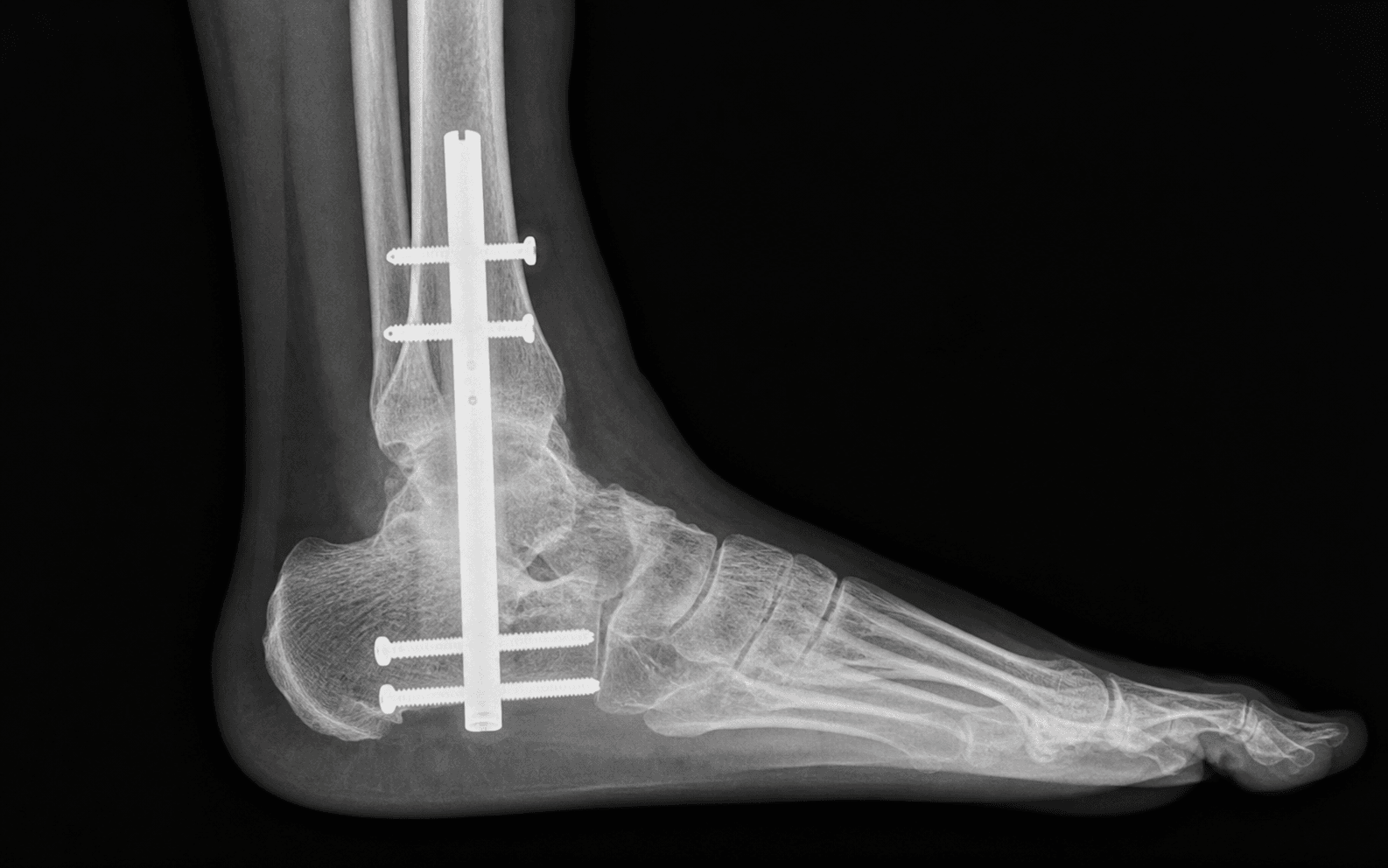
Simultaneous fusion of the tibiotalar and subtalar joints using a retrograde intramedullary nail | advanced
- Tibiotalocalcaneal (TTC) arthrodesis fuses BOTH the tibiotalar (ankle) AND subtalar (talocalcaneal) joints through a single retrograde intramedullary nail inserted from the plantar heel. Because the nail crosses both joints it is distinct from isolated ankle or subtalar fusion, and is reserved as a salvage procedure for combined end-stage disease when isolated fusion is insufficient.
- The plantar entry portal is the danger zone. The lateral plantar neurovascular bundle runs from the medial heel pad toward the lateral midfoot and lies just medial to the entry trajectory — place the incision slightly LATERAL to the heel-pad midline, identify the bundle medially, and retract it before reaming.
- Joint preparation combines an anterior ankle arthrotomy (or a lateral transfibular approach) with a sinus tarsi approach to the subtalar joint: denude cartilage, fish-scale the subchondral plate to bleeding bone, and correct alignment to a plantigrade hindfoot (5 degrees of valgus, neutral forefoot, tibial axis through the central hindfoot) BEFORE nail insertion.
- Union runs 70-90 percent in primary TTC fusion but falls to 50-70 percent in Charcot, avascular talus and failed total ankle replacement. Use a LONG nail (180-300 mm) to the tibial metaphysis — short nails ending in the diaphysis invite a stress fracture at the tip within 1-2 years.
- Varus malunion is the worst-tolerated alignment error: the patient loads the lateral border, develops fifth-metatarsal overload and may ulcerate. Small degrees of residual valgus are well tolerated; varus is not.
When & Why
The operation in one line. A retrograde intramedullary nail is driven from the plantar calcaneus across the subtalar and ankle joints into the tibial metaphysis, simultaneously arthrodesing both joints and bypassing global hindfoot pathology. It is a salvage procedure — the patient trades all ankle and hindfoot motion for a stable, pain-free, plantigrade foot. Primary indications. Reserve TTC arthrodesis for disease that isolated ankle or subtalar fusion cannot address:
- Combined tibiotalar AND subtalar arthritis — the most common indication; isolated fusion will not relieve the patient's pain.
- Failed total ankle replacement (TAR) with subtalar arthritis, talar component subsidence or aseptic loosening where revision TAR is not feasible.
- Charcot neuroarthropathy (Eichenholtz stage 2-3) of the hindfoot with instability, deformity or ulceration — a load-sharing construct that bypasses both joints.
- Avascular necrosis of the talus with collapse — either preserve the talus with structural graft bridging to the calcaneus, or perform talectomy with tibiocalcaneal arthrodesis.
- Severe hindfoot deformity (post-traumatic varus, equinocavovarus, equinus contracture) requiring correction across both joints.
- Failed prior ankle or subtalar arthrodesis with nonunion, malunion or symptomatic adjacent joint disease.
- Tumour resection of the talus requiring intercalary reconstruction. Relative indications include salvage of a failed TAR in a lower-demand patient (where conversion to a TTC nail is definitive), a talar body fracture too comminuted for ORIF, and severe post-traumatic hindfoot bone loss needing a bridging graft. Contraindications.
- Absolute: active infection (osteomyelitis of the tibia, talus or calcaneus) — clear it first with staged debridement; uncorrectable vascular insufficiency — check the ankle-brachial pressure index and revascularise first; severe peripheral neuropathy with open ulceration through the planned incision — heal the wound first.
- Relative: a young, high-demand patient — consider staged ankle and subtalar fusion to preserve whatever hindfoot motion is possible; active Charcot with severe fragmentation (Brodsky 3B) — consider external fixation or staged management; a smoker (nonunion risk up to 2-3 times higher — counsel and use graft adjuncts); severe osteoporosis (T-score less than minus 3) — consider a plate-augmented construct or external fixation. The one decision: TTC versus isolated or staged fusion.
- Fuse both joints when there is documented arthritis of both, a failed isolated fusion with symptomatic adjacent joint disease, a Charcot hindfoot, severe deformity across both joints, or AVN of the talus.
- Consider isolated or staged fusion when only one joint is diseased (isolated tibiotalar arthritis with a normal subtalar joint → ankle arthrodesis alone; isolated subtalar arthritis → subtalar arthrodesis alone), or in a young high-demand patient with combined disease where staged fusions preserve some hindfoot motion. In a young patient with a TAR and subtalar arthritis, TAR plus an isolated subtalar fusion retains ankle sagittal motion. Functional trade-off. TTC fusion sacrifices ALL ankle and subtalar motion for a stiff but functional gait. Staged ankle-plus-subtalar fusion ultimately loses both motions too — the practical difference is the order of surgery, not the final motion. A young patient undergoing TTC fusion is committed to a stiff hindfoot for life, so counsel carefully. Special-case decisions.
- Avascular talus: options are core decompression (early AVN without collapse), TTC arthrodesis with structural graft (talus preserved as a scaffold), talectomy with tibiocalcaneal arthrodesis (higher union, lower hindfoot height), and total talar replacement (emerging, limited long-term data).
- Failed TAR: when revision arthroplasty is not feasible (bone loss, infection, severe deformity), TTC nailing is the gold-standard salvage — there is no further revision option afterwards.
- Charcot: stage by Eichenholtz. Stage 1 (development) is managed conservatively in a total contact cast; stage 2 (coalescence) and stage 3 (reconstruction with residual deformity) are when TTC nailing is considered. Pre-operative work-up. Examine the foot in stance and gait — identify the deformity apex, skin status, ulceration and the soft-tissue envelope, and check the contralateral foot for reference alignment. Assess the Achilles with the Silfverskiold test (knee flexed and extended) to decide between gastrocnemius recession and formal Achilles lengthening. Document neurovascular status (posterior tibial and dorsalis pedis pulses, capillary refill, sensation). Image with weight-bearing AP, mortise and lateral ankle radiographs, a Saltzman hindfoot alignment view, CT for joint destruction and bone loss, and MRI (sagittal STIR/T1) for suspected AVN or Charcot. In diabetics, optimise hard before surgery: HbA1c less than 7.5 percent, fasting glucose controlled, albumin greater than 30 g/L, lymphocytes greater than 1500, and screen for Charcot with bilateral weight-bearing radiographs. If infection is suspected, check inflammatory markers, review the wound and aspirate. Consent. Quote specific risks: nonunion (10-30 percent overall, up to 40-50 percent in AVN and Charcot), malunion, infection (5-10 percent), nerve injury, plantar wound problems, stress fracture at the nail tip (3-8 percent), DVT/PE, complex regional pain syndrome, and the need for revision. Set realistic expectations: pain relief and a plantigrade foot, but loss of ALL ankle and hindfoot motion (inversion/eversion and dorsiflexion/plantarflexion) — the gait will be stiff but functional.
The Operation
The goal is a stable, pain-free, plantigrade hindfoot. The exposure is the heart of the operation: prepare both joints through an anterior (or lateral transfibular) approach and a sinus tarsi approach, then establish the plantar entry portal while protecting the lateral plantar neurovascular bundle, correct alignment, and lock a long nail across both joints.
Operative sequence
- Supine on a radiolucent table with a bump under the ipsilateral hip to bring the foot into neutral rotation; thigh tourniquet inflated after exsanguination; leg prepped and draped free from the knee distally.
- A foot-rest or towel stack under the calf lifts the heel off the table and improves access to the plantar entry portal.
- Image intensifier on the contralateral side — confirm AP and lateral views of the tibia, ankle and calcaneus are obtainable and the C-arm swings freely before draping.
- General or regional anaesthesia; pre-operative antibiotics (e.g. cefazolin 2 g IV) within 60 minutes of incision; tranexamic acid per local protocol.
- Prepare the iliac crest or proximal tibia if structural graft is anticipated — otherwise tibial reamings will provide sufficient cancellous autograft.
- Perform this FIRST. A percutaneous triple hemisection or a formal open Z-lengthening; aim for 5-10 degrees of dorsiflexion with the foot plantigrade.
- If the Silfverskiold test shows gastrocnemius-only contracture (dorsiflexion improves with knee flexion), a Strayer recession suffices and avoids the calcaneal gait of an over-lengthened Achilles.
- Danger of over-lengthening: calcaneal gait, push-off weakness, plantar heel ulceration. Danger of under-lengthening: residual equinus, rocker-bottom deformity, lateral forefoot overload. Confirm dorsiflexion with the knee in both extension and flexion.
- Anterior approach (most common): a longitudinal incision over the ankle just lateral to the extensor hallucis longus (EHL) tendon. The deep peroneal nerve and anterior tibial artery lie between EHL and extensor digitorum longus — identify and protect them. Open the extensor retinaculum, retract the tendons, and capsulotomise to expose the tibiotalar joint. The mortise-shaped tibiotalar articulation (distal tibial plafond and malleoli around the talar dome) moves primarily in the sagittal plane; the anterior capsule is thin and accessible, the posterior capsule thicker.
- Remove anterior osteophytes and cartilage with osteotomes, curettes and a burr; use a lamina spreader to reach the posterior cartilage. Fish-scale the subchondral plate to bleeding bone — sclerotic bone will not unite, and burr heat necrosis without irrigation causes bone death and nonunion.
- Lateral transfibular approach (Charcot, revision, severe deformity, or when anterior access is contraindicated): an oblique incision over the distal fibula continuing distally toward the sinus tarsi. Osteotomise the fibula 6-8 cm proximal to its tip and reflect it distally with the anterior talofibular and calcaneofibular ligaments intact (or detach and reattach through bone tunnels later). It gives a single broad view of both joints and the deformity, and the fibrectomy decompresses the lateral soft tissues — at the cost of the sural nerve and peroneal tendons in the field.
- A 3-4 cm incision over the sinus tarsi from the tip of the lateral malleolus toward the fourth metatarsal base. The sinus tarsi is the soft-tissue corridor between the talar neck and the posterior facet of the calcaneus — the key lateral route to the subtalar joint, whose posterior facet is the principal weight-bearing surface and whose oblique axis (posteromedial to anterolateral) governs inversion-eversion.
- Excise the sinus tarsi fat pad, open the posterior facet capsule, and denude cartilage with curettes and a high-speed burr; clear the middle and anterior facets through the same incision or a separate medial approach. Fish-scale both sides to punctate bleeding bone; pack any large cyst with cancellous graft from the tibial reamings.
- Dangers: the sural nerve (lateral border of the foot) and the peroneal tendons (peroneus longus beneath the cuboid, peroneus brevis at the fifth metatarsal base) posterior to the lateral malleolus; the flexor hallucis longus medially (it runs in a fibro-osseous tunnel along the posteromedial talus and beneath the sustentaculum tali, passing between the medial and lateral tubercles of the posterior talar process).
- Palpate the weight-bearing heel pad and make a 3-4 cm transverse or short oblique incision slightly LATERAL to the midline of the heel pad, centred over the calcaneal tuberosity.
- Dissect bluntly through subcutaneous fat. Identify the lateral plantar neurovascular bundle — it arises from the posterior tibial bundle beneath the flexor retinaculum and courses from the medial heel pad distally and laterally, deep to abductor hallucis and superficial to flexor digitorum brevis, toward the base of the fifth metatarsal. It lies MEDIAL to a correctly placed lateral entry — identify it, place a Senn or right-angle retractor medially to keep it out of the field, and never let it be the lateral-most structure in the wound.
- Incise the plantar fascia in line with its fibres, split flexor digitorum brevis in line with the incision, and identify the calcaneal tuberosity and posterior facet.
- Place the guide wire at the junction of the posterior and middle calcaneal facets, in line with the tibial canal. On AP it should lie in the centre of the tibial plafond; on lateral, in line with the tibial shaft axis, slightly posterior to the centre of the talar body. Do NOT start reaming until both views are perfect.
- Neighbouring anatomy to respect: the medial plantar nerve runs along the medial border of the plantar fascia toward the great toe (spared by a lateralised entry, at risk with extensive medial dissection); the posterior tibial bundle lies in the tarsal tunnel behind the medial malleolus; the sural nerve runs along the lateral foot; the saphenous nerve and vein run anteromedially.
- Ream sequentially over the guide wire from 8 mm, increasing in 0.5-1 mm increments, to 1 mm greater than the chosen nail diameter; collect cancellous autograft in the bone-sieve. Confirm trajectory on AP and lateral at each step.
- Select a nail length so the proximal tip rests in the tibial metaphysis — long nails of 180-300 mm reduce the risk of a stress fracture at the tip. Diameter is typically 10-13 mm, matched to the reamed canal.
- Dangers: reaming beyond the anterior tibial cortex (anterior cortical perforation); eccentric reaming (varus/valgus malalignment); inadequate reaming (nail incarceration or fracture); heat necrosis without irrigation.
- Before nail insertion, correct the hindfoot to a plantigrade position: 5 degrees of hindfoot valgus, neutral forefoot, tibial axis through the central hindfoot, 0-5 degrees of tibial torsion.
- Address residual equinus (the Achilles has already been lengthened); translate the calcaneus medially or laterally relative to the tibia as needed; hold the position with the guide wire and provisional K-wires during reaming.
- Check rotation by the position of the second metatarsal relative to the tibial crest. Confirm alignment on AP and lateral with the leg hanging free (no force) before final nail insertion.
- Varus is the worst-tolerated error (lateral border overload, fifth-metatarsal pain and ulceration); over-correction into valgus greater than 10 degrees causes lateral ankle pain and shoe difficulty; residual equinus produces a rocker-bottom and forefoot overload.
- Pack cancellous autograft (tibial reamings or iliac crest) into the tibiotalar and subtalar joints BEFORE nail insertion — it is far harder to do afterwards.
- For AVN, severe bone loss or Charcot, add a structural graft bridging the tibial plafond to the calcaneus: a tricortical iliac crest autograft (anterior crest preferred — less nerve injury than posterior) or a femoral-head allograft (no donor morbidity, slower incorporation). Consider a bone morphogenetic protein (BMP) adjunct in Charcot, AVN or revision.
- Distribute graft circumferentially around the nail after insertion. The graft is the biology; the nail is the stability — both are required.
- Insert the chosen nail over the guide wire under fluoroscopic control, watching depth and trajectory. Stop if there is resistance and re-check alignment — a nail that will not advance usually means a malalignment to correct, not more force.
- On lateral, confirm the proximal tip sits in the tibial metaphysis; on AP, that the nail is centred in the canal. Remove the guide wire and confirm rotational alignment before locking.
- Place proximal locking screws in the tibia through the targeting guide — typically two screws in different planes.
- Place distal locking screws in the calcaneus and talus. Use at least two calcaneal screws in different planes for rotational control (a single screw cannot provide it); add a talar screw if bone quality permits.
- Confirm all screw lengths on fluoroscopy — bicortical purchase in the calcaneus, and avoid a tip protruding into the plantar or medial soft tissues. In osteoporotic bone, consider longer screws or PMMA cement augmentation.
- Dangers: a screw breaching the subtalar or Chopart joint (measure carefully); a tip irritating a nerve or causing screw-head pain; loss of rotational control.
- Irrigate all wounds copiously. Close the anterior or lateral approach in layers — joint capsule, extensor retinaculum (if divided), subcutaneous tissue, skin; close the sinus tarsi incision in layers.
- Close the plantar incision meticulously in layers — the deep intrinsic muscle layer, the plantar fascia, subcutaneous tissue, then skin with interrupted non-absorbable sutures (nylon or Prolene). The plantar skin is a weight-bearing surface and any dehiscence is catastrophic.
- Apply a sterile non-adherent dressing and a well-padded posterior splint in neutral position. Do NOT apply a circumferential cast in theatre because of post-operative swelling.
- Dangers: plantar dehiscence (deep infection, nail exposure, potential loss of the construct); haematoma; suture under tension (skin necrosis); compartment syndrome from tight closure or a circumferential cast.
Before any reaming, identify the lateral plantar neurovascular bundle in the plantar wound. It courses from the medial heel pad toward the lateral midfoot, deep to abductor hallucis and superficial to flexor digitorum brevis, and lies just medial to a correctly sited entry trajectory. Place the incision slightly lateral to the heel-pad midline, stay lateral to the medial band of the plantar fascia, dissect bluntly, identify the bundle medially, retract it medially, and enter the calcaneus under direct vision. The bundle must never be the lateral-most structure in the wound. Injury (1-5 percent) presents as medial-sole/lateral-midfoot numbness or a painful plantar neuroma.
Use the anterior approach for most primary cases: it is direct and reliable, and it preserves the fibula for any future revision. Reserve the lateral transfibular approach for Charcot and revision cases with severe deformity — it gives a single broad view of both joints and the deformity, and the fibrectomy decompresses the lateral soft tissues, at the cost of the sural nerve and peroneal tendons in the field.
Select a long hindfoot nail of 180-300 mm so the proximal tip rests in the tibial metaphysis. A short nail ending in the tibial diaphysis concentrates stress at the tip and is a set-up for a transverse anterior tibial stress fracture 1-3 years post-operatively (an incidence of 3-8 percent). Ream to 1 mm greater than the nail diameter, sequentially, and collect the reamings for graft.
The single most important technical variable is a plantigrade foot. Check alignment with the leg hanging free and the foot plantigrade before finalising the nail: 5 degrees of hindfoot valgus, neutral forefoot, tibial axis through the central hindfoot. If the heel sits in varus, translate the calcaneus laterally or apply a medial closing-wedge correction at the ankle. Do not finalise the nail until the foot is plantigrade — small degrees of residual valgus are tolerated, varus is not.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation / weight-bearing | Milestones | |-------|--------|----------------------------------|------------| | Early | Day 0-14 | Posterior splint, well-padded; strict elevation 48-72 h; strict non-weight-bearing | Wound review at 48-72 h; multimodal analgesia; VTE prophylaxis | | Intermediate | Weeks 2-12 | Sutures out at 10-14 days; removable boot or short-leg cast once healed; progressive weight-bearing in a boot from 6-8 weeks in primary cases | Radiographs at 6 and 12 weeks for early bridging | | Consolidation | Weeks 12-24 | Boot weaning; custom-moulded foot orthosis | CT at 3-6 months if union is uncertain | | Return to function | 3-6 months+ | Long-term custom-moulded orthosis | Office work 8-12 weeks; manual work 4-6 months; low-impact sport from 6 months | Charcot and AVN cases remain strictly non-weight-bearing for 3 months and progress only when CT confirms union. Driving: right foot 8-12 weeks minimum; left foot in an automatic 4-6 weeks. High-impact sport is often not advisable after TTC fusion. Long-term follow-up monitors for a stress fracture at the nail tip (years 1-3) and adjacent-joint arthritis (years 3 and beyond). Complications
- Incidence
- 10-30 percent overall; up to 40-50 percent in AVN and Charcot
- Recognition
- Persistent pain greater than 6-9 months; no progressive bridging trabeculae on CT; lucency at the joint lines on serial radiographs
- Prevention & management
- Prevention: meticulous fish-scaling, structural graft in high-risk cases, BMP adjunct, prolonged non-weight-bearing (3 months) in Charcot/AVN. Management: CT at 6 months; revision with bone graft, nail exchange or addition of plate fixation at 9-12 months if symptomatic
- Incidence
- 5-15 percent
- Recognition
- Weight-bearing hindfoot view shows varus greater than 5 degrees; lateral border foot pain; fifth-metatarsal overload; lateral ulceration
- Prevention & management
- Prevention: aim for a plantigrade foot with 5 degrees of valgus intra-operatively; check alignment with the leg hanging free before final nail insertion. Management: custom-moulded orthosis for mild varus; revision osteotomy for symptomatic varus greater than 5 degrees
- Incidence
- 3-8 percent
- Recognition
- New anterior tibial pain 1-3 years post-operatively; transverse fracture line at the proximal nail tip on radiograph
- Prevention & management
- Prevention: use a long nail (180-300 mm) to the tibial metaphysis; avoid short nails ending in the diaphysis. Management: long-leg cast or brace; revision with a longer nail if symptomatic nonunion
- Incidence
- 1-5 percent
- Recognition
- Numbness or burning on the medial sole and lateral midfoot; positive Tinel sign; plantar neuroma
- Prevention & management
- Prevention: lateralised plantar incision; identify the lateral plantar bundle medially and retract; do not transect subcutaneous tissue blindly. Management: expectant for numbness; neuroma excision or burial for a painful neuroma
- Incidence
- 3-10 percent
- Recognition
- Plantar incision dehiscence; purulent discharge; exposed nail; deep infection
- Prevention & management
- Prevention: meticulous layered closure; non-weight-bearing on the plantar heel until healed (3-6 weeks); strict glucose control in diabetics. Management: wound care, oral or IV antibiotics; debridement and vacuum-assisted closure; nail removal only as a last resort
- Incidence
- 2-7 percent
- Recognition
- Persistent pain, fever, elevated CRP/ESR; deep wound drainage; bone lucency around the implant
- Prevention & management
- Prevention: sterile technique; peri-operative antibiotics; minimise operating time; avoid prolonged tourniquet. Management: two-stage revision — implant removal, debridement, antibiotic cement spacer, 6-8 weeks IV antibiotics, then revision nail
- Incidence
- 2-5 percent
- Recognition
- Pain over a screw head; Tinel sign from a screw irritating a nerve; CT shows a screw outside bone
- Prevention & management
- Prevention: measure screw lengths on fluoroscopy; bicortical purchase in the calcaneus; avoid medial screw protrusion. Management: remove the symptomatic screw once arthrodesis is healed (6-12 months)
- Incidence
- 1-3 percent
- Recognition
- Calf swelling and pain; PE: pleuritic chest pain, hypoxia, tachycardia; CTPA is definitive
- Prevention & management
- Prevention: mechanical prophylaxis (foot pumps, TED stockings); chemical prophylaxis per local protocol (enoxaparin 40 mg daily for 4-6 weeks in high-risk patients). Management: treat per haematology guidelines
- Incidence
- 1-3 percent
- Recognition
- Disproportionate pain; allodynia; hyperaesthesia; stiffness; trophic changes; bone demineralisation
- Prevention & management
- Prevention: gentle tissue handling; early mobilisation; vitamin C 500 mg daily for 6 weeks. Management: multidisciplinary pain clinic; gabapentinoids, bisphosphonates, sympathetic blocks; physiotherapy
- Incidence
- Up to 30 percent at 10 years
- Recognition
- Progressive midfoot pain; collapse of the medial longitudinal arch; midfoot swelling
- Prevention & management
- Prevention: plantigrade alignment at the index fusion; avoid overloading adjacent joints. Management: orthosis; midfoot fusion in late cases
Viva & Exam Focus
PLANTARPLANTAR — the entry portal: anatomy and dangers
HINDFOOTHINDFOOT — indications and decision-making
The trap: A plantar midline entry or a medialised nail transits directly through the bundle as it courses from the medial heel toward the lateral midfoot. The fix: Place the incision lateral to the heel-pad midline, stay lateral to the medial band of plantar fascia, dissect bluntly, identify the bundle medially and retract it. It must never be the lateral-most structure in the wound.
Location: Runs along the medial border of the plantar fascia from the medial heel toward the great toe; spared by a lateralised entry but at risk with extensive medial dissection or correction of severe valgus. Risk: Numbness and a painful neuroma of the medial sole and great toe. Identify and protect it during any medial dissection for tibial preparation or graft harvest.
Location: The posterior tibial artery, tibial nerve and veins lie behind the medial malleolus and enter the foot beneath the flexor retinaculum (tarsal tunnel), branching into medial and lateral plantar nerves. Risk: In a posterior approach to the ankle and subtalar joint, posterior retractors can injure or stretch the bundle. Identify it before any posterior capsular or subtalar work and keep retractors anterior to it.
The trap: In osteonecrosis of the talus the talar body is largely avascular, so standard tibiotalar coaptation has a nonunion rate up to 40-50 percent. The fix: Recognise AVN pre-operatively (MRI, or CT with sclerosis/crescent sign). Plan STRUCTURAL bone graft (tricortical iliac crest or femoral-head allograft) bridging the plafond to the calcaneus, or a tibiocalcaneal arthrodesis after talectomy. Warn the patient about the high nonunion rate and possible revision.
Why different: Charcot bone is hyperaemic, osteopenic and fragmented with poor screw purchase; the construct is load-bearing from day 1 and union runs 50-70 percent. Implications: Use a long nail to the tibial metaphysis, supplement with autogenous graft (tibial reamings, iliac crest or proximal tibia), consider adjunctive plating of the tibiotalar or subtalar joints, and accept prolonged non-weight-bearing (often 3 months) until union. Correct the rocker-bottom deformity and restore a plantigrade foot.
The trap: Leaving the hindfoot in varus loads the lateral border, causing fifth-metatarsal overload, lateral foot pain and lateral ulceration. The fix: Aim for a plantigrade foot with 5 degrees of valgus, neutral forefoot and the tibial axis through the central hindfoot. Small degrees of residual valgus are tolerated; varus is not.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old man with Type 2 diabetes and 6 months of midfoot and ankle swelling presents with a rocker-bottom deformity of the right foot and a non-healing plantar ulcer under the cuboid. The foot is warm, swollen and erythematous; protective sensation is absent on 10 g monofilament testing. What is your assessment and management plan?”
“A 58-year-old woman had a total ankle replacement 8 years ago for post-traumatic ankle arthritis. She now has progressive hindfoot pain, swelling and difficulty weight-bearing. Radiographs show talar component subsidence, polyethylene wear and subtalar joint-space narrowing, and conservative measures have failed. What are the options and which do you recommend?”
“A 45-year-old labourer presents 2 years after a talar neck fracture with collapse of the talar body and severe hindfoot pain. He is otherwise healthy and active. MRI shows extensive avascular necrosis of the talar body. What are the surgical options, and which do you recommend?”
Indication
- Fuses BOTH the tibiotalar and subtalar joints through one retrograde nail — distinct from isolated ankle or subtalar fusion
- Primary triggers: combined ankle and subtalar arthritis; failed TAR with subtalar arthritis; Charcot (Eichenholtz 2-3); talar AVN; severe deformity; failed prior fusion
- Absolute contraindications: active infection, uncorrectable ischaemia, open ulceration at the incision; relative: young high-demand, severe osteoporosis, smoker
Critical anatomy at the entry portal
- Plantar entry slightly LATERAL to the heel-pad midline, over the lateral half, in line with the tibial canal on AP and lateral
- Lateral plantar neurovascular bundle — the principal danger; lies medial to a lateral entry; identify and retract medially
- Medial plantar nerve — at risk with extensive medial dissection; posterior tibial bundle — at risk in a posterior approach
- Sural nerve at risk laterally; assess the Achilles with the Silfverskiold test and lengthen if equinus greater than 5 degrees
Pre-operative planning
- Clinical: alignment, soft-tissue envelope, ulceration, neurovascular status, Achilles contracture, the contralateral foot for reference
- Imaging: weight-bearing AP/mortise/lateral, Saltzman view, CT for bone loss, MRI for AVN or Charcot
- Optimise: HbA1c less than 7.5 percent, albumin greater than 30 g/L, no active infection
- Plan graft: tibial reamings for primary cases; structural iliac crest or femoral-head allograft for AVN/Charcot; BMP adjunct in revision
Operative sequence
- 1. Position supine on a radiolucent table, C-arm contralateral; 2. Lengthen the Achilles first if equinus
- 3. Prepare the ankle (anterior or lateral transfibular) and the subtalar joint (sinus tarsi) — fish-scale to bleeding bone
- 4. Plantar entry lateral to the heel-pad midline; guide wire confirmed on AP and lateral; 5. Ream to 1 mm greater than the nail, collect reamings
- 6. Correct to a plantigrade foot (5 degrees valgus); 7. Pack graft into both joints; 8. Insert a long nail (180-300 mm) to the metaphysis; 9. Multiplanar locking; 10-11. Meticulous layered closure, posterior splint
Danger zones
- Lateral plantar bundle — lateralise the incision, identify and retract medially
- Varus malalignment — the worst-tolerated error; aim for 5 degrees of valgus
- Short nail in the diaphysis — stress fracture at the tip; use a long nail to the metaphysis
- Eccentric entry — varus/valgus malalignment or tibial cortical perforation; confirm fluoroscopy at each step
- Achilles over-lengthening — calcaneal gait, push-off weakness, plantar heel ulceration
Implants and fixation
- Long hindfoot nail (180-300 mm) to the tibial metaphysis — preferred over short nails
- Diameter 10-13 mm, reamed 1 mm greater than the nail
- At least two calcaneal locking screws in different planes for rotational control; add a talar screw if bone permits
- Two proximal tibial screws in different planes via the targeting guide
- Graft: cancellous autograft for primary cases; structural allograft or iliac crest for AVN/Charcot; BMP in revision
Complications
- Nonunion 10-30 percent (up to 40-50 percent in AVN/Charcot); revision with graft, nail exchange or plate
- Varus malunion 5-15 percent — the worst-tolerated error; revision osteotomy if greater than 5 degrees
- Stress fracture at the nail tip 3-8 percent — prevented by a long nail
- Lateral plantar nerve injury 1-5 percent; plantar wound breakdown 3-10 percent; deep infection 2-7 percent
- DVT/PE 1-3 percent; CRPS 1-3 percent; adjacent joint arthritis up to 30 percent at 10 years
Post-operative protocol
- Strict non-weight-bearing for 6-12 weeks (3 months in Charcot and AVN)
- Posterior splint for 2 weeks, then a removable boot or short-leg cast
- CT at 6 months to confirm union if uncertain on radiographs
- Progressive weight-bearing in a boot from 6-8 weeks (12 weeks in Charcot/AVN)
- Long-term custom-moulded orthosis; driving 8-12 weeks (right foot); manual work 4-6 months
Special cases
- Failed TAR: TTC nail is the gold-standard salvage; structural graft for talar bone loss; long nail to the metaphysis; satisfaction 75-85 percent
- Charcot: long nail, graft and BMP, strict 3-month non-weight-bearing; limb salvage 85-90 percent at 5 years; union 50-70 percent
- Talar AVN: structural graft improves union; consider talectomy with tibiocalcaneal arthrodesis for severe collapse; union 50-70 percent
- Severe deformity: Achilles lengthening, soft-tissue release, osteotomy as needed; correct to plantigrade with 5 degrees of valgus
- Young high-demand patient: consider staged ankle and subtalar fusion to preserve motion; counsel on stiffness and irreversibility
Background & Evidence
Epidemiology of the indications. TTC arthrodesis is a salvage operation, so its epidemiology tracks its indications. Combined tibiotalar and subtalar arthritis most often follows intra-articular ankle fractures or inflammatory arthritis. Failed total ankle replacement is a growing indication: modern TAR has a 10-year survivorship of 80-90 percent in most series, but a proportion fail by talar component subsidence, polyethylene wear, aseptic loosening, deep infection or progression of subtalar arthritis. Charcot neuroarthropathy is increasing with the global diabetes pandemic and is a primary indication for the TTC nail. Classifications that guide decision-making.
- Stage / type
- Stage 1 (development)
- Features
- Swelling, erythema, warmth; no deformity; fragmentation on imaging
- Implication for TTC nailing
- Conservative — total contact cast; do not operate
- Stage / type
- Stage 2 (coalescence)
- Features
- Fragmentation and subluxation; reducing warmth
- Implication for TTC nailing
- Consider TTC nailing if deformity progresses
- Stage / type
- Stage 3 (reconstruction)
- Features
- Consolidation with residual deformity
- Implication for TTC nailing
- TTC nailing is the primary reconstruction
- Stage / type
- Type 1
- Features
- Midfoot (most common)
- Implication for TTC nailing
- Often managed with offloading/orthoses; TTC if hindfoot involved
- Stage / type
- Type 2
- Features
- Subtalar and Chopart joints
- Implication for TTC nailing
- TTC nailing when unstable or ulcerated
- Stage / type
- Type 3A / 3B
- Features
- Ankle (3A); ankle with calcaneal involvement (3B)
- Implication for TTC nailing
- TTC nailing for 3A; consider external fixation or staging for 3B
For talar avascular necrosis, the Ficat-Arlet classification (originally for the hip) can be applied to the talus, and MRI (sagittal STIR/T1) is the investigation of choice to define the extent of necrosis and talar-body viability. Outcomes by indication. Union and satisfaction differ markedly by pathology, which is why pre-operative counselling must be indication-specific.
- Union rate
- 70-90 percent
- Special considerations
- Standard technique; correct alignment carefully
- Adjuncts often required
- Cancellous autograft; BMP occasionally
- Union rate
- 75-85 percent
- Special considerations
- Talar bone loss; use a long nail; prepare the tibia to host bone
- Adjuncts often required
- Structural allograft; antibiotic cement spacer if infected
- Union rate
- 50-70 percent
- Special considerations
- Poor bone quality; long nail to the metaphysis; staged offloading
- Adjuncts often required
- Autograft; BMP; sometimes an adjunctive plate
- Union rate
- 50-70 percent
- Special considerations
- Talar collapse; consider talectomy with structural graft
- Adjuncts often required
- Tricortical iliac crest or femoral-head allograft
- Union rate
- 70-85 percent
- Special considerations
- Soft-tissue release, Achilles lengthening, osteotomy correction
- Adjuncts often required
- Autograft; internal bone stimulator
Primary TTC arthrodesis. A systematic review of retrograde hindfoot nailing reports union rates of 70-90 percent with modern compression and angle-stable nail designs. Patient satisfaction exceeds 75 percent, with substantial pain relief and improved function; gait analysis shows near-normal ankle power but loss of hindfoot inversion and eversion. AOFAS scores improve from a mean of 30-40 pre-operatively to 70-80 post-operatively. Time to union is 3-6 months in primary cases and up to 9-12 months in Charcot, AVN and revision. Failed total ankle replacement. A meta-analysis of TAR failures converted to a TTC nail reports union of 75-85 percent with satisfaction approaching that of primary TTC. The TTC nail is now considered the gold-standard salvage for failed TAR with subtalar arthritis; bone loss from the explanted talar component often requires structural graft or bone-substitute augmentation. Charcot neuroarthropathy. A multi-centre review of TTC nailing for Charcot reports union of 50-70 percent with limb salvage exceeding 85 percent at 5 years; correction of rocker-bottom deformity permits ulcer healing in 70-90 percent. Solid intramedullary constructs have largely replaced external fixation, and a long nail extending to the tibial metaphysis is preferred for stable load-sharing. Avascular necrosis of the talus. AVN is a high-risk subset with union of 50-70 percent; structural bone graft (autogenous iliac crest or femoral-head allograft) bridging the plafond to the calcaneus is often required, and talectomy with tibiocalcaneal arthrodesis (around 70 percent union) is the salvage option for severe AVN with collapse.
References
Risk factors for nonunion following tibiotalocalcaneal arthrodesis: a systematic review and meta-analysis
- Systematic review and meta-analysis of risk factors for nonunion after TTC arthrodesis with a retrograde intramedullary nail
- Diabetes, smoking, Charcot neuroarthropathy and avascular necrosis of the talus were the most consistently reported risk factors for nonunion
- Overall pooled nonunion rate was approximately 20-30 percent across studies, with Charcot and AVN subgroups having the highest rates
Tibiotalocalcaneal arthrodesis with a retrograde intramedullary nail: a prospective cohort study at a minimum five year follow-up
- Prospective cohort study of TTC arthrodesis with a retrograde intramedullary nail with minimum five-year follow-up
- Union achieved in the majority of patients; AOFAS and VAS pain scores improved significantly from pre-operative values
- Complications included nonunion, stress fracture at the nail tip and superficial wound infection; long nails to the tibial metaphysis were associated with lower stress-fracture rates
Tibiotalocalcaneal arthrodesis with structural allograft for management of large osseous defects of the hindfoot and ankle: a systematic review and meta-analysis
- Systematic review and meta-analysis of TTC arthrodesis with structural allograft for large osseous defects
- Union rates were acceptable with structural allograft supplementation, though lower than in primary arthrodesis without bone loss
- Femoral-head and tibial allograft were the most commonly used structural grafts; bulk allograft was required for failed TAR conversion and talar AVN
Comparison of dynamic versus static locked retrograde tibiotalocalcaneal arthrodesis with intramedullary nail fixation: evaluation of the RAIN database
- Multi-centre RAIN database study comparing dynamic compression versus static locked TTC arthrodesis
- Both fixation techniques achieved satisfactory union, with dynamic compression showing a trend toward faster time to radiographic union
- Complication profiles were similar between groups; nail-related complications were driven by stress fracture at the nail tip in short nails
Tibiotalocalcaneal arthrodesis using retrograde intramedullary nail fixation: comparison of patients with and without diabetes mellitus
- Comparative study of TTC arthrodesis with a retrograde nail in diabetic versus non-diabetic patients
- Non-diabetic patients had higher union rates and lower complication rates than diabetic patients
- Diabetic patients with well-controlled disease had outcomes approaching those of non-diabetics; glycaemic control was a key modifiable factor
Mid-term follow-up of patients with hindfoot arthrodesis with retrograde compression intramedullary nail in Charcot neuroarthropathy of the hindfoot
- Retrospective multi-centre series of Charcot hindfoot patients treated with a retrograde compression TTC nail with minimum two-year follow-up
- Union rates in the Charcot cohort were lower than primary TTC arthrodesis, consistent with the published literature; limb salvage remained high
- Long nail constructs extending to the tibial metaphysis and adjunctive bone grafting were associated with improved union
Tibio-talo-calcaneal arthrodesis with retrograde compression intramedullary nail fixation for salvage of failed total ankle replacement: a systematic review
- Systematic review of TTC arthrodesis with a retrograde compression nail for salvage of failed total ankle replacement
- The TTC nail is an effective salvage strategy for failed TAR with satisfactory union rates and functional improvement in most reported series
- Talar bone loss from the explanted component frequently required structural graft augmentation; a long nail to the tibial metaphysis was recommended
Salvage of avascular necrosis of the talus by combined ankle and hindfoot arthrodesis without structural bone graft
- Case series of patients with AVN of the talus treated with TTC arthrodesis without structural bone graft
- Combined ankle and hindfoot arthrodesis can salvage the AVN talus even without structural grafting, though union rates are lower than primary TTC
- Pre-operative staging of talar AVN severity guides the choice between in-situ fusion and talectomy with tibiocalcaneal arthrodesis