or staged
Plating & the posterior-ring principle
- Single superior 3.5 mm or 4.5 mm reconstruction plate with three screws each side when the posterior ring is stable
- Double plating (superior plus anterior) for APC-III, osteoporotic or comminuted bone
- Anterior plating restores greater than 80 percent of ring stiffness only when the posterior ring is stable
- Isolated anterior plating fails in up to 30 percent without posterior fixation (drops below 5 percent with it)
Post-op & complications
- Touch-down or partial weight-bearing for 6–12 weeks if the posterior ring was unstable
- Limit hip flexion to 90 degrees for 6 weeks to protect the repair
- AP, inlet and outlet radiographs at 2, 6 and 12 weeks
- Corona mortis bleeding 5–15 percent, plate failure 5–15 percent (less than 5 percent with posterior fixation), infection 3–8 percent, HO 10–25 percent
- Hardware removal at 12–18 months only if symptomatic
Background & Evidence
Relevant surgical anatomy - Pubic symphysis — a fibrocartilaginous joint between the medial ends of the pubic bones, stabilised by the superior and inferior pubic ligaments and the anterior and posterior ligaments; the 3–5 mm symphyseal disc is not violated during plating, and the pubic tubercles are the key landmarks for rectus insertion and plate placement.
- Corona mortis — an anomalous vascular anastomosis present in 20–30 percent of patients (up to 34 percent in anatomic series), arising from the inferior epigastric or external iliac artery and crossing the superior pubic ramus 5–7 cm lateral to the symphysis to drain into the obturator or external iliac vein; mean calibre about 2.5 mm.
- Space of Retzius — the extraperitoneal space between the pubic symphysis and the bladder, developed between rectus abdominis and transversalis fascia; the bladder lies immediately posterior and must be decompressed and protected.
- Rectus abdominis insertion — onto the superior pubic tubercle and the anterior pubic body; elevated sharply for exposure and reattached at closure to prevent hernia and maintain core stability.
- Spermatic cord / round ligament — cross the inguinal canal just lateral to the pubic tubercle and are protected by lateral retraction.
- Obturator nerve and vessels — exit the pelvis through the obturator canal 2–3 cm lateral to the symphysis; at risk during lateral superior ramus dissection and screw placement. Classification. The Young-Burgess anteroposterior compression (APC) grades describe how far the ring has opened and how unstable it is, and they map directly onto the operative decision:
- Mechanism
- Mild anteroposterior compression
- Posterior ring
- Symphysis widened less than 2.5 cm; posterior ligaments intact
- Typical management
- Symptomatic care; pelvic binder, surgery rarely needed
- Mechanism
- Moderate anteroposterior compression
- Posterior ring
- Diastasis greater than 2.5 cm; anterior SI ligaments disrupted, posterior SI intact — rotationally unstable, vertically stable
- Typical management
- Anterior symphyseal plating, with or without posterior SI screw fixation
- Mechanism
- Severe anteroposterior compression
- Posterior ring
- Complete posterior ring disruption (SI and sacrotuberous/sacrospinous ligaments) — rotationally and vertically unstable
- Typical management
- Anterior plating AND posterior fixation (SI screws or posterior plating)
In the Tile system these map to Tile B1 (open-book, rotationally unstable) for APC-II and Tile C (vertically unstable) for APC-III. Key evidence. Anterior symphyseal plating restores greater than 80 percent of native pelvic ring stiffness when the posterior ring is stable or simultaneously fixed. A single superior plate with three screws on each side is adequate for APC-II injuries, while double plating (superior plus anterior) is reserved for APC-III or osteoporotic bone. Implant failure runs 5–15 percent when posterior ring instability is not addressed and falls below 5 percent with concurrent posterior stabilisation — isolated anterior plating in the presence of a posterior ring injury leads to early plate breakage or screw loosening in up to 30 percent. Simultaneous or staged posterior fixation (percutaneous SI screws preferred) is the standard of care for APC-III and combined injuries. Anatomic series report the corona mortis in 20–40 percent of specimens, making its routine identification and ligation the single most important step in preventing life-threatening anterior pelvic bleeding.
References
Corona mortis. Incidence and location.
- Anatomic dissection demonstrated corona mortis in 34 percent of specimens
- Mean distance from the symphysis to the vessel crossing was 6.2 cm
- Vessel calibre averaged 2.5 mm — sufficient to cause significant bleeding if divided
Genitourinary injuries in pelvic fracture morbidity and mortality using the National Trauma Data Bank.
- Bladder injury in 14 percent and urethral injury in 5 percent of pelvic fractures
- Blood at the urethral meatus and high-riding prostate were highly specific for urethral injury
- CT cystogram detected all bladder injuries; delayed diagnosis increased infection risk
Does Posterior Fixation of Partially Unstable Open-Book Pelvic Ring Injuries Decrease Symphyseal Plate Failure? A Biomechanical Study.
- Posterior fixation significantly decreased symphyseal plate failure in partially unstable open-book injuries
- Isolated anterior plating had higher rates of failure under biomechanical testing
- Posterior stabilisation is critical to protect anterior constructs
Early failure of symphysis pubis plating.
- Early failure of symphysis pubis plating is associated with untreated posterior ring instability
- Recurrent diastasis and hardware loosening common when posterior ring not addressed
- Emphasises the necessity of comprehensive pelvic ring stabilisation